
Abstract
Background:
Vascular cognitive impairment (VCI) encompasses cognitive impairment attributable to cerebrovascular disease, including post-stroke cognitive impairment (PSCI). Exercise and multidomain interventions have been investigated in these populations; however, cognitive outcomes remain heterogeneous.
Aims:
To synthesize randomized controlled trials on exercise-based and exercise-inclusive multidomain interventions in VCI (including PSCI) and examine how population definition, intervention delivery, and outcome selection influence cognitive outcomes.
Summary of review:
A narrative review identified randomized or controlled trials reporting cognitive outcomes following exercise-only or multidomain interventions. Studies were grouped into three populations: documented cerebrovascular brain injury, vascular or metabolic risk-enriched populations without cognitively defined inclusion criteria, and cognitively defined risk states. The latter two groups were included as contextual comparators and were not assumed to meet criteria for VCI. In populations with documented cerebrovascular brain injury (n = 20), longer-duration multidomain interventions focused on vascular risk-factor optimization and lifestyle advice improved vascular targets without consistent cognitive benefit. In contrast, structured and supervised exercise in chronic stroke and cerebral small-vessel disease more often reported domain-specific cognitive improvements, commonly in executive functioning and attention. In risk-enriched and cognitively defined populations, cognitive effects were more detectable when exercise was actively delivered and cognition was the primary outcome.
Conclusions:
Detectability of cognitive effects in exercise and multidomain interventions for VCI depends on population definition, outcome selection, and whether exercise is prescribed and delivered rather than simply advised.
Keywords
Introduction
Vascular cognitive impairment (VCI) refers to cognitive impairment due to cerebrovascular disease and encompasses a range of clinical presentations, including post-stroke cognitive impairment (PSCI). Cognitive deficits in these conditions are often domain-specific, with prominent involvement of executive function and processing speed, reflecting disruption of fronto-subcortical networks.1–6 Despite their prevalence and clinical impact, few interventions have demonstrated reliable modification of cognitive trajectories once vascular brain injury is established.
Pharmacological management of vascular risk factors is central to stroke prevention, but cognitive outcomes are rarely the primary therapeutic target. Trials of intensive vascular risk-factor optimization after stroke have improved vascular profiles without consistent cognitive benefit, highlighting a dissociation between systemic vascular control and cognition in populations with documented cerebrovascular disease.7,8 This has increased interest in lifestyle-based strategies, particularly exercise and exercise-inclusive multidomain interventions.
Randomized trials of exercise-based and multidomain interventions in PSCI have reported heterogeneous cognitive findings. Systematic reviews of post-stroke exercise trials pool diverse intervention types across broad post-stroke populations, often including rehabilitation or mixed physical activity programs in which cognition is secondary or exploratory. Across these reviews, cognitive effects are generally small-to-moderate, most consistently observed in attention and processing speed rather than global cognition, with substantial between-study heterogeneity.9,10 However, existing reviews do not resolve how differences in population definition, intervention delivery, and outcome selection contribute to the detectability of cognitive effects in PSCI.
Interpretation is further complicated by similar intervention approaches being evaluated across populations that differ in vascular burden, cognitive definition, and outcome prioritization. In vascular or cardiometabolic risk-enriched populations without cognitively defined inclusion criteria, multidomain interventions have been tested in large prevention trials, including Finish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER), 11 Prevention of Dementia by Intensive Vascular Care (preDIVA), 12 Healthy ageing through internet counselling in the elderly (HATICE), 13 Multidomain Alzheimer Preventive Trial (MAPT), 14 and AgeWell.de, 15 in which cognition was variably specified as a primary or secondary outcome. Related approaches have also been examined in cognitively defined risk states, most commonly subjective cognitive decline (SCD), mild cognitive impairment (MCI), or cognitive impairment no dementia (CIND), trials such as The Exercise and NutritionaL Interventions for neurocoGnitive HealTh EnhaNcement (ENLIGHTEN),16,17 Active Prevention in People at risk of dementia through Lifestyle, bEhaviour change and Technology to build REsiliEnce (APPLE-Tree), 18 and Japan-Multimodal Intervention Trial for prevention of dementia (J-MINT), 19 where cognition is explicitly targeted and outcome sensitivity differs from post-stroke populations. Although these studies do not focus on PSCI or VCI, they provide context for how cognitive effects are assessed across different population definitions.
This narrative review synthesizes evidence from randomized trials of exercise-only and exercise-inclusive multidomain interventions in PSCI and VCI while considering vascular risk-enriched and cognitively defined populations without established brain injury as contextual comparators. The review examines how population definition, intervention delivery, and cognitive outcome selection relate to the detectability of cognitive effects.
Methods
Search strategy and selection criteria
This narrative review synthesized randomized or controlled trials of exercise-only or multidomain interventions reporting cognitive outcomes in VCI, including PSCI and cerebral small-vessel disease (CSVD) while also considering contextual trials in vascular risk-enriched and cognitively defined populations.
Structured searches were conducted in PubMed/MEDLINE to identify trials in adults with (1) documented cerebrovascular brain injury, (2) vascular or cardiometabolic risk enrichment without cognitively defined inclusion criteria, and (3) cognitively defined risk states without required cerebrovascular disease. Searches used MeSH and free-text terms and were restricted to human randomized or controlled trials. Protocols, feasibility studies without outcomes, qualitative studies, and reviews were excluded. Search strategies are provided in the Supplementary Methods.
The search identified 1105 records. After screening and full-text review, 22 stroke/VCI trials and 17 contextual trials were included.
Titles and abstracts were screened by two reviewers, followed by a full-text review. Discrepancies were resolved by discussion. Extracted variables included population characteristics, intervention structure, cognitive outcomes, and vascular or physiological measures. A formal risk-of-bias assessment was not performed, given the narrative synthesis approach.
Conceptual framework and population grouping
Studies were grouped into three categories (Figure 1):
Documented cerebrovascular brain injury (predominantly post-stroke populations, with additional studies in CSVD and clinically defined VCI).
Vascular or metabolic risk-enriched populations without cognitively defined inclusion criteria.
Cognitively defined risk states (SCD, CIND, or MCI) are not selected on the basis of post-stroke syndromes.
This grouping was applied to support the interpretation of heterogeneity in cognitive outcomes and does not imply that all included populations met criteria for VCI or formed a single biological continuum. Frailty, multimorbidity, and reduced intrinsic capacity may influence intervention response within groups but were not used to define them.
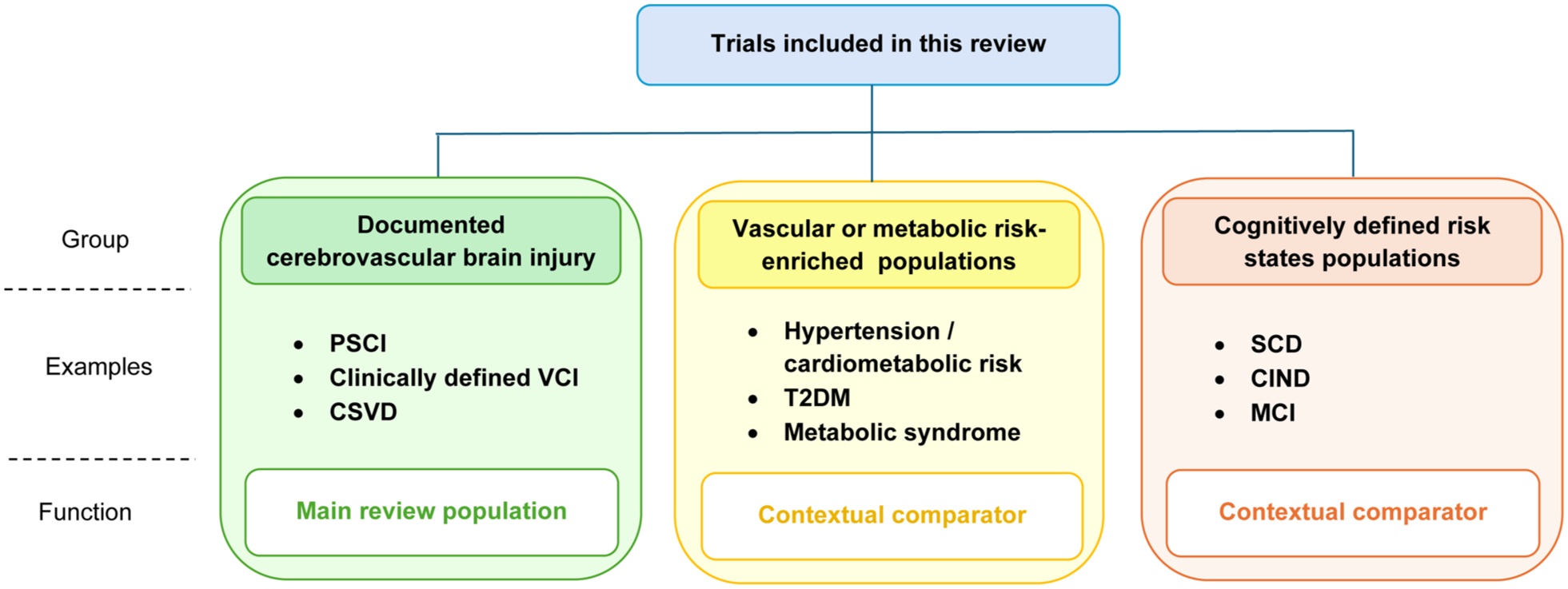
Study classification framework. Studies were grouped by enrolled population to interpret heterogeneity in cognitive outcomes. The latter two groups were contextual comparators and were not assumed to meet criteria for VCI. PSCI: post-stroke cognitive impairment, VCI: vascular cognitive impairment, CSVD: cerebral small-vessel disease, T2DM: type-2 diabetes mellitus, SCD: subjective cognitive decline, CIND: cognitive impairment not dementia, MCI: mild cognitive impairment.
Intervention classification and synthesis approach
Interventions were categorized as exercise-only, exercise-anchored multidomain (exercise combined with at least one additional lifestyle or vascular risk-factor component), or non-exercise multidomain (⩾2 non-exercise components). Non-exercise multidomain trials were retained as comparators to contextualize whether cognitive effects differed when exercise was actively delivered versus when vascular risk management or lifestyle advice was provided without a structured exercise component. In the stroke/VCI literature, these interventions were generally examined within usual post-stroke care and secondary prevention, rather than as replacements for standard medical management.
Given heterogeneity in intervention design and cognitive measures, findings were synthesized qualitatively. Cognitive outcomes were grouped by domain and interpreted relative to intervention type and population context, with emphasis on consistent patterns rather than individual trial effects.
Documented vascular brain injury (VCI, including PSCI and CSVD)
Twenty randomized controlled trials were conducted in populations with documented cerebrovascular disease, including PSCI, chronic stroke, CSVD, or clinically defined VCI (Table 1). Cognitive outcomes ranged from single screening measures or individual executive tests to broader neuropsychological batteries and domain composites, while vascular or physiological measures were variably reported (Supplementary Table S1).
Characteristics of exercise and multidomain intervention trials in PSCI, chronic stroke, and clinically defined VCI.
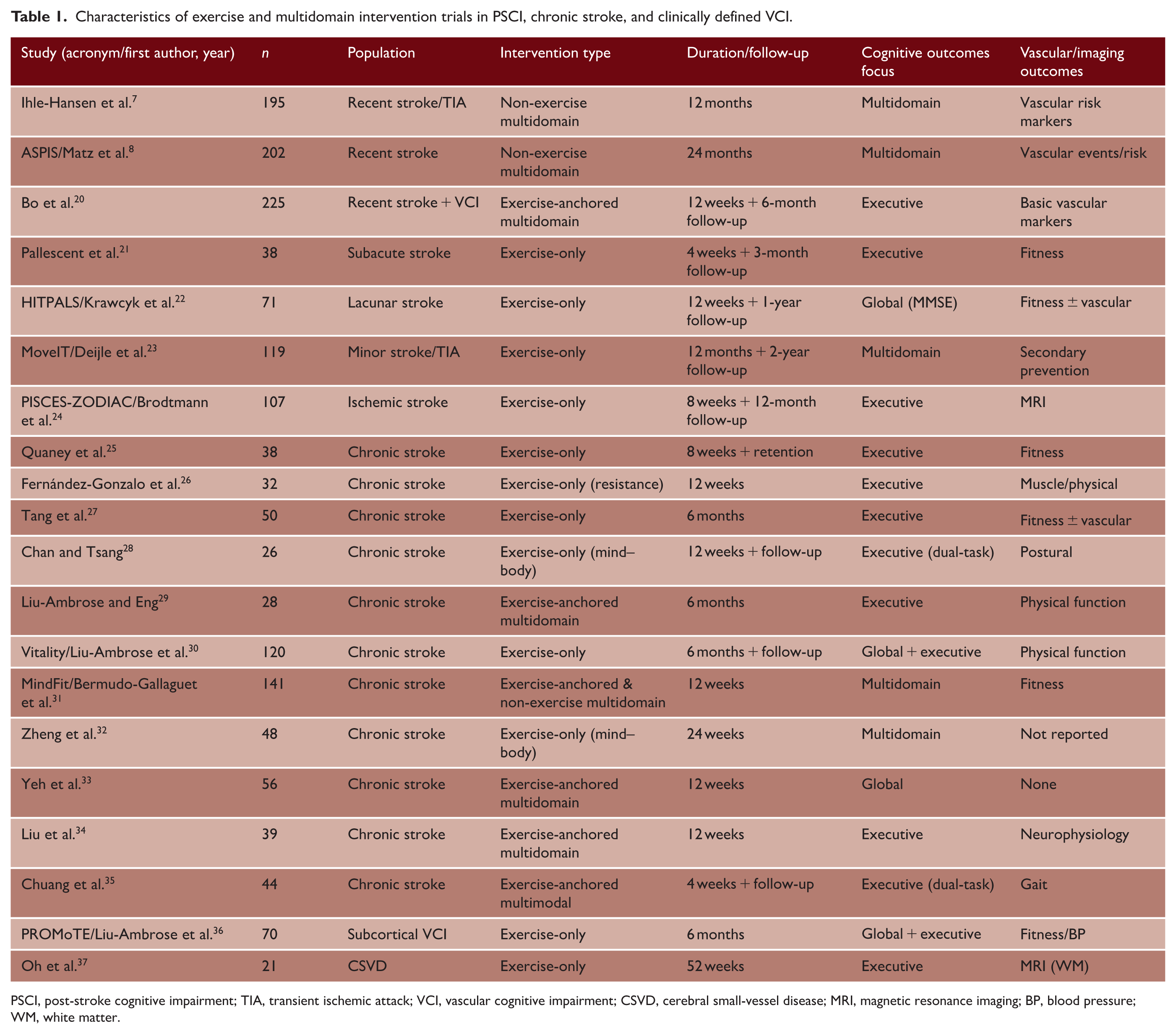
PSCI, post-stroke cognitive impairment; TIA, transient ischemic attack; VCI, vascular cognitive impairment; CSVD, cerebral small-vessel disease; MRI, magnetic resonance imaging; BP, blood pressure; WM, white matter.
Recent and subacute post-stroke
In recent and subacute post-stroke populations, the largest trials employed multidomain programs centered on lifestyle counseling and vascular risk-factor management, rather than structured exercise delivery. In ASPIS 8 and the trial by Ihle-Hansen et al., 7 intensive lifestyle counseling improved vascular target attainment but did not produce between-group differences in global cognition or cognitive decline over 12–24 months. Physical activity was advised but not actively delivered or supervised.
Smaller trials incorporating structured exercise delivery in recent or subacute post-stroke populations reported variable but occasionally domain-specific cognitive effects, most commonly in executive function.21–23 Brodtmann et al. 24 reported faster Trail Making Test-B completion and better Alzheimer’s Disease Assessment Scale–Cognitive Subscale (ADAS-Cog) performance at 12 months following combined aerobic and resistance training, without preservation of hippocampal volume. In individuals within 6 months of stroke meeting criteria for VCI, Bo et al. 20 demonstrated greater improvement in global cognition and executive function with supervised multicomponent exercise combined with cognitive training relative to control. Across these trials, vascular or cerebrovascular outcomes were inconsistently reported, limiting inference regarding underlying mechanisms.
In recent post-stroke populations, counseling-based multidomain strategies improved vascular profiles without measurable cognitive benefit, whereas structured exercise was associated with small, domain-specific executive effects.
Chronic stroke
In chronic stroke populations (typically >6 months post-event), interventions more often involved structured exercise delivery over shorter durations (8–24 weeks). Exercise-only trials included training, 25 resistance training, 26 intensity comparisons, 27 and mind-body modalities including Tai Chi or Baduanjin.28,32 Although sample sizes were modest and cognition was frequently secondary, several studies reported small to modest improvements in executive function, attention, or processing speed, while memory and global cognition effects were inconsistent.
Exercise-anchored multidomain interventions in chronic stroke populations included combinations of structured exercise with cognitive training30,33,34 or recreational/leisure activities, 29 dual-task or cognitively demanding exercise paradigms, 35 and hybrid or remotely delivered programs. 31 Cognitive improvements were reported in some studies, but effects were heterogeneous and not clearly separable from those observed in exercise-only interventions. Chronic stroke trials suggest that structured exercise may yield modest, domain-specific cognitive effects (particularly in executive function) without consistent evidence of global or sustained cognitive improvement.
CSVD and subcortical VCI
Only two small and exploratory studies targeted CSVD or subcortical VCI without recent stroke. In PROMoTE, 6 months of aerobic exercise produced a small short-term improvement in global cognition that was not sustained at follow-up, 36 with ancillary analyses examining functional activation. 38 Oh et al. 37 examined a 52-week resistance training program in older women with CSVD reported preservation of white matter integrity without a clear cognitive benefit.
Summary of studies of subjects with documented vascular brain injury
Across populations with documented vascular brain injury, cognitive findings varied by population stage and intervention delivery. Advice-based multidomain strategies improved vascular targets without consistent cognitive benefit, whereas structured exercise in chronic stroke and CSVD was more often associated with modest executive improvements.
Contextualizing evidence from high vascular risk and early cognitive impairment
Vascular or metabolic risk-enriched
Trials enrolling vascular or cardiometabolic risk-enriched populations without cognitively defined inclusion criteria are summarized in Table 2 and Supplementary Table S2.
Selected randomized trials of exercise-based and multidomain lifestyle interventions in vascular risk-enriched and cognitively defined populations.
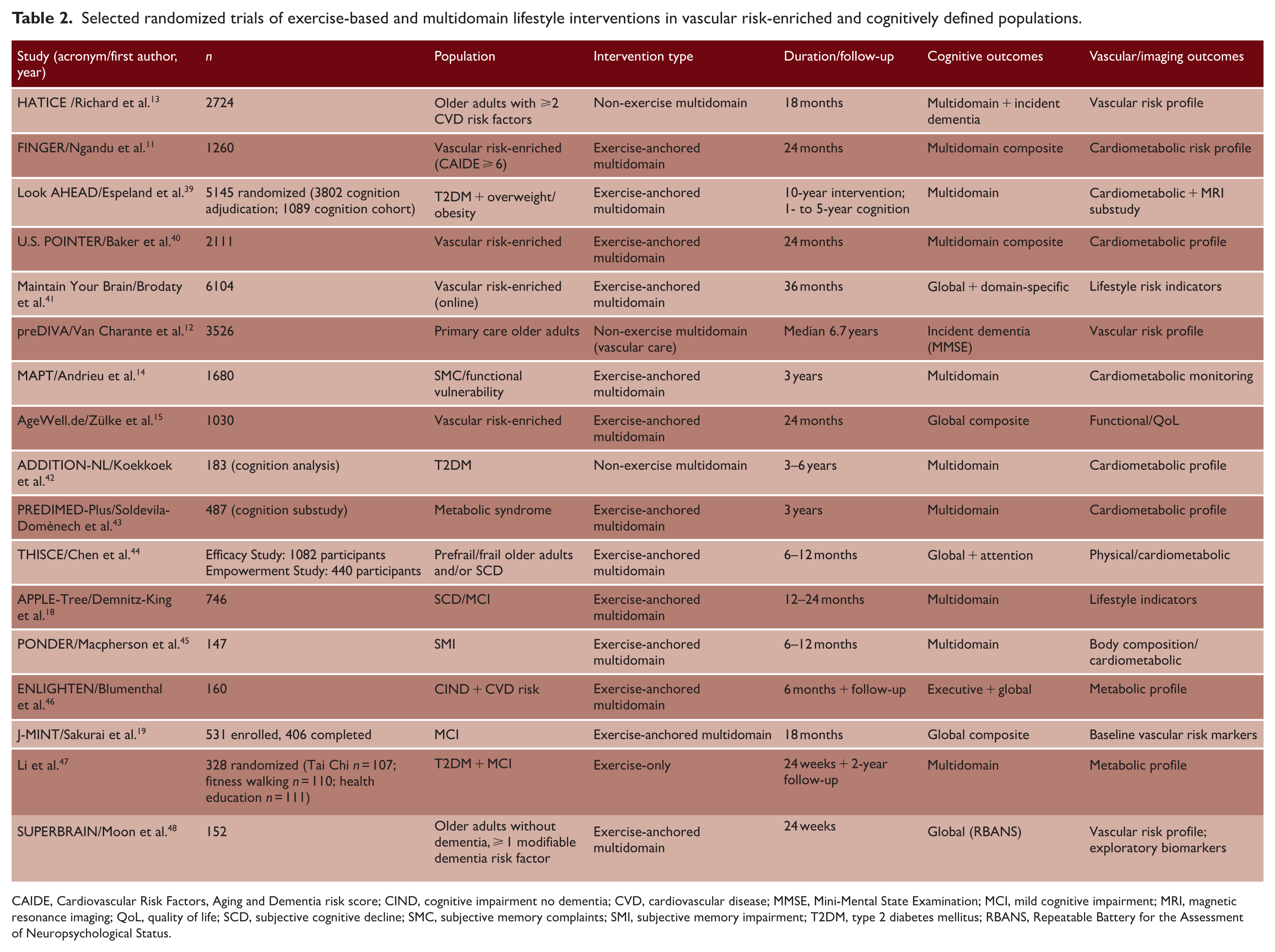
CAIDE, Cardiovascular Risk Factors, Aging and Dementia risk score; CIND, cognitive impairment no dementia; CVD, cardiovascular disease; MMSE, Mini-Mental State Examination; MCI, mild cognitive impairment; MRI, magnetic resonance imaging; QoL, quality of life; SCD, subjective cognitive decline; SMC, subjective memory complaints; SMI, subjective memory impairment; T2DM, type 2 diabetes mellitus; RBANS, Repeatable Battery for the Assessment of Neuropsychological Status.
In large prevention trials such as HATICE and preDIVA, improvements in vascular risk profiles were observed without corresponding cognitive benefit, consistent with cognition not being a primary intervention target.12,13 In contrast, FINGER delivered a structured, exercise-anchored multidomain program over 24 months with cognition as a primary outcome, demonstrating improvement in global and domain-specific cognitive composites alongside vascular and metabolic changes. 11 Other risk-enriched trials (AgeWell.de, U.S. POINTER, and Maintain Your Brain) monitored vascular and lifestyle indicators, with modest effects sensitive to outcome selection and follow-up duration.15,40,41
In metabolically defined cohorts such as Look AHEAD, ADDITION-NL, and PREDIMED-Plus, interventions targeted weight, glycemic control, and cardiovascular risk factors, while cognitive outcomes were assessed in ancillary analyses.39,42,43 In ADDITION-NL, cognition was assessed several years after randomization, limiting the detection of change. Across these trials, cognitive effects were modest and heterogeneous.
Cognitively defined risk states
A separate group of trials enrolled participants based on cognitive status (SCD, MCI, CIND) without requiring documented cerebrovascular disease.
Trials including J-MINT, ENLIGHTEN, SUPERBRAIN, APPLE-Tree, THISCE, and PONDER evaluated exercise-based or multidomain interventions over 6–24 months, with cognition typically specified as a primary endpoint.18,19,44–46,48 Effects were generally modest and domain-specific, while vascular or physiological measures were secondary and variably reported. Li et al.’s 47 Tai Chi intervention uniquely enrolled participants with both type 2 diabetes mellitus and MCI, reducing metabolic heterogeneity at baseline and allowing clearer assessment of exercise-related cognitive effects.
Synthesis across populations
Across trials in vascular risk-enriched and cognitively defined populations without documented cerebrovascular injury, cognitive outcomes varied primarily by trial intent and intervention delivery. Studies designed to modify vascular or metabolic risk factors did not consistently demonstrate cognitive benefit, even when systemic markers improved. In contrast, trials explicitly targeting cognition, particularly those incorporating structured and supervised exercise, were more likely to demonstrate modest improvements in composite or domain-specific measures.
Together, these findings suggest that cognitive detectability depends less on risk category alone than on whether cognition is the intended target, the biological pathways engaged, and the intensity and structure of delivery.
Cognitive outcomes in relation to vascular, metabolic, and imaging measures
Cognitive effects across exercise and multidomain intervention trials may depend on which neurobiological pathways remain modifiable and whether intervention delivery provides sufficient stimulus.
In populations with documented cerebrovascular injury, particularly recent and subacute post-stroke cohorts, multidomain interventions without structured exercise components improved systemic vascular markers without corresponding cognitive benefit over typical trial durations.7,8 This suggests that once structural vascular injury is established, modification of systemic risk alone may be insufficient to produce measurable short-to medium-term cognitive change.
Trials incorporating structured, supervised exercise have frequently reported selective improvements in executive function and attention, even when conventional vascular markers or structural imaging outcomes were unchanged or not reported.25,27,28 While ancillary PROMoTE analyses links executive change to altered task-evoked neural activity, 38 structural imaging correlates have been inconsistent across studies.24,49
In vascular risk-enriched and cognitively defined populations without prior stroke, broader pathways may be engaged. In ENLIGHTEN, improvements in executive function were accompanied by changes in metabolic indices, including insulin sensitivity, suggesting a role for metabolic regulation in cognitive response. 46 In larger multidomain prevention trials, cognitive effects are generally modest. However, secondary analyses from FINGER and MAPT indicate stronger cognitive benefit among participants with higher adherence,14,50 suggesting that biological pathway and achieved dose influence detectability.
Clinical implications
In recent or subacute post-stroke populations, counseling-based multidomain programs improved vascular profiles but did not produce consistent cognitive benefit.7,8 Exercise appears more relevant as an adjunct for secondary prevention and functional recovery than for reliable cognitive improvement.
In chronic stroke and CSVD, structured and supervised exercise interventions were more consistently associated with selective improvements in executive and attentional functions.25,27,37,38 When cognitive improvement is the objective, delivered exercise appears more informative than advice-based approaches. Where multidomain programs are used, the exercise component is most closely aligned with short-term cognitive outcomes, while other components may support longer-term vascular control.
Outcome selection has important implications. Global measures were often insensitive, whereas executive and processing speed measures were more responsive.25,27 Domain-specific cognitive assessments alongside fitness or functional measures may provide a more informative evaluation when global cognitive change is not expected.
Outcome selection and assessment timing are important considerations. In PROMoTE, a small between-group difference favouring aerobic training on ADAS-Cog was present at the end of the 6-month intervention but was not sustained at the 6-month follow-up, while Executive Interview (EXIT-25) and Alzheimer’s Disease Cooperative Study–Activities of Daily Living (ADCS-ADL) remained non-significant. 36 This highlights the need to select outcomes that match the treatment effect and to distinguish immediate post-intervention effects from sustained benefit.
Evidence gaps and research priorities
Vascular or physiological outcomes were often incompletely analyzed or not formally compared between groups. This limits the assessment of whether cognitive effects or null findings were accompanied by changes in systemic vascular risk, fitness, or cerebrovascular parameters.
Treatment fidelity and physiological verification were variably reported across the VCI and stroke exercise trials. Prescribed intensity was described in several studies,21,23–25,31,36,37 attendance or adherence was documented in a subset,21,28,29,31,36 and objective physiological or functional change was reported in some trials.21,23–25,31,36,37 However, none of the included VCI/stroke trials formally tested whether achieved exercise dose, adherence, or physiological change were associated with cognitive outcomes, and several provided only limited information on achieved dose or compliance.27–29,32 This makes it difficult to distinguish insufficient biological stimulus from true lack of cognitive effect and precludes firm conclusions regarding dose–response relationships. Future trials should report prescribed and achieved exercise dose, supervision model, adherence, and objective physiological markers alongside cognitive outcomes.
Global cognitive measures may lack sensitivity in vascular populations with heterogeneous baseline impairment. Alignment between hypothesized mechanisms, population definition, and domain-specific cognitive outcomes would improve interpretability.
Differences in population definition and intervention structure limit comparability across studies. Trials conducted in vascular risk-enriched or mildly impaired populations differ fundamentally from those in established cerebrovascular disease, yet few studies examine similar interventions across these stages.
Mechanistic evidence remains limited. Few trials integrated cognitive outcomes with neuroimaging, neurophysiological, or biomarker measures in a way that permits testing of biological pathways underlying change. Mechanistically informed designs remain a research priority.
Limitations
This review is a narrative synthesis rather than a systematic review. Heterogeneity limits direct comparison, and cognitive outcomes were often secondary or exploratory.
Conclusion
In populations with documented vascular brain injury, multidomain interventions centered on vascular risk management improved systemic markers but did not consistently improve cognition. Structured exercise, particularly in chronic stroke and CSVD, was associated with selective executive and attentional benefits.
Evidence from vascular risk-enriched and cognitively defined populations helps contextualize how intervention goals, delivery, and outcome selection influence cognitive detectability, but these populations were considered as contextual comparators and not as equivalent to established VCI. Intervention goals, delivery, and outcome selection should align with population definition and baseline vascular pathology.
Supplemental Material
sj-docx-1-wso-10.1177_17474930261451077 – Supplemental material for Exercise and multidomain interventions for vascular cognitive impairment: A narrative review
Supplemental material, sj-docx-1-wso-10.1177_17474930261451077 for Exercise and multidomain interventions for vascular cognitive impairment: A narrative review by Kwong Hsia Yap, Rozene Cher Wei Yap, Evangeline Hui Jie Ong, Narayanaswamy Venketasubramanian and Christopher Li-Hsian Chen in International Journal of Stroke
Supplemental Material
sj-xlsx-2-wso-10.1177_17474930261451077 – Supplemental material for Exercise and multidomain interventions for vascular cognitive impairment: A narrative review
Supplemental material, sj-xlsx-2-wso-10.1177_17474930261451077 for Exercise and multidomain interventions for vascular cognitive impairment: A narrative review by Kwong Hsia Yap, Rozene Cher Wei Yap, Evangeline Hui Jie Ong, Narayanaswamy Venketasubramanian and Christopher Li-Hsian Chen in International Journal of Stroke
Footnotes
Acknowledgements
The authors thank colleagues at the Memory Aging and Cognition Centre for discussions.
Author Contributions
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Data availability
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.