
Abstract
Background:
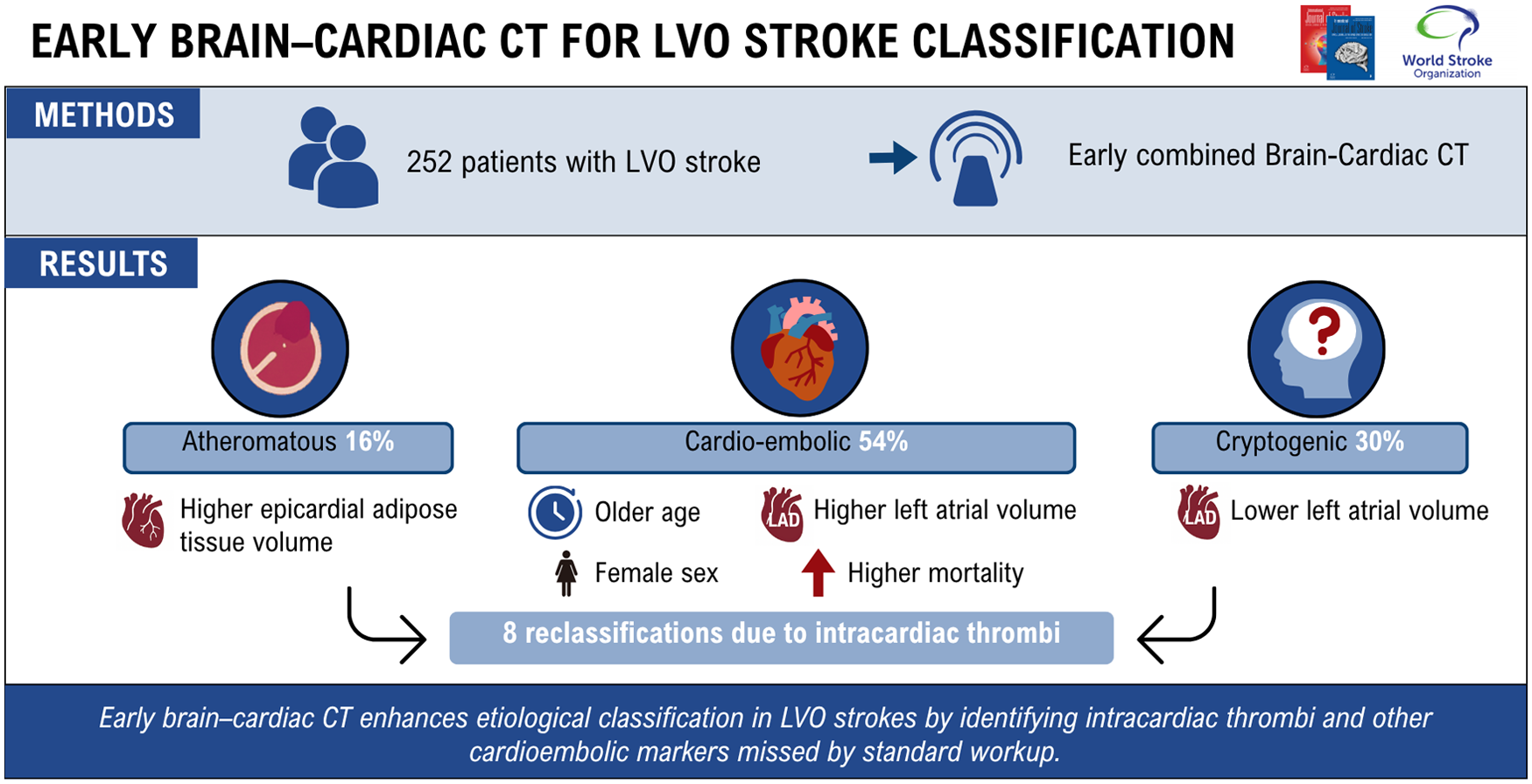
Timely identification of stroke etiology is crucial in managing large vessel occlusion (LVO) strokes. However, a substantial proportion remains cryptogenic despite comprehensive workup, raising concern about underdiagnosed cardioembolic sources. This study assessed the diagnostic contribution of early combined brain–cardiac CT imaging in patients with LVO stroke and explored imaging markers associated with each etiological subtype.
Methods:
A total of 252 consecutive patients admitted for LVO stroke who underwent standardized acute-phase brain and cardiac CT imaging were included. Patients were classified as atheromatous, cardioembolic, or cryptogenic LVO stroke before and after consideration of cardiac CT results. Clinical and imaging characteristics of patients were compared according to final causes of stroke.
Results:
Cardiac CT led to etiological reclassification in 8 patients (3.2%), including 7 cryptogenic cases upgraded to cardioembolic due to detection of intracardiac thrombi in the absence of atrial fibrillation. Patients with cardioembolic LVO stroke (n = 137, 54%) were older, more frequently women, and had higher left atrial surface areas and volumes compared to atheromatous (n = 40, 16%) and cryptogenic cases (n = 75, 30%). Epicardial adipose tissue volume was highest in atheromatous strokes, while cryptogenic cases lacked markers of atrial cardiomyopathy. At follow-up, mortality was highest in the cardioembolic group.
Conclusion:
Early brain–cardiac CT imaging enhances etiological classification in LVO strokes by identifying intracardiac thrombi and other cardioembolic markers missed by standard workup. A substantial subset of cryptogenic LVO strokes may represent a distinct pathophysiological entity. Broader adoption of cardiac CT could inform targeted stroke prevention strategies.
Introduction
Ischemic stroke due to large vessel occlusion (LVO) is associated with severe neurological deficits and poor functional outcomes.1,2 Timely identification of the underlying etiology is essential for guiding acute management and informing secondary prevention strategies. Cardioembolic stroke, most commonly related to atrial fibrillation (AF), is a leading etiology of LVO. Nevertheless, the detection of AF is frequently delayed or missed during initial hospitalization, complicating etiological classification of the cerebrovascular ischemic event. In addition, a substantial proportion of LVO strokes remain classified as cryptogenic, despite comprehensive diagnostic workups. This diagnostic uncertainty limits the ability to tailor treatment and may delay interventions that reduce the risk of recurrence. Recent advancements in imaging technologies including cardiac computed tomography (CT) offer promising tools. At our institution, the implementation of combined brain–cardiac CT imaging in the hyperacute phase of stroke care since 2018 enabled early and comprehensive vascular and cardiac assessment. 3 This protocol demonstrated high sensitivity and specificity for the detection of intracardiac thrombi.4,5 Moreover, recent evidence suggested that cardiac CT may provide early imaging markers of atrial cardiomyopathy—such as epicardial adipose tissue volume and left atrial remodeling—which could precede the clinical detection of AF. 6 In the specific context of LVO stroke, the potential usefulness of early cardiac CT to differentiate between underlying etiologies remains unclear. In addition, whether cryptogenic LVO represents an underrecognized cardioembolic subset or a distinct clinical entity is still a matter of debate.
The study aimed to evaluate the diagnostic contribution of combined brain–cardiac CT imaging in patients with LVO stroke. By comparing imaging and clinical characteristics across atheromatous, cardioembolic, and cryptogenic LVO subtypes, we investigated how cardiac CT might influence early etiological reclassification. We also explored the specific imaging biomarkers associated with each subtype to determine whether cryptogenic LVO strokes represent a distinct clinical and pathophysiological entity.
Methods
Study population
This retrospective analysis included 620 consecutive patients aged ⩾18 years old with imaging-confirmed acute ischemic stroke who were admitted to our University Hospital between November 2018 and March 2021, and who underwent combined brain–cardiac CT at the acute phase of stroke management.
Only patients with an LVO stroke were considered (Figure 1).
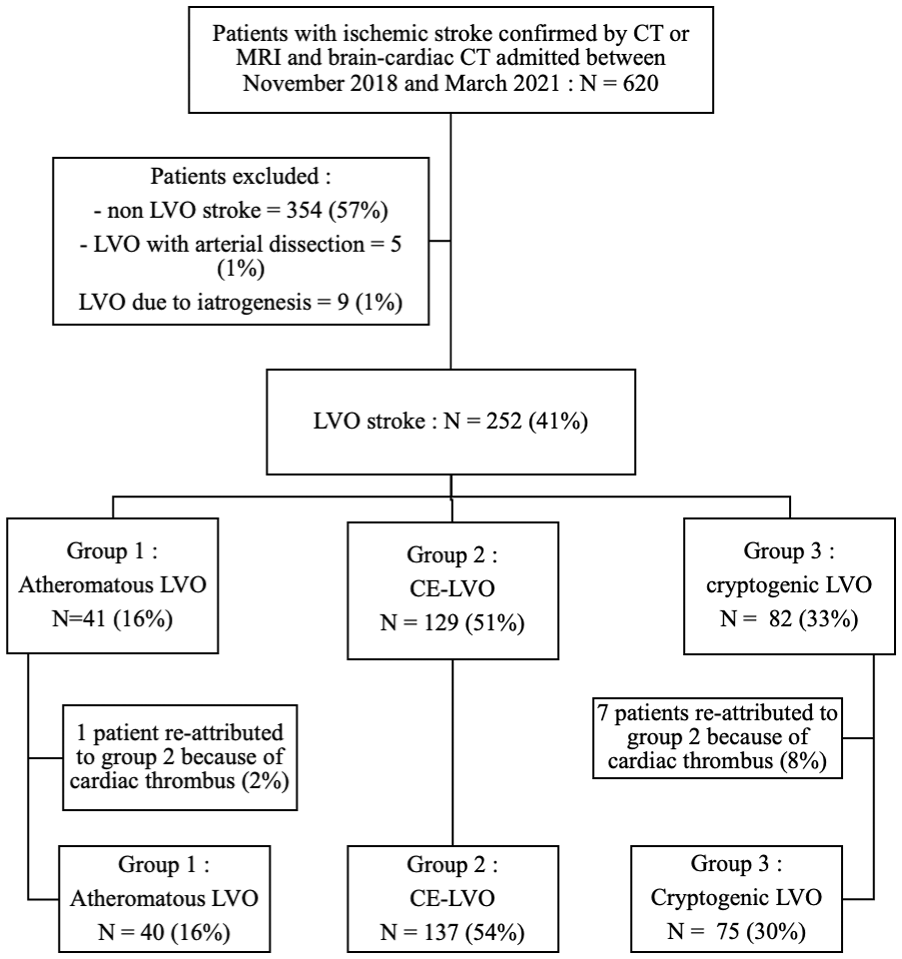
Flowchart of patient inclusion and etiological reclassification.
Imaging protocol
All patients underwent a brain CT scan, brain CT perfusion, angio-CT scan of aortic arch, cervical and intracranial arteries, and electrocardiogram (ECG)-gated cardiac CT scan in accordance with local protocol, using a 320-detector scanner (Aquilion ONE GENESIS, Canon Medical Systems, Otawara, Japan). This device allows an acquisition of the heart volume in a single rotation synchronized with the heartbeat 4 (Supplementary Table 1).
Imaging analysis
Patients’ imaging was reviewed by a senior neuroradiologist using a workstation (Centricity Universal Viewer, GE Healthcare, General Electric Company, United States, version 6.0). Acute ischemic stroke was defined as a low density on plain brain CT scan suggestive of a recent infarct corresponding to a vascular territory, and/or an increase of the time to peak on the perfusion CT. If there was no evidence of stroke on the cerebral CT with persistence of clinical symptoms, magnetic resonance imaging (MRI) with diffusion-weighted imaging was performed to confirm diagnosis. The site of arterial occlusion was determined on angio-CT scan. LVO of the anterior circulation was defined as an occlusion of the terminal intracranial internal carotid artery, M1 and M2 segments of the middle cerebral artery (including tandem occlusions), or A1 and A2 segments of the anterior cerebral artery. LVO of the posterior circulation was defined as an occlusion site affecting the basilar trunk or P1 segment of the posterior cerebral artery.
Left atrial appendage thrombus (LAAt) was defined as a well-circumscribed filling defect persisting on delayed-phase images with attenuation < 100 HU compared to the adjacent contrast-enhanced blood pool, slow flow as homogeneous attenuation between 100 and 120 HU without clear boundaries on delayed-phase images, and left ventricular thrombus as a persistent filling defect on end-systolic reconstructions with density difference >30 HU compared to the blood pool (Supplemental Figure 1).
All abnormalities on cardiac CT were reviewed by two radiologists specialized in cardiac and neurological imaging (A.B. and T.L.), and disagreements were resolved by consensus. Epicardial adipose tissue (EAT) volume and attenuation were measured by manually contouring the pericardium on axial slices to create a volume. Based on previous studies, 7 we defined a window range from −200 to −50 HU to isolate the fat tissue. The software then automatically calculated the EAT volume and attenuation.
Left atrial volume (LAV) and left atrial surface (LAS) were measured using the same contouring method.
Final diagnosis of ischemic stroke was confirmed by a stroke-trained neurologist based on clinical and imaging features. The etiological classification of ischemic stroke was derived from the TOAST (trial of ORG 10172 in acute stroke treatment) classification as follows: 8 large artery atheroma; cardioembolic ischemic stroke; and cryptogenic ischemic stroke. Since we excluded patients without LVO, no lacunar strokes were considered in this study. In addition, patients with LVO stroke from another determined cause as defined in the original TOAST classification were excluded from the analysis. Information was collected on the basis of the discharge report from the stroke unit and neurology ward.
Clinical and biological data
Clinical data including demographics, past medical history, cardiovascular risk factors, prior-to-stroke treatments, and acute stroke therapy (IV thrombolysis and mechanical thrombectomy) were gathered retrospectively from electronic medical records. Stroke severity at onset and discharge was assessed using the National Institutes of Health Stroke Scale (NIHSS) score. 9 The modified Rankin scale (mRS) score 10 was used to assess the disability at hospital discharge. Results from routine biological sample including were collected. Patent foramen ovale (PFO) evaluation relied on echocardiography (bubble study). PFO was considered stroke-related only when no alternative cause was identified and a significant shunt (≧ 20 microbubbles shunt within three cardiac cycles and/or interatrial septum aneurysm) was documented.
Follow-up
Patients were scheduled for outpatient visits with a neurologist at 6 months and with a neurologist or primary care physician every year, according to routine practice. Patients who received an implantable cardiac monitor (ICM) were scheduled for follow-up visits with a cardiologist at 6 weeks and then at 3-month intervals or via remote monitoring.
Statistical analysis
The statistical results of the continuous variables were presented as medians (first quartile—third quartile) and the results of the dichotomous variables as n (%). For categorical data, a chi-square or Fischer’s exact test was used. Continuous variables were analyzed using the Mann–Whitney U-test with Kruskal–Wallis post hoc test if appropriate. Kaplan-Meier survival statistics were used to assess survival. Data were censored at the last date of follow-up or death and compared using the log-rank test. The threshold of significance was set at 5%. All analyses were performed using SPSS 29.0 software (IBM Corp., Armonk, NY, USA).
Results
Patients’ characteristics
Of the 620 patients enrolled, 266 patients were diagnosed with LVO stroke (43%). Among them, 5 were attributed to arterial dissection, and 9 to a complication of a medical/surgical procedure (after cardiac surgery or percutaneous intervention) and were consequently excluded from the analysis. Without considering cardiac CT data, among the remaining 252 LVO patients, 41 (16%) would have been attributed to large atheroma (group 1: atheromatous LVO), 129 (51%) to cardioembolic causes (group 2: cardioembolic LVO), and 82 (33%) would have been classified of unknown etiology (group 3: cryptogenic LVO).
Cardiac CT led to a change in stroke etiology in 8 patients (3.2%): one patient was reclassified from group 1 to group 2 due to the presence of a left ventricular thrombus (1/41, 3%) and seven patients were reclassified from group 3 to group 2 (7/95, 7%), including 4 patients with LAAt in the absence of known AF or AF during hospitalization and 3 patients with a left ventricular thrombus.
Thus, 40 (16%) patients were finally attributed to major atheroma conditions (group 1: atheromatous LVO), 137 (54%) were attributed to cardioembolic causes (group 2: cardioembolic LVO), and 75 (30%) remained cryptogenic (group 3: cryptogenic LVO) at hospital discharge (Figure 1).
Baseline characteristics of patients according to final etiological diagnosis are shown in Table 1. The proportion of women was higher in the cardioembolic LVO group compared to atheromatous and cryptogenic LVO strokes (86/137, 62.8% vs. 15/40, 37.5%, p = 0.006 and 35/75, 46.7%, p = 0.006), and patients with cardioembolic LVO were older (82 (73–89) vs. 73 (61.5–81.8), p < 0.001 and 70 (58–82), p < 0.001).
Clinical and biological characteristics of patients with LVO according to final etiological diagnosis.
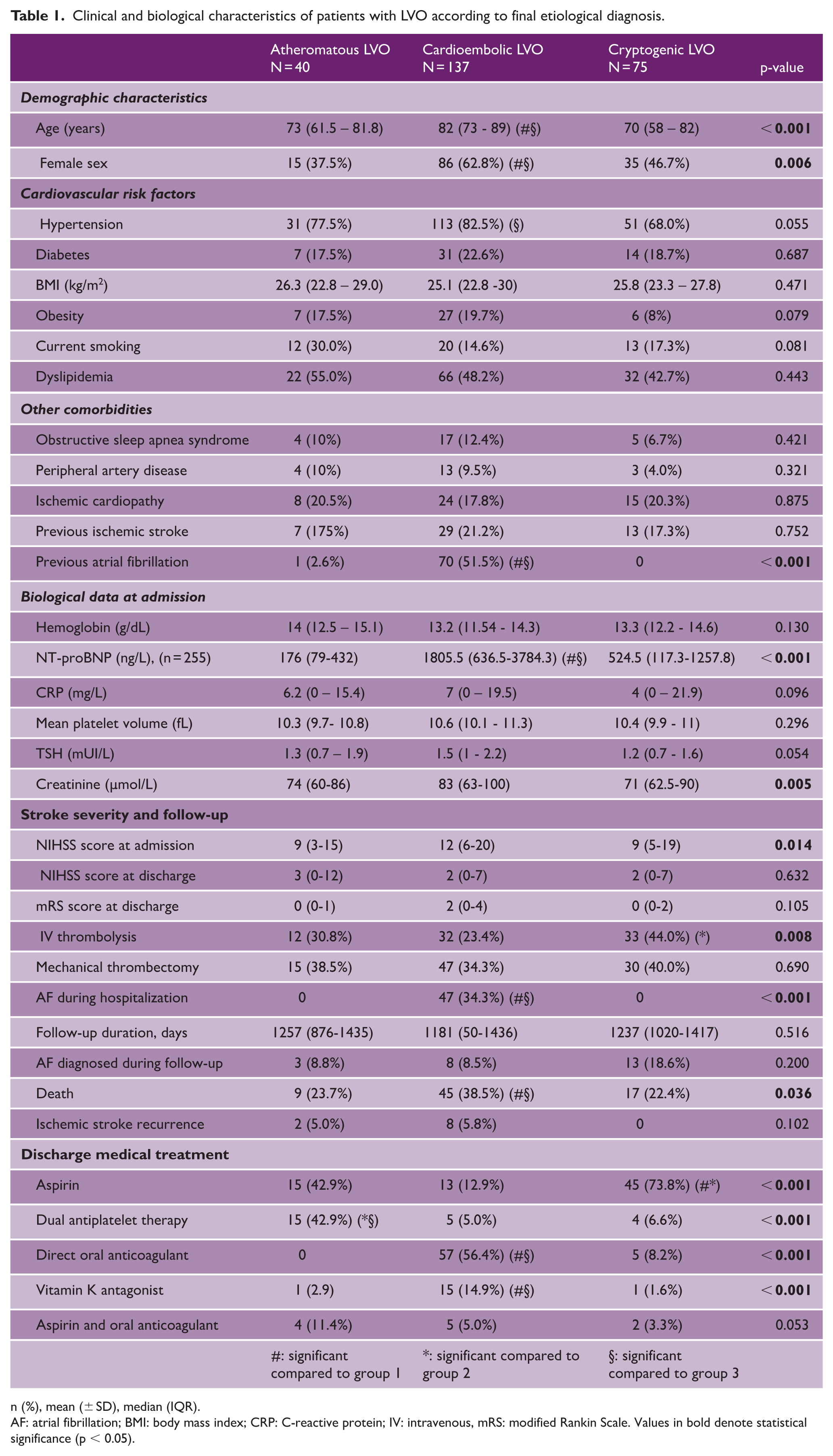
n (%), mean (± SD), median (IQR).
AF: atrial fibrillation; BMI: body mass index; CRP: C-reactive protein; IV: intravenous, mRS: modified Rankin Scale. Values in bold denote statistical significance (p < 0.05).
There was no difference in the distribution of other variables except for previous AF. Stroke severity at onset was greater among patients with cardioembolic LVO, but no difference was observed between groups regarding severity and disability at discharge. Patients with cryptogenic LVO were more frequently treated with IV thrombolysis. Regarding biological data, NT-pro-BNP levels were higher in the cardioembolic LVO group than in the atheromatous and cryptogenic groups (1805.5 (636.5–3784.3) ng/L vs. 176 (79–432) p < 0.001 and 524.5 (117.3–1257.8) p < 0.001, respectively).
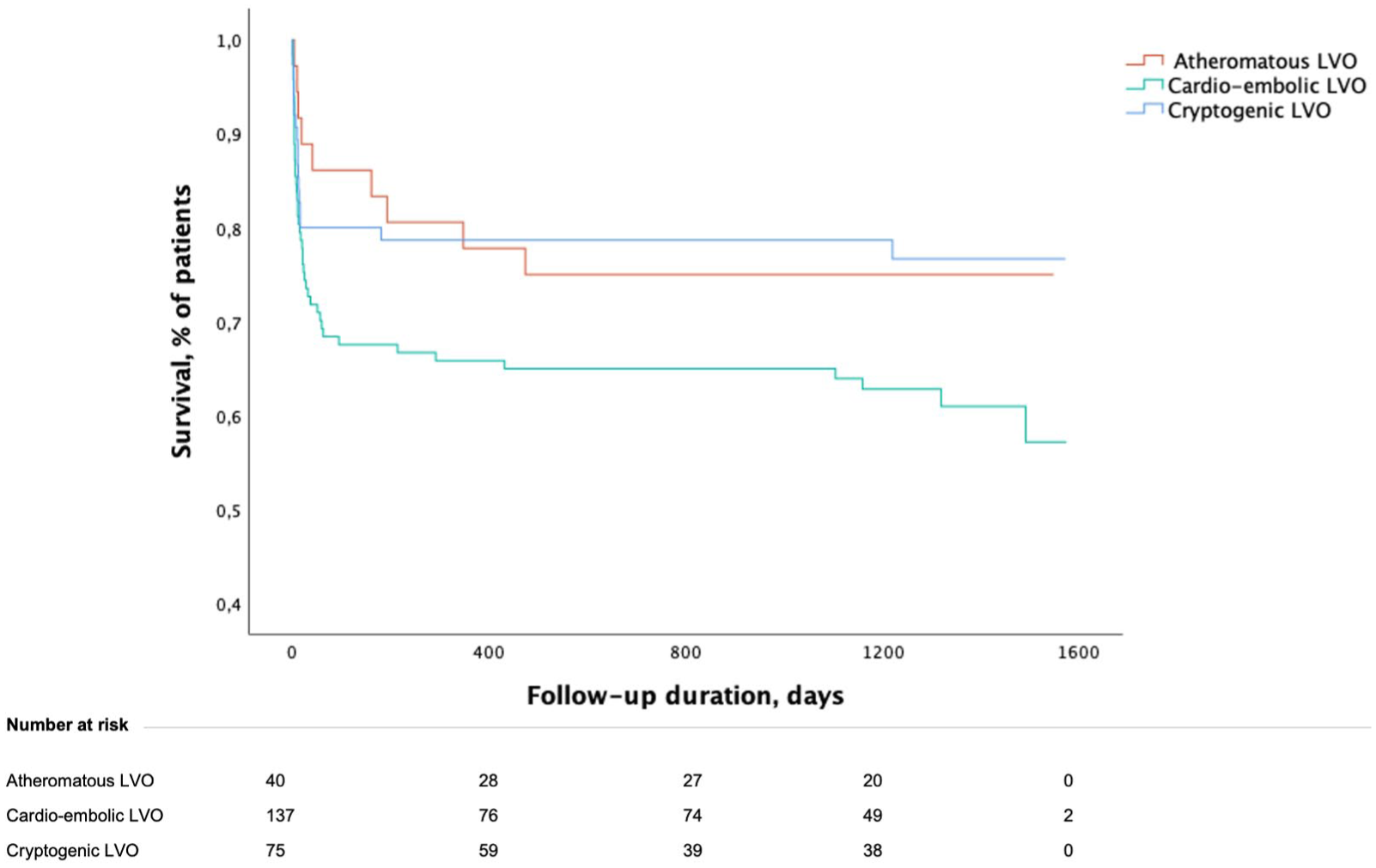
After a median follow-up of 1221 (2321417) days, patients with cardioembolic LVO had greater case-fatality (38.5% vs. 23.7% in patients with atheromatous LVO and 22.4% in patients with cryptogenic LVO, p = 0.036) (Figure 2). There was no difference between groups in recurrent ischemic stroke rate and new-onset AF after hospital discharge.
Kaplan–Meier curves for mortality according to stroke etiology. Survival estimates are shown for patients with large vessel occlusion (LVO) stroke stratified into atheromatous (n = 40), cardioembolic (n = 137), and cryptogenic (n = 75) groups. Log-rank test for overall comparison (p = 0.052).
In the cryptogenic LVO stroke group, AF was diagnosed in 13 patients (18.6%). Among them, six patients (8%) exhibited active malignancy, predominantly metastatic at the time of diagnosis. In addition, 3 patients (4%) were identified with blood coagulation disorders, while the remaining 53 patients (71%) continued to be classified as truly cryptogenic.
Imaging characteristics
Brain angio-CT showed significant variations in thrombi location, with tandem occlusions being more frequent in atheromatous LVO compared to cardioembolic and cryptogenic LVO (10/40, 25.0% vs. 2/137, 1.5% and 1/75, 1.3%, p < 0.001) (Table 2).
Imaging features across LVO etiological subgroups.
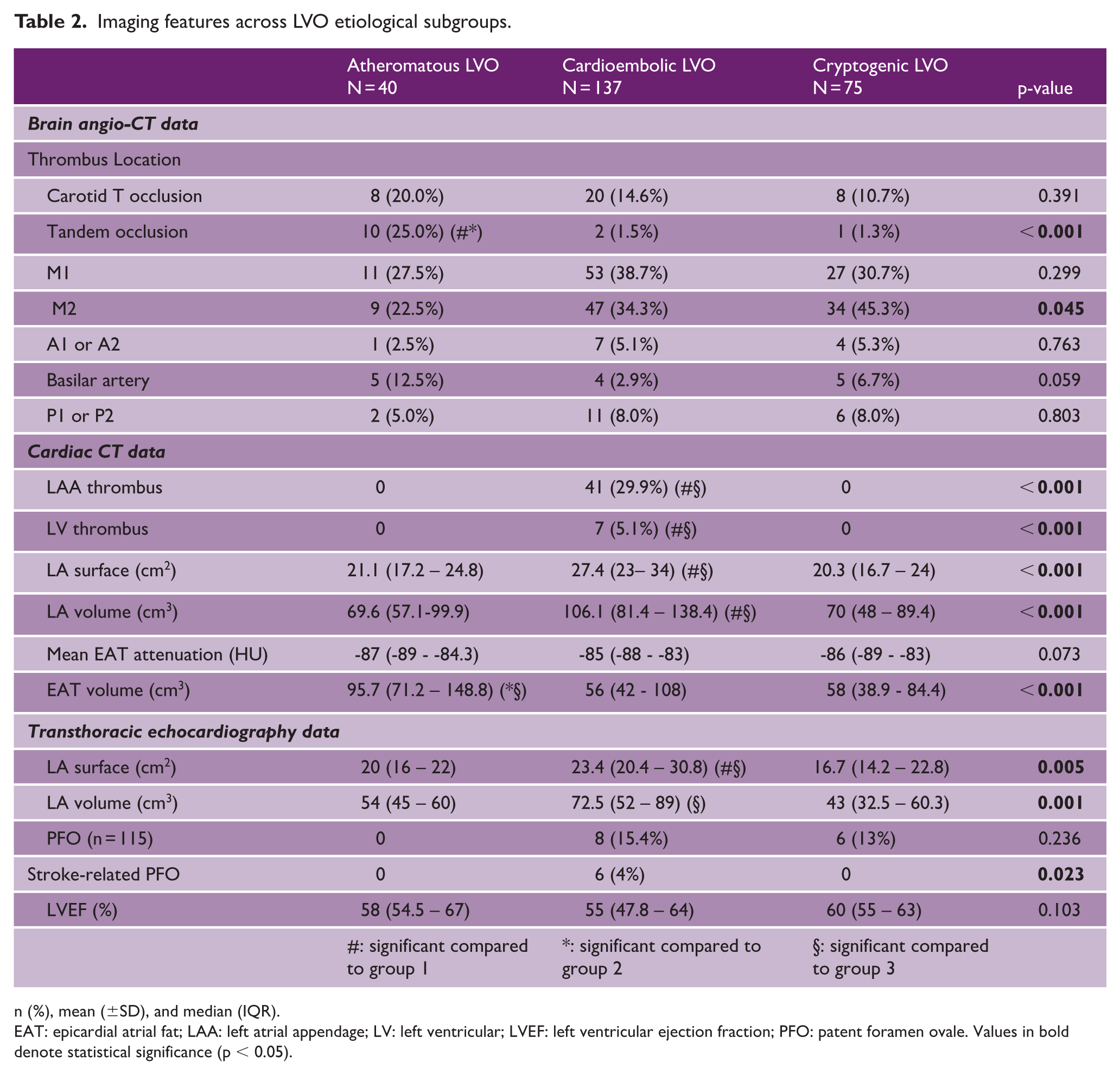
n (%), mean (±SD), and median (IQR).
EAT: epicardial atrial fat; LAA: left atrial appendage; LV: left ventricular; LVEF: left ventricular ejection fraction; PFO: patent foramen ovale. Values in bold denote statistical significance (p < 0.05).
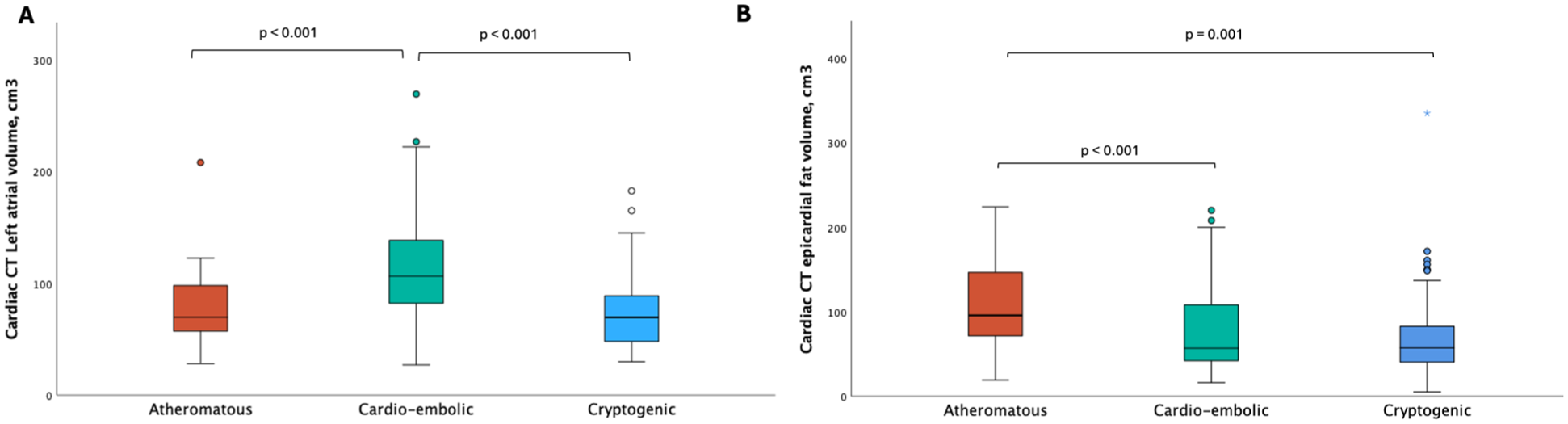
Cardiac CT data showed that 30% of cardioembolic LVO patients had a LAAt and 5% had a left ventricular thrombus. In our population, LAAt was found in 41 patients, 27 of whom had a history of AF. Of the remaining 14 patients, 10 were diagnosed with AF during hospitalization and 2 during follow-up, and among the remaining 2 patients, one died 8 days after stroke, and one was lost to follow-up. Cardioembolic LVO patients had a significantly higher left atrial (LA) surface area than atheromatous and cryptogenic LVO patients (27.4 (23–34) vs. 21.1 (17.2–24.8) and 20.3 (16.7–24), p < 0.001). They also had a higher LA volume (106.1 (81.4–138.4) vs. 69.6 (57.1–99.9), p < 0.001 and 70 (48–89.4), p < 0.001) (Figure 3(a)). Epicardial adipose tissue (EAT) volume was significantly higher in atheromatous LVO patients (95.7 (71.2–148.8)) than in cardioembolic (56 (42–108), p < 0.001) and cryptogenic LVO patients (58 (38.9–84.4), p = 0.001) (Figure 3(b)).
(a) Left atrial volume (cm3) and (b) Epicardial adipose tissue volume (cm3) measured by early combined brain–cardiac CT, stratified by stroke etiology in large vessel occlusion (LVO) patients. p-values derived from post hoc Kruskal–Wallis comparisons.
Transthoracic echocardiography also revealed a larger LA surface area in the cardioembolic group than in the atheromatous and cryptogenic groups (23.4 (20.4–30.8) vs. 20 (16–22), p = 0.005 and 16.7 (14.2–22.8), p = 0.005). LA volume followed a similar pattern between cardioembolic LVO and cryptogenic LVO (72.5 (52–89) vs. 43 (32.5–60.3), p = 0.001) but was not significantly different between cardioembolic LVO and atheromatous LVO (72.5 (52–89) vs. 54 (45–60), p = 0.082). In addition, six patients were classified as cardioembolic because they had a significant PFO in the absence of any other stroke etiology and were indicated for PFO closure.
Discussion
This study highlighted the value of combined brain–cardiac CT imaging in the acute stage of LVO strokes for their etiological classification. By enabling rapid detection of cardiac thrombi, this approach facilitated early reclassification of patients from cryptogenic to cardioembolic stroke. Furthermore, our findings suggest that truly cryptogenic LVO strokes, as defined after exhaustive cardiac imaging, did not exhibit typical cardioembolic markers such as left atrial dilatation or epicardial fat activation. This supports the hypothesis that mechanisms other than silent AF may contribute to these events.
Cardiac CT scan appears as an innovative tool in patients admitted for stroke with LVO. Previous study reported that it allowed the detection of intracardiac thrombus with a sensitivity of 0.99 and a specificity of 0.94 11 and was thus a safe alternative imaging modality for identification of LAAt compared to trans-esophageal echocardiography. 12 Thirty-five percent of patients classified as cardioembolic (48/147) in our study had a cardiac thrombus on admission, most commonly in the left atrial appendage. Although the detection of LAAt was associated with pre-stroke AF, as also pointed out in other studies, 13 8 patients did not have AF (either previously known or diagnosed during hospitalization) and would have been classified as cryptogenic without cardiac CT.
Moreover, early cardiac CT is useful for identifying left atrial dilatation that has been shown to be associated with LVO in patients with acute ischemic stroke. 14 Noteworthy, left atrial dilatation is strongly associated with atrial cardiomyopathy and the risk of developing AF at follow-up6,15,16 after stroke.
Furthermore, cardiac CT provides critical insights into left atrial dimensions and epicardial fat volume and attenuation, thereby enhancing the understanding of the cardiovascular context underlying different subtypes of LVO stroke.
Epicardial adipose tissue (EAT) is a visceral fat deposit surrounding the heart and coronary arteries, characterized by higher rates of lipogenesis and lipolysis compared to other visceral fat depots. Increased EAT volume has been demonstrated to be associated with subclinical atherosclerosis at multiple sites 17 and an elevated long-term cardiovascular risk, 18 leading to more fatal and non-fatal coronary events in the general population. 19 Our study corroborates these findings, as EAT volume was significantly greater in patients with atheromatous LVO compared to those with cryptogenic LVO. However, there was no significant difference in EAT volume between atheromatous and cardioembolic LVO patients. One explanation could be that we assessed the total cardiac EAT and not specifically that on the left atrium.
AF is the most common cause of cardio-embolism in stroke patients. 20 Previous studies showed that LA dilatation was associated with an increased incidence of AF 6 and a higher thromboembolic risk. 12 Similarly, in our study, patients with cardioembolic LVO more frequently exhibited LA remodeling with higher LA surface and volume than other groups. The different phenomenon that lead to LA dilatation are still not fully elucidated, but a recent study pointed out that high blood pressure was an independent risk factor for LA enlargement in patients with AF. 21
Regarding cardiac thrombus, it should be considered as direct evidence of cardioembolic origin of LVO, even in the absence of AF or previous myocardial infarction. LAA is the most common site of LA thrombus formation 22 and the incidence of LAAt in our population was 16%, one of the highest rates among published series of acute cardiac CT in the stroke setting. 23 This underscores the prevalence of cardioembolic mechanisms in LVO patients and the role of cardiac CT in detecting cardiac thromboembolism concurrently with stroke diagnosis.
Cryptogenic stroke remains frequent despite the implementation of diagnostic workup strategies in ischemic stroke patients. 24 Because cardiac CT can detect intracavitary thrombus and morphologic changes of the left atrium in cardioembolic patients, it helps to isolate purely cryptogenic causes.
In our study, 30% of LVO stroke cases remained of undetermined cause at discharge. Cryptogenic patients were more often men and were younger than cardioembolic patients, but we did not emphasize any other significant difference in their clinical baseline characteristics. An original finding of our study was that unlike cardioembolic LVO, cryptogenic LVO stroke did not harbor any sign of atrial cardiomyopathy, without left atrial dilatation on CT scan or echocardiography. However, at follow-up, 19% were diagnosed with AF. These results highlight the heterogeneity of cryptogenic stroke population, even in the case of LVO, where the more proximal occlusion may suggest more obvious pathophysiologic mechanisms.
Of note, several studies have attempted to delineate cardioembolic features within cryptogenic strokes, notably by comparing outcomes based on empiric anticoagulation versus antiplatelet therapy, but with inconclusive or neutral results, even when targeting patients with atrial cardiomyopathy criteria.25,26
Our study has several limitations. First, the single-center and retrospective design may have contributed to a risk of selection bias. However, because our institution serves as both a regional and community center, the potential for selection bias is probably mitigated. Second, the use of emergency CCTA in patients with suspected stroke is currently practiced by only a few centers, limiting the generalizability of our findings. Finally, LA contouring remains a time-consuming task for radiologists who do not have access to artificial intelligence tools, which can make this practice difficult to implement in daily practice. The implementation of automated measurements using artificial intelligence-guided software should help to generalize the use of cardiac CT in the acute stroke imaging protocol.
To conclude, this study highlighted the usefulness of early combined brain–cardiac CT imaging in the etiological assessment of LVO strokes. By enabling the detection of cardiac thrombi and markers of atrial cardiomyopathy, cardiac CT allowed reclassification of a subset of cryptogenic strokes as cardioembolic before discharge. Truly cryptogenic LVO cases showed distinct profiles, lacking typical cardioembolic features. These findings suggest that a portion of cryptogenic LVO strokes may represent a separate pathophysiological entity rather than unrecognized cardioembolism. Additional studies are needed to assess whether incorporating cardiac CT into acute stroke protocols could guide more targeted secondary prevention strategies.
Supplemental Material
sj-docx-1-wso-10.1177_17474930251398254 – Supplemental material for Early combined brain–cardiac CT imaging refines etiological classification of large vessel occlusion stroke
Supplemental material, sj-docx-1-wso-10.1177_17474930251398254 for Early combined brain–cardiac CT imaging refines etiological classification of large vessel occlusion stroke by Pierre-Antoine Garbuio, Cédric Fasolin, Angélique Bernard, Gauthier Duloquin, Thibault Leclercq, Soundous M’Rabet, Camil-Cassien Bamdé, Pierre-Olivier Comby, Frédéric Ricolfi, Yannick Béjot and Charles Guenancia in International Journal of Stroke
Supplemental Material
sj-docx-2-wso-10.1177_17474930251398254 – Supplemental material for Early combined brain–cardiac CT imaging refines etiological classification of large vessel occlusion stroke
Supplemental material, sj-docx-2-wso-10.1177_17474930251398254 for Early combined brain–cardiac CT imaging refines etiological classification of large vessel occlusion stroke by Pierre-Antoine Garbuio, Cédric Fasolin, Angélique Bernard, Gauthier Duloquin, Thibault Leclercq, Soundous M’Rabet, Camil-Cassien Bamdé, Pierre-Olivier Comby, Frédéric Ricolfi, Yannick Béjot and Charles Guenancia in International Journal of Stroke
Supplemental Material
sj-tif-3-wso-10.1177_17474930251398254 – Supplemental material for Early combined brain–cardiac CT imaging refines etiological classification of large vessel occlusion stroke
Supplemental material, sj-tif-3-wso-10.1177_17474930251398254 for Early combined brain–cardiac CT imaging refines etiological classification of large vessel occlusion stroke by Pierre-Antoine Garbuio, Cédric Fasolin, Angélique Bernard, Gauthier Duloquin, Thibault Leclercq, Soundous M’Rabet, Camil-Cassien Bamdé, Pierre-Olivier Comby, Frédéric Ricolfi, Yannick Béjot and Charles Guenancia in International Journal of Stroke
Footnotes
Acknowledgements
The authors acknowledge the use of automated writing assistance tools, including ChatGPT (OpenAI) and DeepL, to support the drafting and revision of the English manuscript. These tools were used to enhance clarity and language precision. The authors remain solely responsible for the accuracy, validity, and originality of the content.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics statement
In accordance with French ethical regulations (MR004), approval from an ethics committee was not required. The study was registered with the French National Health Data Hub (ID: 23294219) and conducted in compliance with the Declaration of Helsinki, as revised in 2013.
Data availability
Data available upon request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.