
Abstract
Background:
Covert brain infarction is a common neuroimaging-defined manifestation of covert cerebrovascular disease and is associated with increased risks of future stroke and cognitive decline. Covert brain infarction has been included as an outcome in randomized trials evaluating coagulation-pathway-targeting strategies. However, whether these strategies consistently reduce incident covert brain infarction and whether treatment effects on covert brain infarction parallel those for acute ischemic stroke remain uncertain.
Methods:
Following PRISMA 2020 guidelines, we searched PubMed, Ovid MEDLINE, Embase, and Web of Science through 10 November 2025, for randomized controlled trials and magnetic resonance imaging substudies enrolling patients without an established indication for anticoagulation. Eligible trials compared antithrombotic strategies targeting the coagulation pathway (oral anticoagulation or direct factor inhibition, with or without background antiplatelet therapy) with antiplatelet-based regimens and reported incident covert brain infarction on follow-up magnetic resonance imaging. Trial-level treatment effects for covert brain infarction, acute ischemic stroke, and their composite were compared. Exploratory cross-outcome comparisons were performed using the ratio of relative risks with prespecified interpretability bounds.
Results:
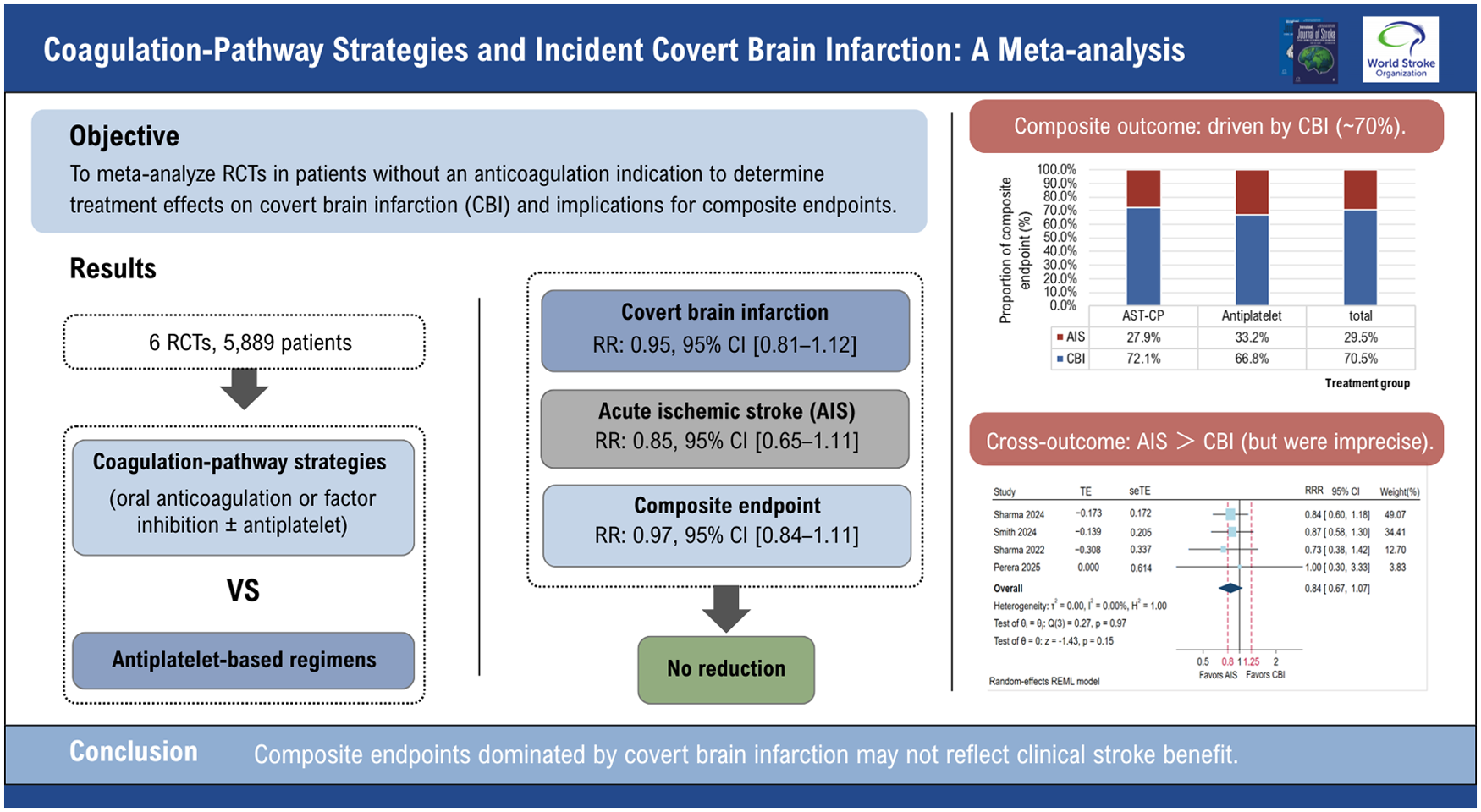
Six randomized trials met the inclusion criteria, encompassing diverse clinical populations and varying antiplatelet regimens in the control arms. In stratified analyses according to treatment structure, coagulation-pathway strategies were not associated with a statistically significant reduction in incident covert brain infarction compared with antiplatelet therapy alone, with similar estimates across treatment strata and no evidence of interaction (P_interaction = 0.249). An exploratory pooled estimate was similar (risk ratio, 0.95; 95% confidence interval, 0.81–1.12). Findings were consistent across covert brain infarction subtypes, including lacunar and non-lacunar lesions. In trials reporting all three outcomes, these strategies were not associated with significant reductions in covert brain infarction, acute ischemic stroke (risk ratio, 0.85; 95% confidence interval, 0.65–1.11), or their composite endpoint (risk ratio, 0.97; 95% confidence interval, 0.84–1.11). The composite endpoint was predominantly driven by covert brain infarction (~70% of events). Exploratory cross-outcome comparisons yielded point estimates favoring acute ischemic stroke over covert brain infarction, although confidence intervals crossed unity.
Conclusion:
In clinical settings without a mandatory indication for anticoagulation, coagulation-pathway strategies were not associated with reduced incident covert brain infarction compared with antiplatelet therapy. Although effect estimates for covert brain infarction and acute ischemic stroke were broadly similar, uncertainty remains. Composite endpoints predominantly driven by covert brain infarction warrant cautious interpretation when inferring treatment effects on clinically manifest ischemic stroke.
Keywords
Background
Covert brain infarction (CBI) refers to ischemic brain lesions detected on neuroimaging, including magnetic resonance imaging (MRI) or computed tomography (CT), in the absence of corresponding acute neurological symptoms. 1 With the widespread use of MRI, CBI is increasingly identified in both clinical and research settings. 2 Population-based studies have shown that CBI is associated with increased risks of subsequent symptomatic stroke, cognitive decline, dementia, and mortality. 3
Given these clinical implications, CBI has increasingly been used as an imaging-defined outcome in randomized stroke prevention trials, either as a secondary endpoint or within composite outcomes alongside acute ischemic stroke (AIS). Including CBI in composite endpoints increases event rates and statistical power, and in several trials, incident CBI accounted for a substantial proportion of ischemic events. However, interpretation of such composite endpoints requires concordant treatment effects on imaging-defined CBI and clinically manifest AIS. Although the two conditions share vascular risk factors and lie along the same disease spectrum, their underlying mechanisms and clinical implications may differ. 4 If treatment effects differ between CBI and AIS, composite endpoints predominantly driven by CBI may not accurately reflect effects on clinically important stroke outcomes.5,6
In recent years, several randomized trials have evaluated antithrombotic strategies targeting the coagulation pathway (coagulation-pathway strategies) in high-risk populations without a clear indication for long-term anticoagulation. While these trials differ in patient populations and treatment regimens, several have reported incident CBI on follow-up neuroimaging, providing an opportunity to examine treatment effects on covert ischemic events across clinical contexts. Prior meta-analyses have shown that, among patients with AIS and no clear indication for anticoagulation, the addition of oral anticoagulation to standard antiplatelet therapy does not reduce the risk of recurrent AIS compared with antiplatelet therapy alone. 7
We conducted a systematic review and meta-analysis of randomized controlled trials reporting incident CBI to evaluate the association between coagulation-pathway strategies and CBI. Specifically, we aimed to (1) assess stratified and exploratory overall effects of coagulation-pathway strategies on incident CBI across trials with differing treatment intensities and (2) examine whether relative treatment effects were consistent between CBI and AIS, with implications for interpreting composite endpoints in which CBI constitutes a substantial proportion of events.
Methods
Protocol and reporting standards
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines. 8 The study protocol was prospectively registered in PROSPERO (CRD420251229186).
Search strategy and study selection
A comprehensive literature search was performed on 11 October 2025, in PubMed, Ovid MEDLINE, Embase, and Web of Science. Trial registries (ClinicalTrials.gov and the WHO International Clinical Trials Registry Platform) were also screened to identify completed or ongoing trials. The detailed search strategy is provided in the Supplemental Material (Supplemental Table S1). Records were imported into reference management software, and duplicates were removed. Two investigators (Y.F. and W.L.), both neurologists, independently screened titles, abstracts, and full texts. Discrepancies were resolved by consensus.
Eligibility criteria
We included randomized controlled trials enrolling patients without a mandatory long-term indication for anticoagulation (e.g. atrial fibrillation requiring therapeutic anticoagulation). Eligible trials compared antiplatelet therapy alone with coagulation-pathway strategies and reported incident CBI detected on follow-up MRI. We excluded observational studies, nonrandomized trials, narrative or systematic reviews, case series, and case reports. Trials focusing on perioperative or procedure-related infarcts were also excluded because such events are typically driven by acute procedural or surgical factors and differ mechanistically from spontaneous vascular brain infarction.
Outcomes
The primary outcome was incident CBI identified as new lesions on follow-up MRI. Coagulation-pathway strategies included therapeutic-dose oral anticoagulation as monotherapy and combination strategies administered on a background of antiplatelet therapy, including factor XI inhibition and low-dose factor Xa inhibition. Control arms consisted of single antiplatelet therapy, although specific agents and doses varied across trials.
Primary analyses evaluated relative treatment effects in stratified analyses according to the type of coagulation-pathway strategy and background antiplatelet use, with tests for interaction to assess differences between strata. An exploratory pooled analysis was performed to estimate the overall treatment effects on incident CBI. Additional analyses explored heterogeneity of treatment effects across CBI subtypes, including lacunar versus non-lacunar infarctions when reported. Secondary analyses examined the consistency of treatment effects on CBI and AIS. Safety outcomes included symptomatic intracranial hemorrhage and all-cause mortality as defined in each trial. Sensitivity analyses included exclusion of trials enrolling non-stroke populations and exclusion of trials judged to be at high risk of bias.
MRI populations and analytical data sets
For the primary analysis of incident CBI, effect estimates were derived from participants who completed both baseline and follow-up MRI, reflecting the imaging-defined populations reported in the included trials. Where available, incident CBI was further classified as lacunar or non-lacunar according to definitions used in the original trials. Given heterogeneity in imaging criteria across studies, subtype analyses were conducted using trial-specific classifications without redefinition (Supplemental Table S2). For analyses comparing treatment effects across incident CBI, AIS, and their composite endpoint, we included trials that concurrently reported all three outcomes. These data were typically derived from intention-to-treat populations, with trial-specific handling of missing MRI data, including imputation where applicable.
Statistical analysis
Treatment effects were summarized as risk ratios (RRs) with corresponding 95% confidence intervals (CIs). Meta-analyses were performed using random-effects models to account for potential clinical and methodological heterogeneity across trials. For outcomes with zero events in one or both study arms, a continuity correction of 0.5 was applied. Statistical heterogeneity was assessed using Cochran’s Q test and quantified with the I2 and τ2 statistics, which were interpreted descriptively.
Stratified meta-analyses were conducted according to the type of coagulation-pathway strategy and background antiplatelet use, and differences between strata were evaluated using tests for interaction. An exploratory pooled meta-analysis was performed to estimate the overall treatment effect on incident CBI across all trials. Subgroup analyses further examined treatment effects across CBI subtypes (lacunar versus non-lacunar) when subtype-specific outcomes were reported.
To formally compare relative treatment effects across different outcome definitions, cross-outcome comparisons were conducted in trials reporting incident CBI, AIS, and their composite outcomes. Relative treatment effects were compared using the ratio of risk ratio (RRR), defined as the ratio of the RR for AIS to that for incident CBI. An RRR < 1.0 indicated a greater relative treatment effect for AIS than for CBI, whereas an RRR > 1.0 indicated a greater effect for CBI. Within-trial correlation between AIS and CBI effect estimates was accounted for under prespecified assumptions; detailed formulae and correlation sensitivity analyses are provided in the Supplemental Methods. 9 Trial-level logRRR estimates were pooled using random-effects meta-analysis with restricted maximum likelihood estimation.
Beyond statistical differences, we assessed whether relative treatment effects across outcome definitions were sufficiently similar to support direct clinical interpretability. We prespecified bounds corresponding to a ±25% relative difference (RRR, 0.80–1.25; logRRR, −0.223 to 0.223). 10 This range was intended as a pragmatic threshold to facilitate interpretation of similarities in relative treatment effects rather than to define a formal equivalence margin. To facilitate interpretation of cross-outcome comparisons, we examined whether the 95% CI of the pooled RRR fell within the prespecified reference range using a confidence interval containment approach. In addition, directional consistency of treatment effects across AIS and CBI was examined at the trial level (definition provided in the Supplement Methods).11,12 To further illustrate the contribution of individual components to the composite outcome, stacked bar charts were used to display the proportions of CBI and AIS.
Publication bias for the primary outcome was assessed by visual inspection of funnel plots and by Egger’s regression test for small-study effects. Prespecified sensitivity analyses included exclusion of the trial enrolling non-stroke populations, stratification by antithrombotic strategy, and exclusion of one trial with a higher proportion of potential cardioembolic sources in analyses of non-lacunar CBI. Risk of bias was assessed using the Cochrane risk-of-bias tool (RoB 2). 13 All analyses were performed using Stata version 18 (StataCorp).
Results
Study selection and trial characteristics
A total of 4929 records were identified through systematic database searches. After removal of duplicates and screening of titles and abstracts, 79 full-text articles were assessed for eligibility, of which six randomized controlled trials met the inclusion criteria and were included in the final meta-analysis (Figure 1). Searches of trial registries did not identify additional eligible studies. Publication bias assessment is presented in Supplemental Figure S1. Funnel plot inspection did not suggest substantial asymmetry (Supplemental Figure S2). Egger’s regression test did not indicate statistically significant small-study effects (β = −1.62, SE = 0.995, p = 0.10), noting that such assessments are limited when fewer than 10 studies are available.
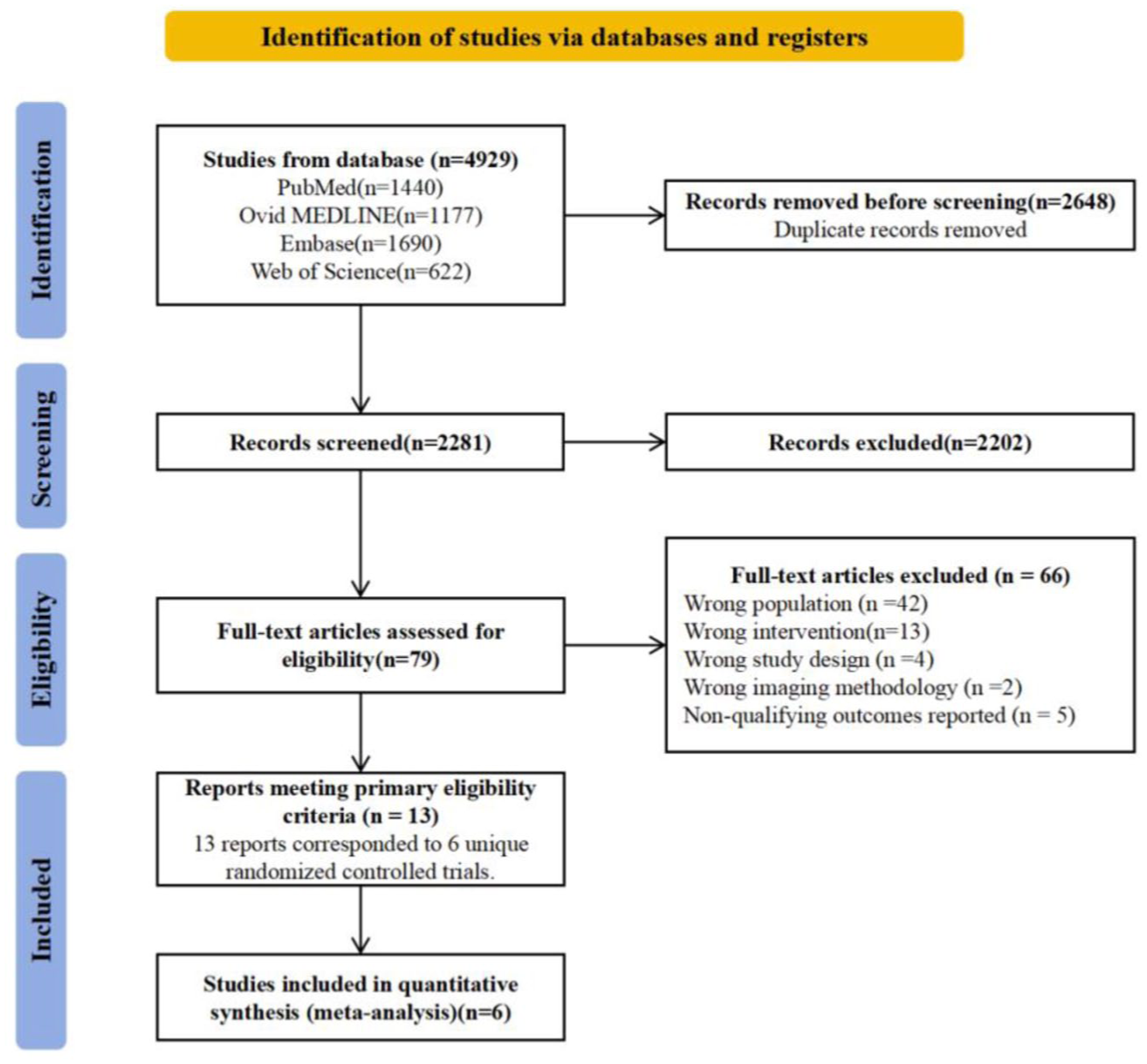
Flow diagram of study selection.
The six included trials differed in clinical setting, timing of randomization, and background risk profiles. Five trials were conducted in secondary stroke prevention populations with varying stroke subtypes, while one enrolled patients with stable atherosclerotic vascular disease. Antithrombotic strategies targeting the coagulation pathway also varied across trials. Two trials evaluated therapeutic-dose oral anticoagulation as monotherapy. The remaining trials investigated pharmacologic inhibition of the coagulation pathway administered on a background of antiplatelet therapy, including factor XI inhibition and low-dose factor Xa inhibition. One trial had three arms, including therapeutic-dose oral anticoagulation alone, coagulation-pathway strategies administered on a background of antiplatelet therapy, and antiplatelet therapy alone. In the meta-analysis, this study contributed two pairwise comparisons. To avoid double-counting of participants in the shared antiplatelet control group, the control arm was split in accordance with standard meta-analytic methods. Control arms consisted of single antiplatelet therapy, although specific agents and doses differed across trials. These clinical and pharmacologic differences were addressed in prespecified stratified and exploratory analyses. All included trials incorporated a follow-up MRI to assess incident CBI.
Across the included trials, CBI was assessed among participants who completed follow-up MRI rather than the entire randomized population. Overall, the six included trials comprised 6001 patients who completed follow-up MRI. In one small trial (Perera et al. 14 ), 101 patients were randomized and 86 completed follow-up MRI; because the number of participants completing MRI in each treatment group was not reported and the sample size was limited, the randomized group size was used as the denominator for analysis. In another trial (Sharma et al. 6 ), 19 participants who completed follow-up MRI were excluded from the CBI analysis for reasons not explicitly specified. In two trials (Smith et al. 15 and Sharma et al. 16 ), participants who experienced symptomatic ischemic stroke during follow-up were excluded from the CBI analysis, resulting in the exclusion of 127 patients despite completion of follow-up MRI. In contrast, two trials (Sharma et al. 17 and Lansberg et al. 18 ) included all participants who completed follow-up MRI in the CBI analysis, regardless of whether a symptomatic stroke occurred. These differences in outcome ascertainment strategies contributed to the judgment of high risk of bias in one trial.
Based on the analytic populations reported by each trial, the primary CBI meta-analysis included 5889 participants. The main characteristics of the included trials are summarized in Table 1, and key features of CBI definitions and imaging protocols are summarized in Table 2.
Characteristics of randomized controlled trials selected for inclusion in the meta-analysis.
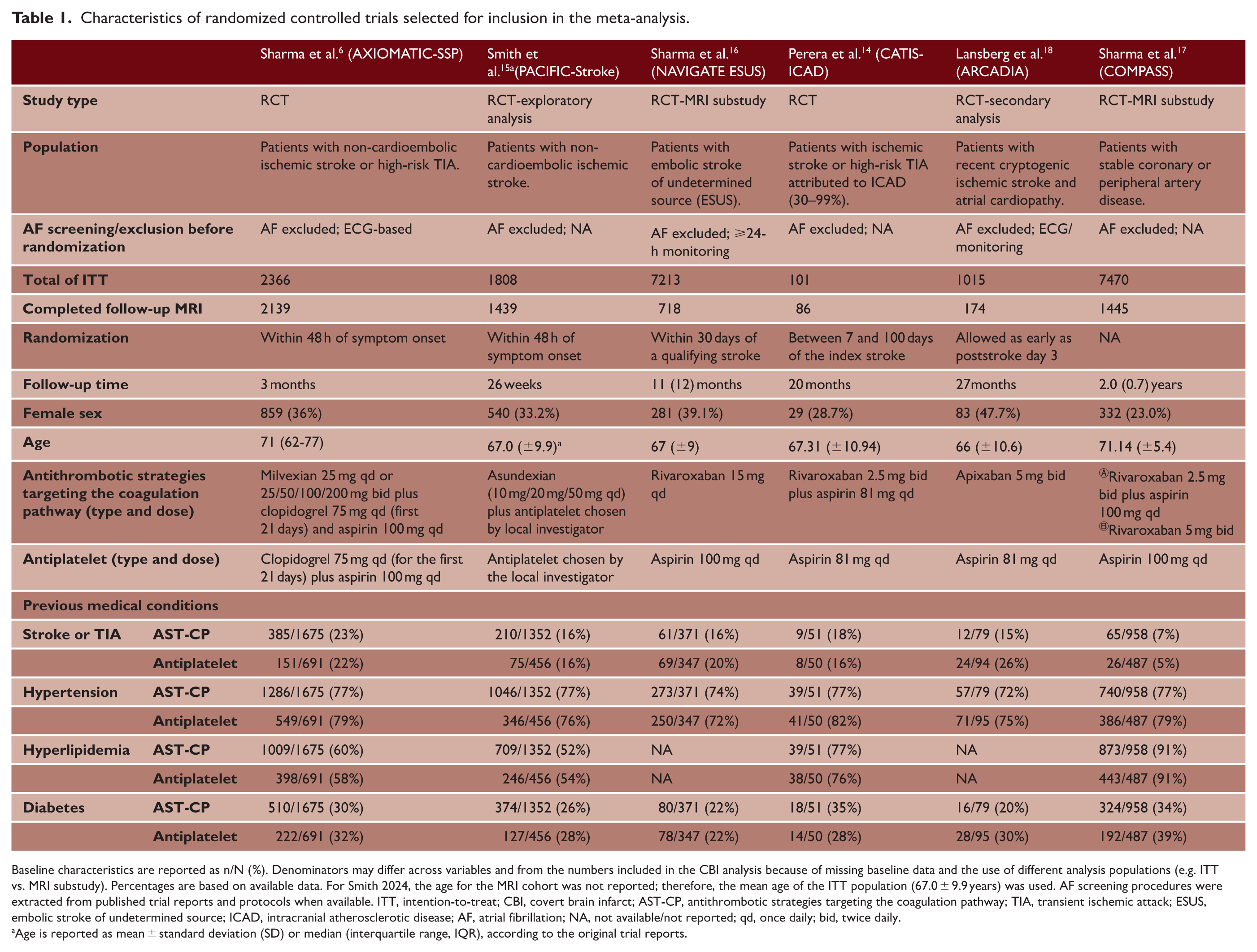
Baseline characteristics are reported as n/N (%). Denominators may differ across variables and from the numbers included in the CBI analysis because of missing baseline data and the use of different analysis populations (e.g. ITT vs. MRI substudy). Percentages are based on available data. For Smith 2024, the age for the MRI cohort was not reported; therefore, the mean age of the ITT population (67.0 ± 9.9 years) was used. AF screening procedures were extracted from published trial reports and protocols when available. ITT, intention-to-treat; CBI, covert brain infarct; AST-CP, antithrombotic strategies targeting the coagulation pathway; TIA, transient ischemic attack; ESUS, embolic stroke of undetermined source; ICAD, intracranial atherosclerotic disease; AF, atrial fibrillation; NA, not available/not reported; qd, once daily; bid, twice daily.
Age is reported as mean ± standard deviation (SD) or median (interquartile range, IQR), according to the original trial reports.
Trial-specific definitions of CBI and criteria for lacunar and non-lacunar subtypes.
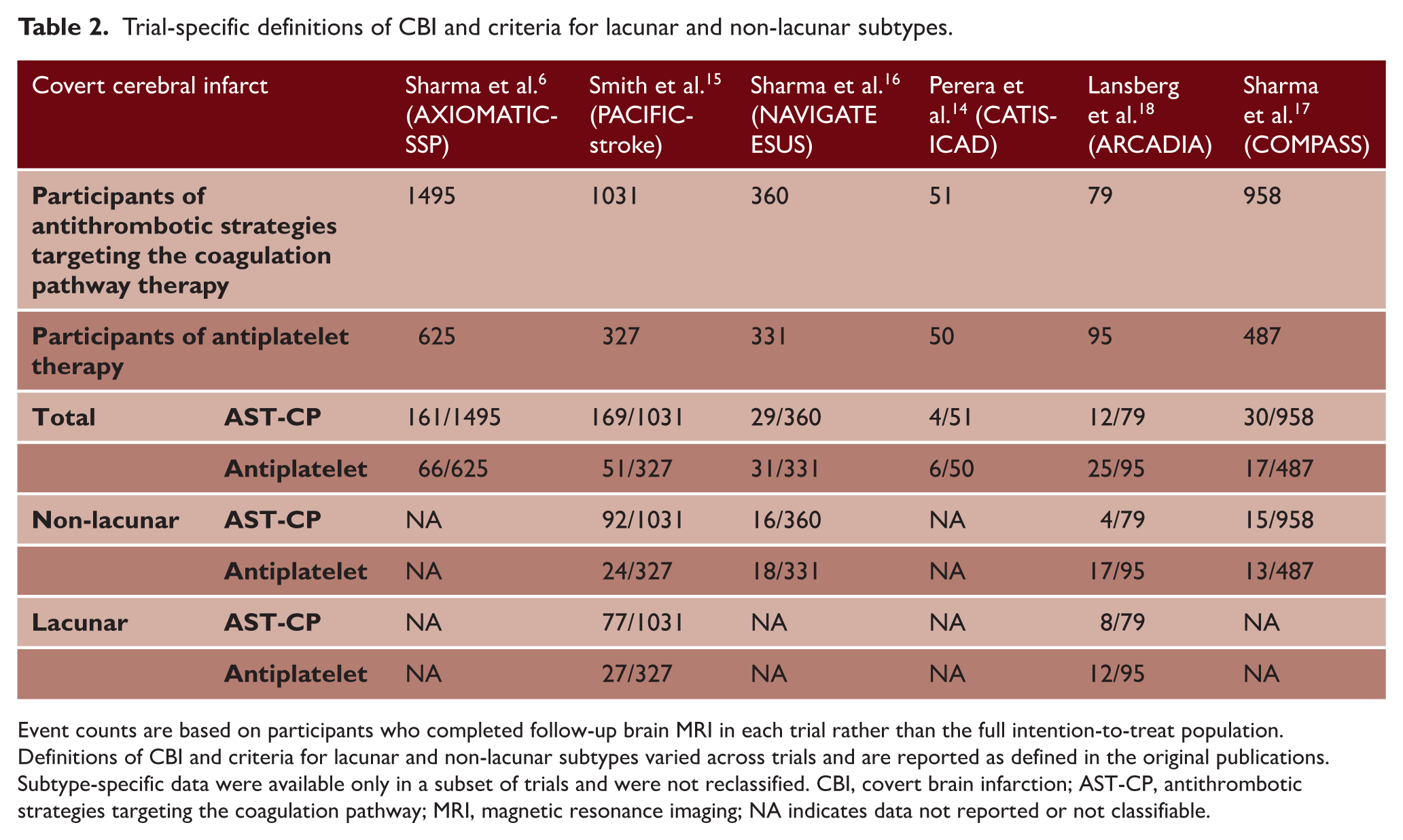
Event counts are based on participants who completed follow-up brain MRI in each trial rather than the full intention-to-treat population. Definitions of CBI and criteria for lacunar and non-lacunar subtypes varied across trials and are reported as defined in the original publications. Subtype-specific data were available only in a subset of trials and were not reclassified. CBI, covert brain infarction; AST-CP, antithrombotic strategies targeting the coagulation pathway; MRI, magnetic resonance imaging; NA indicates data not reported or not classifiable.
Incident CBI and subtype analyses
In prespecified stratified analyses, effect estimates were similar in direction and had overlapping CIs for full-dose oral anticoagulation alone (RR, 0.80; 95% CI, 0.58–1.12) and for low-dose factor Xa or factor XI inhibition in combination with antiplatelet therapy (RR, 1.00; 95% CI, 0.83–1.21), with CIs overlapping unity in both strata (Figure 2(a) and (b)). The test for interaction was not statistically significant (P_interaction = 0.249), providing no evidence of differential treatment effects between strategies. In exploratory pooled analyses, no statistically significant difference in incident CBI was observed between coagulation-pathway strategies and antiplatelet therapy (RR, 0.95; 95% CI, 0.81–1.12). Although the included trials varied in clinical setting and treatment intensity, statistical heterogeneity was negligible (I2 = 0%) (Figure 2(c)).
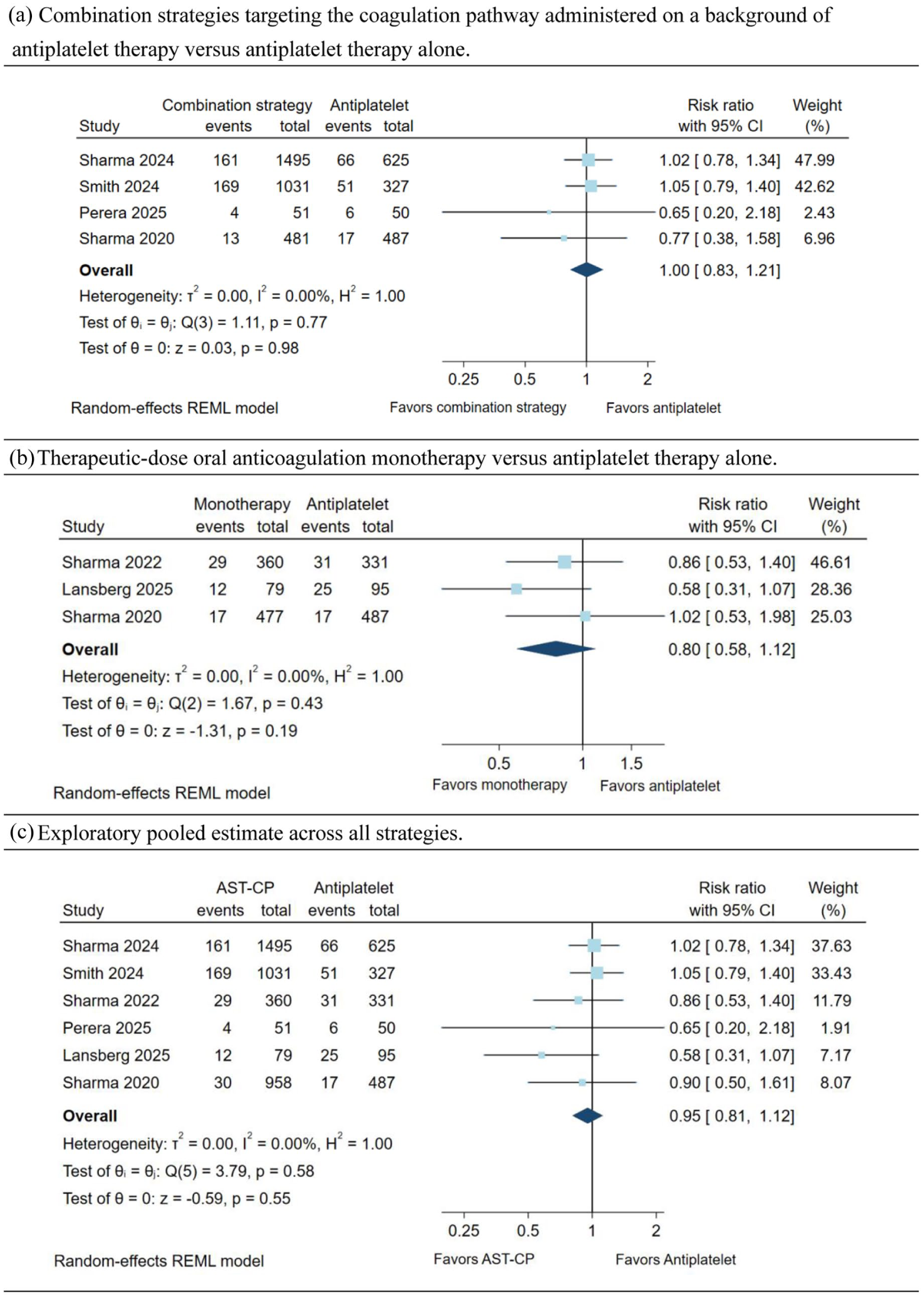
Effects of antithrombotic strategies targeting the coagulation pathway on incident covert brain infarction: Forest plot showing the effect of antithrombotic strategies targeting the coagulation pathway on incident CBI across included randomized trials. Because of clinical and pharmacologic heterogeneity across included trials, stratified analyses according to treatment structure were designated as the primary analyses: (a) Combination strategies targeting the coagulation pathway administered on a background of antiplatelet therapy versus antiplatelet therapy alone, (b) therapeutic-dose oral anticoagulation monotherapy versus antiplatelet therapy alone and (c) an exploratory pooled estimate across all strategies is shown to illustrate the overall direction of treatment effects. Effect estimates are expressed as risk ratios (RRs) with 95% confidence intervals (CIs). Pooled estimates were calculated using random-effects models. Incident CBI was defined based on follow-up magnetic resonance imaging in each trial. Between-study heterogeneity was assessed using the I2 statistic. AST-CP, antithrombotic strategies targeting the coagulation pathway; CBI, covert brain infarction; RR, risk ratio; CI, confidence interval.
Subgroup analyses were performed according to CBI subtype (Supplemental Figure S3). Among trials reporting non-lacunar CBI, coagulation-pathway strategies were not associated with a statistically significant reduction in incident lesions compared with antiplatelet therapy (RR, 0.72; 95% CI, 0.42–1.25). Exclusion of the trial with a high proportion of patients at elevated cardioembolic risk (Lansberg et al.) yielded similar results (RR, 0.91; 95% CI, 0.59–1.39; Supplemental Figure S4). Likewise, no significant difference was observed for lacunar CBI (RR, 0.88; 95% CI, 0.61–1.29).
Comparison across outcome definitions
To examine differences in treatment effect across imaging-defined and clinical outcomes, four randomized controlled trials reporting AIS, CBI, and a composite endpoint of AIS and CBI were included. The trials included in this analysis were conducted in populations with ischemic stroke without a mandatory indication for long-term anticoagulation. Across outcome definitions, no statistically significant differences in treatment effect were observed (Figure 3). Coagulation-pathway strategies were not associated with a statistically significant reduction in AIS (RR, 0.85; 95% CI, 0.65–1.11) or CBI (RR, 1.03; 95% CI, 0.86–1.22). Similarly, analysis of the composite endpoint comprising AIS and CBI yielded a neutral effect estimate (RR, 0.97; 95% CI, 0.84–1.11).
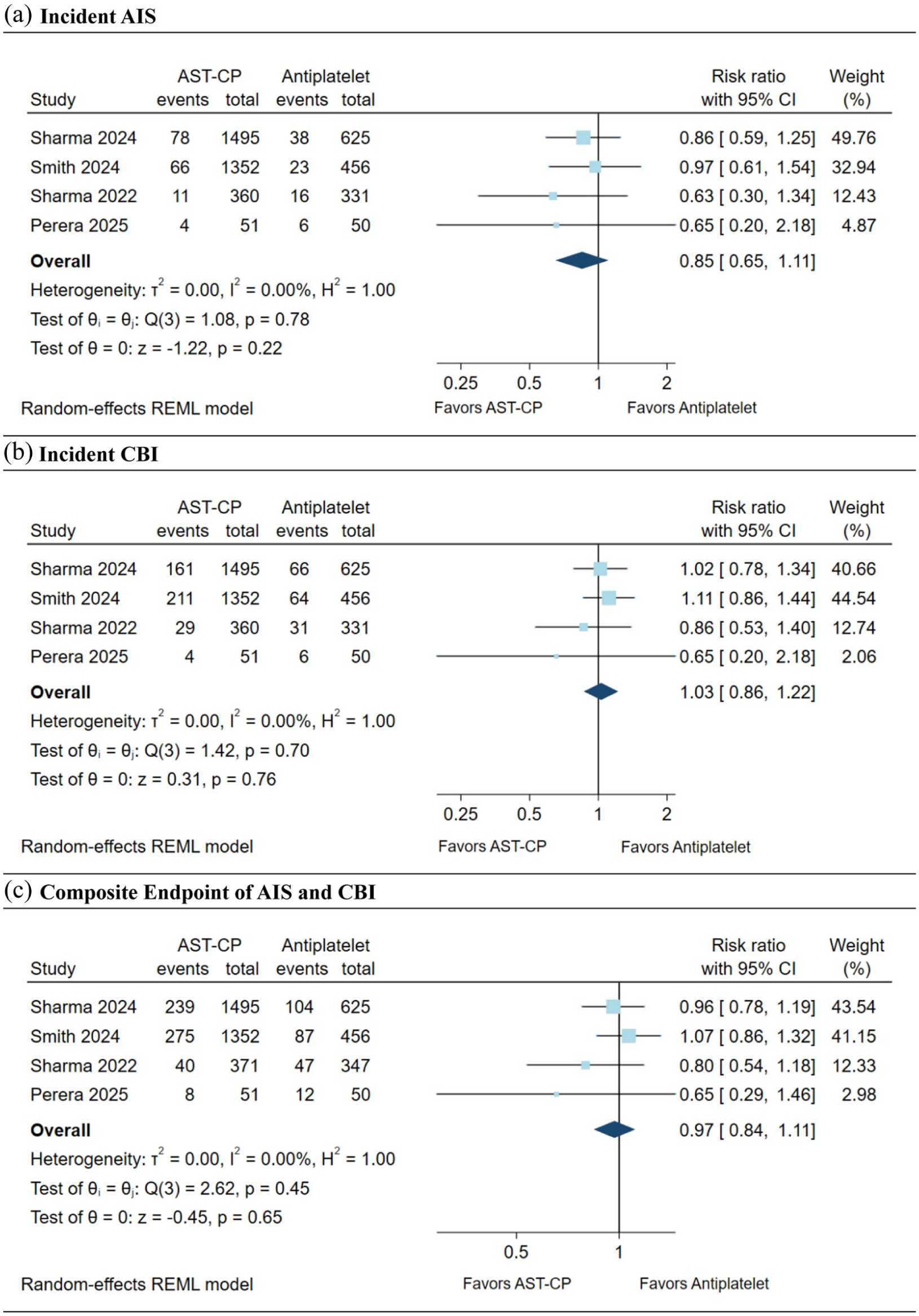
Comparison of treatment effects across outcome definitions: (a) incident AIS, (b) incident CBI, and (c) composite endpoint of AIS and CBI. Forest plots comparing the effects of antithrombotic strategies targeting the coagulation pathway versus antiplatelet therapy across different outcome definitions. Analyses were restricted to randomized controlled trials that simultaneously reported all three outcomes. Treatment effect estimates are expressed as risk ratios (RRs) with 95% confidence intervals (CIs) and were primarily derived from intention-to-treat analyses. Pooled estimates were calculated using random-effects models. AST-CP, antithrombotic strategies targeting the coagulation pathway; CBI, covert brain infarction; RR, risk ratio; CI, confidence interval.
Exploratory cross-outcome comparisons using the RRR produced trial-level point estimates generally close to unity (Figure 4). Assuming a within-trial outcome correlation of ρ = 0.5, the pooled RRR was 0.84 (95% CI, 0.67–1.07). Point estimates favored a greater relative risk reduction for AIS than for CBI, but CIs were wide and crossed unity. Across sensitivity analyses spanning assumed correlations from ρ = 0 to 0.9, pooled point estimates were similar. Higher assumed correlations were associated with progressively narrower CIs (Supplemental Table S3). A prespecified similarity range of 0.80–1.25 was applied as a descriptive reference, but the CI of the pooled RRR extended beyond this range across all assumed values of ρ. Across the four trials included in the cross-outcome comparison, RRR point estimates ranged from 0.73 to 1.00. Two trials showed concordant treatment effects for AIS and CBI, whereas two trials showed discordant effects (Supplemental Table S4). The composite endpoint was predominantly driven by CBI, accounting for 72.1% of events in the coagulation-pathway strategies group, 66.8% in the antiplatelet group, and 70.5% overall (Figure 5). These analyses were exploratory and should be interpreted cautiously.
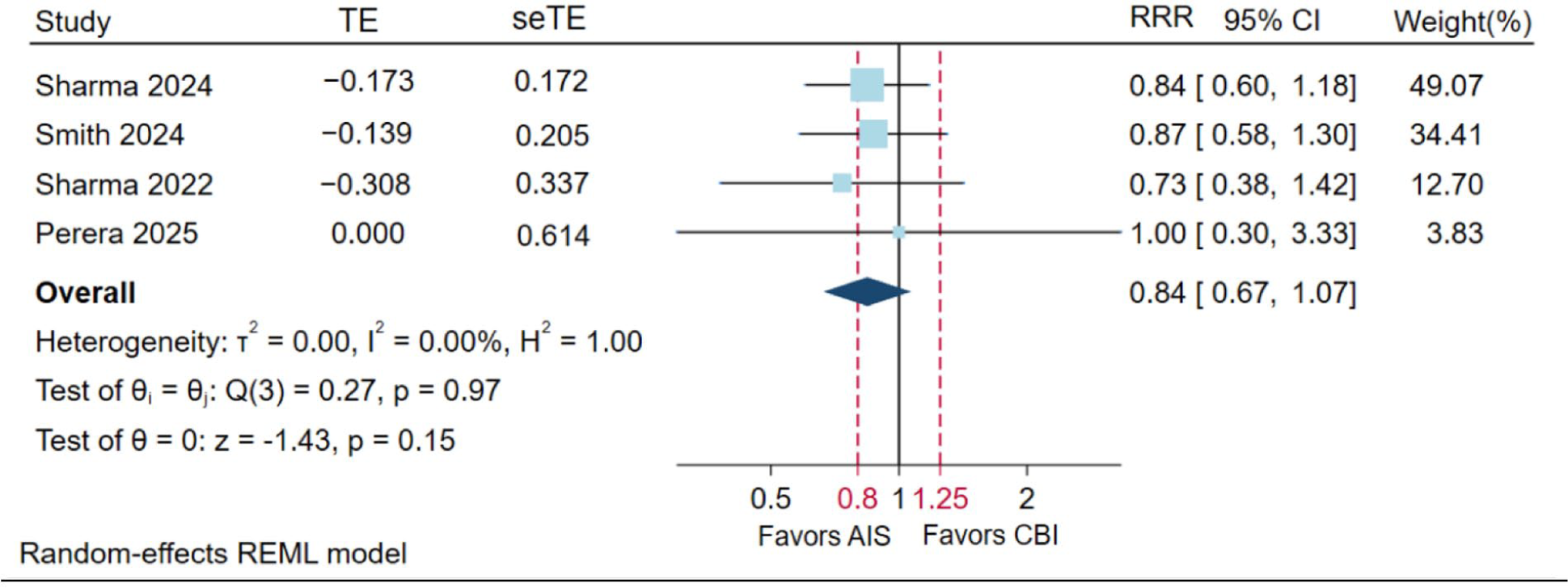
Trial-level ratio of risk ratio (RRR) comparing treatment effects on AIS and CBI. Forest plot of trial-level ratio of risk ratio (RRR = RRAIS/RRCBI) with pooled estimates from a random-effects (REML) model assuming ρ = 0.5. RRR < 1 indicates a greater relative treatment effect for AIS, whereas RRR > 1 indicates a greater relative treatment effect for CBI. Dashed vertical lines indicate prespecified interpretability bounds (RRR, 0.80–1.25), shown for descriptive comparison of treatment effects across outcomes. TE = logRRR, seTE = SE(logRRR). AST-CP, antithrombotic strategies targeting the coagulation pathway; CBI, covert brain infarction; RR, risk ratio; CI, confidence interval.
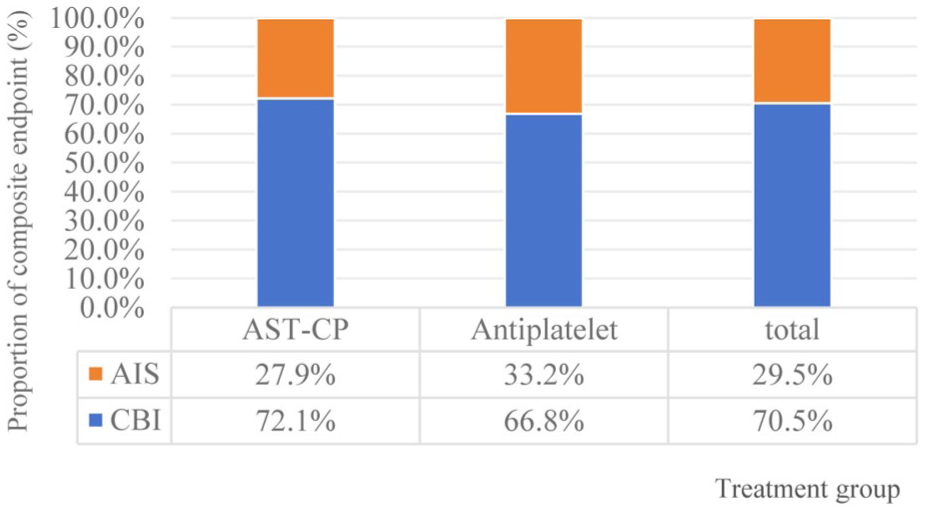
Composite endpoint events are predominantly driven by CBI. Stacked bar chart showing the composition of the composite endpoint by treatment group. AST-CP, antithrombotic strategies targeting the coagulation pathway; CBI, covert brain infarction; RR, risk ratio; CI, confidence interval.
Safety outcomes
Safety outcomes were derived from intention-to-treat populations as reported in the original trials. Results are summarized in Supplemental Figure S5. Across the included trials, symptomatic intracranial hemorrhage occurred in 38 of 12,144 participants receiving coagulation-pathway strategies and in 17 of 7963 participants receiving antiplatelet therapy. There was no statistically significant difference between groups (RR, 0.94; 95% CI, 0.33–2.65), with wide CIs reflecting substantial imprecision. Similarly, all-cause mortality occurred in 390 of 12,279 participants in the coagulation-pathway strategies group and 219 of 7967 participants in the antiplatelet group, with no significant difference between treatment groups (RR, 1.06; 95% CI, 0.86–1.32).
Sensitivity analyses
Sensitivity analyses yielded consistent results. Excluding the single trial that enrolled non-stroke populations did not materially alter the pooled estimate for incident CBI (RR, 0.96; 95% CI, 0.80–1.14; Supplemental Figure S6a). Similarly, exclusion of the trial judged to be at high risk of bias (Smith 2024) produced a comparable estimate (RR, 0.90; 95% CI, 0.73–1.10; Supplemental Figure S6b). These analyses indicate that the overall findings were robust to key study-level exclusions.
Discussion
In this systematic review and meta-analysis of six randomized trials, coagulation-pathway strategies were not associated with a reduction in incident CBI in the prespecified stratified analyses. Exploratory pooled analyses yielded similar estimates, with no suggestion of subtype-specific effects. Although clinical heterogeneity was present across study populations and treatment strategies, effect estimates were broadly consistent across treatment strata. However, the limited number of trials warrants cautious interpretation. Exploratory cross-outcome comparisons showed point estimates favoring AIS, but CIs were wide and crossed unity. These analyses do not permit firm conclusions regarding differences in treatment effects between imaging-defined and clinical stroke outcomes. The predominance of CBI events within composite endpoints further complicates the interpretation of such outcomes as reflecting effects on AIS.
Several explanations may account for the absence of a detectable benefit of coagulation-pathway strategies over antiplatelet therapy for CBI. First, neither strategy meaningfully reduces CBI risk in this clinical context, and anticoagulation may not provide incremental benefit beyond antiplatelet therapy. Evidence suggesting a protective effect of antiplatelet therapy on CBI is limited to small studies in selected populations and should, therefore, be interpreted with caution.19,20 In our analyses, stratified comparisons yielded null results across treatment contrasts. Second, lacunar CBI was more frequent than non-lacunar lesions. Lacunar infarctions are commonly linked to cerebral small vessel disease and may be less responsive to anticoagulation targeting fibrin-mediated thrombosis. 21 Non-lacunar CBI may also arise from heterogeneous embolic mechanisms, such as artery-to-artery embolism, that are less sensitive to anticoagulation.22–24 Importantly, the absence of subtype-specific treatment effects should not be interpreted as etiologic homogeneity, as CBI encompasses heterogeneous imaging phenotypes with distinct mechanisms and prognostic implications.4,25,26
In trials reporting AIS, CBI, and their composite outcome, coagulation-pathway strategies were not associated with a significant reduction in any endpoint. Exploratory cross-outcome comparisons were conducted to examine relative treatment effects across imaging-defined and clinical outcomes. Although treatment estimates for AIS and CBI were broadly similar, the ratio of relative risks produced point estimates modestly favoring AIS. However, CIs were wide, and directions of effect were inconsistent across individual trials. Notably, composite endpoints were predominantly driven by CBI, accounting for approximately 70% of events across treatment groups. 27 As a result, composite outcomes largely driven by CBI may not reliably reflect treatment effects on clinically manifest ischemic stroke. Comparisons across outcome definitions should, therefore, be interpreted cautiously. 28
Prior observational and imaging studies suggest that covert and symptomatic ischemic infarctions lie along a common spectrum of cerebrovascular disease, with clinical manifestation influenced by lesion size, location, and network connectivity rather than fundamentally distinct pathophysiological processes.26,29–31 Population-based data indicate that individuals with lacunar CBI may have long-term risks of recurrent stroke and mortality comparable to those with symptomatic lacunar infarction. 32 However, a shared disease spectrum does not imply equivalence of treatment responsiveness across outcome definitions. Several factors may limit the sensitivity of CBI to treatment effects on clinically manifest ischemic events. Most CBI lesions are small subcortical or lacunar infarcts attributed to cerebral small vessel disease, reflecting microvascular injury rather than fibrin-rich thromboembolic occlusion.31–33 Challenges related to lesion ascertainment and temporal attribution further complicate interpretation, as some lesions detected on early MRI may reflect progression of the index event or evolve over time within regions of pre-existing white matter disease.34,35
Several limitations should be acknowledged. First, CBI was assessed only among participants who completed follow-up MRI, and MRI completion rates varied across trials. In addition, some studies also excluded participants who developed symptomatic stroke from CBI analyses. As a result, outcome ascertainment did not fully reflect an intention-to-treat population and may have introduced selection bias. Second, MRI acquisition protocols and the timing of follow-up scans differed across studies, potentially contributing to heterogeneity in CBI detection. Third, the included trials varied with respect to study populations, antithrombotic regimens, antiplatelet regimens used in the control arms, and the extent of atrial fibrillation screening before enrollment. Such clinical and methodological heterogeneity may influence the generalizability of pooled estimates. Fourth, analyses of CBI subtypes were limited by small sample sizes and incomplete reporting. Fifth, without individual patient-level data, we could not formally assess within-trial interactions between outcome type and treatment effect. Finally, although symptomatic intracranial hemorrhage was reported, data on asymptomatic intracranial hemorrhage were generally unavailable, limiting a more complete assessment of safety. In this context, no randomized trials have been specifically designed to evaluate anticoagulation strategies with incident CBI as a primary outcome. However, delayed or selective reporting cannot be excluded and may have influenced the observed estimates. Ongoing studies are beginning to assess CBI as an outcome, predominantly in the context of antiplatelet-based interventions rather than anticoagulation, and may provide indirect insights into this question.
Conclusion
In patients without an indication for anticoagulation, antithrombotic strategies targeting the coagulation pathway were not associated with a reduction in incident CBI, and no subtype-specific effects were observed. Exploratory comparisons between CBI and AIS do not permit firm conclusions regarding differences in treatment effects between imaging-defined and clinical stroke outcomes. Composite endpoints predominantly driven by CBI should be interpreted with caution when inferring treatment effects on clinically manifest ischemic stroke.
Supplemental Material
sj-docx-1-wso-10.1177_17474930261446363 – Supplemental material for Antithrombotic strategies targeting the coagulation pathway and incident covert brain infarction: A systematic review and meta-analysis of randomized trials
Supplemental material, sj-docx-1-wso-10.1177_17474930261446363 for Antithrombotic strategies targeting the coagulation pathway and incident covert brain infarction: A systematic review and meta-analysis of randomized trials by Fuxia Yang, Lu Wang, Xiao Wu, Lulan Li, Xueqiao Jiao, Fangfang Zhang, Xunming Ji and Xiuhai Guo in International Journal of Stroke
Footnotes
Acknowledgements
The authors thank Fang Wu, Department of Radiology, Beijing Xuanwu Hospital, Capital Medical University, Beijing, for her assistance in article preparation.
Author contributions
F.X.Y. and L.W. contributed equally. F.X.Y., X.M.J., and X.H.G. conceived and designed the study. F.X.Y., L.W., X.W., X.Q.J., L.L.L., and F.F.Z. contributed to statistical analyses and interpretation of data. F.X.Y., L.W., and X.H.G. drafted and revised the manuscript for content. All authors have read and approved the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Science and Technology Major Project (2023ZD0503801 and 2023ZD0503806), the National Natural Science Foundation of China (82171302), and the Capital’s Funds for Health Improvement and Research (2024-1-2011).
Data availability statement
Data collected for the study may be made available from the corresponding author to others upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.