
Abstract
Background:
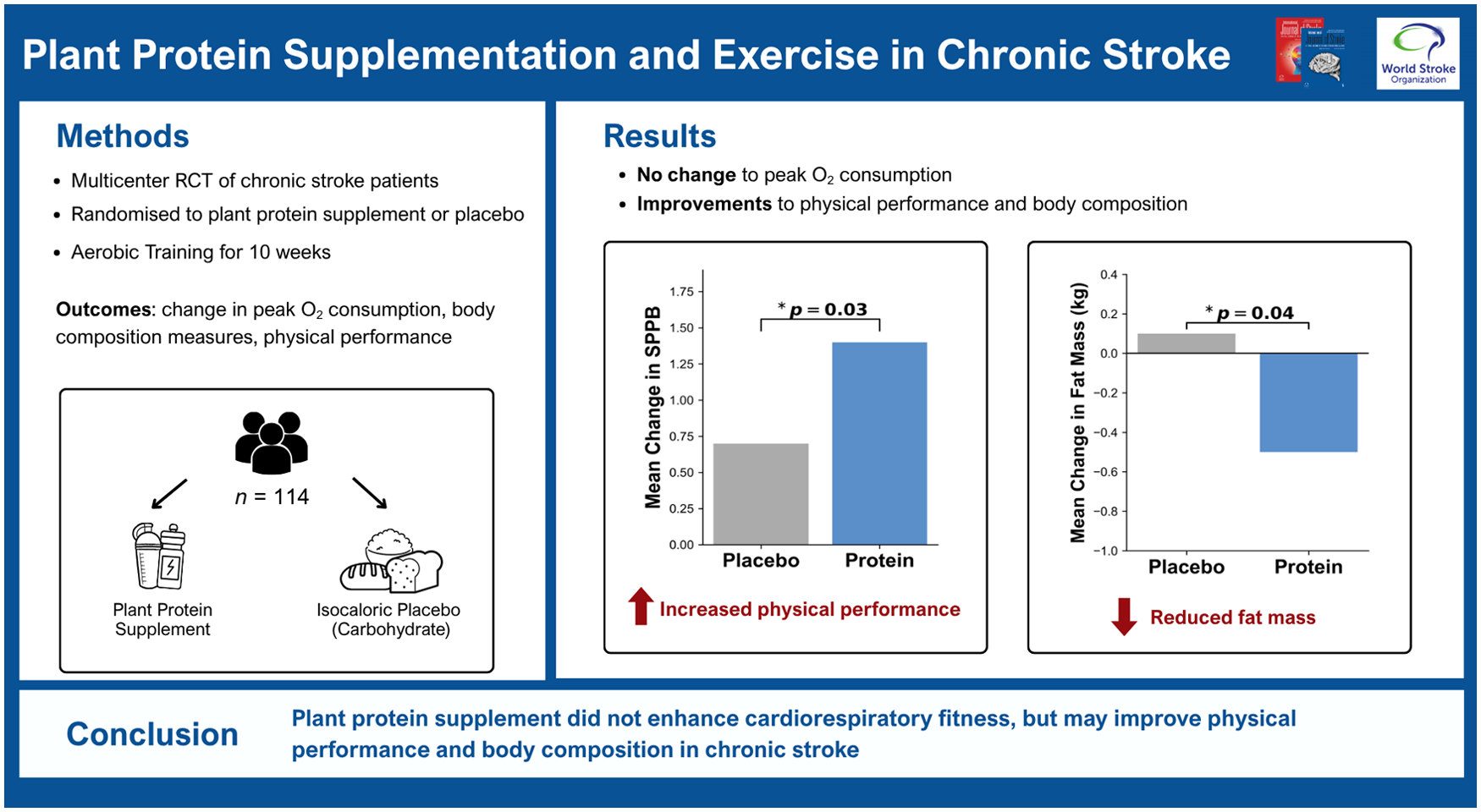
Decreased cardiorespiratory fitness (CRF) is prevalent in stroke patients, and aerobic training can improve CRF in this population. Protein supplementation has been proposed as a strategy to enhance exercise adaptations by promoting muscle protein synthesis, reducing muscle loss, and improving physical function. However, the potential of protein supplementation to further improve CRF during aerobic training among stroke patients remains unclear. This study aims to evaluate the effect of protein supplementation on CRF and physical performance in patients with chronic stroke undergoing aerobic training.
Methods:
This multicenter, participant- and assessor-blinded, randomized clinical trial enrolled 114 ambulatory adults with chronic stroke at four teaching hospitals. Participants were randomized to receive protein supplementation (n = 58) or an isocaloric carbohydrate placebo (n = 56) during 30 supervised aerobic training sessions over 10 weeks. The primary outcome was the change in peak oxygen consumption (V̇O2peak, mL/kg/min) at 11 weeks. Secondary outcomes included CRF-related measures, body composition (total lean and fat mass), and physical performance (Short Physical Performance Battery (SPPB), Physical Performance Test, Berg Balance Scale, and Timed Up-and-Go test).
Results:
Participants had a mean age of 57.2 years, 30% were women, and 87% completed the primary outcome assessment. At the 11-week follow-up, V̇O2peak increased by 1.7 mL/kg/min (95% CI: 1.0–2.4) in the protein group and 1.6 mL/kg/min (95% CI: 0.9–2.3) in the placebo group, with no between-group difference (mean difference, 0.1 mL/kg/min; 95% CI: −0.8 to 1.1; p = 0.43). Both groups showed improvements in most CRF-related and physical performance measures. At 20 weeks, the protein group demonstrated greater SPPB improvement (mean difference, 0.7 points; 95% CI: 0.1–1.3; p = 0.03) and lower fat mass at 11 weeks (mean difference, −0.6 kg; 95% CI: −1.2 to −0.06; p = 0.04).
Conclusions:
Protein supplementation during aerobic training did not significantly enhance CRF compared with an isocaloric placebo. These findings warrant further investigation in populations with a broader range of baseline protein intake.
Introduction
Cardiorespiratory fitness (CRF) is widely recognized as an important predictor of health outcomes and mortality across various populations. 1 Among stroke survivors, low CRF is prevalent, 2 with peak oxygen consumption (V̇O2peak) values reported to be as low as half those of age- and sex-matched healthy controls. 3 Aerobic training after stroke holds the potential to enhance CRF and physical performance.4,5
Protein supplementation has gained popularity as a strategy to enhance the effects of exercise training.6,7 This approach is based on the rationale that protein supplementation can amplify post-exercise muscle protein synthesis, inhibit muscle protein breakdown, and thereby stimulate net muscle protein accretion. 8 While the majority of supporting evidence comes from the research focused on the impact of protein supplementation on resistance training-induced gains in muscle mass and strength, 9 its potential benefit in improving CRF during aerobic training remains insufficient and studies have reported conflicting findings. 10 Yet, a recent meta-analysis indicated a potential of 26.4% additional gain in V̇O2peak to aerobic training among various populations (e.g. healthy adults, COPD patients, mobility-limited older adults, healthy marines, trained cyclists, and others). 11 Only two of the studies included in this meta-analysis were conducted among stroke patients, a population with unique needs for recovery and rehabilitation. This highlights the necessity for a randomized controlled trial to assess the aforementioned potential benefits of protein supplementation in stroke patients.
The Incorporating Supplementary Protein into Rehabilitative Exercise (INSPIRE) trial is a multicenter, double-blinded, randomized controlled trial designed to determine whether dietary protein supplementation further improves CRF and physical performance, compared with isocaloric placebo, in patients with chronic stroke undergoing aerobic-dominant training.
Methods
Study design
The INSPIRE trial was conducted at four teaching hospitals (Taipei Medical University Hospital, Wan Fang Hospital, Shuang Ho Hospital, Taipei Tzu Chi Hospital) in Taipei to ensure diverse representation among trial participants. The Joint Institutional Review Board of Taipei Medical University reviewed and approved the research protocol (approval number: N201810056). This trial was registered at clinicaltrials.gov (NCT03637270). This double-blinded, multicenter, randomized clinical trial with two parallel groups enrolled participants between December 2018 and January 2023, and the follow-ups were completed by April 2023. The study protocol followed that of our pilot study. 12 The detailed study protocol (Supplement 1) is available online.
Participants
The study participants were adults (aged 20–75 years) who had a stroke that occurred over 6 months before recruitment, were able to walk independently for 10 min (with or without orthosis), and were able to use a stationary bike. Those who were unable to coordinate with examination or treatment, had malnutrition, renal insufficiency, or a body mass index > 35 kg/m2 were excluded. Eligible participants who provided written consent were arranged with a cardiopulmonary exercise test (CPET). Those who were unable to tolerate CPET (e.g. too short stature to fit the machine, too strong leg spasticity to peddle, unable to maintain 50 r/min at the beginning of CPET, and indications for early termination of CPET based on the American College of Sports Medicine suggestions) were excluded.
Randomization and masking
Participants were randomly assigned in a 1:1 ratio to either the protein supplementation (protein) or isocaloric placebo supplementation (placebo) group. A central coordinator who was responsible for concealing the allocation performed the computer-generated randomization, with block sizes of four stratified by sex. The protein and placebo supplements were identical in terms of appearance. The procedure of masking and blinding efficiency was introduced in our pilot study 12 and Supplement 1. The participants and outcome assessors were blinded to the group allocation.
Interventions
All participants underwent 40-min aerobic training followed by approximately 10-min resistance training three times per week for 10 weeks at the Department of Rehabilitation of recruiting hospitals under the supervision of a site trainer. Aerobic training with cycling ergometry included 5-min warm-up and 5-min cool-down. During the 30-min training period, the participants maintained an intensity of 60% to 80% heart rate reserve determined by the baseline CPET. 12 The resistance training included three sets of 15 repetitions of resisted arm reaching and sit-to-stand movements using TheraBand and a vest with weight loads. Progressive resistance was achieved by using TheraBand with different levels of resistance and a gradual increase in the weight of the jacket depending on the individual’s tolerance and performance. (Supplement 1)
Nutritional supplements were produced in the laboratory of the Graduate Institute of Sports Science at the National Taiwan Sport University. A 40 g serving of the protein supplement which was made from isolate soy protein contained 23.2 g of protein, 11 g of carbohydrates, and 144.2 kcal, while a 40 g serving of the carbohydrate-based control supplement contained identical calories but 35.2 g of carbohydrates and 0.2 g of protein. This isocaloric carbohydrate-based placebo was used as the control to distinguish the specific effects of protein supplementation from those of additional caloric intake alone. The Protein group drank 20 g of protein supplement powder dissolved in 250 mL of water immediately before and after each training session, whereas the control group drank the placebo supplement under the same setting (Details of the nutritional supplement composition are provided in Supplement 1).
All participants received usual care including outpatient stroke rehabilitation if clinically needed.
Measurement
Basic characteristics
Basic participant characteristics, including sociodemographic data, stroke-related information, comorbidities, and associated medications, were obtained through interviews and chart reviews using structured questionnaires. Baseline nutritional intake was assessed using two 3 day diet diaries (including two weekdays and one weekend day) collected before the intervention. Participants received two 1-week dietary education courses prior to the intervention to ensure accurate reporting. A registered dietitian reviewed the dietary records, scored the Mini Nutritional Assessment based on the interview and dietary diaries, 13 estimated the daily nutritional intake, and provided suggestions aimed at avoiding body weight changes during the intervention. Information obtained from CPET was recorded. The V̇O2peak value was transformed as the percentage of expected value of the healthy population with Itoh’s formula. 14 Serum blood urea nitrogen and creatinine were checked.
Primary outcome
The primary outcome was the 11-week change in V̇O2peak value (mL/kg/min), which was assessed via CPET performed by an experienced physiatrist in an environmentally controlled laboratory. A standardized symptom-limited ramp protocol was conducted using a cycle ergometer (VIAsprint 150 P; Ergoline, Bitz, Germany). Details of outcome assessments are described in Supplement 1. Although the minimal clinically important change of V̇O2peak is unclear, it has been reported that every 3.5 mL/kg/min (equal to 1 metabolic equivalence of task) increase in V̇O2peak is associated with 10%–25% improvement in overall survival.1,15 Moreover, a modest gain in V̇O2peak in individuals with chronic stroke, irrespective of traditional risk factors and initial CRF level, can improve daily functional capacity, mobility, and quality of life.16,17
Secondary outcomes
The secondary outcomes covered three aspects: (1) CRF-related outcomes, including V̇O2peak (at 20 week), workloadpeak measured by CPET, 18 and 6-min walk test 19 ; (2) body composition outcomes, including total lean mass and fat mass measured by dual-energy x-ray absorptiometry 20 ; and (3) physical performance outcomes, including the 9-item Physical Performance Test (score range, 0 to 36 (best performance)), 21 Short Physical Performance Battery (score range, 0 to 12(best performance)), 22 Berg Balance Scale (score range, 0 to 56 (best performance)), 23 Timed Up-and-Go test, 24 and maximal voluntary isometric contraction of the affected quadriceps. 25 All the outcomes were measured at baseline, 11-week, and 20-week follow-ups.
In addition, adherence was evaluated on the basis of the number of training sessions attended. Compliance with training intensity was evaluated by the achievement of the target heart rate (i.e. 60%–80% heart rate reserve) at the mid time point of each aerobic training session. 12 The number of sessions in which the target heart rate was achieved was recorded. Adverse events that occurred during the study period were collected at 11- and 20-week follow-ups. If the participants received concurrent rehabilitation for usual care, the number of physical and occupational therapy sessions during the intervention period was recorded.
Statistics
Sample size
Based on our pilot study, 12 which reported an effect size of 0.62 regarding the between-group difference of V̇O2peak (mL/kg/min) after the intervention, a minimal total of 106 was required, considering an alpha of 0.05, a power of 80%, 2-tailed, and an estimated drop-out rate of 20%.
Statistical analysis
Participants were analyzed based on their originally assigned randomization group. For the comparison of baseline characteristics between the two groups, the independent t-test and chi-square test were used for continuous variables and for categorical variables, respectively. For primary and secondary outcomes, the paired t-test was used to assess within-group changes and the independent t-test was performed to investigate the between-group differences in changes between the baseline and follow-ups. A two-tailed p-value of < 0.05 represented statistical significance. Data were analyzed using R version 4.3.0 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Among the 114 participants randomized (mean age 57.2 years (SD = 8.2), 70.2% male), 106 (93.0%) completed the intervention, 94 (82.5%) completed the primary outcome assessment at 11-week follow-up, and 92 (80.7%) contributed data for at least one secondary outcomes at 20-week follow-up. Loss to follow-up and withdrawal was primarily due to COVID-19-related issues (Figure 1). Specifically, before the 11-week assessment, 3 of 58 participants (5.2%) in the protein group and 2 of 56 (3.6%) in the placebo group were lost to follow-up due to COVID-19-related issues, with no significant difference in COVID infection rate between the groups.
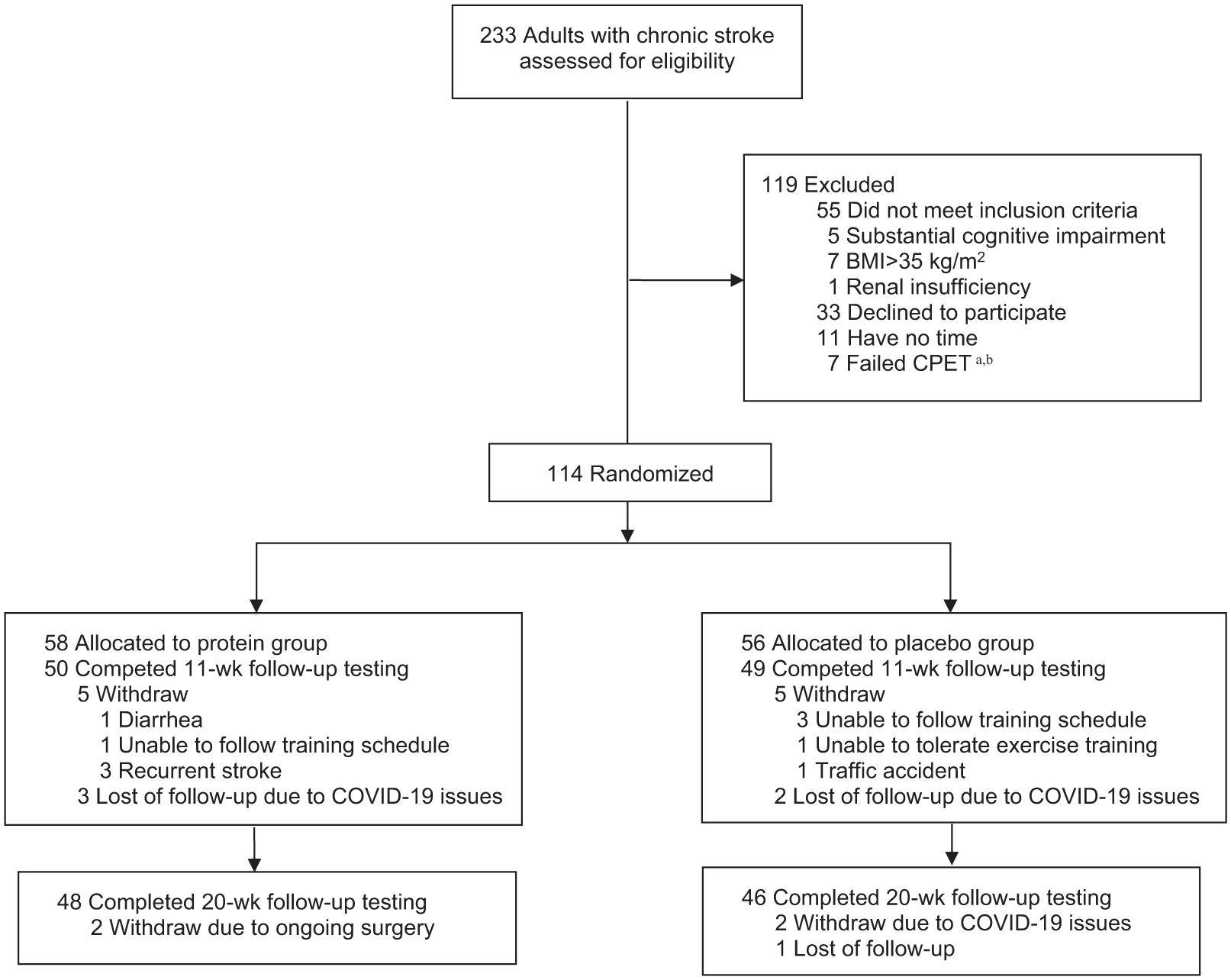
Flow of participants through the INSPIRE trial. INSPIRE indicates Incorporating Supplementary Protein into Rehabilitative Exercise.
Basic characteristics
The basic information of the participants is summarized in Table 1. Most participants were mildly disabled after stroke, with 79 (69.6%) having a modified Rankin Scale of 1 and 2. Fifty-six (49.1%) had a Mini Nutritional Assessment (long-form) score below 23.5, indicating some risk of malnutrition; but none had a score below 17, indicating malnutrition. On average, participants had a daily oral protein intake of 1.0 g/kg. At baseline, the mean V̇O2peak was 17.5 mL/kg/min, corresponding to 67.6% of the expected value in the healthy population.
Participant characteristics.
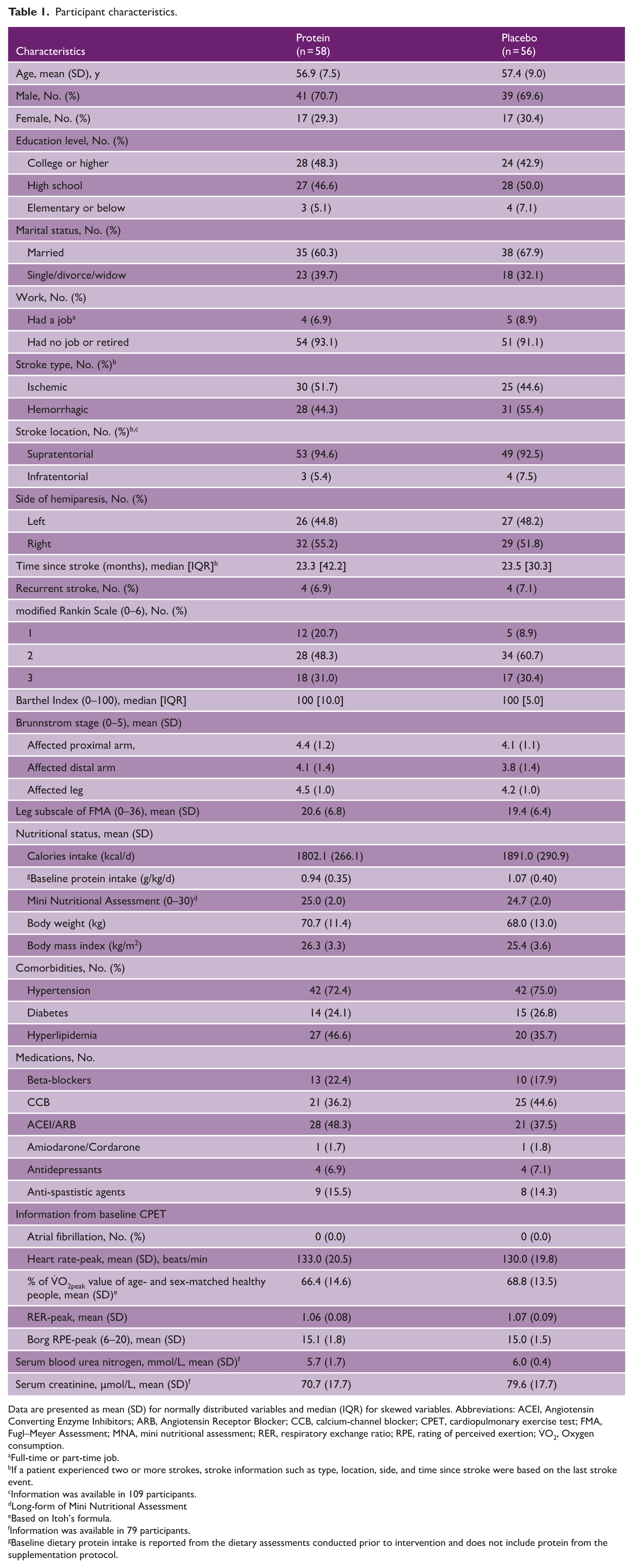
Data are presented as mean (SD) for normally distributed variables and median (IQR) for skewed variables. Abbreviations: ACEI, Angiotensin Converting Enzyme Inhibitors; ARB, Angiotensin Receptor Blocker; CCB, calcium-channel blocker; CPET, cardiopulmonary exercise test; FMA, Fugl–Meyer Assessment; MNA, mini nutritional assessment; RER, respiratory exchange ratio; RPE, rating of perceived exertion; V̇O2, Oxygen consumption.
Full-time or part-time job.
If a patient experienced two or more strokes, stroke information such as type, location, side, and time since stroke were based on the last stroke event.
Information was available in 109 participants.
Long-form of Mini Nutritional Assessment
Based on Itoh’s formula.
Information was available in 79 participants.
Baseline dietary protein intake is reported from the dietary assessments conducted prior to intervention and does not include protein from the supplementation protocol.
Primary outcome
Among the 94 participants who completed the 11-week follow-up, the V̇O2peak significantly increased by 1.7 mL/kg/min (95% CI: 1.0 to 2.4) and 1.6 mL/kg/min (95% CI: 0.9 to 2.3) from baseline in the protein supplementation and placebo groups respectively (Table 2, eTable 1, and eFigure 1 in Supplement 2). The individual change values at the 11-week follow-up in relation to the baseline values of V̇O2peak are shown in Figure 2. There was no significant between-group difference regarding the V̇O2peak changes (p = 0.43) (Table 2). No between-group differences were observed in the analyses stratified by sex, age, stroke type, and baseline performance or body composition outcomes (eFigure 2 in Supplement 2).
Effects of protein supplementation on primary and secondary outcomes.
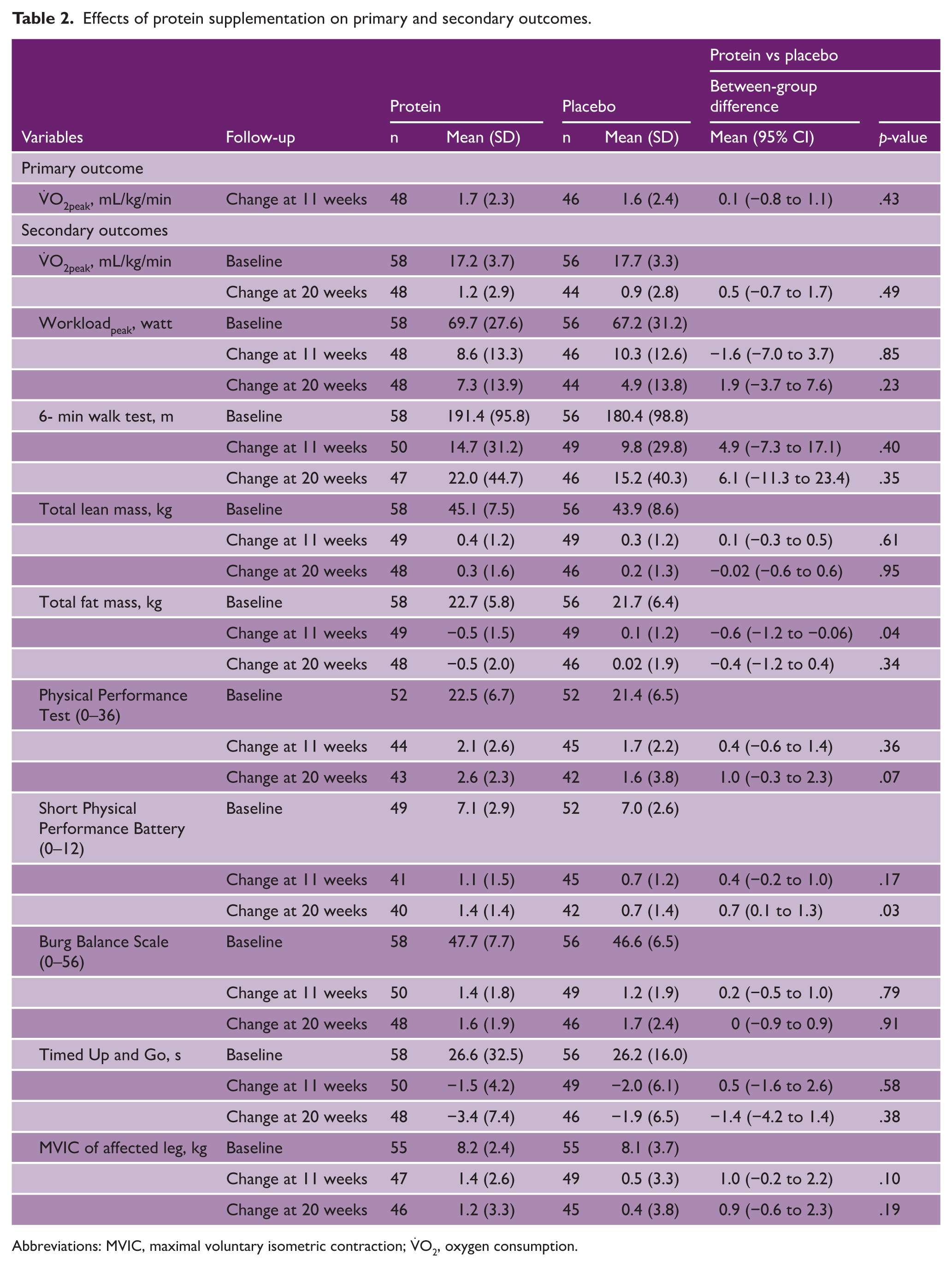
Abbreviations: MVIC, maximal voluntary isometric contraction; V̇O2, oxygen consumption.
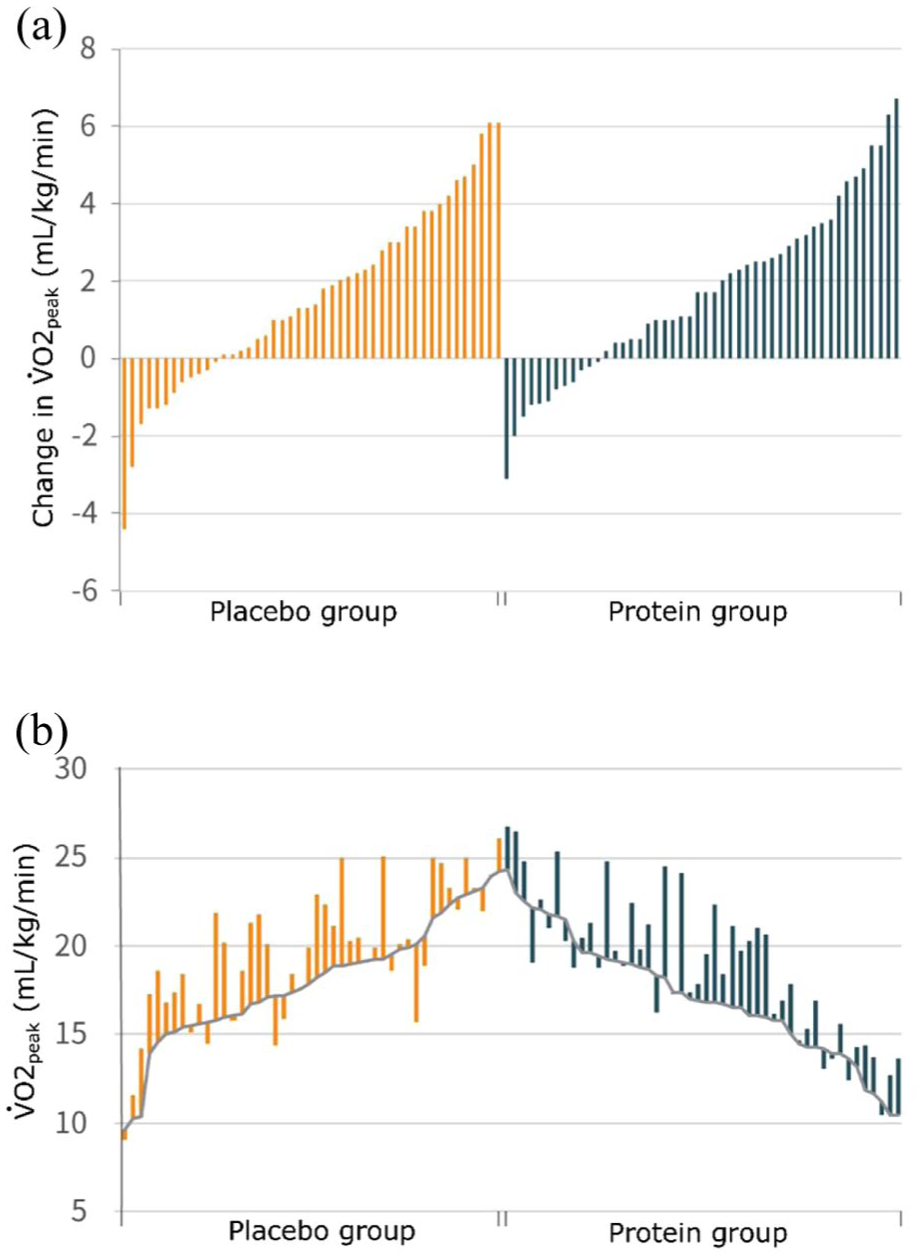
Changes from baseline in V̇O2peak. a. Every vertical bar symbolizes an individual participant, arranged based on their baseline measurement, and the vertical bar extends upward (improvement) or downward (decline) to the measurement at 11 weeks. b. Vertical lines ascending indicate the extent of enhancement in V̇O2peak during the 11-week follow-up, while descending vertical lines indicate the degree of decrease in V̇O2peak.
Secondary outcomes
At the 11-week follow-up, the protein group showed a statistically significant within-group increase in total lean mass (0.4 kg, 95% CI: 0.05 to 0.7), total fat mass reduction (−0.5 kg, 95% CI: −1.0 to −0.1), and improvement in muscle strength of the affected leg (1.4 kg, 95% CI: 0.6 to 2.1). Both groups developed statistically significant improvements in workloadpeak, 6 min walk test, Physical Performance Test, SPPB, Berg Balance Scale, and Timed Up-and-Go test. (eTable 1 in Supplement 2)
At the 20-week follow-up, the protein group showed a statistically significant within-group improvement in the V̇O2peak (1.2 mL/kg/min, 95% CI: 0.3 to 2.0) and muscle strength of the affected leg (1.2 kg, 95% CI: 0.2 to 2.2). Both groups developed significant improvements in workloadpeak, 6 min walk test, Physical Performance Test, SPPB, Berg Balance Scale, and Timed Up and Go test. (eTable 1 in Supplement 2)
The protein group demonstrated enhanced physical performance compared to the placebo group at the 20 week, as indicated by SPPB scores (mean difference between groups: 0.7 (95% CI: 0.1 to 1.3); p = 0.03). In addition, the protein group exhibited lower total fat mass relative to the placebo group at 11 weeks (mean difference between groups: −0.6 (95% CI: −1.2 to −0.06); p = 0.04) (Table 2). The protein group showed within-group improvements from baseline to both 11 weeks (mean increase of 1.1, 95% CI: 0.6 to 1.6, p < 0.001) and 20 weeks (mean increase of 1.4, 95% CI: 0.9 to 1.8, p < 0.001), respectively. The placebo group demonstrated within-group improvements from baseline to 11 weeks (mean increase of 0.7, 95% CI: 0.3 to 1.1, p < 0.001) and 20 weeks (mean increase of 0.7, 95% CI: 0.2 to 1.1, p = 0.003) (eTable 1 in Supplement 2).
Among the 106 patients who completed the intervention, 90 (84.9%) attended all 30 sessions. Among a total of 3117 sessions attended, 1826 (58.6%) achieved the target heart rate. No significant between-group differences were found in the number of sessions attended, the number of sessions in which the target heart rate was achieved, and the number of concurrent rehabilitation sessions based on their protein supplementation status. As for severe adverse events, three participants in the protein group experienced recurrent stroke during the study period. No significant between-group difference regarding the proportion of recurrent stroke was found (3 of 58 in the protein supplementation group vs 0 of 56 in the placebo group; p = 0.085) (eTable 2 in Supplement 2).
Discussion
Interpretation
The present study was designed to determine the impact of protein supplementation on CRF and physical performance adaptation to aerobic-dominant training in patients with chronic stroke. Both groups showed significant improvements in most CRF-related outcomes and physical performance measures after 10 weeks of aerobic-dominant training. While protein supplementation did not further enhance V̇O2peak, the protein group demonstrated significantly greater improvement in physical performance, as measured by the Short Physical Performance Battery, and a lower fat mass compared to the placebo group.
Prolonged exercise enhances muscle protein breakdown and stimulates an increase in amino acid oxidation, 26 while protein supplementation potentially enhances post-exercise muscle protein synthesis and inhibits muscle protein breakdown. 8 Whether protein supplementation elicits greater improvements in CRF remains unclear. The available evidence is inconclusive and diverse. A recent review, concentrating on the impact of protein supplementation on athletic performance, found no noticeable effect on concurrent training-induced enhancements in V̇O2peak among healthy adults. 10 By contrast, in a recent meta-analysis involving 19 trials, it was observed that protein supplementation, when compared to placebo, led to an additional increase of 0.89 mL/kg/min in V̇O2peak during concurrent aerobic training. 11 However, this outcome was derived from trials encompassing a varied population, with only two trials specifically addressing stroke patients.12,27
In the current trial, while improvements in cardiorespiratory fitness were present in both groups, there was no meaningful between-group difference in V̇O2peak. This finding may be explained by several factors. First, our cohort’s relatively adequate baseline protein intake (averaging 1.0 g/kg/day) may have blunted the potential effect of supplementation. Second, while our 10-week intervention was based on a successful pilot study, a longer duration may be necessary to elicit significant changes in cardiorespiratory fitness. 28 Despite this result for the primary outcome, the SPPB scores improved to a greater extent in the protein group compared to placebo. The improvement in the SPPB score for the protein group exceeded the large clinically meaningful difference of 1 point29,30 at 11 weeks and was able to maintain this clinically meaningful improvement over the 20-week period. In contrast, the placebo group experienced a smaller improvement that did not reach the large clinically meaningful difference threshold. The between-group differences in SPPB score changes were also clinically meaningful, exceeding the clinically meaningful difference of 0.5 points. 29 Regarding other functional outcomes, the within-group changes provide context on the overall effect of the exercise program. For instance, at 11 weeks, the mean improvements in the 6-min walk test did not meet the established minimal clinically important difference (MCID) of 34–44 m. 31 Similarly, gains on the Berg Balance Scale were also below the reported MCID of 4–5 points, 32 suggesting these improvements were modest. This pattern suggests that while the 10-week aerobic-dominant training program was broadly beneficial for mobility, a clinically significant advantage from protein supplementation was most clearly detected by the multi-component SPPB. This finding is compatible with prior studies suggesting that the SPPB may be a particularly sensitive measure for detecting changes in functional progression after stroke compared to other secondary outcomes.22,33
In addition to the improvement in SPPB scores, the protein group also showed a lower fat mass compared to the placebo group, with no significant change in muscle mass. This reduction in fat mass might suggest that protein supplementation could help preserve lean body mass while reducing fat. The potential mechanisms could involve protein’s role in enhancing fat oxidation during exercise or its effects on satiety and energy expenditure, leading to a more favorable body composition overall, although further research is needed to further elucidate these effects.
While our findings may not align with initial expectations that protein supplementation would significantly enhance stroke patients’ CRF when combined with exercise training, a potential benefit of protein supplementation for improving functional mobility and body composition was observed. The field of sports nutrition has evolved significantly, with a notable increase in the use of various nutritional supplements during exercise routines. Conversely, the use of nutritional supplements in the rehabilitation of cardiovascular conditions, including stroke, remains relatively underexplored. Since rehabilitation programs for stroke patients often incorporate exercise to improve cardiovascular health and overall physical function, the potential to enhance these outcomes with nutritional supplements warrants further investigation. Results from the current study also suggest that the SPPB may serve as a sensitive tool for detecting changes in physical performance in future studies investigating the effects of nutritional supplementation on stroke patients undergoing exercise training. Future studies may also consider selectively enrolling protein-deficient participants who may derive greater benefit from supplementation, as having a broader range of baseline protein intakes could have diluted the average treatment effect across the full cohort. Furthermore, our trial focused specifically on the effects of a timed, peri-exercise supplement to test a hypothesis related to nutrient timing; an alternative approach for future research would be to evaluate a more comprehensive dietary regimen designed to increase total daily protein intake, which may elicit different or more pronounced benefits on functional outcomes and body composition in this population. Finally, investigating interventions of a longer duration would be valuable to determine if more substantial benefits emerge over an extended period.
Strengths and limitations
This study’s strengths include its multicenter, participant- and assessor-blinded, randomized clinical trial design. It also features a relatively large sample size for stroke RCT research. In addition, the study conducted a comprehensive assessment of multiple outcomes, providing a well-rounded evaluation of the intervention’s effects. Moreover, despite the challenges of the COVID-19 era, the trial achieved high compliance and maintained a low dropout rate, further supporting the reliability of the results. This study also had several limitations. First, dietary assessments were not repeated during or after the training period to investigate possible changes in dietary habits over time. Second, the trial enrolled participants with relatively milder disabilities and independent in mobility, which may limit the generalizability when applied to stroke patients with severe disabilities. Third, the age range of our participants (20–75 years, with a mean of 57.2 years) limits the generalizability of our findings to older stroke survivors (e.g. >75 years old), who may have different metabolic needs and responses to intervention. Fourth, concurrent rehabilitation was allowed, which might have obscured the effects of protein supplementation. Finally, our study focused on patients with chronic stroke. While this limits the generalizability of our findings to the subacute phase, this specific population was chosen to minimize the confounding effects of spontaneous neurological recovery and to better isolate the impact of the training and supplementation intervention.
Conclusions
Protein supplementation did not further improve cardiorespiratory fitness following aerobic-dominant training in patients with chronic stroke. Further investigations targeting specific subpopulations, such as individuals with baseline protein deficiency, may provide insights into the differential effects of protein supplementation on outcomes in stroke patients.
Supplemental Material
sj-docx-1-wso-10.1177_17474930251403727 – Supplemental material for Effect of protein supplementation on cardiorespiratory fitness with aerobic training in chronic stroke: A multicenter randomized controlled trial
Supplemental material, sj-docx-1-wso-10.1177_17474930251403727 for Effect of protein supplementation on cardiorespiratory fitness with aerobic training in chronic stroke: A multicenter randomized controlled trial by Yen-Nung Lin, Anand Viswanathan, Elisa F. Ogawa, Pim Knuiman, Chin-Hao Chang, Wing P. Chan, Shih-Wei Huang, Jeffrey C. Schneider, Jonathan F. Bean and Tian-Shin Yeh in International Journal of Stroke
Supplemental Material
sj-docx-2-wso-10.1177_17474930251403727 – Supplemental material for Effect of protein supplementation on cardiorespiratory fitness with aerobic training in chronic stroke: A multicenter randomized controlled trial
Supplemental material, sj-docx-2-wso-10.1177_17474930251403727 for Effect of protein supplementation on cardiorespiratory fitness with aerobic training in chronic stroke: A multicenter randomized controlled trial by Yen-Nung Lin, Anand Viswanathan, Elisa F. Ogawa, Pim Knuiman, Chin-Hao Chang, Wing P. Chan, Shih-Wei Huang, Jeffrey C. Schneider, Jonathan F. Bean and Tian-Shin Yeh in International Journal of Stroke
Footnotes
Author contributions
Dr YNL and TSY act as guarantors of the study, they had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Concept and design: YNL, AV, EFO, PK, CHC, WPC, LW, JCS, JFB, and TSY.
Acquisition, analysis, or interpretation of data: YNL, AV, EFO, PK, CHC, WPC, JCS, JFB, and TSY.
Drafting of the manuscript: YNL, AV, EFO, PK, WPC, JCS, JFB, and TSY
Critical revision of the manuscript for important intellectual content: All authors.
Statistical analysis: CHC and TSY.
Obtained funding: YNL and TSY.
Administrative, technical, or material support: WPC, LW, JYS, YSH, SWH, and LFL.
Supervision: YNL, AV, JCS, JFB, and TSY.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funded by grant 107-2320-B-038-016, 109-2314-B-038-046 from the National Science and Technology Council (Taiwan) (YNL); grant number NSTC 114-2314-B-038-021 from the National Science and Technology Council (Taiwan) (TSY); grant number TMU111-AE1-B24 from Taipei Medical University (TSY); Supported by the Wan Fang Hospital and Taipei Medical University.
Role of the funder/sponsor
The National Science and Technology Council, Wan Fang Hospital, and Taipei Medical University had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Data availability statement
Data will be made available upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.