
Abstract
Background:
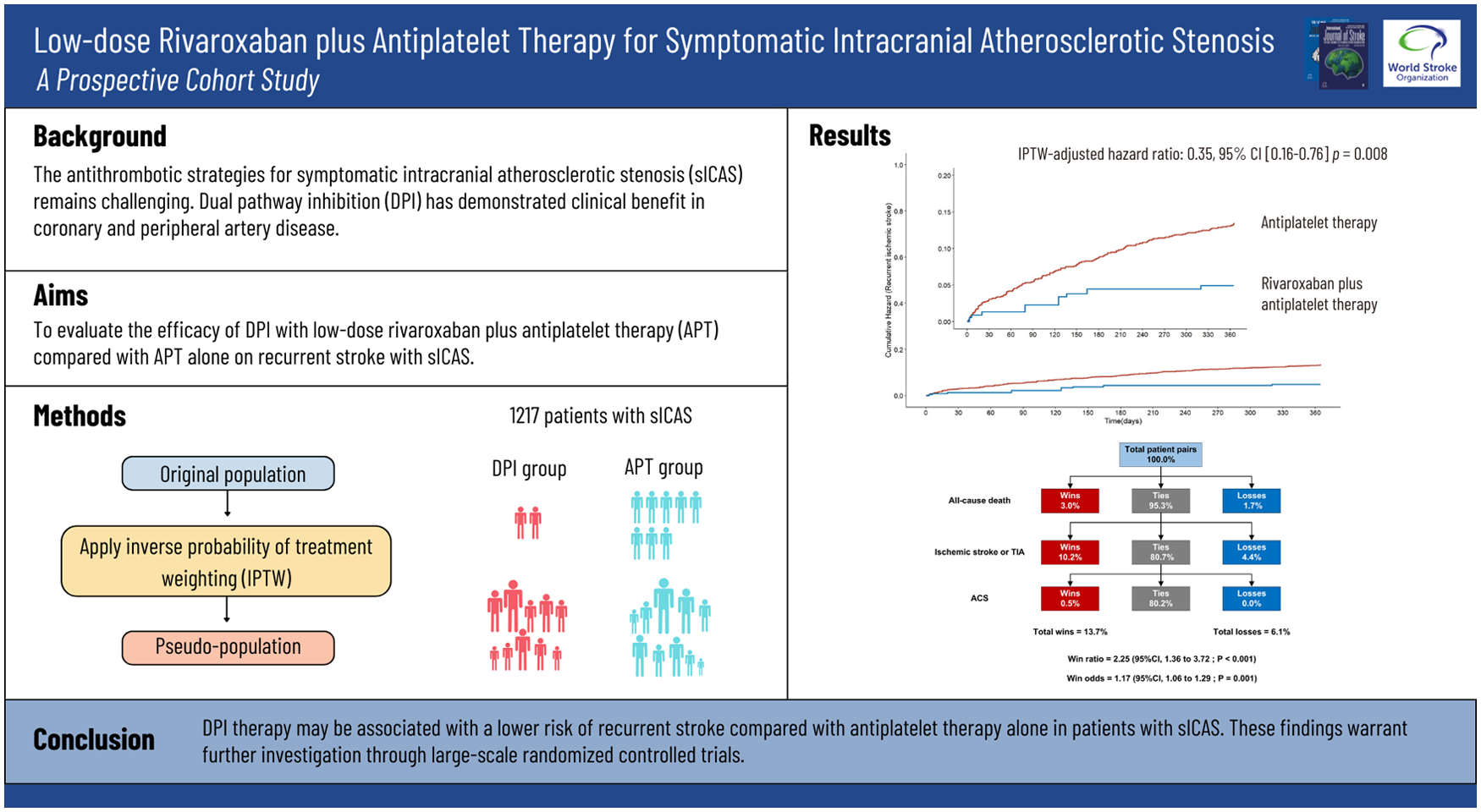
The antithrombotic strategies for symptomatic intracranial atherosclerotic stenosis (sICAS) remains challenging. Dual pathway inhibition (DPI) has demonstrated clinical benefit in coronary and peripheral artery disease.
Aims:
This study aimed to evaluate the efficacy of DPI with low-dose rivaroxaban plus antiplatelet therapy (APT) compared with APT alone on recurrent stroke with sICAS.
Methods:
This prospective cohort study included patients with sICAS identified from the Ischemic Cerebrovascular Disease Database of the First Affiliated Hospital of Zhengzhou University between January 2019 to August 2023. Low-dose rivaroxaban was prescribed off-label to patients in the DPI group. The outcomes were ischemic stroke, transient ischemic attack (TIA), acute coronary syndrome (ACS), all-cause death and cardio-cerebrovascular death within 1 year of discharge. Cox regression with inverse probability of treatment weighting (IPTW) was applied to compare outcomes between the DPI and APT groups. The win-ratio method was used to assess the major adverse cardiovascular events (MACE), prioritized in the order of all-cause death, recurrent ischemic stroke or TIA, and ACS.
Results:
Among the 1217 patients with sICAS, 131 (10.8%) received DPI therapy. The recurrence rate of ischemic stroke was lower in the DPI group compared to the APT group (8/131 [6.1%] vs 136/1086 [12.5%]). DPI significantly reduced the risk of ischemic stroke recurrence (HR = 0.46, 95% CI: 0.23–0.94, p = 0.034) and the incidence of MACE (HR = 0.53, 95% CI: 0.29–0.97, p = 0.041) during the 1-year follow-up, consistent with the IPTW-based cohort (HR = 0.35, 95% CI: 0.16–0.76, p = 0.008; HR = 0.43, 95% CI: 0.22–0.83, p = 0.012). The win-ratio analysis of MACE favored DPI therapy (win ratio = 2.34, 95% CI: 1.41–3.90, p = 0.001). Symptomatic intracranial hemorrhage, fatal bleeding, and hospitalization for gastrointestinal bleeding were infrequent in this cohort.
Conclusions:
DPI therapy may be associated with a lower risk of recurrent stroke compared with antiplatelet therapy alone in patients with sICAS. These findings warrant further investigation through large-scale randomized controlled trials.
Keywords
Introduction
Intracranial atherosclerotic stenosis (ICAS) is a major cause of ischemic stroke in Asian populations and has long been associated with a high risk of recurrent stroke. 1 The antithrombotic strategies for symptomatic intracranial atherosclerotic stenosis (sICAS) lack uniformity, although dual antiplatelet therapy (DAPT) for 90 days post-onset is commonly favored in clinical practice,2,3 its efficacy has not yet been validated by randomized controlled trials.
The SAMMPRIS (Stenting and Aggressive Medical Management for Preventing Recurrent Stroke in Intracranial Stenosis) trial and the VISSIT (Vitesse Intracranial Stent Study for Ischemic Stroke Therapy) trial demonstrated that despite strict medical management, patients with sICAS still had a high recurrence rate of 12.2% and 15.1% within 1 year.4,5 Although the efficacy of medical treatment has significantly improved in recent years, the CASSISS (China Angioplasty and Stenting for Symptomatic Intracranial Severe Stenosis) study indicates that the risk of stroke recurrence or death within 1 year of medical treatment remains at 7.2%, and the risk of stroke in the same territory reaches 11.2% within 3 years. 6 Therefore, more effective antithrombotic strategies are needed to prevent stroke recurrence.
Rivaroxaban is an oral direct Factor Xa inhibitor that binds competitively to the active site of serine protease, preventing substrate binding and subsequently inhibiting the generation of thrombin and the formation of fibrin. In the COMPASS (Cardiovascular Outcomes for People Using Anticoagulation Strategies) trial, the combination of low-dose rivaroxaban (2.5 mg) and aspirin had better cardiovascular outcomes in patients with stable atherosclerotic vascular disease. 7 The stroke outcomes of the COMPASS trial indicated that dual pathway inhibition (DPI) therapy reduced the incidence of fatal and disabling strokes by nearly half compared to aspirin monotherapy. 8 These findings suggest the potential value of combining antiplatelet therapy with low-dose oral anticoagulants in stroke prevention.
In this study, we aimed to investigate the efficacy of DPI therapy versus antiplatelet therapy (APT) alone in preventing recurrent ischemic stroke in a prospective cohort of patients with sICAS.
Methods
Study design and participants
This was a prospective cohort study based on the Ischemic Cerebrovascular Disease Database of the First Affiliated Hospital of Zhengzhou University, details of the database and related studies have been published in previous works.9,10 We included patients from January 1, 2019 through August 31, 2023 fulfilling the following criteria: (1) age ⩾ 18 years; (2) diagnosed with acute ischemic stroke (AIS) within the past 7 days, attributed to intracranial atherosclerotic stenosis in the corresponding vascular territory, as confirmed by computed tomographic angiography (CTA) or magnetic resonance angiography (MRA).11,12 The exclusion criteria were as follows: (1) modified Rankin Scale (mRS) > 4 at discharge; (2) with ipsilateral moderate to severe (⩾50%) extracranial atherosclerotic stenosis; (3) received or planned to undergo stenting, angioplasty, or endarterectomy of an extracranial (carotid or vertebral artery) or intracranial artery; (4) co-morbid conditions requiring standardized anticoagulation therapy; and (5) not receiving antithrombotic therapy due to a combined contraindication to antiplatelet therapy or anticoagulation. This study is reported in accordance with the STROBE guidelines (Strengthening the Reporting of Observational Studies in Epidemiology). 13
Ethics statement
The study protocol was approved by the Ethics Committee of the First Affiliated Hospital of Zhengzhou University (approval number: 2009-KY-05). Written informed consent was obtained from the participants and their families for the publication of any information included in this article.
Data collection
Baseline characteristics such as demographics, medical history, clinical and laboratory characteristics, stroke characteristics, medication prescriptions were collected from the Ischemic Cerebrovascular Disease Database of the First Affiliated Hospital of Zhengzhou University. The stroke cause and location of stenotic artery were determined independently by two neurologists based on the Trial of ORG 10172 in Acute Stroke Treatment (TOAST) classification, 14 and conflicts in the classification were resolved by consulting another senior neurologist. Although some patients had concomitant atrial fibrillation, they were categorized as having large-artery atherosclerosis when the dominant stroke mechanism was adjudicated as atherosclerotic rather than cardioembolic. ICAS was defined as the presence of more than 50% stenosis or occlusion in the following arterial segments: the intracranial portion of the internal carotid arteries or vertebral arteries, and the proximal anterior, middle, or posterior cerebral arteries, or the basilar artery. 15 Intracranial stenosis was assessed using CTA or MRA among the included patients. Degree of culprit vessel stenosis was calculated using the published method for the Warfarin-Aspirin Symptomatic Intracranial Disease Study (WASID): percent stenosis =[(1 − (Dstenosis/Dnormal))] × 100. 16
Primary exposure
Exposure was defined based on treatment allocation at discharge, which served as the starting point for subsequent follow-up. The primary exposure was the antithrombotic regimen used and categorized into APT group and DPI group. In the DPI group, low-dose rivaroxaban (2.5 mg twice daily) was prescribed off-label in combination with aspirin (100 mg once daily) or clopidogrel (75 mg once daily) at discharge and continued this regimen long-term, regardless of the antithrombotic therapy previously used. APT group included antiplatelet monotherapy (aspirin, clopidogrel, or ticagrelor) and dual antiplatelet therapy (combination of aspirin, clopidogrel, or ticagrelor, continued for at least 21 days, followed by antiplatelet monotherapy).
Follow-up and outcomes
Patients were followed-up at 3 months, 6 months, and 1 year after discharge by face-to-face or telephone interviews to determine whether any events had occurred. Clinical follow-up for outcome assessment began at discharge, and events occurring prior to discharge were not counted as follow-up outcomes. Clinical outcome events were adjudicated based on clinical records, relevant imaging findings when available, and follow-up documentation. The primary outcome was a recurrent ischemic stroke during follow-up. Recurrent stroke is defined as a new neurological event occurring after a previous stroke, lasting at least 24 h, or <24 h but accompanied by imaging evidence of new or enlarging acute infarction.
The secondary efficacy outcomes included major adverse cardiovascular events (MACE), defined as a composite of all-cause death, stroke or transient ischemic attack (TIA), and acute coronary syndrome (ACS), as well as individual components such as TIA, ACS, all-cause death, and cardio-cerebrovascular death.
Statistical analysis
The baseline variables in the DPI group and antiplatelet group were compared using the Kruskal–Wallis test for continuous variables and the χ2 test for categorical variables.
A propensity score approach was employed to mitigate allocation biases arising from the lack of randomization in treatment assignment. 17 Propensity scores were estimated using a multivariable logistic regression model, with treatment assignment as the dependent variable. Covariates included in the propensity score model were age, sex, smoking status, drinking status, qualifying event, hypertension, diabetes, dyslipidemia, prior stroke or TIA, coronary heart disease, heart failure, renal disease, location of stenotic artery, degree of culprit vessel stenosis, and baseline NIHSS score. Inverse probability of treatment weighting (IPTW) was applied to create a pseudo-population by using the estimated propensity score, with weights derived as the inverse of the probability of receiving the actual treatment or exposure that the subject received. Non-stabilized weights were used, and no truncation of extreme weights was performed. A standardized mean difference (SMD) ⩽ 0.10 indicated balanced covariates.
Hazard ratios and corresponding 95% confidence intervals were derived from robust Cox proportional-hazards models. Time-to-event was defined as the time from hospital discharge to the first occurrence of the outcome of interest or censoring at 1 year. Kaplan-Meier estimates were used to assess the cumulative risk of event occurrence across the two antithrombotic treatment groups in the IPTW-based cohort.
A win-ratio analysis was conducted to evaluate the impact of dual pathway inhibition on the prevention of composite vascular endpoint events in the IPTW-based cohort. The win ratio approach can incorporate benefits and risks into a hierarchy of outcomes based on clinical importance to assess superiority between treatment groups.18,19 A win ratio that exceeds 1.00 reflects a better outcome. The hierarchical composite endpoint included (1) all-cause death, (2) ischemic stroke or transient ischemic attack or (3) acute coronary syndrome.
All analyses were conducted in R version 4.4.1 (R Foundation for Statistical Computing, Vienna, Austria) or SPSS version 26.0 (IBM Corp., Armonk, NY, USA). All reported P values are two-sided, P values of 0.05 or less were considered statistically significant.
Results
Study population
A total of 1825 patients meeting the inclusion criteria were classified as sICAS. Among the 1217 patients included in the final analysis, 1086 (89.2%) were on antiplatelet medications and 131 (10.8%) on low-dose rivaroxaban plus antiplatelet medication. The flowchart of enrollment and treatment is shown in Figure 1.
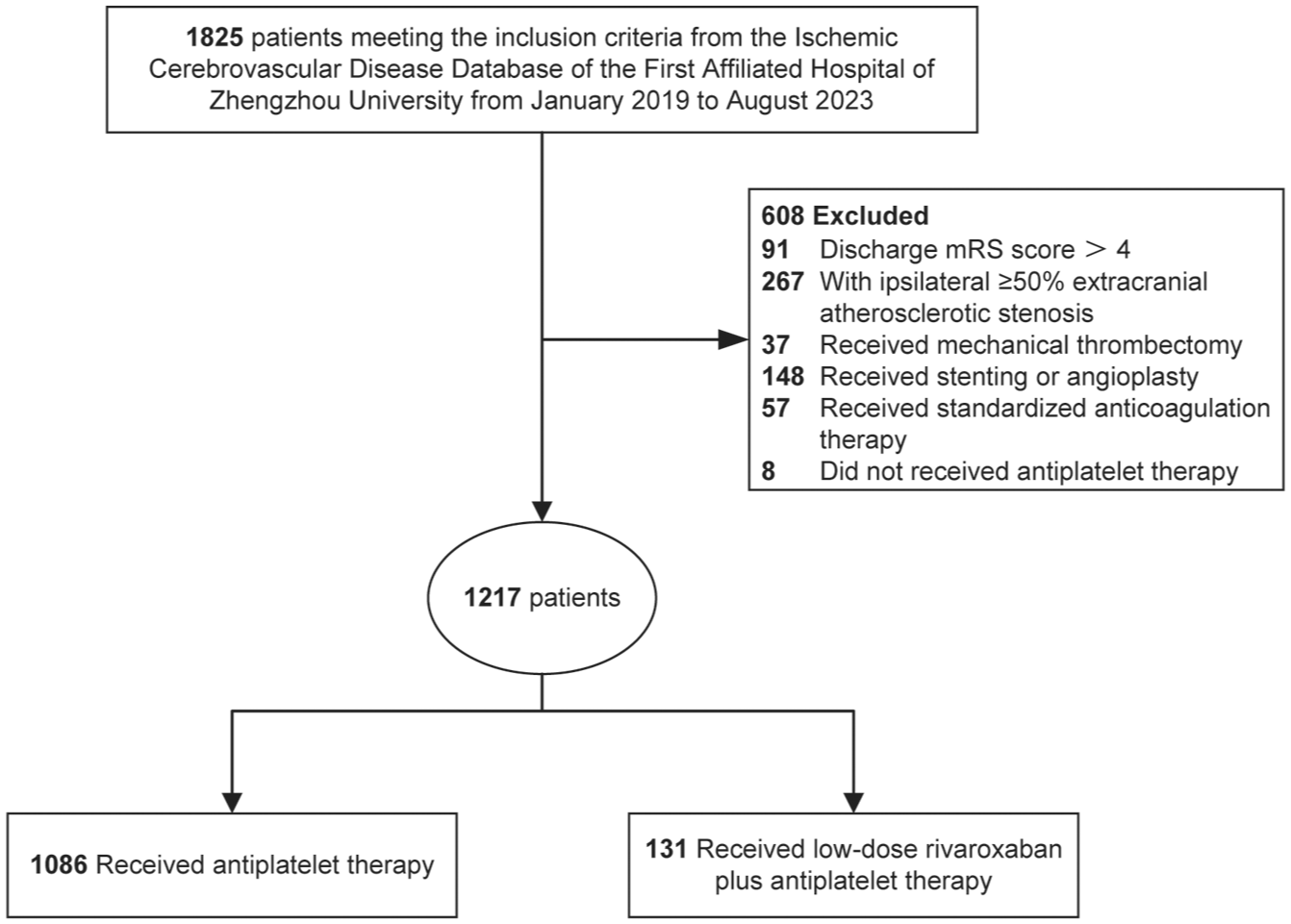
Flowchart of enrollment and treatment.
The mean age was 60.2 years in the APT group and 61.1 years in the DPI group (SMD 0.071). Low-dose rivaroxaban was initiated at a mean time of 12.3 days (±6.4 days) after ischemic stroke or TIA (Supplementary Table 1). Prior stroke or TIA was more common in the DPI group (47.3% vs 27.5%, p < 0.001). Upon adjustment by IPTW, patient characteristics were well balanced (Table 1).
Baseline characteristics before and after adjustment with inverse probability of treatment weighting.
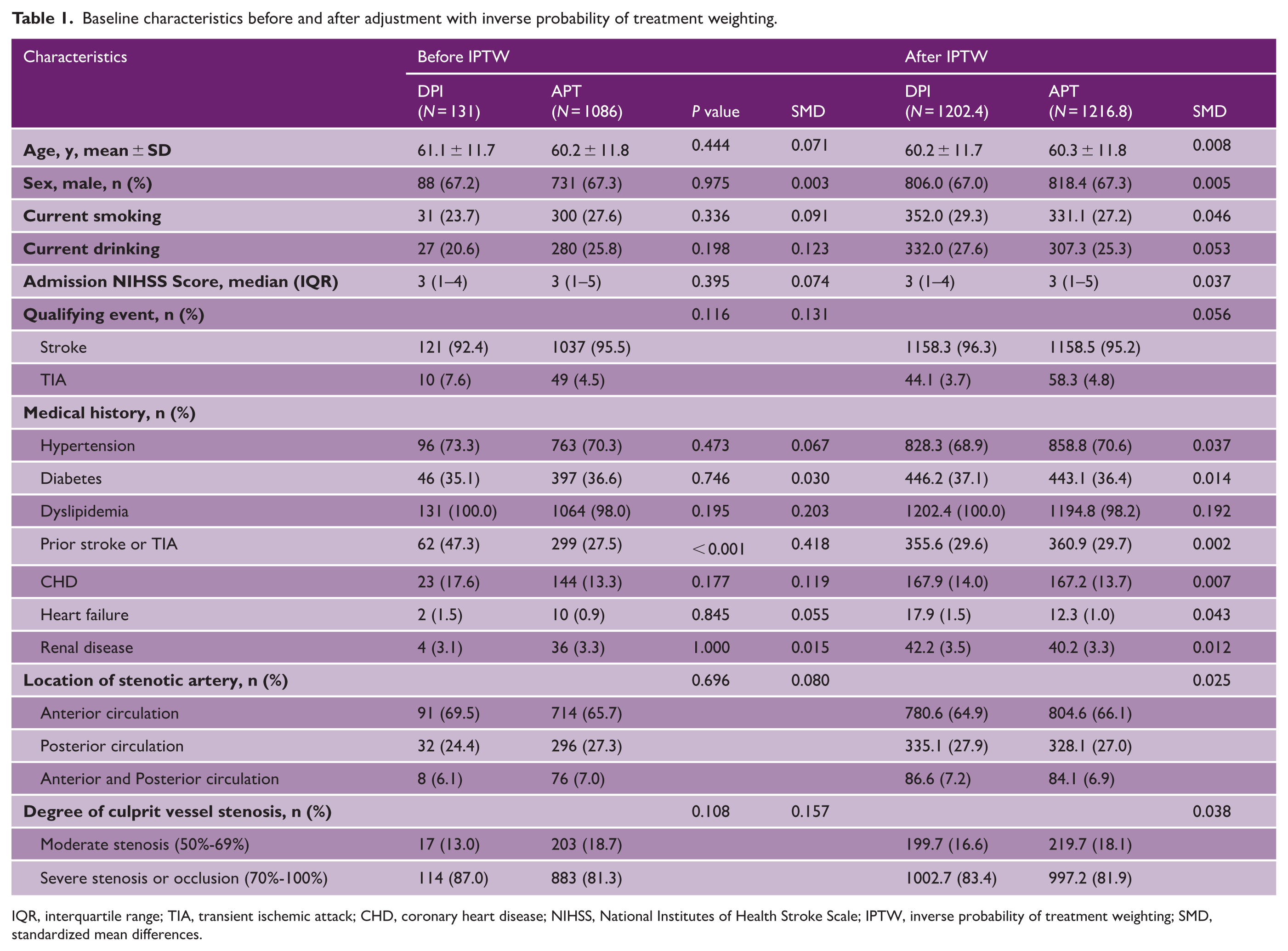
IQR, interquartile range; TIA, transient ischemic attack; CHD, coronary heart disease; NIHSS, National Institutes of Health Stroke Scale; IPTW, inverse probability of treatment weighting; SMD, standardized mean differences.
Association between antithrombotic strategies and clinical outcomes
During the 1-year follow-up, the rate of recurrent stroke was 6.1% in DPI group and 12.5% in APT group, and the hazard ratio for ischemic stroke was 0.46 (95% CI: 0.23–0.94, p = 0.034). After balancing baseline characteristics, the similar results were observed, with a hazard ratio of 0.35 (95% CI: 0.16–0.76, p = 0.008) in the IPTW-based cohort. In addition, the occurrence of MACE was less frequent in the DPI group in the unmatched cohort (11/131, 8.4% versus 162/1086, 14.9%; HR = 0.53, 95% CI: 0.29–0.97, p = 0.041), as well as in the IPTW-based cohort (HR = 0.43, 95% CI: 0.22–0.83, p = 0.012) (Table 2). Kaplan-Meier curves illustrate that DPI significantly reduced the cumulative incidence of both recurrent ischemic stroke and MACE compared with antiplatelet therapy alone in the IPTW-based cohort (Figure 2).
Efficacy and safety outcomes in study population.
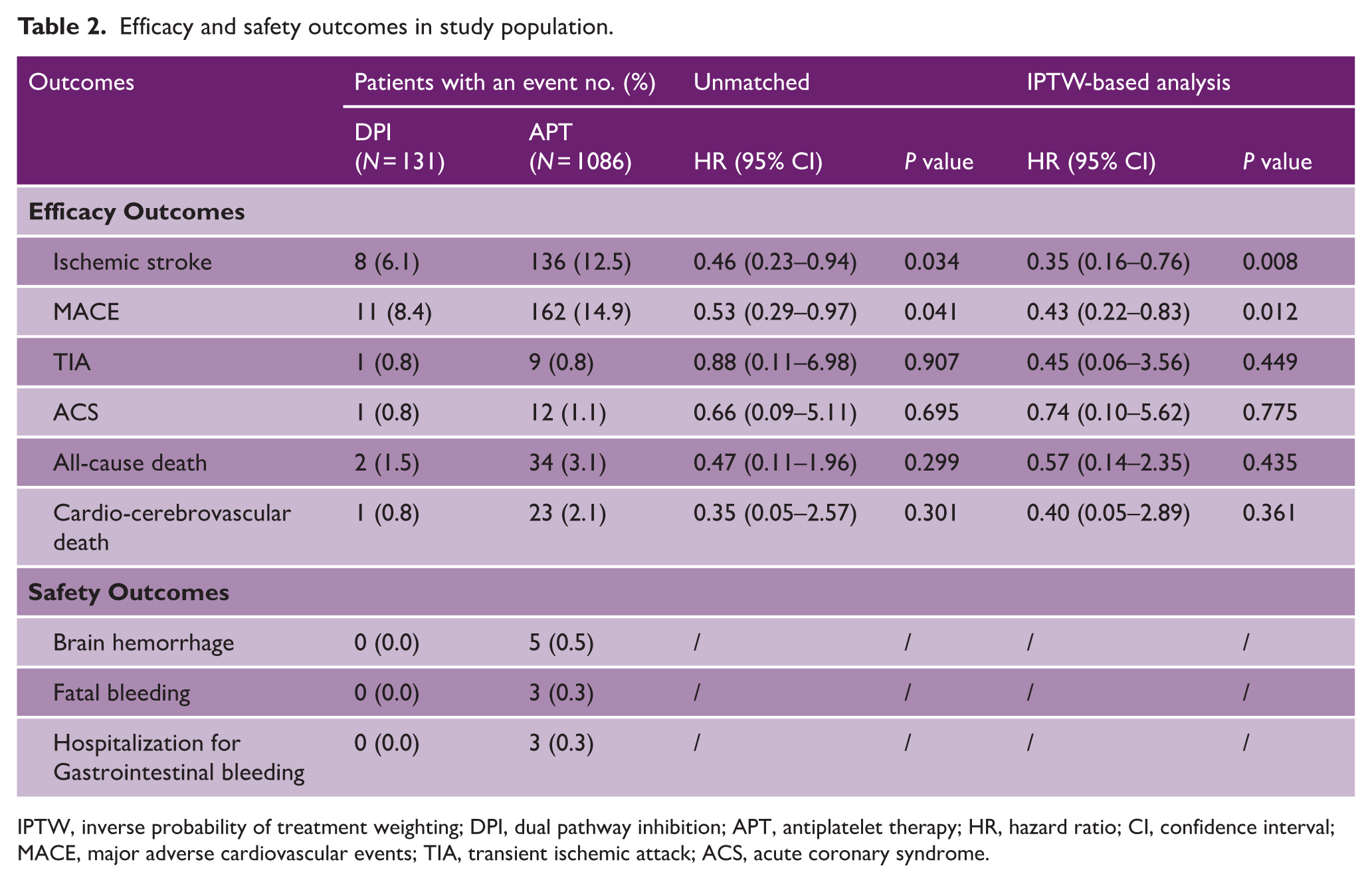
IPTW, inverse probability of treatment weighting; DPI, dual pathway inhibition; APT, antiplatelet therapy; HR, hazard ratio; CI, confidence interval; MACE, major adverse cardiovascular events; TIA, transient ischemic attack; ACS, acute coronary syndrome.
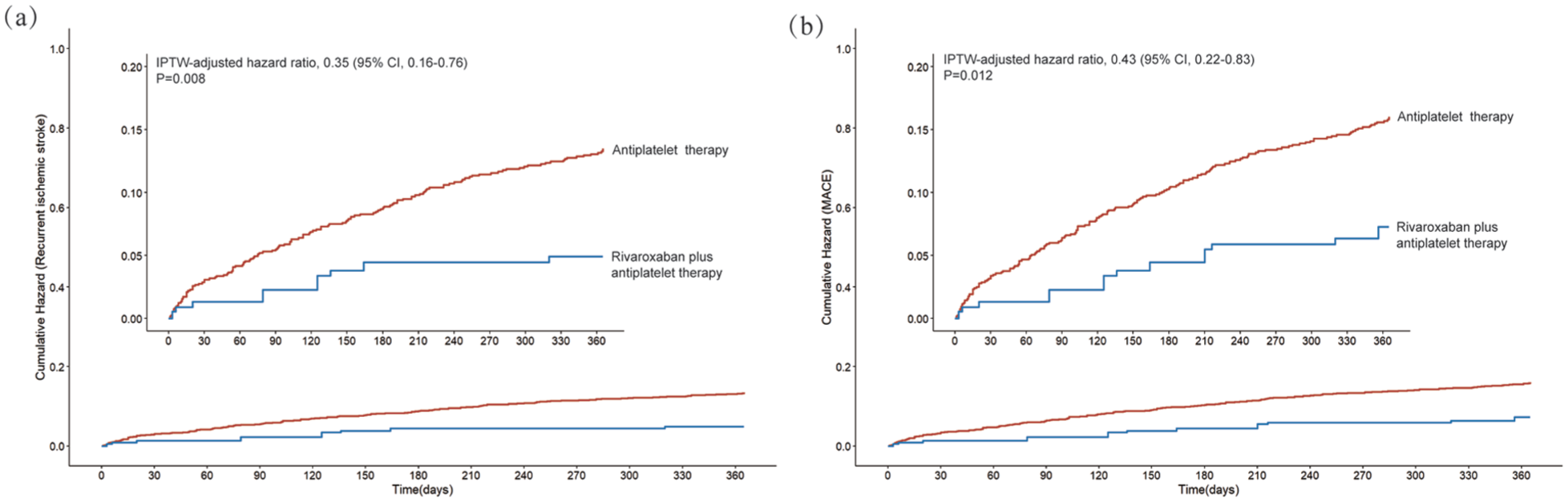
Cumulative incidence of recurrent ischemic stroke (a) and MACE (b) in the IPTW-based cohort.
Moreover, the win ratio analysis was applied to evaluate composite endpoint in the IPTW cohort (Figure 3). The composite prioritized mortality as the most severe outcome, followed by cerebrovascular events (relapse), and finally cardiovascular events. In the comparison, DPI demonstrated wins in 13.7% of paired comparisons, antiplatelet alone exhibited wins in 6.1%, and a tie occurred in 80.2% of comparisons. DPI displayed a consistent numerical treatment benefit across all components of the clinical hierarchy, with a win ratio of 2.25 (95% CI, 1.36–3.72, p < 0.001). Of the three components in the win ratio, the ischemic stroke or TIA pairwise comparisons yielded both the highest ratio of wins to losses (10.2% vs 4.4%). Due to the small proportion of events for each outcome, 80.2% of the pairs remained tied. We accounted for these ties by calculating the “win odds,” which was 1.17 (95% CI, 1.06–1.29, p = 0.001). The results indicated that patients in the DPI group had a 13% probability of achieving better composite outcomes compared to the APT group
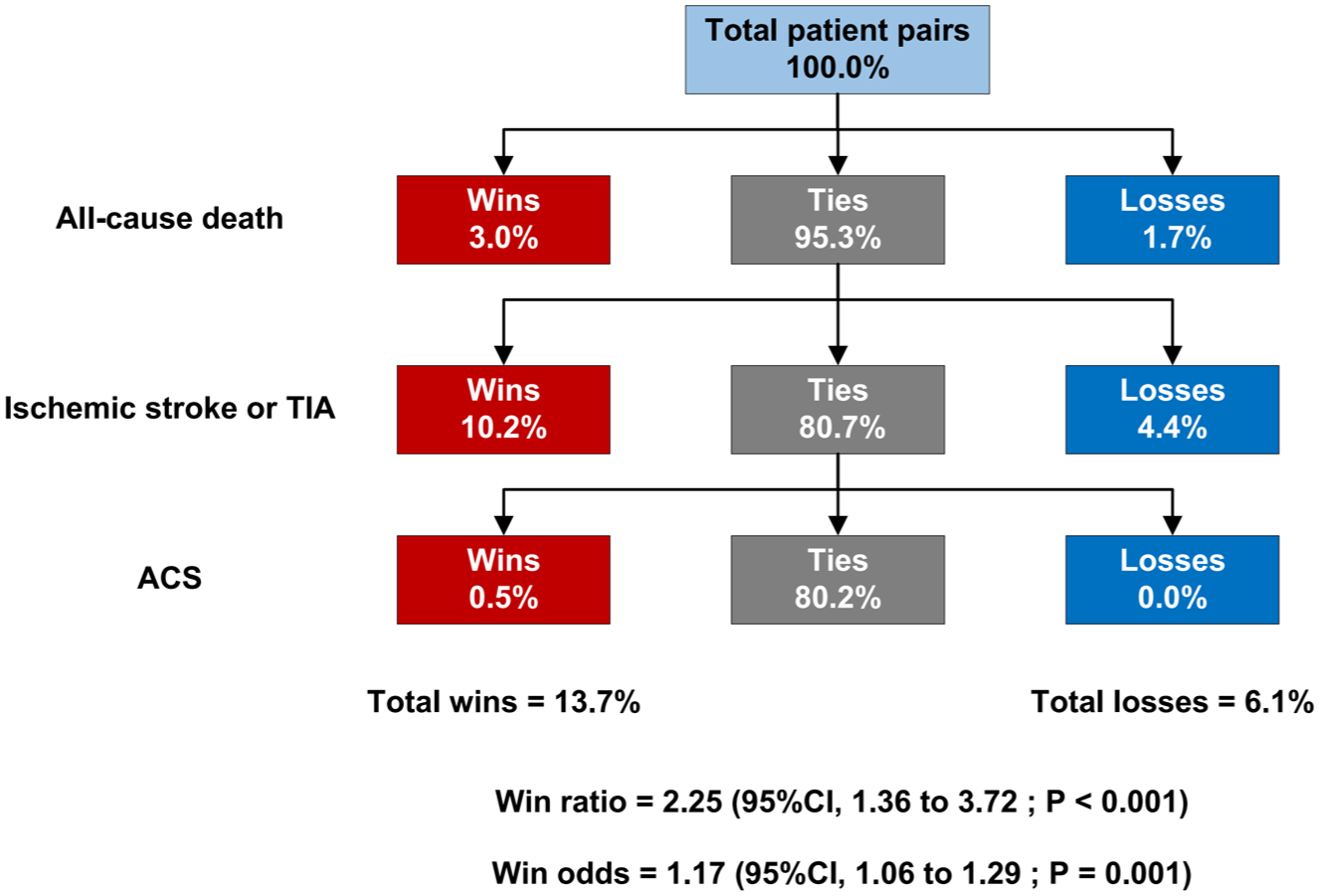
The win ratio analysis in the IPTW-based cohort.
Of the 1086 patients treated with antiplatelet therapy, 3 patients were hospitalized for gastrointestinal bleeding, and symptomatic intracranial hemorrhage occurred in 5 patients, 3 of whom died from intracranial hemorrhage (Table 2). Notably, no intracranial hemorrhage or fatal bleeding events were observed in the DPI group.
Sensitivity analyses
Dual pathway inhibition versus single antiplatelet therapy
There were 162 patients treated with single antiplatelet therapy (SAPT). IPTW was applied to balance baseline covariates between the DPI and SAPT groups (Supplementary Table 2). The risk of ischemic stroke and MACE was significantly lower in patients treated with DPI when compared with SAPT by 1 year (HR = 0.24, 95% CI: 0.11–0.52, p < 0.001; HR = 0.28, 95% CI: 0.14–0.54, p < 0.001). After IPTW, overall findings were similar with the analyses in unmatched cohort (HR = 0.18, 95% CI: 0.08–0.39, p < 0.001; HR = 0.21, 95% CI: 0.11–0.42, p < 0.001). Of the 162 patients treated with SAPT, 2 patients were hospitalized for gastrointestinal bleeding, and no patients experienced brain hemorrhage (Supplementary Table 3).
Dual pathway inhibition versus dual antiplatelet therapy
A total of 924 patients received DAPT. IPTW was employed between the DAPT and DPI groups (Supplementary Table 4). After IPTW, DPI was associated with a significantly lower risk of ischemic stroke and MACE by 1 year (HR = 0.42, 95% CI:0.19–0.93, p = 0.033; HR = 0.51, 95% CI: 0.26–1.00, p = 0.050) (Supplementary Table 5). Among patients in the DAPT group, the mean duration of therapy was 83.0 ± 31.3 days (Supplementary Table 1), and a total of 757 patients received standard 90-day DAPT (Supplementary Table 6). Compared with the 90-day DAPT group, DPI remained associated with a significantly lower risk of ischemic stroke (HR = 0.42, 95% CI: 0.19–0.93, p = 0.033) and MACE (HR = 0.50, 95% CI: 0.25–0.98, p = 0.044) at 1 year (Supplementary Table 7). All intracranial hemorrhages and fatal bleeding events among patients treated with antiplatelet therapy occurred exclusively in the DAPT group.
Sensitivity analyses comparing DPI with SAPT, DAPT, and 90-day DAPT showed consistent directions of association for ischemic stroke and MACE.
Discussion
In this study, we evaluated the efficacy of DPI with low-dose rivaroxaban plus antiplatelet therapy in preventing stroke recurrence in patients with sICAS compared to antiplatelet therapy alone. During the 1-year follow-up period, patients receiving the combination therapy experienced more than a 50% reduction in the risk of stroke recurrence. Bleeding events were infrequent in this cohort, and the small sample size precluded a reliable assessment of comparative bleeding risk.
In interpreting our findings, we considered the heterogeneity of antiplatelet therapy within the APT group. In routine clinical practice, APT encompasses both SAPT and DAPT with variable duration. A 90-day DAPT regimen has been widely adopted in contemporary secondary prevention following minor ischemic stroke or TIA. To enhance clinical interpretability, sensitivity analyses comparing DPI separately with SAPT, DAPT, and 90-day DAPT showed similar directions of association for ischemic stroke and MACE.
ICAS has been recognized as a high-risk factor for stroke recurrence. Studies indicate that patients with vascular stenosis exceeding 70% have a one-year stroke recurrence rate of over 20%.15,20,21 In contemporary clinical practice, DAPT is the cornerstone of secondary prevention for sICAS.22,23 In the SAMMPRIS and CASSISS trials, even with aggressive medical management based on DAPT, patients with sICAS still experienced substantial recurrence rates of 12.2% and 7.2%.4,6 Our study also observed a high recurrence rate of 12.5% in patients with sICAS receiving antiplatelet therapy, potentially attributable to the use of monotherapy in some patients. In this context, we explored whether long-term dual pathway inhibition might be associated with a lower risk of recurrent ischemic stroke compared with antiplatelet-based strategies.
Dual pathway inhibition exerts a synergistic effect by simultaneously inhibiting platelet aggregation, thrombin generation, and fibrin formation, thereby suppressing arterial thrombus growth.24–27 The stroke outcomes of the COMPASS trial indicated that, in patients with stable coronary artery disease or peripheral artery disease, the combination of low-dose rivaroxaban and aspirin reduced the incidence of fatal and disabling strokes by nearly half compared to aspirin monotherapy. 8 Another observational study found that high vascular risk patients who were prioritized for DPI treatment had a lower MACE incidence rate consistent with the findings of the COMPASS study. 28 Findings from the VOYAGER PAD (Vascular Outcomes Study of ASA Along with Rivaroxaban in Endovascular or Surgical Limb Revascularization for Peripheral Artery Disease) indicate that, in patients with peripheral artery disease undergoing lower-extremity revascularization, low-dose rivaroxaban in combination with aspirin significantly reduced the composite incidence of acute limb ischemia, major amputation of vascular origin, myocardial infarction, ischemic stroke, or cardiovascular mortality compared to aspirin monotherapy. 29 The DPI approach demonstrates promising efficacy in the prevention of atherosclerotic disease.
CATIS-ICAD (Combination Antithrombotic Treatment for Prevention of Recurrent Ischemic Stroke in Intracranial Atherosclerotic Disease) was a small-scale randomized controlled trial to evaluate the efficacy of DPI therapy for intracranial atherosclerotic disease. Although the difference was not statistically significant, the results indicated a trend toward a lower incidence of ischemic stroke in the rivaroxaban plus aspirin group compared to the aspirin monotherapy group in terms of absolute numbers, without an increased risk of hemorrhagic stroke. 30 The CATIS-ICAD pilot study confirmed the feasibility and safety of DPI therapy for sICAS. In this study, our findings demonstrated that DPI was associated with an improved prognosis in patients with sICAS compared with antiplatelet therapy alone in a real-world setting. The direction of effect observed in our cohort was generally consistent with that reported in CATIS-ICAD. Differences in effect magnitude may reflect variations in study design and patient characteristics. Our study represents a real-world cohort with a predominantly Asian population and a higher proportion of patients with prior stroke or TIA in the DPI group. Our study will provide new evidence for DPI therapy of sICAS and may offer insights for secondary prevention of sICAS.
As an observational study, our research inevitably has certain limitations. First, as a single-center study, it inevitably carries the risk of selection bias. In addition, as a regional tertiary stroke center, a portion of our patients were referred from other hospitals, which resulted in a relatively higher severity of symptoms and a higher incidence of prior stroke among our cohort. This may limit the generalizability of our findings. Second, as a real-world study, antiplatelet therapy was heterogeneous, including SAPT and DAPT, with variability in DAPT duration and regimen composition. Although sensitivity analyses comparing DPI separately with SAPT, DAPT, and 90-day DAPT were conducted to explore the impact of this heterogeneity, these analyses were exploratory and limited. Third, in this prospective registry study, patients were not randomly assigned to the two secondary prevention strategies, and outcome assessment was not blinded to treatment allocation. Although IPTW effectively controls for known confounders, it cannot fully eliminate the influence of unknown or unmeasured confounding factors. In addition, in-hospital events were not captured, which may limit the generalizability of our findings to very early post-stroke risk.
In conclusion, we observed that low-dose rivaroxaban combined with antiplatelet therapy may be associated with a lower risk of recurrent stroke compared with antiplatelet therapy alone in patients with sICAS. Given the small sample size and low number of bleeding events, this study cannot reliably assess the comparative bleeding risk. Our findings highlight a promising antithrombotic strategy for the secondary prevention of sICAS, offering new hope for secondary prevention in this high-risk population. These findings are preliminary and warrant further investigation through large-scale randomized controlled trials.
Supplemental Material
sj-docx-1-wso-10.1177_17474930261423387 – Supplemental material for Low-dose rivaroxaban plus antiplatelet therapy for symptomatic intracranial atherosclerotic stenosis: A prospective cohort study
Supplemental material, sj-docx-1-wso-10.1177_17474930261423387 for Low-dose rivaroxaban plus antiplatelet therapy for symptomatic intracranial atherosclerotic stenosis: A prospective cohort study by Ding Zhang, Zhaoyang Zhao, Yiwei Qian, Lulu Pei, Kai Liu, Yuan Cao, Wenzheng Rong, Haiman Hou, Yige Zhang, Wan Zhang, Ce Zong, Yifang Zhou, Jiaxin Wang, Chao Lan, Xinsheng Han, Duolao Wang, Yuesong Pan, MingMing Ning, Ferdinando S. Buonanno, Xinyi Leng, Yuming Xu and Bo Song in International Journal of Stroke
Footnotes
Acknowledgements
None.
Author contribution
Bo Song and Yuming Xu conceived and designed the study. Ding Zhang, Zhaoyang Zhao, Yiwei Qian, Yige Zhang, Wan Zhang, Ce Zong, Yifang Zhou, and Jiaxin Wang collected the data. Ding Zhang performed the statistical analysis and drafted the manuscript. Ding Zhang, Zhaoyang Zhao, and Bo Song had full access to all data and verified the analyses. Lulu Pei, Kai Liu, Yuan Cao, Wenzheng Rong, Haiman Hou, Chao Lan, Xinsheng Han, Yuesong Pan, MingMing Ning, Ferdinando S. Buonanno, and Xinyi Leng critically revised the manuscript. All authors approved the final version.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the the National Natural Science Foundation of China (No. 82171324, No. 82471349).
Ethical considerations
The study protocol was reviewed and approved by the Ethics Committee of the First Affiliated Hospital of Zhengzhou University (approval number: 2009-KY-05).
Consent to participate
Written informed consent to participate was obtained from each participant or their legally authorized representative prior to inclusion in the registry.
Consent for publication
Written informed consent for publication of anonymized clinical data was obtained from the participants or their legally authorized representatives.
Data availability statement
The data supporting this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.