
Abstract
Background:
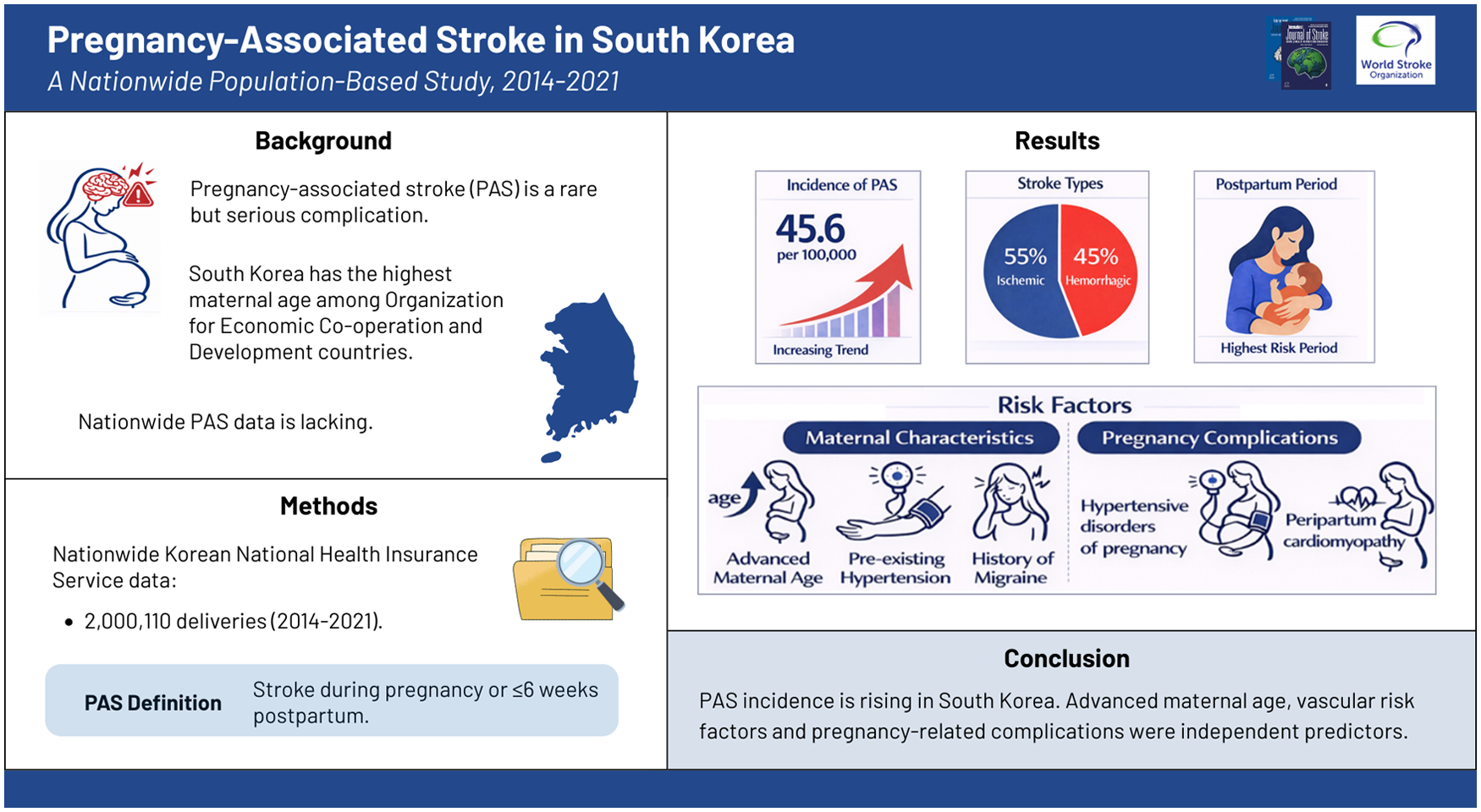
Pregnancy-associated stroke (PAS) is a rare but clinically important complication of pregnancy. Despite its clinical significance, nationwide data on PAS are lacking in South Korea, a representative country with advanced maternal age.
Aims:
This study aimed to investigate the incidence, temporal trends, and risk factors of PAS in South Korea.
Methods:
We retrospectively analyzed nationwide data from the Korean National Health Insurance Service (NHIS) to identify women of reproductive age (15–49 years) who delivered between 2014 and 2021. PAS was defined as an ischemic or hemorrhagic stroke occurring during pregnancy or within 6 weeks postpartum. Multivariable logistic regression analysis was performed to identify independent predictors of PAS.
Results:
Of 2,000,110 deliveries between 2014 and 2021, 909 first-ever strokes occurred during pregnancy or within 6 weeks postpartum, including 500 ischemic (55%) and 409 hemorrhagic (45%) strokes. The overall incidence of PAS was 45.6 per 100,000 deliveries (95% confidence interval (CI), 42.7–48.6) and increased from 41.5 in 2014 to 51.0 in 2021 (p = 0.049), mainly driven by ischemic stroke. PAS occurred predominantly during the postpartum period (p < 0.0001) and among older women (p for trend < 0.0001). In multivariable analysis, advanced maternal age (odds ratio [OR] per year, 1.02; 95% CI, 1.01–1.05), hypertension (OR, 2.04; 95% CI, 1.37–3.04), migraine (OR, 1.33; 95% CI, 1.02–1.74), gestational hypertension (OR, 1.49; 95% CI, 1.04–2.12), pre-eclampsia/eclampsia (OR, 5.00; 95% CI, 3.59–6.96), and peripartum cardiomyopathy (OR, 14.26; 95% CI, 4.48–45.42) were identified as independent predictors of PAS.
Conclusion:
The incidence of PAS is increasing in South Korea, with advanced maternal age, vascular risk factors, and pregnancy-related complications serving as independent predictors. These findings emphasize the importance of clinical awareness and the identification of women at high risk of PAS.
Introduction
Pregnancy is a stroke risk factor unique to women, attributable to physiological changes during pregnancy—such as alterations in hemodynamics, coagulation, and the immune system—as well as pregnancy-related pathological conditions, including hypertensive disorders of pregnancy and peripartum cardiomyopathy (PPCM). 1 Pregnancy-associated stroke (PAS), also known as maternal stroke, refers to ischemic or hemorrhagic stroke occurring during pregnancy or the postpartum period. Although PAS is relatively rare, it affects not only the mother but also the infant and places a substantial burden on the family.
The association between pregnancy and stroke has long been recognized, but reported PAS incidence varies widely across studies, likely reflecting differences in data sources, inclusion criteria, and geographic factors such as healthcare systems, socioeconomic conditions, and population genetics. 2 A 2017 meta-analysis reported a pooled crude PAS incidence of 30.0 per 100,000 pregnancies, nearly threefold higher than that in non-pregnant women of reproductive age. 2 Since then, nationwide data from North America and Europe (the United States, 3 Canada, 4 the United Kingdom, 5 Sweden, 6 Finland, 7 and France 8 ) have provided updated insights into PAS incidence and trends. Most studies report a rising incidence,4,5,7–9 largely attributed to increasing maternal age. 9
South Korea stands out for having the lowest total fertility rate among all member countries of the Organisation for Economic Co-operation and Development (OECD), 10 accompanied by a marked increase in maternal age at childbirth; in 2022, the mean maternal age exceeded 33 years, the highest among OECD countries. 11 Advanced maternal age is a well-established risk factor for adverse pregnancy outcomes, including maternal mortality.12,13 However, nationwide data on PAS in South Korea are lacking. Given the global trend toward advanced maternal age, South Korea provides a valuable context for understanding PAS. Accordingly, this study aimed to investigate the incidence, temporal trends, and risk factors of PAS in South Korea.
Methods
Data sources
All clinical data were obtained from the national health insurance claims database of the Korean National Health Insurance Service (NHIS). 14 The Korean NHIS is a universal health insurance system that provides comprehensive medical coverage to approximately 97% of the population. The remaining 3% of the population, consisting of low-income individuals, are covered by a government-financed Medical Aid program administered by the NHIS, ensuring that nearly all citizens are included in the NHIS database. 15 The NHIS database contains claims data on medical service utilization, including records of diagnoses, treatments, procedures, hospitalizations, discharges, and prescriptions. 15 All data are encrypted and de-identified to protect patient privacy.
This study was approved by the Institutional Review Board of Inha University Hospital (IRB No. 2024-06-012). The requirement for written informed consent was waived due to the retrospective use of anonymized data. The study was conducted in accordance with the Declaration of Helsinki and relevant guidelines.
Study population
Because data on the last menstrual period and gestational age were unavailable, the exact onset and duration of pregnancy could not be determined. Therefore, delivery was used as a proxy for the pregnancy period. The study population included women aged 15–49 years who delivered between 1 January 2014 and 31 December 2021. Deliveries were identified using domestic Korean procedure codes (R3131–R3148, R4351–R4362, R4380, R4504–R4520, and R5001–R5002). The delivery date was defined as the date the delivery code was recorded.
Definition of PAS
PAS was defined as stroke occurring during pregnancy or the postpartum period. Pregnancy was defined as the 280 days before delivery, and the postpartum period as the day of delivery through 6 weeks postpartum. Stroke was identified using the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) for hemorrhagic stroke (subarachnoid hemorrhage (SAH) [I60.X] and intracerebral hemorrhage (ICH) [I61.X]) and ischemic stroke (I63.X). Women with a history of stroke before pregnancy were excluded.
Patient characteristics
Patient characteristics included demographic variables and medical comorbidities, which were identified using the corresponding ICD-10-CM codes (Supplementary Table 1). Infertility treatment was defined using the Korean Standard Classification of Diseases (KCD) code Z31, corresponding to assisted reproductive technology. Cesarean delivery was identified using domestic Korean procedure codes for cesarean section (R4504–R4520 and R5001–R5002).
Statistical analysis
Crude PAS incidence was calculated as the number of cases per total deliveries. The 95% confidence intervals (CIs) for incidence were estimated using the Poisson distribution, and temporal and age-related trends were assessed using the Cochran–Armitage trend test. Differences in the distribution of PAS across the four periods (first, second, and third trimesters, and the postpartum period) were assessed using the chi-square test. Group comparisons used the chi-square test for categorical variables and the t test for continuous variables. Odds ratios (ORs) and 95% CIs were estimated using logistic regression. Univariate and age-adjusted analyses were performed, and variables significant in univariate analysis were entered into multivariable models. Analyses were performed using SAS software (version 9.4; SAS Institute Inc., Cary, NC, USA), with two-tailed p values < 0.05 considered statistically significant.
Results
Among 2,000,110 deliveries between January 2014 and December 2021, 909 first-ever strokes occurred during pregnancy or within 6 weeks postpartum (Figure 1), including 500 ischemic (55.0%) and 409 hemorrhagic strokes (45.0%).
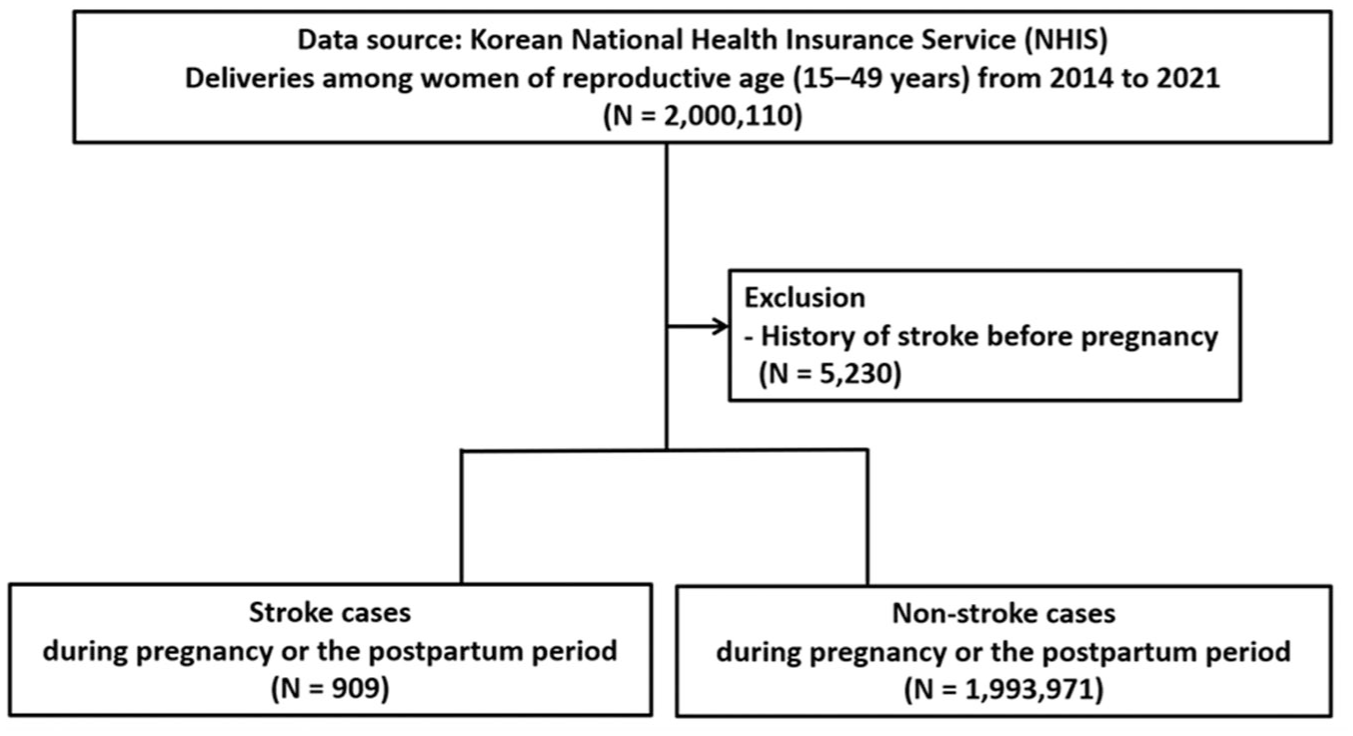
Flowchart of the study population. Flowchart illustrating the selection of the study cohort.
Incidence over time
The cumulative stroke incidence was 45.6 per 100,000 deliveries (95% CI, 42.7–48.6). The incidence of ischemic stroke, ICH, and SAH was 25.1 (95% CI, 22.9–27.4), 16.2 (95% CI, 14.5–18.1) and 7.3 (95% CI, 6.1–8.6) per 100,000 deliveries, respectively. Overall stroke incidence increased from 41.5 per 100,000 deliveries in 2014 to 51.0 in 2021 (p = 0.049; Figure 2), mainly driven by ischemic stroke, which rose from 21.3 to 28.3 per 100,000 deliveries (p = 0.004). In 2014, hemorrhagic and ischemic stroke incidence was identical (21.3 per 100,000 deliveries); thereafter, ischemic stroke increased steadily, whereas hemorrhagic stroke remained relatively stable. During the same period, mean maternal age increased significantly from 30.69 years in 2014 to 32.56 years in 2021 (p for trend < 0.0001) (Figure 3).
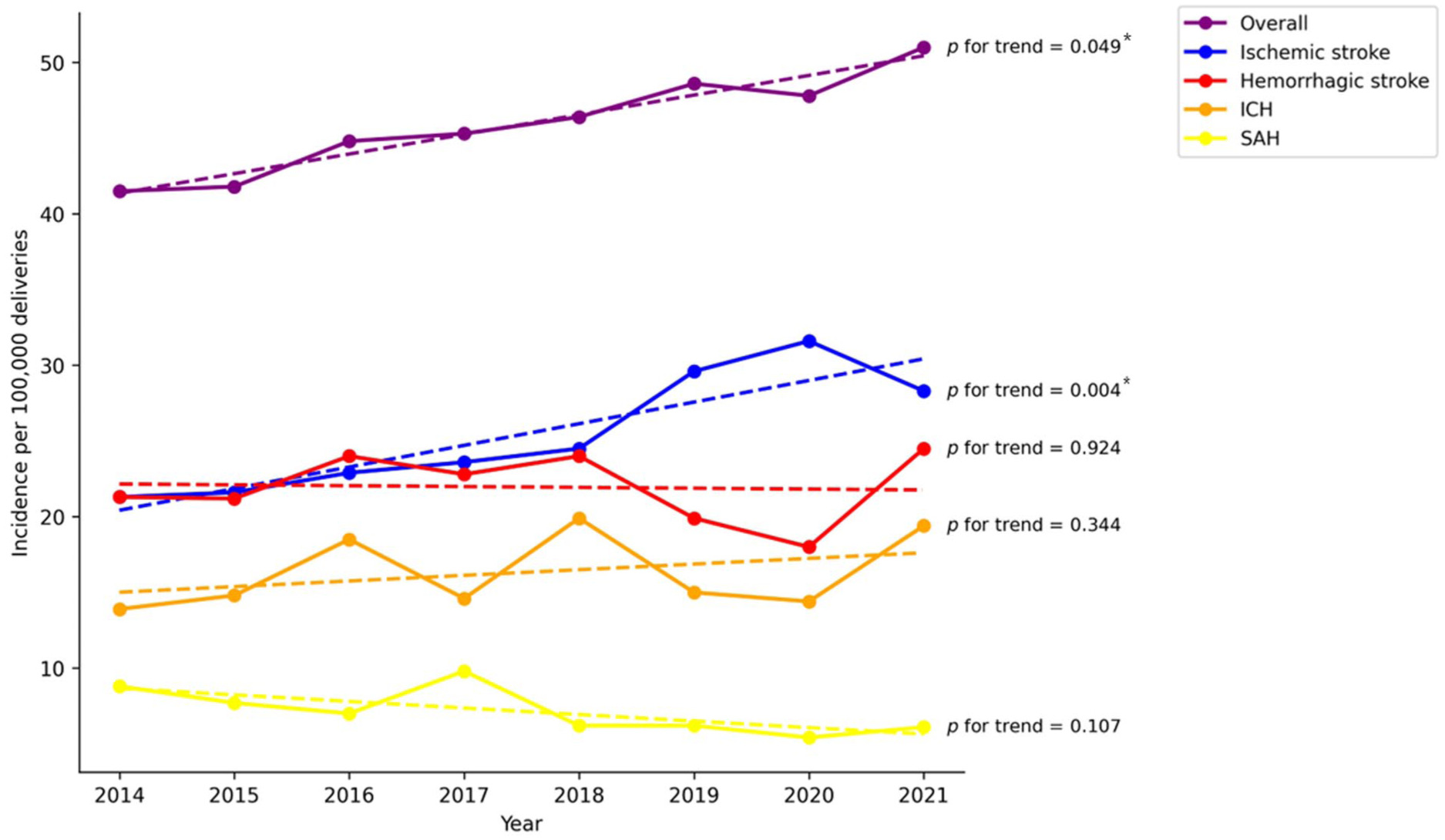
Temporal trends in the incidence of pregnancy-associated stroke. ICH, intracerebral hemorrhage; SAH, subarachnoid hemorrhage. Hemorrhagic stroke comprises ICH and SAH.
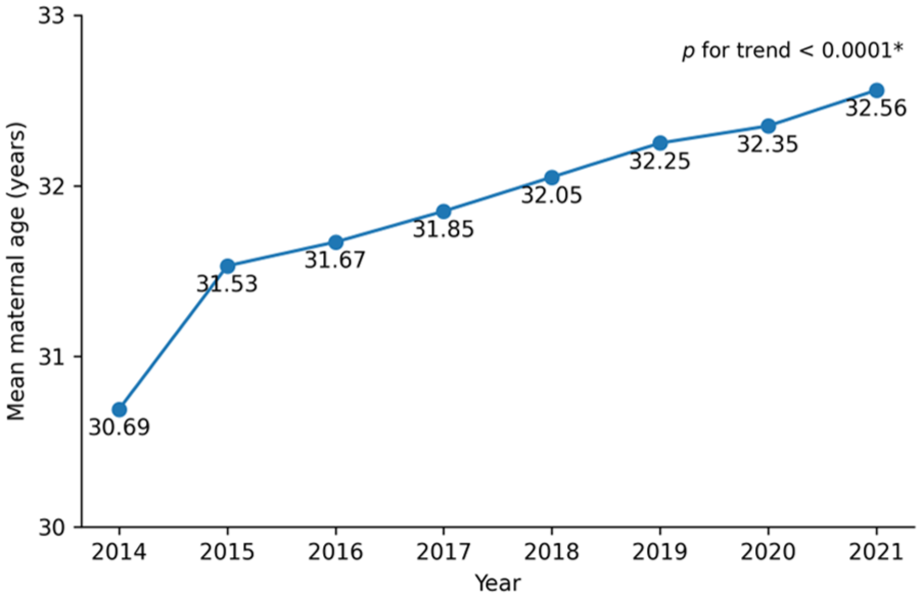
Mean maternal age from 2014 to 2021.
Incidence by age and pregnancy period
The incidence of PAS generally increased with maternal age, except among women aged 18–24 years (Figure 4). Overall incidence rose from 34.7 per 100,000 deliveries in women aged 25–29 years to 87.9 in those aged ⩾40 years (p for trend < 0.0001). A similar age-related pattern was observed across stroke subtypes. The incidence of ischemic stroke increased from 19.0 to 45.9 per 100,000 deliveries, that of ICH from 13.6 to 32.8, and that of SAH from 4.4 to 21.0 when comparing women aged ⩾40 years with those aged 25–29 years (p < 0.0001, p = 0.0003, and p < 0.0001, respectively).
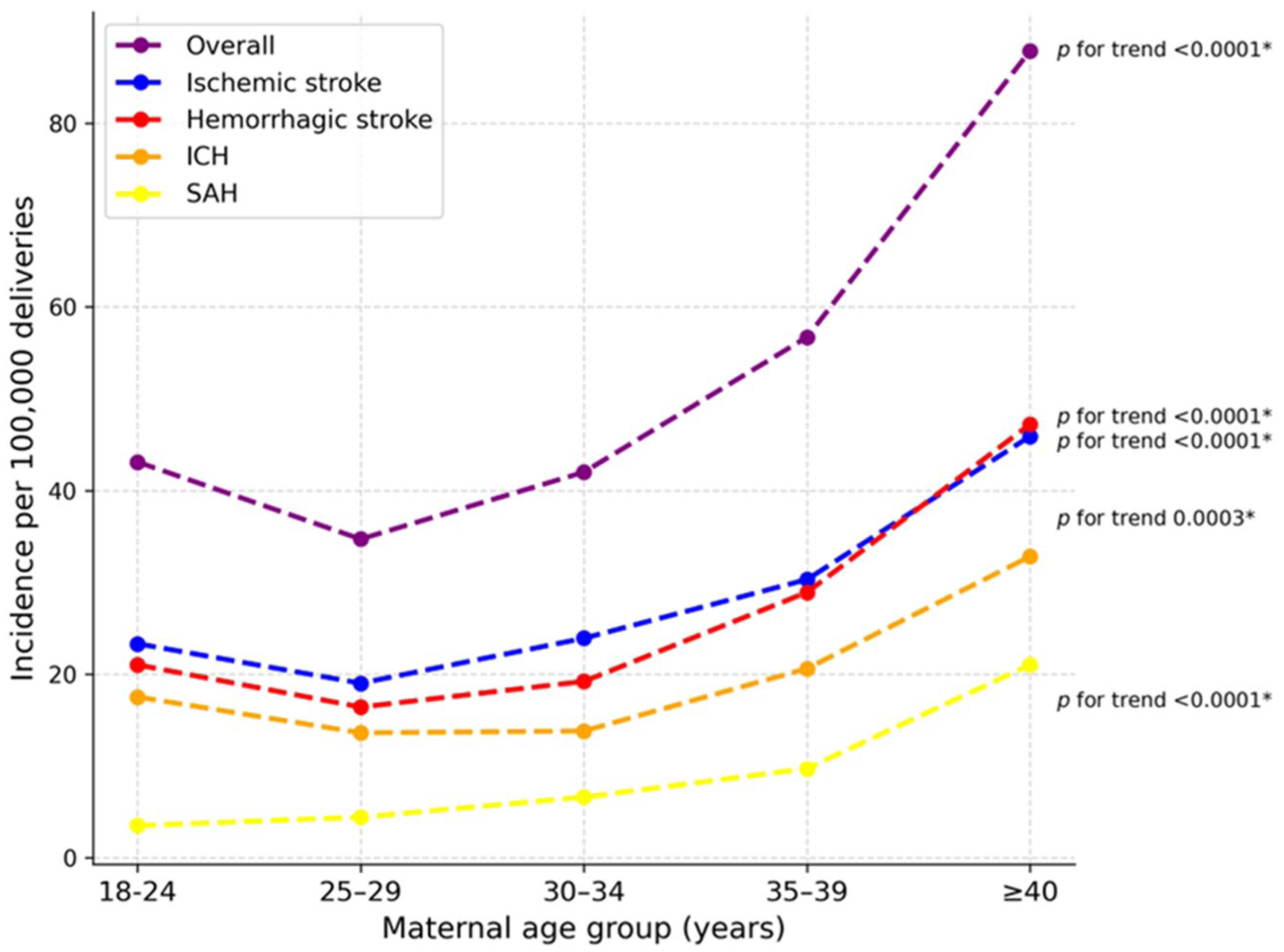
Age-specific incidence of pregnancy-associated stroke. ICH, intracerebral hemorrhage; SAH, subarachnoid hemorrhage. Hemorrhagic stroke comprises ICH and SAH.
The incidence of PAS varied by pregnancy period (Figure 5). Across all stroke subtypes, incidence was significantly higher during the first 6 weeks postpartum than during pregnancy trimesters (all p < 0.0001).
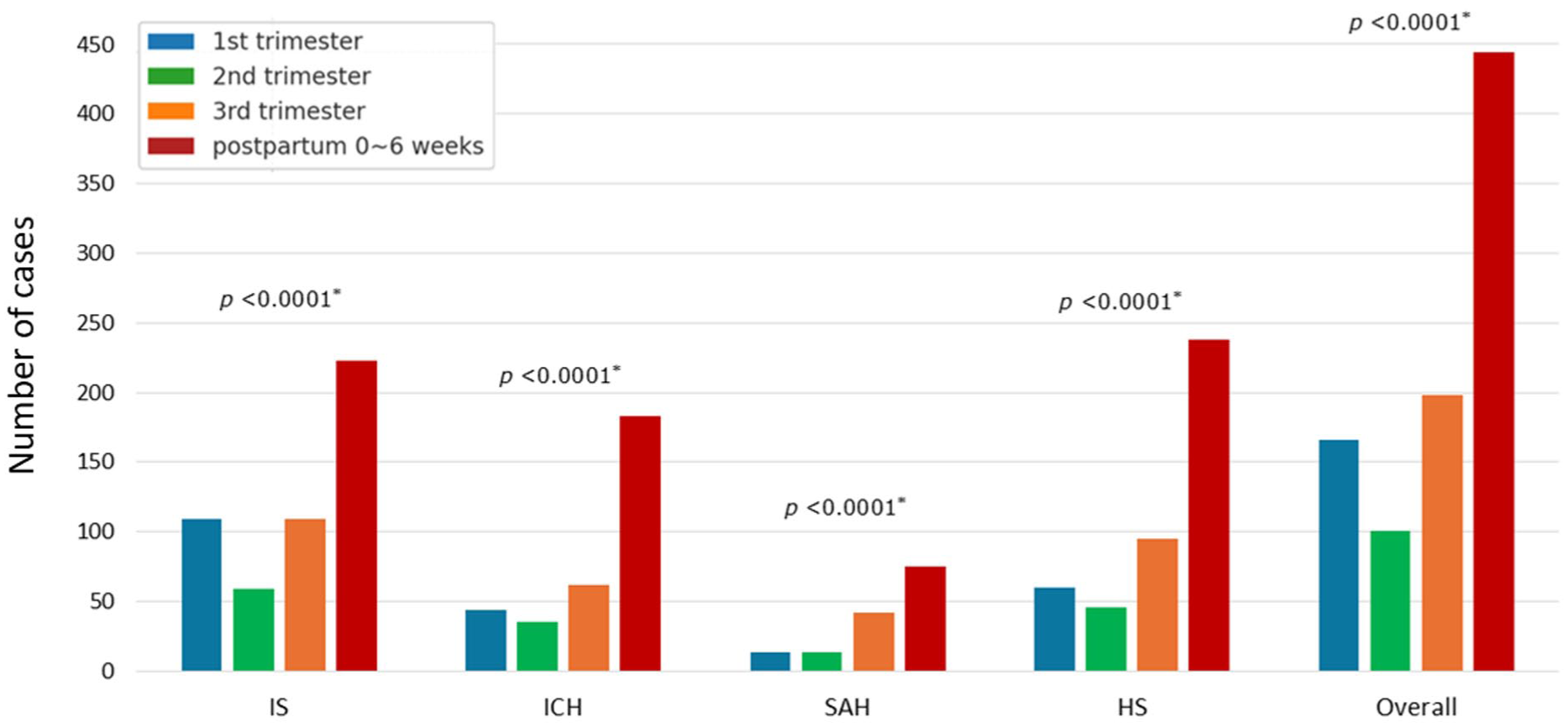
Distribution of pregnancy-associated stroke across the pregnancy trimesters and the postpartum period. IS, ischemic stroke; ICH, intracerebral hemorrhage; SAH, subarachnoid hemorrhage; HS, hemorrhagic stroke. HS comprises ICH and SAH.
Clinical characteristics and risk factor analyses
The characteristics of women with and without PAS are summarized in Table 1. Women with PAS were older than those without PAS (mean age, 33.1 ± 4.6 vs 32.0 ± 4.3 years; p < 0.0001), with a higher proportion aged ⩾35 years. Vascular risk factors were more prevalent among women with PAS, including hypertension (7.6% vs 2.0%, p < 0.0001), diabetes mellitus (7.3% vs 3.9%, p < 0.0001), hyperlipidemia (28.9% vs 19.2%, p < 0.0001), and smoking (10.5% vs 8.3%, p = 0.022). Body mass index (BMI) was also higher in the PAS group (23.1 ± 4.1 vs 22.7 ± 3.8 kg/m², p = 0.003). Cardiac conditions, including atrial fibrillation (0.6% vs 0.1%, p = 0.001) and ischemic heart disease (3.6% vs 1.8%, p < 0.0001), were more common among women with PAS. In addition, migraine (15.2% vs 9.1%, p < 0.0001), systemic lupus erythematosus (1.4% vs 0.5%, p < 0.0001), and antiphospholipid antibody syndrome (0.7% vs 0.3%, p = 0.033) were more frequent in the PAS group.
Characteristics of women with and without pregnancy-associated stroke.
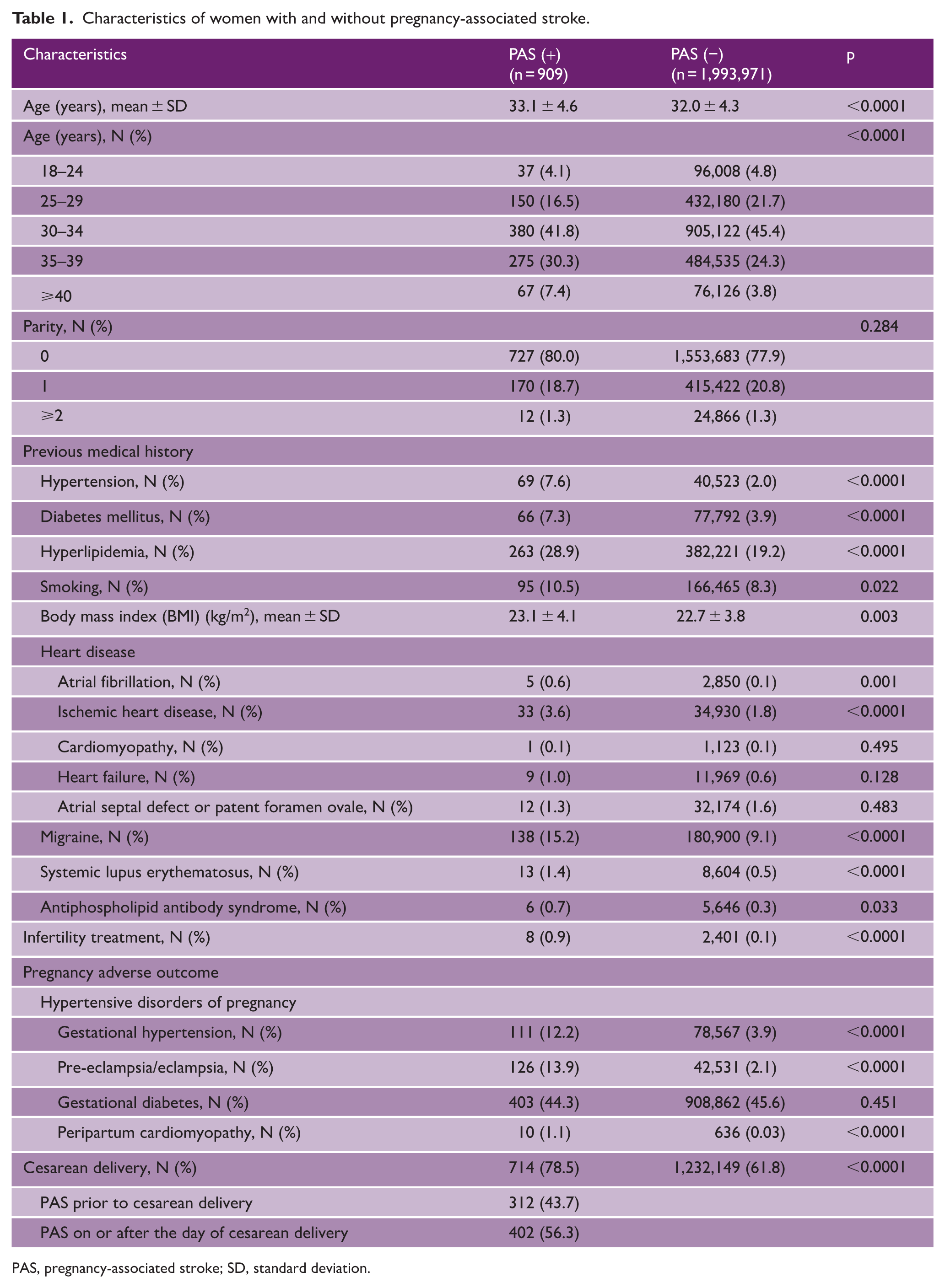
PAS, pregnancy-associated stroke; SD, standard deviation.
Women with PAS had higher rates of infertility treatment than those without PAS (0.9% vs 0.1%, p < 0.0001). Hypertensive disorders of pregnancy were more common among women with PAS, including gestational hypertension (12.2% vs 3.9%, p < 0.0001) and pre-eclampsia/eclampsia (13.9% vs 2.1%, p < 0.0001). PPCM was also more prevalent in the PAS group (1.1% vs 0.03%, p < 0.0001), whereas the prevalence of gestational diabetes did not differ between groups. Cesarean delivery was more frequent among women with PAS (78.5% vs 61.8%, p < 0.0001). Specifically, 43.7% of PAS occurred prior to cesarean delivery, whereas 56.3% occurred on or after the day of the procedure.
Factors that differed significantly between women with and without PAS in Table 1 were further analyzed, and their associations with PAS are presented as ORs in Table 2. After adjustment for age, several maternal factors remained significantly associated with PAS, including hypertension (OR, 3.60; 95% CI, 2.81–4.62), diabetes mellitus (OR, 1.80; 95% CI, 1.40–2.32), hyperlipidemia (OR, 1.64; 95% CI, 1.42–1.90), smoking (OR, 1.29; 95% CI, 1.04–1.60), BMI (per 1 kg/m² increase: OR, 1.08; 95% CI, 1.03–1.13), atrial fibrillation (OR, 3.76; 95% CI, 1.56–9.06), and ischemic heart disease (OR, 2.05; 95% CI, 1.45–2.90). Migraine (OR, 1.79; 95% CI, 1.49–2.14) and systemic lupus erythematosus (OR, 2.81; 95% CI, 1.62–4.86) also remained significant. Among pregnancy-related factors, infertility treatment (OR, 3.89; 95% CI, 1.94–7.80), gestational hypertension (OR, 3.23; 95% CI, 2.65–3.95), pre-eclampsia/eclampsia (OR, 6.91; 95% CI, 5.71–8.36), PPCM (OR, 32.20; 95% CI, 17.18–60.36), and cesarean delivery (OR, 2.15; 95% CI, 1.83–2.53) were significantly associated with PAS.
Associations between maternal characteristics and pregnancy-associated stroke.
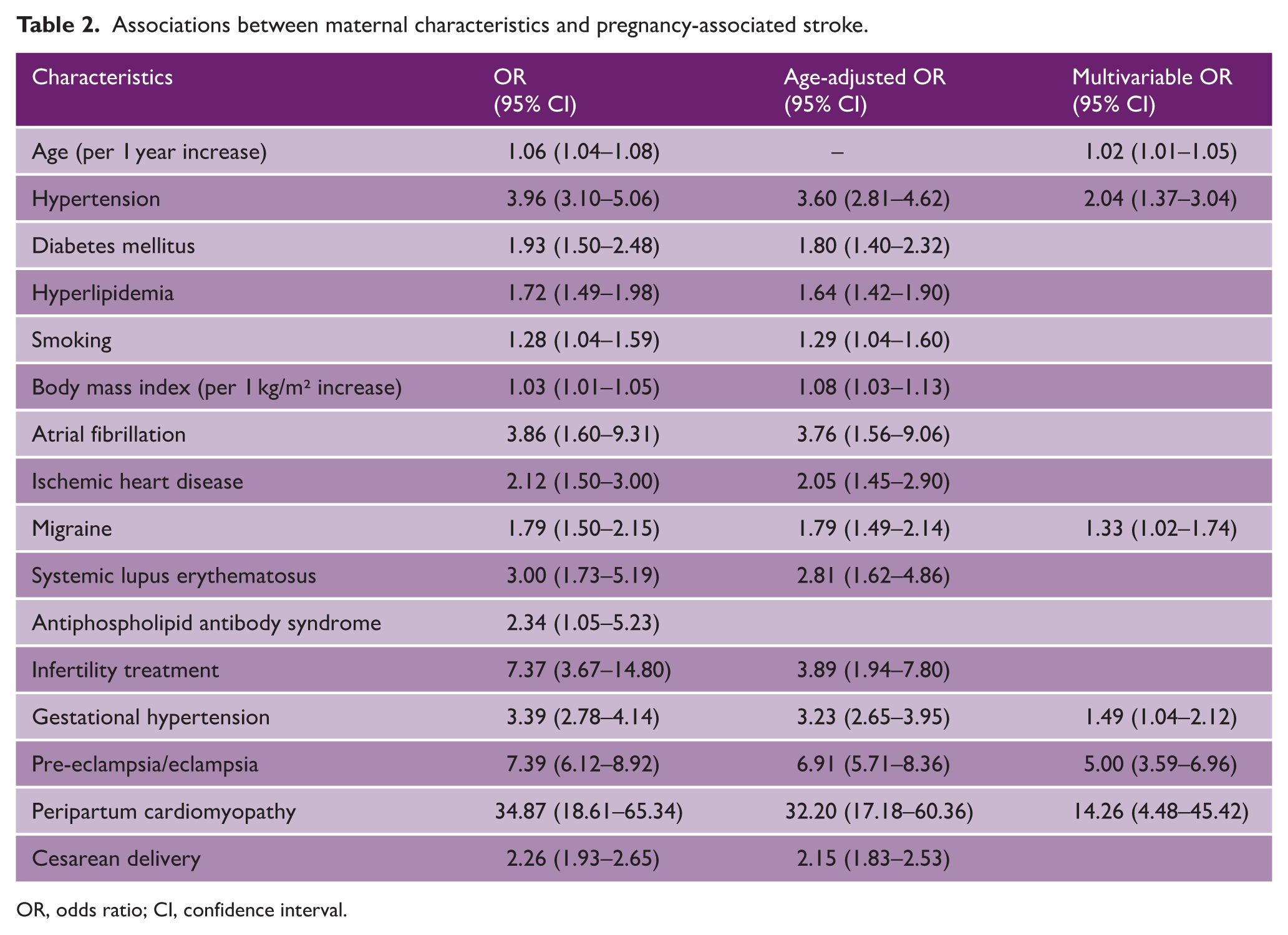
OR, odds ratio; CI, confidence interval.
To further identify independent associations, these factors were included in a multivariable model. In the multivariable analysis, maternal age (OR per year, 1.02; 95% CI, 1.01–1.05), hypertension (OR, 2.04; 95% CI, 1.37–3.04), and migraine (OR, 1.33; 95% CI, 1.02–1.74) remained significantly associated with PAS. Among pregnancy-related factors, gestational hypertension (OR, 1.49; 95% CI, 1.04–2.12), pre-eclampsia/eclampsia (OR, 5.00; 95% CI, 3.59–6.96), and PPCM (OR, 14.26; 95% CI, 4.48–45.42) remained strong independent predictors of PAS.
Discussion
In this nationwide study in South Korea, the PAS incidence was 45.6 per 100,000 deliveries and increased significantly from 41.5 in 2014 to 51.0 in 2021, primarily driven by ischemic stroke. Previous studies have reported a wide range of PAS incidence estimates across studies. 2 Focusing on large-scale nationwide studies, reported PAS incidence is approximately 42 per 100,000 in the United States (2007–2015), 3 24 in France (2010–2018), 8 21.5 in Taiwan (1999–2003), 16 14.5 in Finland (1987–2016), 7 and 13.4 in Canada (2003–2016). 4 Overall, the incidence observed in our study was higher than that reported in most other countries.
Several factors may explain the relatively high incidence of PAS in our study. Differences in study periods are likely an important contributor, as many previous studies have demonstrated increasing temporal trends in PAS incidence.4,7–9,17 For example, a Finnish nationwide study reported more than a twofold increase, from 11.1 per 100,000 deliveries in 1987–1991 to 25.2 in 2012–2016. 7 The use of more recent data (2014–2021) in our study may therefore partly account for the higher incidence observed.
Our relatively high observed incidence, together with the increasing PAS incidence reported in most studies, may largely reflect the rising maternal age in recent years. This upward trend in maternal age was also evident in our cohort. Maternal age is the most important nonmodifiable risk factor for both stroke and PAS. Across most OECD countries, the average age at childbirth has increased, and South Korea had the highest mean maternal age among OECD countries in 2022, exceeding 33 years. 11 The maternal population in our study was generally older than those in previous studies from other countries. In the US study with a PAS incidence most similar to ours, the median age was 30 years among PAS cases and 28 years among non-PAS cases. 3 In the Finnish study, the mean age of PAS cases was 31.2 years 7 ; in the French study, PAS and non-PAS cases had mean ages of 31.7 and 29.9 years, respectively. 8 By comparison, the mean maternal age in our study was 33.1 years among PAS cases and 32.0 years among non-PAS cases, indicating that the overall maternal population was approximately 2–3 years older than that reported in other countries. Maternal age remained an independent risk factor for PAS in our study. Advanced maternal age may increase PAS risk through multiple mechanisms, including a greater burden of vascular risk factors, increased susceptibility to pregnancy-related complications, and a higher likelihood of infertility treatment or cesarean delivery.
In addition to maternal age, established stroke risk factors—including hypertension, diabetes, hyperlipidemia, smoking, and higher BMI—along with pre-existing cardiac and autoimmune conditions, were associated with an increased risk of PAS. After adjustment for maternal age, most factors remained significant, indicating age-independent contributions to PAS risk, even among younger women. In the fully adjusted model, migraine, along with hypertension, emerged as a key pre-existing maternal condition, highlighting the need for attention to PAS in pregnant women with migraine. This association has been reported previously,18–20 and may involve shared mechanisms such as endothelial dysfunction, altered cerebral autoregulation, and prothrombotic states.1,20,21 A previous study found that hypertensive disorders mediated approximately 25% of the association between migraine and PAS, suggesting an important role for hypertensive disorders as well as the involvement of additional mechanisms beyond hypertension. 22
Although the factors analyzed are interrelated, the most influential predictors of PAS were hypertensive disorders of pregnancy—particularly pre-eclampsia/eclampsia—and PPCM. Pregnancy may be viewed as a cardiovascular stress test that unmasks underlying or subclinical cardiovascular vulnerability, with hypertensive disorders of pregnancy and PPCM representing clinical manifestations of this vulnerability. Pre-eclampsia/eclampsia is a well-established risk factor for PAS and is associated with systemic endothelial dysfunction, hypertension, and a hypercoagulable state. PPCM is characterized by impaired cardiac function around delivery, with most cases occurring postpartum. 23 It is associated with hormonal fluctuations in late pregnancy and at delivery that disrupt cardiovascular homeostasis and may increase stroke risk through hemodynamic instability and thromboembolism.23,24 In a multinational PPCM registry, stroke occurred in 3% of patients within 6 months. 25 A meta-analysis found a 22% pre-eclampsia prevalence among women with PPCM—fourfold higher than the 5% global background rate—suggesting shared pathophysiological mechanisms. 26 Careful monitoring and timely management of these complications are crucial for reducing PAS risk. However, the wide 95% CI for PPCM in our study likely reflects its low incidence, and reliance on diagnostic codes may have resulted in missed PPCM cases and underestimation of its true incidence.
As maternal age increases, the use of infertility treatment and cesarean delivery also rises. Although these factors may reflect a high-risk group, particularly women of advanced age, they remained significant predictors of PAS after age adjustment, suggesting that these interventions may contribute to PAS risk. Recent studies have reported an increased risk of stroke following infertility treatment, potentially related to endothelial dysfunction, hypercoagulability, heightened cardiovascular stress, or the possibility that subfertility itself reflects underlying maternal cardiovascular risk.27,28 Cesarean delivery may similarly increase stroke risk through transient hemodynamic changes or hypercoagulability, and a nationwide Taiwanese study identified it as an independent risk factor for postpartum stroke. 29 In our cohort, more than half of PAS cases occurred on or after the day of cesarean delivery, whereas a substantial proportion preceded the procedure. These findings suggest that both the clinical context leading to cesarean delivery and perioperative factors may be relevant to this temporal pattern. When interpreting our findings, it is important to note that cesarean delivery is relatively common in South Korea, exceeding 60% even among women without PAS. This high rate likely reflects not only advanced maternal age and increased use of assisted reproductive technologies, but also maternal and physician preferences within the Korean healthcare context. 30
Both ischemic and hemorrhagic strokes were more frequent postpartum than antepartum, consistent with previous studies.5,7,31,32 Pregnancy induces a hypercoagulable state, 33 potentially exacerbated by delivery-related vascular injury, inflammation, infection, and abrupt hormonal changes. This pronounced postpartum hypercoagulability likely contributes to the increased risk of venous thromboembolism, 34 cerebral venous sinus thrombosis, 35 and PAS.5,7,31,32 Hemodynamic and vascular changes around delivery may increase stroke risk, as blood pressure can rise abruptly during labor and remain unstable postpartum, particularly in women with pre-eclampsia/eclampsia. Rapid postpartum hormonal changes may also reduce vascular elasticity and promote vasoconstriction and hypertension, contributing to the high postpartum incidence of pregnancy-associated cerebral artery dissection 36 and hemorrhagic stroke. 31 Given the high postpartum incidence of PAS, careful monitoring after delivery is warranted, especially in high-risk women.
This is the first nationwide study of PAS in South Korea; however, several limitations should be considered. First, the observational design limits causal inference, and residual confounding by unmeasured variables may persist despite adjustment. Second, although a prior validation study of stroke outcomes in the NHIS database demonstrated acceptable reliability, 37 the use of administrative claims data may still have resulted in some misclassification of PAS cases due to incomplete or inaccurate diagnostic coding, including stroke mimics. Third, our dataset did not capture pregnancies ending in spontaneous or induced abortion. In addition, individual-level analyses were not possible because the NHIS data were de-identified and lacked detailed clinical information, including stroke subtype, imaging findings, and severity. Future prospective studies incorporating comprehensive clinical data are therefore needed. Finally, because the data were derived exclusively from South Korea, the generalizability of these findings may be limited. This may reflect the relative racial and ethnic homogeneity of the Korean population and the unique features of the Korean healthcare system. The near-universal coverage of the Korean NHIS and the high availability and utilization of magnetic resonance imaging (MRI) in South Korea, 38 may further increase the sensitivity of case detection.
In conclusion, this first nationwide population-based study of PAS in South Korea found an incidence of 45.6 per 100,000 deliveries—higher than that reported in most other countries—with a significant increase over an 8-year period, mainly driven by ischemic stroke. PAS occurred most frequently in the postpartum period. Advanced maternal age, hypertension, migraine, and pregnancy-related complications, including gestational hypertension, pre-eclampsia/eclampsia, and PPCM, were strong independent predictors of PAS. These findings highlight the importance of clinical awareness and the identification of women at high risk of PAS.
Supplemental Material
sj-docx-1-wso-10.1177_17474930261435194 – Supplemental material for Stroke during pregnancy and the postpartum period: A nationwide population-based study in South Korea
Supplemental material, sj-docx-1-wso-10.1177_17474930261435194 for Stroke during pregnancy and the postpartum period: A nationwide population-based study in South Korea by Darda Chung, Byung-Ryong Ahn, Cheryl D Bushnell, Je Yeon Lee, Heejung Mo, Hee-Kwon Park, Joung-Ho Rha and Cindy W Yoon in International Journal of Stroke
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Inha University Research Grant (no. 74085-1) and the Inha University Hospital Research Grant.
Data availability statement
The data that support the findings of this study are available from the Korean NHIS. Restrictions apply to the availability of these data, which were used under license for the current study. Data are available from the NHIS upon reasonable request and with permission of the NHIS.
Supplemental material
Supplemental material for this article is available online.