
Abstract
Background:
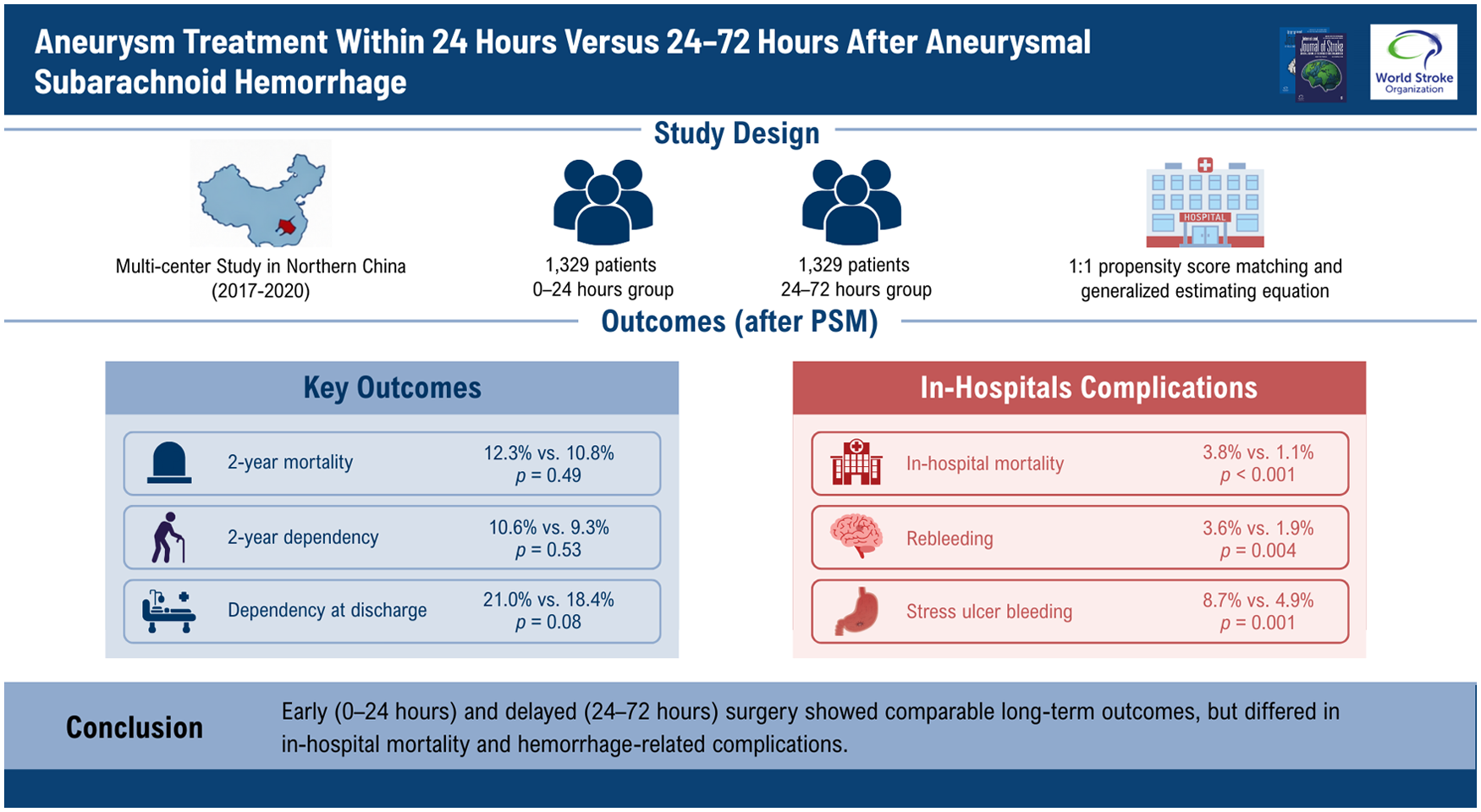
High-quality evidence comparing surgical strategies within 0–24 h and 24–72 h after aneurysmal subarachnoid hemorrhage (aSAH) remains limited. This study aimed to systematically evaluate surgical safety and long-term outcomes across these two critical time windows.
Methods:
Patients with aSAH undergoing aneurysm surgery within 72 h were consecutively enrolled from 12 tertiary centers in northern China between January 2017 and December 2020. A 1:1 propensity score matching (PSM) adjusted for intergroup differences, and a generalized estimating equation (GEE) model accounted for hospital-level clustering. Outcomes were compared between the 0–24 h and 24–72 h groups. Kaplan–Meier curves assessed survival, Cox models identified mortality risk factors, and logistic regression determined predictors of 2-year dependency.
Results:
A total of 3560 patients were included. After PSM, 1329 patients in the 0–24 h group were matched with 1329 in the 24–72 h group. There were no significant differences in 2-year mortality (12.3% vs 10.8%, p = 0.49), dependency at discharge (21.0% vs 18.4%; adjusted odds ratio (OR) = 0.815, 95% confidence interval (CI) = 0.649–1.024, p = 0.079), or 2-year dependency (10.6% vs 9.3%; adjusted OR = 0.896, 95% CI = 0.636–1.264, p = 0.533). Compared with the 0–24 h group, the 24–72 h group had lower in-hospital mortality (3.8% vs 1.1%; adjusted OR = 0.503, 95% CI = 0.349–0.723, p < 0.001), rebleeding (3.6% vs 1.9%; adjusted OR = 0.489, 95% CI = 0.299–0.801, p = 0.004), and stress ulcer bleeding (8.7% vs 4.9%; adjusted OR = 0.811, 95% CI = 0.713–0.922, p = 0.001). Risk factors for mortality and 2-year dependency differed between groups.
Conclusion:
Surgery within 24 h of onset showed similar long-term outcomes compared with treatment at 24–72 h, but in-hospital mortality and some hemorrhage-related complications differed. Risk factor analysis may provide guidance for individualized treatment strategies.
Introduction
Aneurysmal subarachnoid hemorrhage (aSAH) is associated with substantial morbidity and mortality. 1 Rebleeding is one of the most lethal complications of aSAH. The risk of rebleeding is higher within 24 h after the initial rupture and is associated with worse outcomes.2–4 Microsurgical treatment (MST) and endovascular treatment (EVT) have become the primary interventions for ruptured intracranial aneurysms, significantly reducing the risk of rebleeding.
Since key studies in the 1980s reported no significant difference in overall outcomes between treatment within 3 days of rupture and delayed treatment ⩾ 7 days, management strategies for aSAH have gradually shifted from “delayed” to “early” intervention (<72 h). 5 With advances in intensive care, neuroanesthesia, microsurgical techniques, and endovascular technology, an increasing number of centers have attempted to further advance treatment to within 24 h of onset, aiming to minimize the risk of early rebleeding. However, there is currently insufficient evidence to clarify whether surgical timing within <24 h versus 24–72 h affects final clinical outcomes. Notably, ultra-early surgery may be performed while patients still have elevated intracranial pressure, cerebral edema, or unstable physiological status, potentially increasing the risk of perioperative complications. Meanwhile, acute brain injury and ischemic cascades following aneurysm rupture may promote delayed cerebral ischemia (DCI), potentially offsetting the benefits of ultra-early intervention.6,7
Although previous studies have investigated the timing of intervention for aSAH, high-quality evidence directly comparing surgical strategies within <24 h versus 24–72 h remains scarce. This study, based on multicenter clinical data from northern China, systematically evaluates the surgical safety and long-term outcomes associated with these two critical time windows, providing new evidence to inform clinical decision-making and optimize treatment strategies.
Methods
Study design and participants
The China Multicenter Aneurysm Database (CMAD) is a multicenter, observational database that consecutively enrolled patients with aSAH admitted to 12 tertiary medical centers in northern China between January 2017 and December 2020. This study was approved by the Ethics Committee of Tianjin Medical University General Hospital (IRB2022-YX-175-01) and conducted in accordance with the ethical guidelines of the Declaration of Helsinki. As only routine clinical data were collected and the data were anonymized, the requirement for individual informed consent was waived. All surgeries were performed by experienced local surgical teams, with indications for surgery primarily determined by the treating team based on patient condition and in consultation with the patient or their family; nevertheless, all patients were managed in accordance with the recommendations of the American Heart Association/American Stroke Association (AHA/ASA) guidelines. 8
Inclusion criteria include (1) age ⩾ 18 years; (2) diagnosis of subarachnoid hemorrhage (SAH) confirmed by computed tomography (CT) or lumbar puncture; (3) presence of a saccular intracranial aneurysm confirmed by at least one imaging modality (computed tomography angiography (CTA), magnetic resonance angiography (MRA), or Digital Subtraction Angiography (DSA)); and (4) time from symptom onset to surgery ⩽72 h.
Exclusion criteria include (1) fusiform, dissecting, mycotic, or traumatic aneurysms; (2) coexisting arteriovenous malformations, arteriovenous fistulas, or Moyamoya disease; (3) severe comorbidities such as cardiopulmonary insufficiency; and (4) patients who underwent both MST and EVT.
Baseline data collection
Collected baseline characteristics included age, sex, medical history, lifestyle-related risk factors, presence of intracerebral or intraventricular hemorrhage (ICH/IVH), Hunt-Hess (HH) grade, World Federation of Neurosurgical Societies (WFNS) grade, aneurysm location, size, and number, surgical modality, cerebrospinal fluid drainage modality, and onset-to-treatment time (OTT). OTT was categorized as <24 h and 24–72 h. The 24–72 h interval was defined as delayed treatment. Reasons for delayed treatment were classified into four categories: (1) interhospital transfer; (2) weekend or public holidays; (3) nighttime presentation; and (4) unknown. At discharge, survival status, modified Rankin Scale (mRS) score, and in-hospital complications—including cerebral ischemia, hydrocephalus, seizures, rebleeding, and stress ulcer bleeding—were recorded. Rebleeding was defined radiologically as the appearance of new SAH, ICH, or IVH on follow-up CT after aneurysm treatment, compared with prior imaging. Other complications were defined according to standard clinical criteria and, when applicable, corroborated by postoperative imaging, following the definitions established by the National Institute of Neurological Disorders and Stroke (NINDS). Functional and survival outcomes were evaluated by neurosurgeons using the mRS (0 = complete recovery, 6 = death), with unfavorable outcomes defined as an mRS score of 3–6.
Outcome measures
Patients were followed up for 2 years through standardized telephone interviews and outpatient visits. The primary outcome was all-cause mortality. Secondary outcomes included functional status at 2 years (independent survival: mRS = 0–2; dependent survival: mRS = 3–5) and in-hospital complications.
Statistical analyses
Continuous variables were presented as mean ± standard deviation (SD) or median with interquartile range (IQR), and categorical variables were presented as counts (percentages). The Mann–Whitney U-test was used to compare continuous variables, while the chi-square test or Fisher’s exact test was used for categorical variables.
To adjust for intergroup differences, 1:1 nearest-neighbor propensity score matching (PSM) without replacement was performed, with a caliper width of 0.01. Covariate balance after matching was assessed using standardized mean differences (SMD), with SMD < 0.1 considered indicative of adequate balance. A generalized estimating equation (GEE) model was used, with hospital as the clustering variable, applying linear or binary logistic regression and an exchangeable correlation structure to examine the relationship between OTT and outcomes.
The Kaplan–Meier survival curves were used to compare survival between groups. Cox proportional hazards models were employed to identify risk factors for mortality, and logistic regression was used to determine risk factors for dependent survival at 2 years. Univariable analyses were first performed, and variables with p < 0.05 were subsequently included in multivariable analyses.
To assess the impact of loss to follow-up on the analysis of 2-year mortality, a sensitivity analysis was performed. Two extreme assumptions were applied to handle patients lost to follow-up: (1) best-case scenario, assuming all lost patients in both groups survived and (2) worst-case scenario, assuming all lost patients died. Logistic regression models were constructed under each scenario to examine whether loss to follow-up affected the estimated association between OTT and 2-year mortality. Covariates included in the models were age, previous stroke, presence of ICH/IVH, HH grade, WFNS grade, aneurysm location, and treatment modality.
In addition, to evaluate whether cerebrospinal fluid drainage modalities influenced the association between OTT and 2-year outcomes, a sensitivity analysis was performed with further adjustment for cerebrospinal fluid drainage modalities, in addition to the covariates listed above.
Statistical analyses were performed using SPSS version 27 (IBM Corp, Armonk, NY, USA), R version 4.4.1 (R Foundation for Statistical Computing, Vienna, Austria), and GraphPad Prism 9.5. Two-sided p-values < 0.05 were considered statistically significant for 95% confidence intervals (CIs).
Results
Between January 2017 and December 2020, a total of 3560 patients from 12 hospitals were included in the study. The detailed inclusion process is shown in Supplemental Figure S1, and the distribution of surgery timing across the 12 hospitals is presented in Supplemental Figure S2. A total of 1853 patients experienced delayed treatment. The most common reason was interhospital transfer (74.0%), followed by weekend or public holidays (10.0%) and nighttime presentation (9.6%). The remaining 6.4% of cases were classified as having an unknown reason for delay. The distribution of delayed treatment reasons stratified by different factors is presented in Supplemental Table S1. Baseline characteristics differed between groups in terms of the presence of ICH/IVH, HH grade, WFNS grade, aneurysm number, and surgical modality. After PSM, 1329 patients undergoing surgery within 0–24 h were matched to 1329 patients undergoing surgery within 24–72 h, with baseline characteristics well balanced (SMD < 0.1) (Table 1).
Baseline characteristics before and after PSM.
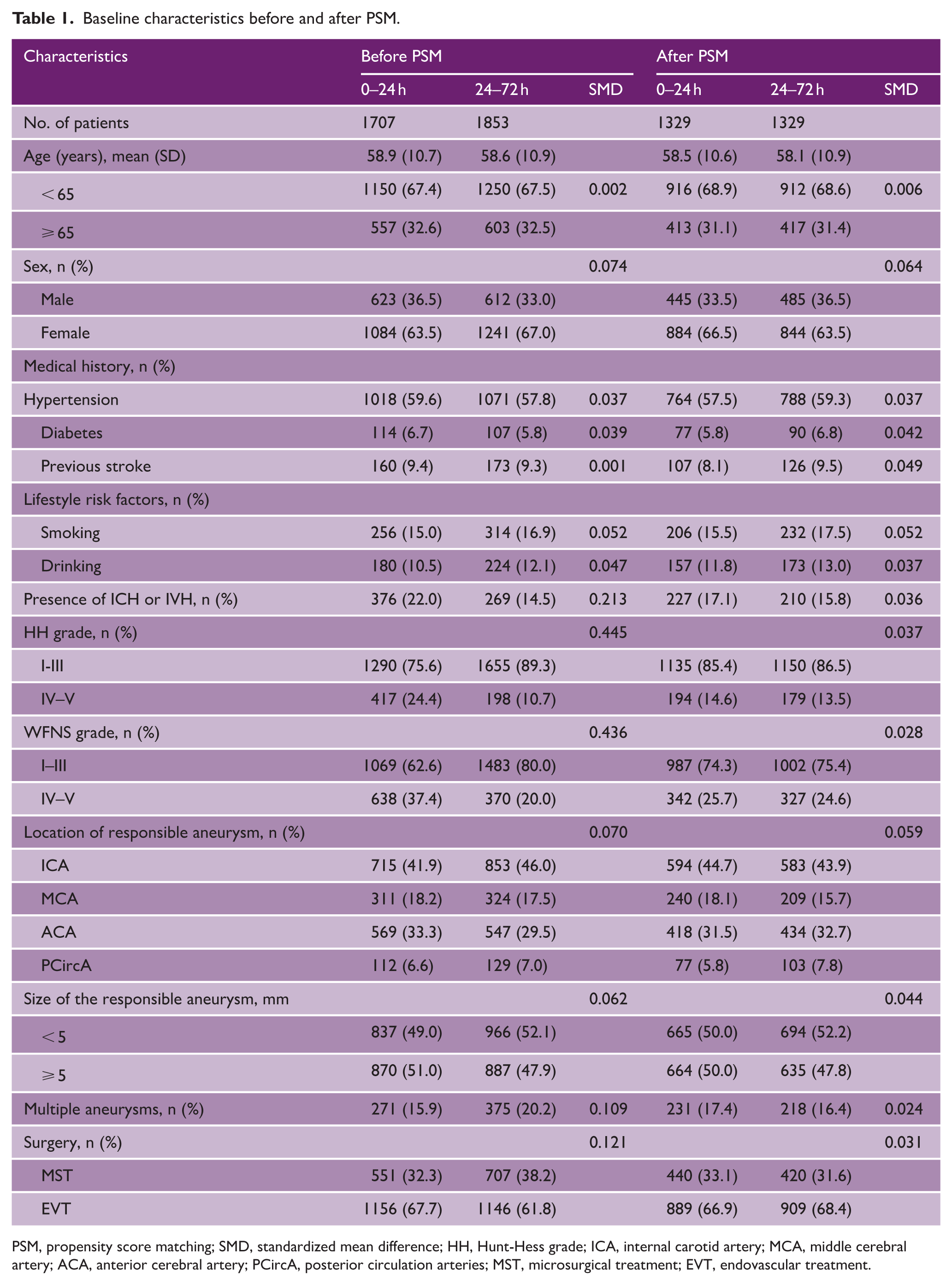
PSM, propensity score matching; SMD, standardized mean difference; HH, Hunt-Hess grade; ICA, internal carotid artery; MCA, middle cerebral artery; ACA, anterior cerebral artery; PCircA, posterior circulation arteries; MST, microsurgical treatment; EVT, endovascular treatment.
Compared with the 0–24 h surgery group, the 24–72 h surgery group had lower in-hospital mortality (3.8% vs 1.1%; adjusted odds ratio (OR) = 0.503, 95% CI = 0.349–0.723, p < 0.001), lower rates of unfavorable outcomes at discharge (24.0% vs 19.3%; adjusted OR = 0.776, 95% CI = 0.625–0.964, p = 0.022), reduced rebleeding (3.6% vs 1.9%; adjusted OR = 0.489, 95% CI = 0.299–0.801, p = 0.004), and decreased stress ulcer bleeding (8.7% vs 4.9%; adjusted OR = 0.811, 95% CI = 0.713–0.922, p = 0.001) (Table 2).
Comparison of discharge information and in-hospital complications between patients treated within <24 h and 24–72 h.
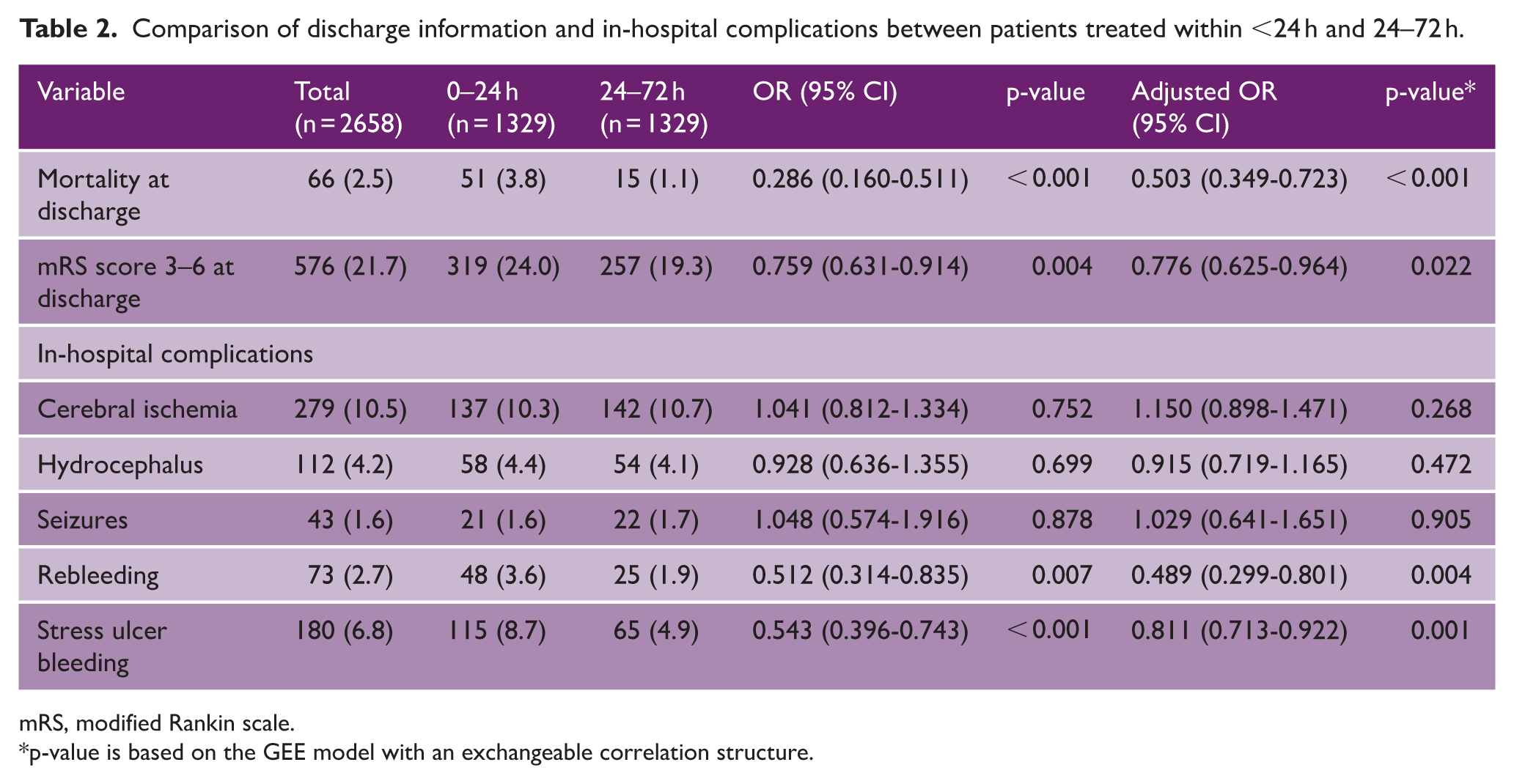
mRS, modified Rankin scale.
p-value is based on the GEE model with an exchangeable correlation structure.
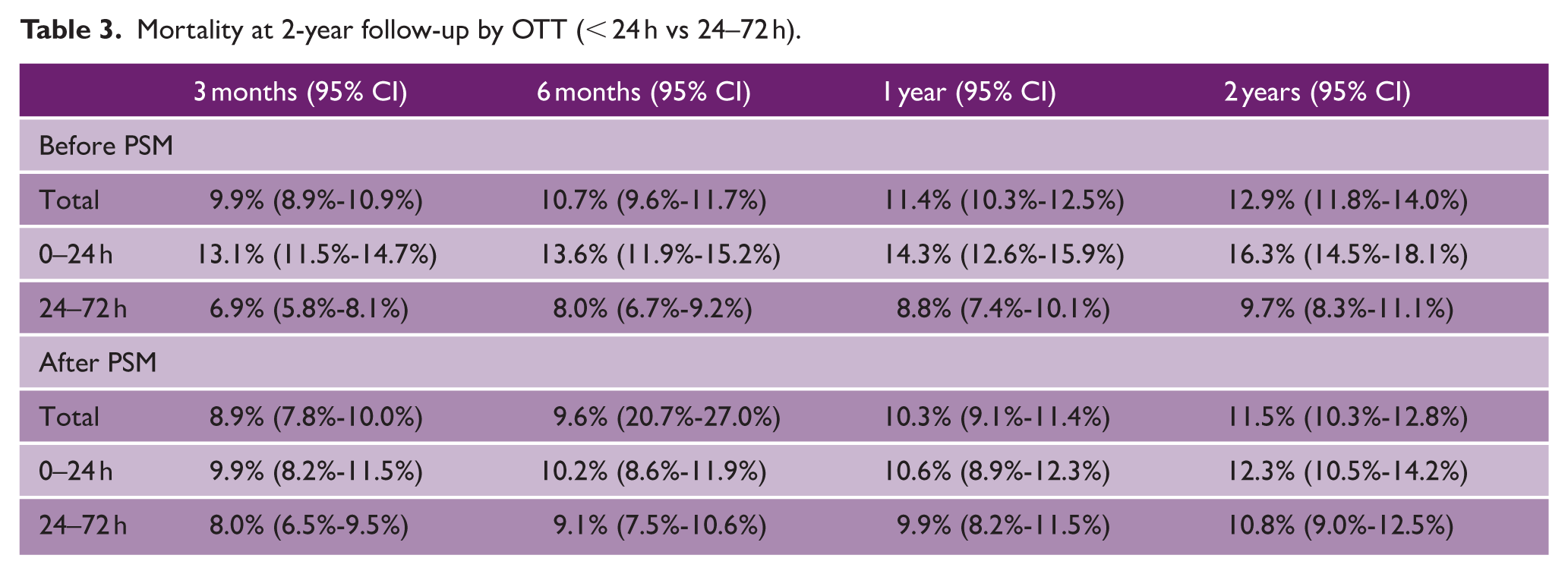
Figure 1 compares the survival outcomes between patients undergoing surgery within 0–24 h and those within 24–72 h. A total of 2658 patients were included in the survival analysis, with a mean follow-up duration of 31.27 ± 22.34 months. The overall 3-month and 2-year mortality rates were 8.9% and 11.5%, respectively. Before PSM, the 24–72 h surgery group had a significantly lower 2-year mortality rate compared with the 0–24 h group (9.7% vs 16.3%, p < 0.001). After PSM, the difference in 2-year mortality between the two groups was no longer significant (10.8% vs 12.3%, p = 0.49). Detailed 2-year mortality data are presented in Table 3. Sensitivity analysis indicated that loss to follow-up did not materially affect the 2-year mortality results (Supplemental Figure S3).
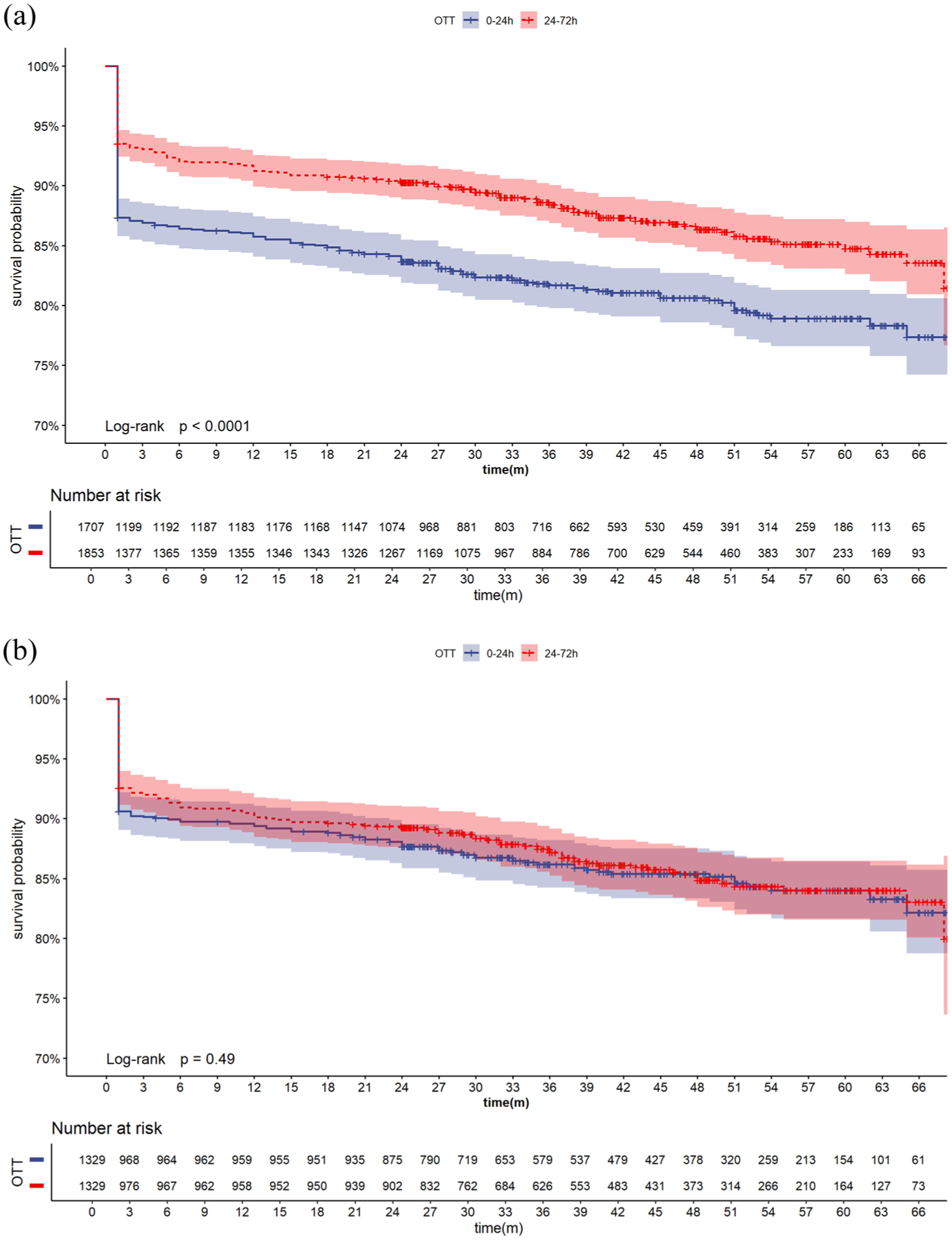
Kaplan–Meier curves for 2-year survival in the 0–24 h vs 24–72 h groups: (a) before PSM and (b) after PSM.
Mortality at 2-year follow-up by OTT (< 24 h vs 24–72 h).
Multivariable Cox proportional hazards models identified the following predictors of mortality in the 0–24 h surgery group: age ⩾ 65 years (hazard ratio (HR) = 2.257, 95% CI = 1.669–3.050, p < 0.001), previous stroke (HR = 1.599, 95% CI = 1.053–2.429, p = 0.028), presence of ICH/IVH (HR = 1.468, 95% CI = 1.043–2.066, p = 0.028), HH grade IV–V (HR = 2.765, 95% CI = 1.711–4.470, p < 0.001), and WFNS grade IV–V (HR = 1.738, 95% CI = 1.071–2.818, p = 0.025). In the 24–72 h surgery group, independent risk factors for mortality included age ⩾ 65 years (HR = 2.880, 95% CI = 2.096–3.957, p < 0.001), previous stroke (HR = 1.974, 95% CI = 1.269–3.071, p = 0.003), WFNS grade IV–V (HR = 2.438, 95% CI = 1.607–3.699, p < 0.001), ACA aneurysm (HR = 1.533, 95% CI = 1.048–2.243, p = 0.028), and posterior circulation aneurysm (HR = 2.859, 95% CI = 1.788–4.573, p < 0.001). EVT (HR = 0.450, 95% CI = 0.320–0.633, p < 0.001) was identified as a protective factor in this group (Supplemental Tables S2 and S3).
A total of 2062 patients completed the 2-year follow-up, of whom 1772 survived. There were no significant differences between the 0–24 h group and the 24–72 h group in terms of dependency at discharge (21.0% vs 18.4%, adjusted OR 0.815, 95% CI = 0.649–1.024, p = 0.079) or at 2 years (10.6% vs 9.3%, adjusted OR 0.896, 95% CI = 0.636–1.264, p = 0.533). In addition, the 2-year mortality (15.2% vs 12.9%, adjusted OR 0.805, 95% CI = 0.627–1.032, p = 0.088) did not differ between groups (Table 4). The detailed distribution of mRS scores is shown in Figure 2.
Outcomes by OTT in patients with completed follow-up.
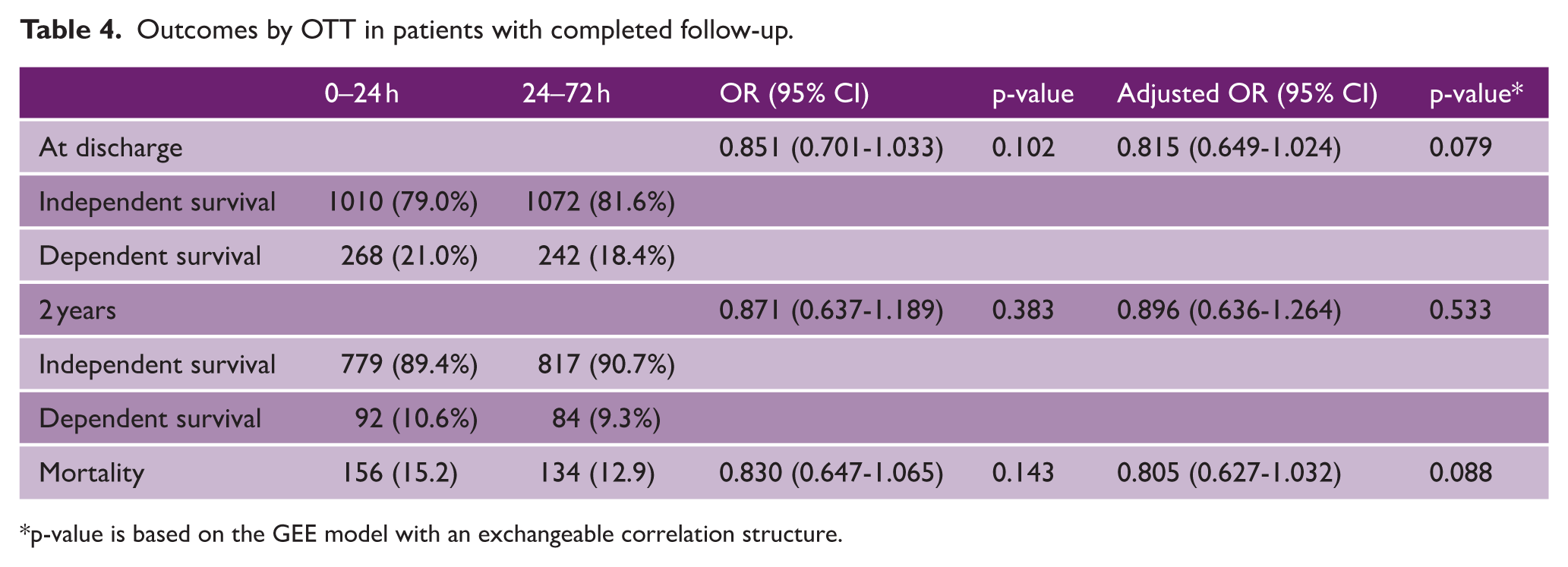
p-value is based on the GEE model with an exchangeable correlation structure.
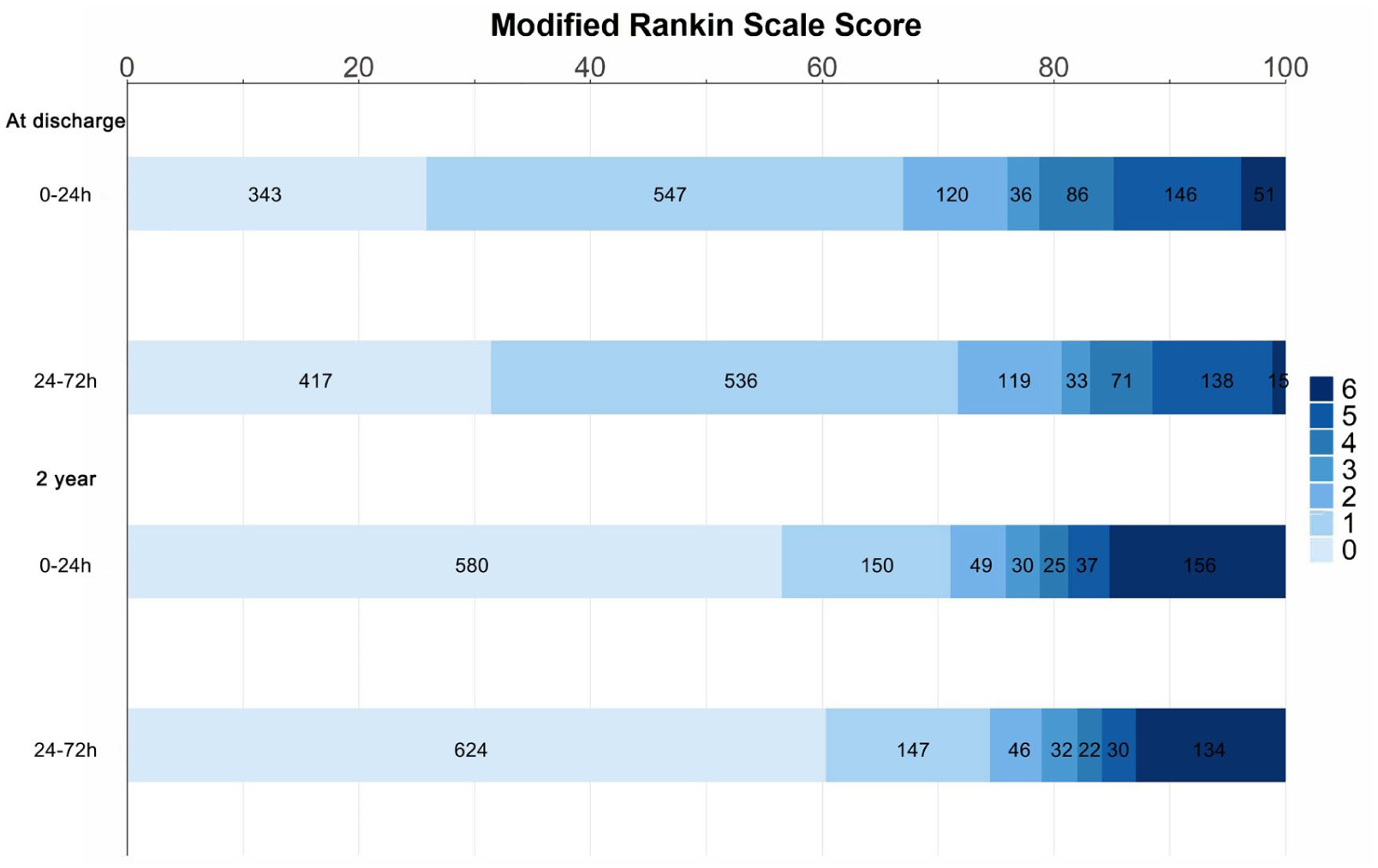
Distribution of mRS scores at discharge and 2-year follow-up.
Multivariable logistic regression identified age ⩾ 65 years (OR = 2.435, 95% CI = 1.437–4.126, p < 0.001), HH grade IV–V (OR = 2.625, 95% CI = 1.221–5.645, p = 0.013), WFNS grade IV–V (OR = 2.305, 95% CI = 1.187–4.474, p = 0.014), and middle cerebral artery (MCA) aneurysm location (OR = 3.022, 95% CI = 1.574–5.800, p < 0.001) as independent risk factors for 2-year dependency in the 0–24 h group, whereas EVT (OR = 0.503, 95% CI = 0.296–0.854, p = 0.011) was a protective factor. In the 24-72 h group, age ⩾ 65 years (OR = 2.695, 95% CI = 1.606–4.524, p < 0.001), diabetes (OR = 3.043, 95% CI = 1.342–6.897, p = 0.088), HH grade IV–V (OR = 3.224, 95% CI = 1.411–7.370, p = 0.006), WFNS grade IV–V (OR = 2.291, 95% CI = 1.082–4.852, p = 0.030), and multiple aneurysms (OR = 1.852, 95% CI = 1.032–3.324, p = 0.039) were independent risk factors for 2-year dependency, while EVT (OR = 0.559, 95% CI = 0.320–0.978, p = 0.042) was protective (Supplemental Tables S4 and S5).
The use of cerebrospinal fluid drainage modalities, including external ventricular drain (EVD) and lumbar drain (LD), differed between the two groups, with detailed distributions shown in Supplemental Table S6. However, sensitivity analyses demonstrated that adjustment for drainage modalities did not materially alter the association between surgical timing and 2-year outcomes (Supplemental Table S7).
Discussion
This multicenter cohort study demonstrated that surgery performed within 0–24 h and 24–72 h yielded comparable long-term mortality and functional outcomes. However, compared with the 0–24 h group, the 24–72 h group exhibited lower in-hospital mortality, rebleeding rates, and stress-related ulcer bleeding. In addition, we identified risk factors for mortality and 2-year dependency in both groups. To our knowledge, this is one of the few multicenter, large-scale studies that systematically compares outcomes between surgery performed within 0–24 h and 24–72 h.
The 2023 AHA/ASA guidelines recommend early aneurysm treatment when feasible, ideally within 24 h of onset, to reduce the risk of rebleeding and other complications. 9 However, whether ultra-early treatment (<24 h) provides additional benefit over intervention within 24–72 h for aSAH patients remains controversial. In this study, surgery performed within 24 h was not associated with a clear advantage in long-term outcomes compared with surgery performed at 24–72 h, which is consistent with findings from two previous large, independent aSAH cohort studies. 10 This may partly be explained by the exclusion of patients treated beyond 72 h in the present study, which may have reduced the bias observed in previous studies where the >24 h group included a substantial proportion of markedly delayed treatments. Früh et al. 11 suggested avoiding surgery on the day of hemorrhage, and Vergouwen et al. 12 indicated that the benefit of treating ruptured aneurysms within the ultra-early window (<6 h) is limited. Moreover, aneurysm surgery performed within the first few hours after rupture carries a higher risk of intraoperative rupture. 13 A meta-analysis even suggested that ultra-early treatment may potentially harm patients. 14 Although baseline characteristics were adjusted using PSM in our study, this conclusion still requires further investigation in large prospective studies.
Rebleeding is one of the main causes of poor outcomes in patients who survive the initial hemorrhage. 15 Previous studies have shown that aneurysm treatment within a 24-h window can halve the risk of clinical rebleeding in patients with aSAH. 16 Interestingly, we found that the risk of rebleeding was significantly lower in patients undergoing aneurysm surgery within 24–72 h compared with those treated within 24 h. Oudshoorn et al. 10 reported that two-thirds of rebleeding episodes occur within the first 3 h after admission, a time frame in which aneurysm occlusion is practically impossible. Moreover, the potential benefit of surgery within 24 h for reducing rebleeding risk may be, at least in part, counterbalanced by early brain injury and physiological instability after aSAH. Consistent with existing evidence, in our study, patients treated within 24 h had a higher in-hospital mortality than those treated within 24–72 h. Furthermore, we observed that patients undergoing surgery within 24–72 h had a 28.7% lower risk of stress-related ulcer bleeding, which may reflect both attenuation of the acute stress response and the supportive effects of clinical gastric mucosal protection therapy.
We also analyzed prognostic risk factors across different time windows. The presence of ICH/IVH was a specific risk factor for mortality in patients undergoing surgery within 24 h. Patients with more severe IVH experienced pathological elevations in intracranial pressure (ICP) and vasospasm more frequently than those with mild or asymptomatic IVH.17,18 Severe early brain injury and impaired intracranial pressure compensation appear to have a greater impact on survival outcomes during the ultra-early surgical period. In contrast, for surgeries performed within 24–72 h, aneurysm characteristics and the chosen surgical approach significantly influenced survival. This suggests that survival outcomes in the hyperacute phase are primarily determined by overall systemic condition and initial injury, whereas in the delayed phase, local anatomical complexity and procedural factors begin to dominate survival differences. Nevertheless, for patients undergoing intervention within <24 h, careful assessment of aneurysm complexity and surgical approach remains crucial, as these factors may substantially affect functional outcomes among survivors. Furthermore, the presence of multiple aneurysms increased the 2-year dependency risk in the 24–72 h group, likely because treating multiple aneurysms requires greater manipulation of major cerebral arteries and brain tissue, thereby elevating the risk of vasospasm.19,20 Age, previous stroke, and admission grading were shared risk factors for mortality in both the <24 h and 24–72 h surgery groups. In addition, age and admission grading also influenced functional outcomes, consistent with previous studies.21,22 These findings indicate that baseline patient status and the severity of initial injury largely determine prognosis, and the timing of surgery alone is insufficient to overcome these core risk factors.
We further analyzed the underlying reasons for delayed treatment. In this study, delayed intervention was most commonly attributable to interhospital transfer, which likely reflects the uneven distribution of healthcare resources in China, where advanced neurosurgical and neurointerventional services are predominantly concentrated in major urban centers. 23 In contrast, rural and remote regions often have limited medical resources and insufficient access to specialized care, making referral to higher-level hospitals frequently unavoidable and a major contributor to treatment delay.
Limitations
This study has several limitations. First, as a retrospective observational study, surgical timing could not be randomly assigned. In clinical practice, patients with less severe disease may experience delayed transfer and treatment, whereas those with greater hemorrhage burden or more severe neurological status often require earlier intervention. Such treatment selection based on disease severity cannot be fully accounted for statistically. In addition, surgical indications are typically determined by the treating team in consultation with the patient or their family, particularly in poor-grade patients (WFNS IV–V), which may introduce unmeasured selection bias. Second, owing to the retrospective nature of the database, the timing of cerebrospinal fluid drainage (EVD/LD) was not systematically recorded and therefore could not be incorporated as a time-dependent variable in the analysis. Rebleeding events were identified based on postoperative follow-up CT findings; because precise temporal information was unavailable, we were unable to determine the exact timing of rebleeding. Although PSM was performed and WFNS and HH grades were included, these measures may not fully capture the heterogeneity of disease severity or hemorrhage burden, leaving residual confounding possible. Third, this study included patients from only 12 hospitals, which may limit its national representativeness. Finally, despite efforts to minimize loss to follow-up, 17.9% of patients were lost; however, sensitivity analyses indicated that missing data did not materially affect the association between surgical timing and 2-year mortality.
Conclusion
This study found that patients undergoing surgery within 24 h of onset had similar long-term outcomes compared with those treated at 24–72 h, although differences were observed in in-hospital mortality and certain hemorrhage-related complications. Identification and evaluation of key risk factors across time windows may help guide individualized surgical decision-making. Given the observational design and potential residual selection bias, these findings should be interpreted with caution and should not be considered causal. Future high-quality prospective studies are needed to validate these results.
Supplemental Material
sj-docx-1-wso-10.1177_17474930261427060 – Supplemental material for Aneurysm treatment within 24 h versus 24–72 h after aneurysmal subarachnoid hemorrhage
Supplemental material, sj-docx-1-wso-10.1177_17474930261427060 for Aneurysm treatment within 24 h versus 24–72 h after aneurysmal subarachnoid hemorrhage by Xiuhu An, Shusheng Che, Litong Zhang, Ruyi Wang, Zhenjie Wang, Bangyue Wang, Hao Zhang, Yang Guo, Xinyu Yang, Shifang Li, Xiaochuan Sun and Feng Guo in International Journal of Stroke
Footnotes
Author contributions
X.A., S.C., and L.Z. designed the study, collected clinical data, and drafted the initial manuscript. R.W., Z.W., B.W., H.Z., and Y.G. contributed to data organization, statistical analysis, and visualization of results. X.A., S.C., and L.Z. also participated in literature interpretation and manuscript refinement. X.Y., S.L., X.S., and F.G. supervised the overall research process, provided critical revisions for intellectual content, and approved the final version of the manuscript. All authors reviewed and agreed on the final submission.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of Tianjin, China (grant no. 20JCZDJC00300), the Tianjin Medical University General Hospital Clinical Research Program (grant no. 22ZYYLCCG07), and the National Natural Science Foundation of China (grant no. 82201530).
Ethical approvals
The study was approved by the Ethics Committee of Tianjin Medical University General Hospital (IRB2022-YX-175-01).
Data availability statement
The data used in this study can be obtained from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.