
Abstract
Background:
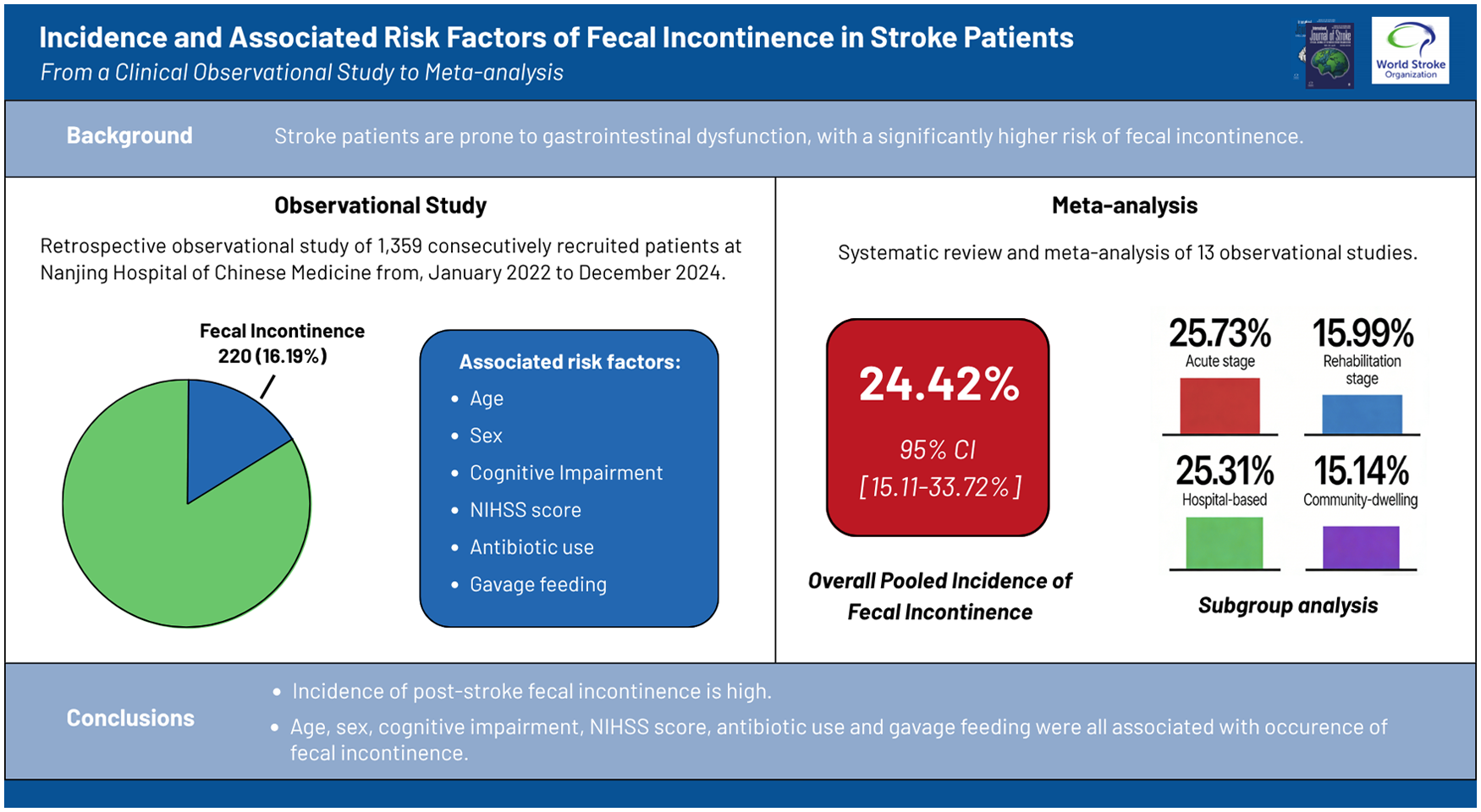
Stroke patients are prone to gastrointestinal dysfunction, with a significantly higher risk of fecal incontinence (FI), which severely affects their quality of life.
Aims:
We investigated the incidence and associated risk factors of FI in stroke patients.
Summary of review:
Stroke patients who met the inclusion and exclusion criteria were consecutively recruited at one university medical center from January 2022 to December 2024. FI occurred in 220 of 1359 stroke patients (16.19%). Logistic regression analysis revealed that age, gender, cognitive impairment, National Institutes of Health Stroke Scale (NIHSS) admission score, antibiotic use, and gavage feeding were closely associated with FI incidence in stroke patients. Subsequently, a systematic review and meta-analysis of observational studies followed the Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines. Studies were included if they reported the incidence or risk factors of FI in stroke patients. Subgroup analyses were conducted according to the stage of stroke and survey site. The forest plot showed that the incidence of post-stroke FI was 24.42% (95% confidence interval (CI) = 15.11–33.72). On subgroup analysis, the incidence of FI was 25.73% (95% CI = 14.61–36.86) in the acute stage and 15.99% (95% CI = 9.32–22.67) in the rehabilitation stage. Meanwhile, the incidence of FI in the hospital-based stroke patients was 25.31% (95% CI = 11.37–39.26), which was higher than that in the community-dwelling stroke patients (15.14%, 95% CI = 2.26–28.02).
Conclusion:
The incidence of post-stroke FI is relatively high. Age, gender, cognitive impairment, NIHSS score, antibiotic use, and gavage feeding are closely associated with FI occurrence in stroke patients.
Introduction
Stroke has long been a significant public health issue, causing enormous economic and social burdens.1–3 In addition, it is a major contributor to morbidity and mortality. It is reported that it is the second leading cause of death and the third most prominent cause of disability-adjusted life years. 4
Stroke is often accompanied by various medical complications, leading to the deterioration of the disease. Gastrointestinal dysfunction, such as fecal incontinence (FI), is a common and painful manifestation after stroke. 5 There is evidence to suggest that gastrointestinal complications may reduce quality of life, leading to prolonged hospitalization, malnutrition, pressure ulcers, and poor neurological prognosis.6,7 These consequences pose significant challenges to stroke patient care, public health systems, and rehabilitation services.
Compared with the general population, patients with central nervous system diseases have a significantly increased risk of gastrointestinal complications. 8 The bidirectional communication between the central nervous system and the gastrointestinal tract, known as the brain–gut axis, plays a crucial role.9–11 Cerebrovascular diseases can damage various components of the brain–gut axis, including the gut and autonomic nervous system.12,13
Currently, gastrointestinal complications receive much less attention, but as many as 50% of stroke patients may experience FI, diarrhea, constipation, or other gastrointestinal complications. 14 The risk of stroke patients losing intestinal control is much higher than that of others. 15 Although FI is common after stroke, the incidence and associated risk factors of FI remain inadequately investigated.
This study focuses on the incidence and risk factors of FI after stroke. The purpose is to draw attention to the development of effective management strategies. We initially conducted a clinical observational study to describe the FI characteristics of stroke patients. Subsequently, a meta-analysis was conducted to synthesize studies from different sources and validate the generalizability of our findings.
Methods
Clinical observational study
This section followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines, conformed to the Declaration of Helsinki, and was approved by the Ethics Committee of Nanjing Hospital of Chinese Medicine Affiliated to Nanjing University of Chinese Medicine (No. KY2022270).
Study design and participants
This retrospective study enrolled stroke inpatients admitted to Nanjing Hospital of Chinese Medicine Affiliated to Nanjing University of Chinese Medicine from January 2022 to December 2024. Based on the presence or absence of FI, the participants were categorized into the observation group (FI group) and the control group (fecal continence group, FC group).
Data sample and patient selection
Patients meeting the following criteria were included in this study: all stroke diagnoses comply with the International Classification of Diseases 11th revision (ICD-11) criteria; irrespective of age and gender, those with brain injury due to ischemic or hemorrhagic stroke, without considering the post-injury time span, cognitive impairment, and language function changes. For patients without cognitive and/or language dysfunction, researchers conducted direct interviews. For those with cognitive and/or language dysfunction, interviews were carried out by caregivers familiar with their bowel function characteristics.
The exclusion criteria were as follows: patients with transient ischemic attack (TIA) or no evidence of ischemia or hemorrhage on imaging examination; pre-stroke history of FI; concomitant spinal cord injury of any type; incomplete or unclear medical information, precluding accurate disease assessment; and refusal to provide relevant information.
According to the symptomatic diagnostic criteria of the Rome IV, FI was defined as the recurrent uncontrolled passage of solid or liquid fecal material. Defecation status was recorded daily during hospitalization for all stroke patients. Data on fecal leakage were routinely reported by nurses in the stroke ward during hospitalization, and the diagnosis was confirmed by two trained and qualified physicians through joint assessment. New-onset FI during hospitalization was defined as post-stroke FI.
Data collection
Information of eligible stroke patients was collected, including (1) demographic data: age and gender; (2) medical history: hypertension, diabetes mellitus, hyperlipidemia, coronary heart disease, atrial fibrillation, chronic renal failure, chronic obstructive pulmonary disease (diagnosed according to ICD-11 criteria); cognitive impairment (assessed by the Mini-Mental State Examination, score <24); gastrointestinal diseases (including peptic ulcer, chronic gastritis, inflammatory bowel disease, irritable bowel syndrome, diagnosed according to ICD-11 criteria); (3) disease-related information: National Institutes of Health Stroke Scale (NIHSS) admission score for stroke severity; stroke subtype (ischemic stroke, hemorrhagic stroke, hemorrhagic infarction); stroke stage (acute stage: first 7 days following stroke onset; rehabilitation stage: more than 7 days after stroke onset); affected cerebral hemisphere (left, right, bilateral); arterial lesions (anterior circulation, posterior circulation, bilateral circulation); and (4) treatment-related information: antibiotic use and gavage feeding.
Objective laboratory markers were also collected in this study, including (1) blood cell tests: white blood cells, neutrophils, lymphocytes, monocytes, and platelets; (2) renal function tests: urea, creatinine, uric acid, cystatin C; (3) lipid indices: total cholesterol, triglycerides, high-density lipoprotein, lipoprotein alpha; (4) D-dimer; (5) glycated hemoglobin; (6) high-sensitivity C-reactive protein (hs-CRP); and (7) interleukin-6 (IL-6).
During data collection, all investigators involved in retrospective data extraction received standardized training on the study protocols. A uniform data collection form was used to extract key study information from electronic medical records (EMRs), with the accuracy and consistency of all extracted data further verified.
Statistical analysis
All the statistical analyses were performed using SPSS Statistics (version 25; IBM Corp., NY, USA). Measurement data with normal distribution were presented as the means ± standard deviations, while non-normally distributed measurement data were presented as medians (interquartile range). The count data were expressed as percentages (%). A Student’s t-test was performed to analyze normally distributed measurement data between two groups. The rank-sum test was used for non-normally distributed measurement data analysis. The chi-square test or Fisher’s exact test was applied for count data. Binary logistic regression was utilized to explore the factors associated with FI. All candidate variables were force-entered into the multivariate model simultaneously using SPSS’s default “Enter” method, without prior univariate screening. For variables with missing data, complete case analysis was uniformly adopted, with no data imputation conducted, to minimize potential bias. Statistical significance was defined as a two-sided P-value < 0.05.
Following the clinical observational study, a systematic review and meta-analysis was conducted to validate the generalizability of our findings regarding the incidence and risk factors of FI in stroke patients. This approach enabled us to compare clinical data with the pooled evidence from existing literature, addressing potential biases in regional patient demographics.
Systematic review and meta-analysis
The study design followed the Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines. Since this section was a systematic review and meta-analysis, ethics approval and informed patient consent were not required.
Search strategy
A literature search was conducted for studies published between January 1, 1980, and December 31, 2024. The relevant literature was identified through the following steps: (1) searching pertinent articles in the electronic databases: MEDLINE, Embase, Cochrane Database, and Web of Science; (2) using electronic search terms included stroke, cerebrovascular accident/disorder, ischemic stroke, cerebral/brain infarction, brain ischemia, intracerebral/cerebral hemorrhage, bowel dysfunction/disorder, and FI; (3) carefully reviewing the abstract of each article to identify appropriate publications; (4) retrieving and thoroughly reading full-text articles, and also examining all reference lists of relevant articles to identify additional eligible publications; and (5) manually searching references from previously retrieved articles and all eligible studies. The detailed full search strategy is provided in the Supplemental Material.
Study selection
In the process of including and excluding studies, the source of selection and measurement bias was considered in terms of study design, context, and participants.
Studies were included if they reported the incidence of FI in stroke patients. The inclusion criteria were as follows: (1) prospective studies, retrospective cohort studies, or cross-sectional studies; (2) original research on adult human stroke survivors; (3) studies that recruited both stroke and non-stroke participants were included if separate stroke data were provided; (4) the incidence of FI was reported in the study; (5) the study population had a history of stroke; and (6) FI was defined as recurrent uncontrolled, involuntary, or unplanned passage of fecal material.
The following articles were excluded: (1) patients with a prior history of FI before the stroke diagnosis; (2) patients who had suffered from gastrointestinal tract disorders or undergone gastrointestinal surgery in the past; (3) studies with an unclear definition of FI; (4) studies involving a non-adult population; (5) highly selected studies or treatment studies without incidence data; (6) commentaries, single case reports, editorials, and reviews; and (7) non-English articles or articles without full text available.
Data extraction and quality assessment
The following general descriptive information was extracted from each study: (1) first author and year of publication; (2) country of participants, survey date, and survey sites; (3) sample, age, and gender; (4) subtype of stroke; (5) various stages following a stroke; and (6) associated risk factors of FI, including age, gender, type of stroke (ischemia/hemorrhage), stroke severity factors (NIHSS, Barthel Index score, Glasgow Coma Scale, initial urinary incontinence, visual field defect, dysphasia, sensory or visual neglect, dysphagia, assistance with toilet access, assistance with transfers, assistance with stairs), clinical characteristics (Mini-Mental score, urinary incontinence, medication use, lesion size, cortical involvement, Scandinavian Stroke Scales score), psychosocial factors (living situation, district nurse since stroke, home help since stroke, poor social support network, general health perception), and medical history (hypertension, diabetes mellitus, dyslipidemia, coronary heart diseases, atrial fibrillation, preceding TIA, current smoking, former stroke, other disabling disease).
Three authors (X.H., W.Q., and Y.B.) independently selected the studies to be included in the review by carefully reading each article, extracting the data independently, and cross-checking the information. Any disagreement was resolved through discussion until a consensus was reached. Two reviewers (J.L. and T.W.) were consulted if disagreement persisted.
The quality of the included studies was assessed using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for studies, which evaluates methodological quality across nine core domains.16,17 The data from all included studies were clearly tabulated, and deviations were identified and considered during the quality assessment stage.
Statistical analysis
For each included study, information on the first author, year of publication, sample size, and the incidence of FI was extracted and recorded before the pooled incidence calculation. The statistical validity of aggregating the studies was assessed with the I2 statistic for heterogeneity. Pooled incidence estimates and 95% confidence intervals (CIs) were determined by the random-effects model. Forest plots were used to present the pooled effect sizes and their 95% CI. Funnel plots were constructed to evaluate publication bias and other potential small-study effects in the meta-analysis. The meta-analysis was performed using Stata MP software (version 18; Stata Corp., Texas, USA). Subgroup analyses were conducted based on stroke stage (acute stage or rehabilitation stage) and survey sites (hospital or community).
Results
Phase I
Incidence of post-stroke FI
A total of 1359 patients were enrolled in this study. Among them, 220 patients (16.19%) experienced FI and were assigned to the FI group, while 1139 patients (83.81%) formed the FC group.
Clinical characteristics associated with post-stroke FI
Demographic data, medical history, disease-related information, and treatment-related information are presented in Table 1. Due to incomplete medical and imaging records, non-randomly distributed missing data were noted in the clinical variables: stroke subtype (46 missing, 3.38%), stroke stage (332 missing, 24.43%), affected cerebral hemisphere (314 missing, 23.11%), and arterial lesions (125 missing, 9.20%).
Clinical characteristics of stroke patients with versus without FI.
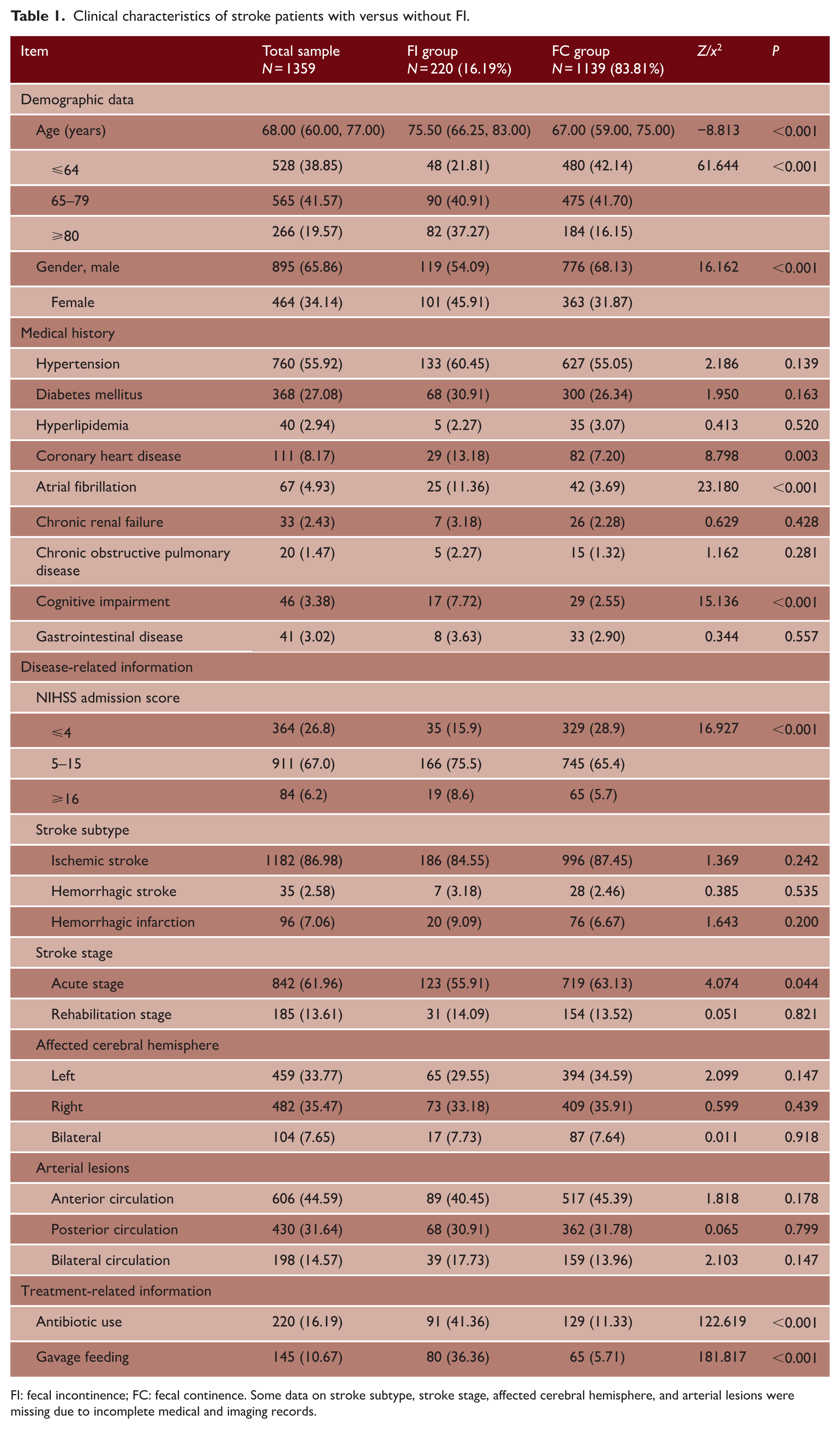
FI: fecal incontinence; FC: fecal continence. Some data on stroke subtype, stroke stage, affected cerebral hemisphere, and arterial lesions were missing due to incomplete medical and imaging records.
A series of significant between-group differences was identified across multiple clinical dimensions. Specifically, there were significant differences in age, gender, coronary heart disease, atrial fibrillation, cognitive impairment, NIHSS admission score, antibiotic use, and gavage feeding (P < 0.01). Patients also showed significant differences between groups in their status in the acute stage (P < 0.05).
Conversely, several other clinical parameters did not demonstrate significant between-group variation. These included medical history such as hypertension, diabetes mellitus, hyperlipidemia, chronic renal failure, chronic obstructive pulmonary disease, and gastrointestinal disease (P > 0.05). In addition, there were no significant differences in the stroke subtype, rehabilitation stage, affected cerebral hemisphere, or arterial lesions (P > 0.05).
Objective laboratory markers associated with post-stroke FI
Results of blood cell tests, renal function markers, lipid profile indices, D-dimer, glycated hemoglobin, hs-CRP, and IL-6 are presented in Table 2.
Univariate analysis of factors associated with FI in stroke patients.
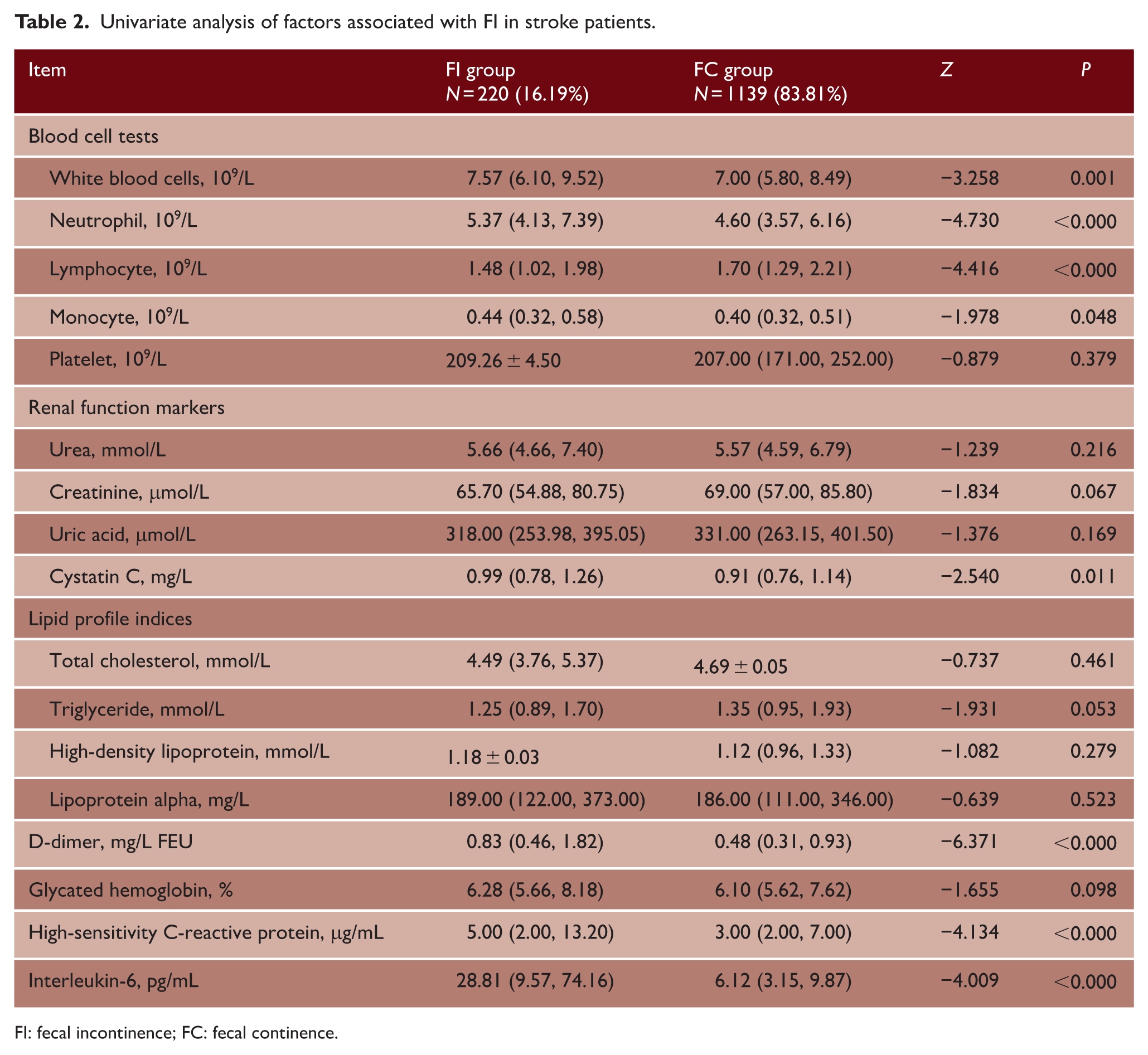
FI: fecal incontinence; FC: fecal continence.
Statistically significant differences were found between the FI group and FC group in white blood cell count, neutrophil count, lymphocyte count, monocyte count, cystatin C, D-dimer, hs-CRP, and IL-6 (P < 0.01, P < 0.05). However, no significant between-group differences were observed in platelet count, urea, creatinine, uric acid, total cholesterol, triglycerides, high-density lipoprotein cholesterol, lipoprotein α, or glycated hemoglobin (P > 0.05).
Binary logistic regression analysis of FI in stroke patients
A logistic regression model revealed that age, gender, cognitive impairment, antibiotic use, and gavage feeding were closely associated with the incidence of FI in the stroke patients.
More specifically, age (odds ratio (OR) = 1.418; 95% CI = 1.119–1.796), the gender (OR = 0.515; 95% CI = 0.363–0.732), cognitive impairment (OR = 2.967; 95% CI = 1.418–6.210), NIHSS admission score (OR = 1.766; 95% CI = 1.337–2.334), antibiotic use (OR = 2.521; 95% CI = 1.654–3.844), and gavage feeding (OR = 5.779; 95% CI = 3.675–9.088) were significantly associated with FI among patients with stroke (Table 3).
Multivariate analysis of factors associated with FI in stroke patients.
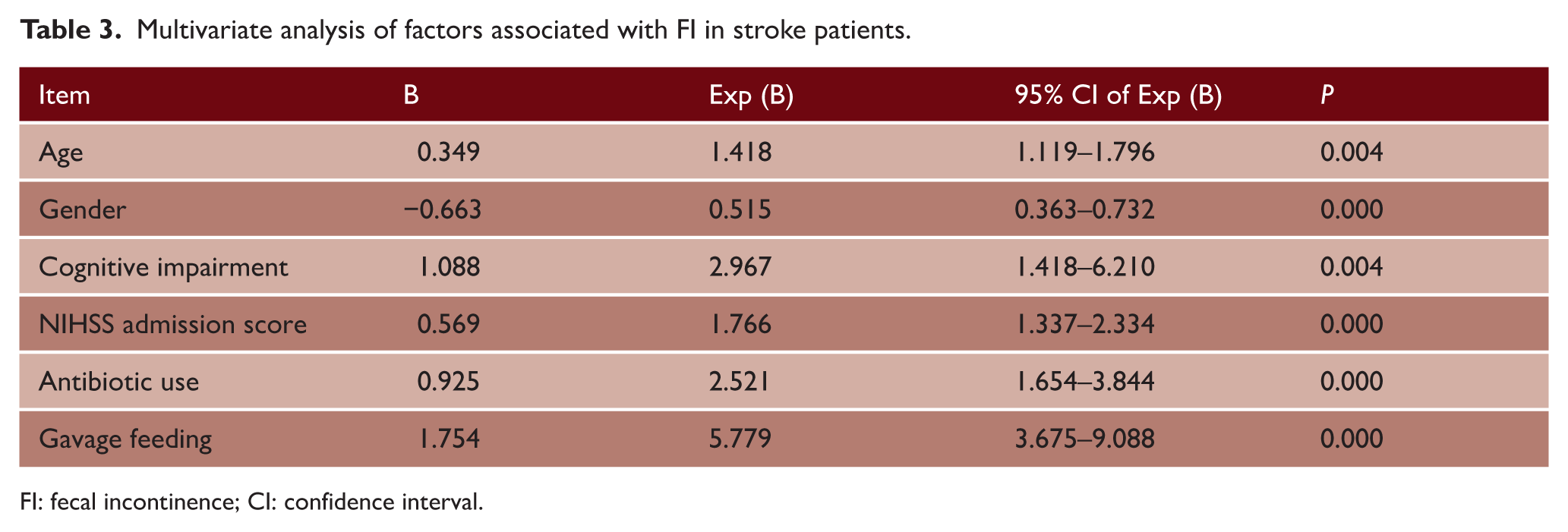
FI: fecal incontinence; CI: confidence interval.
Phase II
Literature review
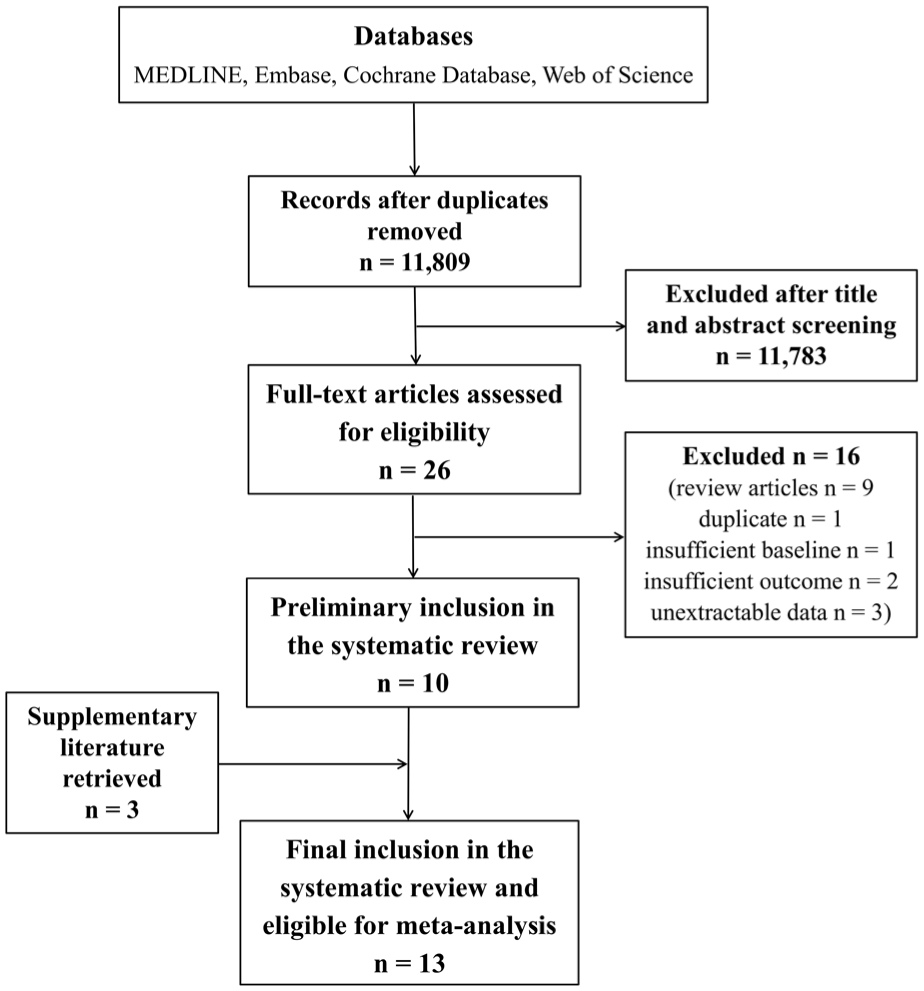
The literature search yielded 11,809 articles, of which 11,783 were excluded after title and abstract screening. A total of 26 full-text articles were assessed for eligibility. Of these, nine were review articles, one was a duplicate, one lacked sufficient baseline data, two provided insufficient outcome data, and three contained unextractable data. After exclusions, 10 eligible studies were selected, with an additional three studies retrieved from manual searching and screening of the reference lists of the included studies. After detailed evaluations, 13 studies were included in the final meta-analysis.18–30 Detailed methodological quality appraisal scores for all included studies (JBI tool) are presented in Table S1, with all studies rated moderate or high quality.
Data from the 13 studies were systematically tabulated with all key elements listed. The flow diagram of the literature search process is illustrated in Figure 1.
The flow diagram of the literature search process.
Study characteristics
The characteristics of the included studies are presented, including the first author, publication year, country, survey date, survey site, total sample size of stroke, gender, age, stroke stage, and samples of FI (Table 4).
Characteristics of included studies investigating the incidence of FI in stroke patients.
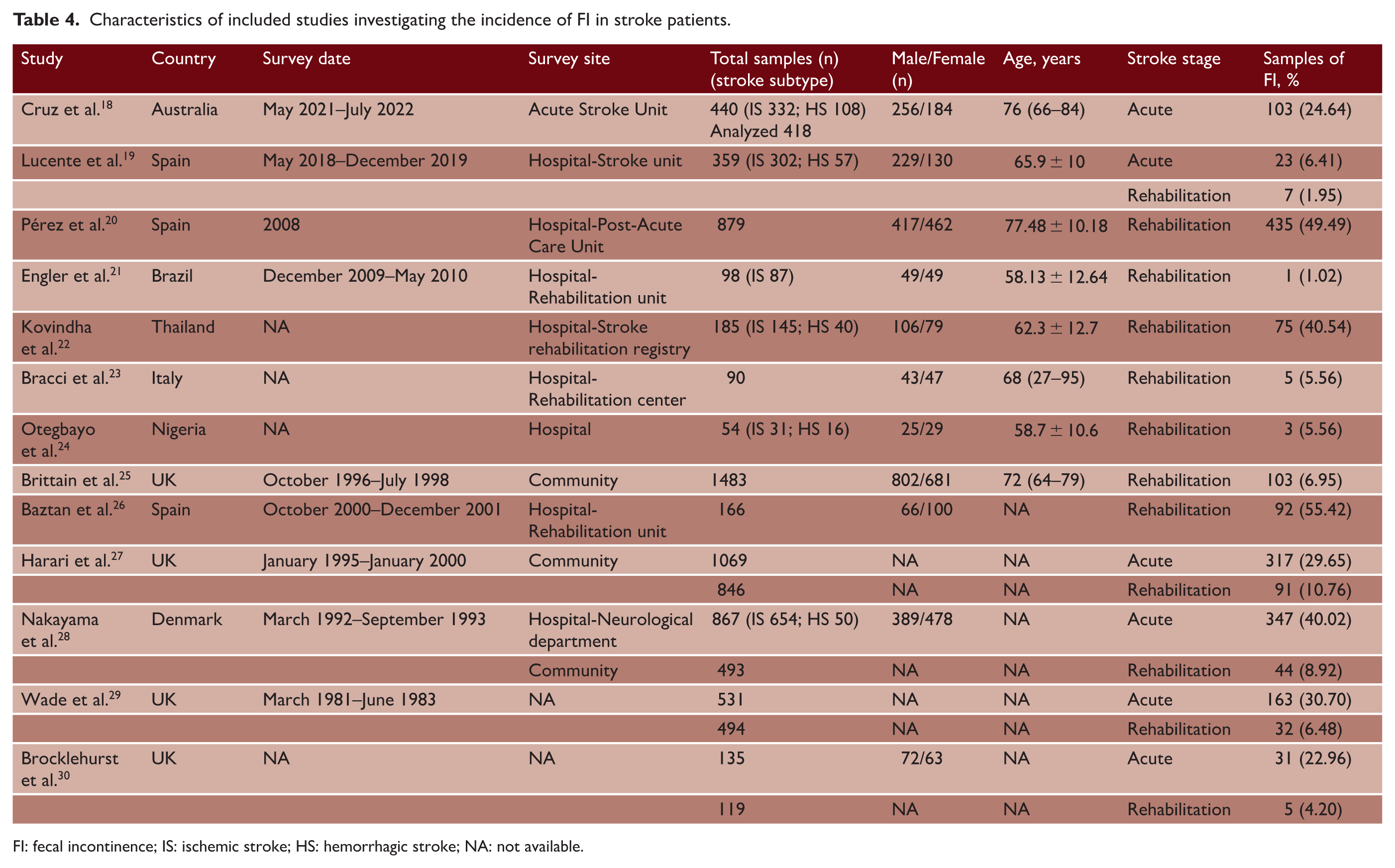
FI: fecal incontinence; IS: ischemic stroke; HS: hemorrhagic stroke; NA: not available.
A total of 6334 stroke patients were investigated, with 1698 patients having suffered FI. The study samples ranged from 54 24 to 1483 25 patients. In terms of survey location, nine studies19,20,23,25–30 were conducted in Europe, one 18 in Oceania, one 21 in America, one 22 in Asia, and one 24 in Africa.
Six studies (3379 patients)18,19,27–30 focused on the acute stroke stage, while 12 studies (5266 patients)19,20,21–30 examined the rehabilitation stage. Nine studies18–24,26,28 involving hospital inpatients included 3116 patients, whereas 3 studies25,27,28 involving community participants included 3045 patients.
Incidence of post-stroke FI and subgroup analysis
The incidence of FI varied significantly, ranging from 1.02% 21 to 55.42%. 26 The forest plot in Figure 2(a) demonstrates an overall FI incidence of 24.42% (95% CI = 15.11–33.72) among stroke patients.
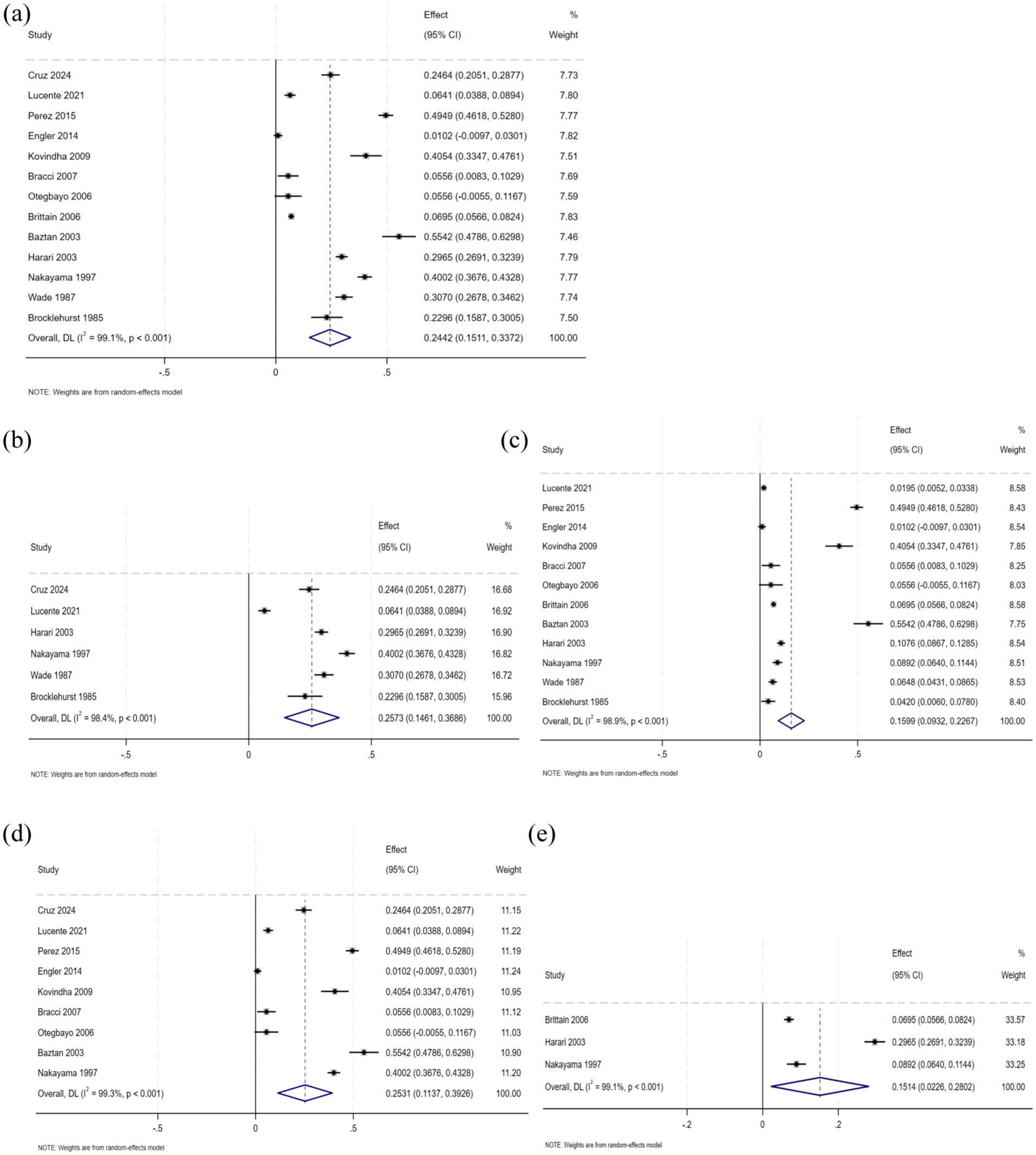
Incidence of FI in stroke patients. (a) The forest plot of the incidence of FI in stroke patients. (b) The forest plot of the incidence of FI in the acute stage of stroke. (c) The forest plot of the incidence of FI in the rehabilitation stage of stroke. (d) The forest plot of the incidence of FI in hospital-based stroke patients. (e) The forest plot of the incidence of FI in community-dwelling stroke patients. FI: fecal incontinence; CI: confidence interval.
Subgroup analysis (Figure 2(b) and (c)) revealed stage-specific incidences of FI. In the acute stage, the incidence of FI ranged from 6.41% 19 to 40.02%, 28 and in the rehabilitation stage, it ranged from 1.02% 21 to 55.42%. 26 The forest plot showed that the incidence of FI was 25.73% (95% CI = 14.61–36.86) in the acute stage and 15.99% (95% CI 9.32–22.67) in the rehabilitation stage.
Figure 2(d) and (e) showed that the incidence of FI in the hospital ranged from 1.02% 21 to 55.42%, 26 and it ranged from 6.95% 25 to 29.65% 27 in community patients. The incidence of FI in the hospital-based stroke patients was 25.31% (95% CI = 11.37–39.26), which was higher than that in the community-dwelling stroke patients (15.14%, 95% CI = 2.26–28.02).
Associated risk factors of FI in stroke patients with statistical significance
Six studies18,19,22,26–28 reported associated risk factors for FI in stroke patients. These factors were categorized into four main types: demographic data, medical history, disease-related information, and treatment-related information.
Table 5 lists the statistically significant risk factors, which fall into four main categories. The first is demographic data, such as age. The second is medical history, including the previous modified Rankin Scale (mRS) and Barthel Index, Charlson Comorbidity Index (CCI), diabetes mellitus, and other disabling diseases. The third is disease-related information, encompassing NIHSS, hemorrhagic stroke (location), Barthel Index, Glasgow Coma Scale (GCS), urinary incontinence, visual field defect, dysphasia, visual and/or sensory neglect, need for assistance with toilet access, Scandinavian Stroke Scale, and lesion size. The fourth is treatment-related information, which covers factors such as anticholinergic medication use.
Associated risk factors for FI in stroke patients.
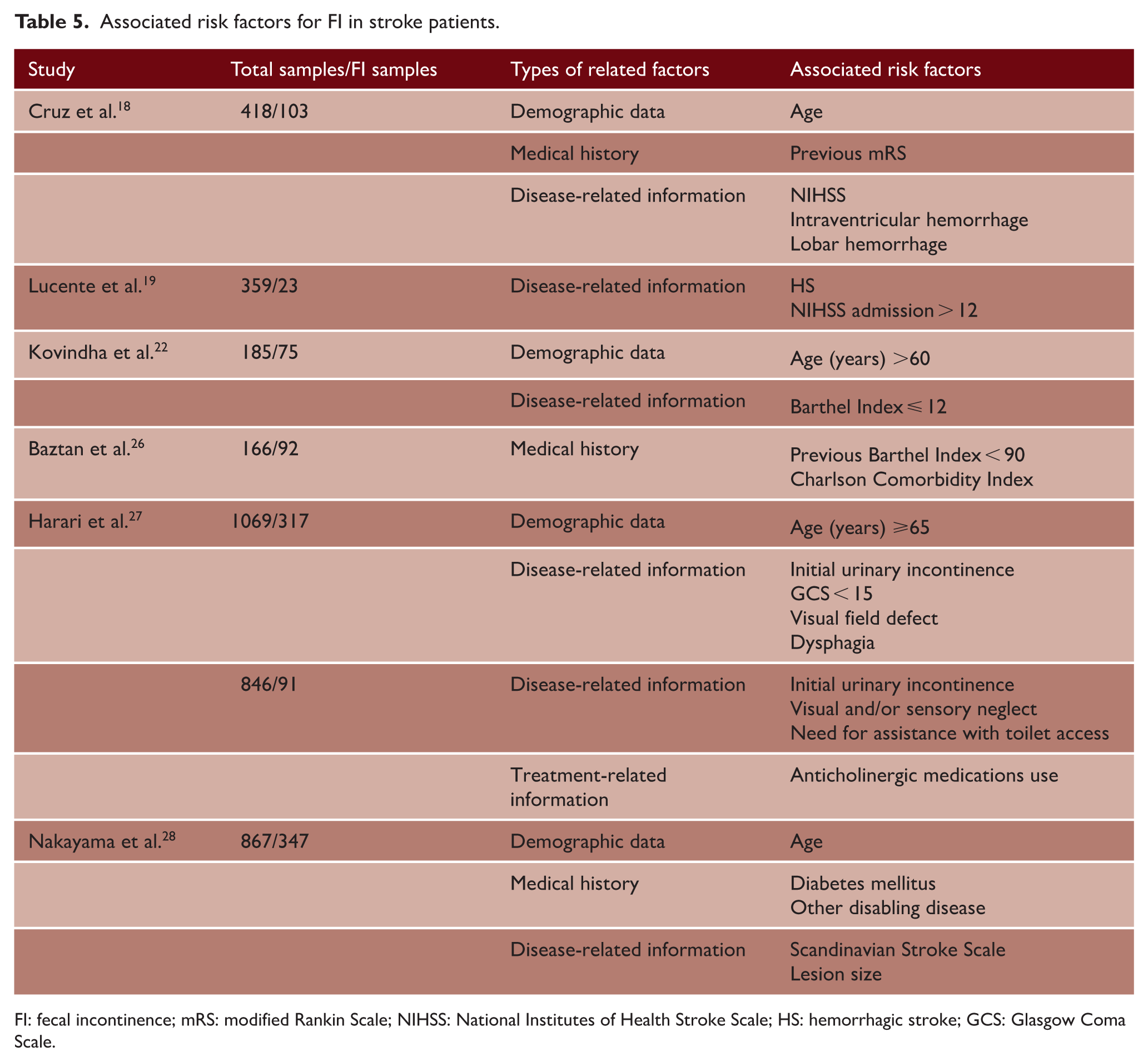
FI: fecal incontinence; mRS: modified Rankin Scale; NIHSS: National Institutes of Health Stroke Scale; HS: hemorrhagic stroke; GCS: Glasgow Coma Scale.
FI after stroke occurs more frequently in aged individuals, those with a medical history of multiple pre-existing comorbidities, diabetes mellitus, or disabling disease. It is also associated with stroke severity, as well as treatment-related factors.
Discussion
The current research aims to investigate the incidence and associated risk factors of FI in stroke patients. In the clinical observational study, the data of stroke patients were analyzed to assess the incidence of FI. Furthermore, multivariate regression analyses were performed to identify associated risk factors. The meta-analysis presented the pooled incidence of FI after stroke, including stroke patients in the acute stage, rehabilitation stage, and those investigated in hospitals and communities. Moreover, the analysis summarized and categorized the associated risk factors from four distinct aspects. This enables a comprehensive comparison between clinical findings and existing evidence. This integrated approach helps to situate the single-center results within the wider literature and provides a more complete overview of post-stroke FI. To clarify the link between the two components, we present the core findings and compare consistencies and differences.
The clinical study showed the incidence of post-stroke FI was 16.19%. This meta-analysis reported its overall incidence was 24.42% (95% CI = 15.11–33.72). The above results suggest that the incidence of post-stroke FI differs across the analyzed studies. This difference may be attributed to multiple potential reasons. For one thing, this clinical study was from a hospital, including acute and rehabilitation patients admitted to a general ward. These patients may have more stable conditions and less severe nerve damage. In contrast, the studies included in the meta-analysis included more patients admitted to stroke units or intensive care units.19,20 These patients were more likely to have more serious neurological damage, which led to a higher incidence of FI. For another thing, the clinical observation study was limited to hospitalized patients, and all patients had received professional and standardized treatment. Meta-analysis included community-based studies with a more representative sample.25,27,28 It included cases with obvious symptoms that did not seek medical assistance, leading to an increase in the overall incidence.
Regarding the comparison of different stroke stages, the clinical study and meta-analysis showed that the incidence of the acute stage is different, while the incidence of the rehabilitation stage is consistent. Compared with the clinical study, the meta-analysis report of FI incidence after acute stroke is higher, which may be due to the above-mentioned similar reasons. As for the consistent results during the rehabilitation phase, there may be the following reasons. First, during the rehabilitation stage, patients had already passed the critical stage of the acute stage, and the degree of neurological impairment remained stable. The recovery or residual state of intestinal function was also more stable.31,32 Second, patients in the rehabilitation stage usually received standardized rehabilitation treatment. This reduced the difference in intervention measures between different studies, and the incidence of FI was more consistent. Third, during the rehabilitation stage, the intestinal diagnosis of FI symptoms was clear. The differences in the definition of rehabilitation stages among different studies have decreased. This reduces the result bias caused by heterogeneity of evaluation criteria.
The analysis of this clinical study showed that post-stroke FI was statistically correlated with demographic data (age, gender), medical history (coronary heart disease, atrial fibrillation, cognitive impairment), disease-related information (NIHSS admission score, acute stage), and treatment-related information (antibiotic use, gavage feeding). There are similarities and differences between the findings of the clinical observation study and the risk factors summarized in the meta-analysis. Both consistently identify age and NIHSS score as key risk factors for post-stroke FI.
This consistency may be attributed to the influence of these reasons. As individuals grow older, the mechanism of gastrointestinal regulation is weakened. Aging was related to the decline of gastrointestinal motility, the reduction in digestive enzyme secretion, the change in intestinal nerve control, and the significant change in intestinal flora.33,34 Notably, three studies22,27,28 observed a significant correlation between age and post-stroke FI, further supporting the role of age in intestinal control disorders. These changes collectively damage the normal function of the intestinal tract, leading to impaired intestinal control. Higher NIHSS scores reflect greater stroke severity, which correlates closely with poor bowel control. Severe neurological impairment from central nervous system damage disrupts brain regulation of intestinal function, leading to loss of voluntary control. In the clinical observational study, additional risk factors were identified. Females are associated with a higher risk of post-stroke FI, possibly due to pelvic floor muscle strength and hormonal effects on gastrointestinal motility. Cognitive impairment also elevates FI risk, as impaired decision-making and reduced awareness of defecatory signals hinder timely bowel management. The use of antibiotics would seriously disrupt the internal environment of the intestinal tract. 35 Antibiotics can also damage the intestinal mucosal barrier function, making harmful substances penetrate the intestinal wall and trigger inflammation.36,37 The gavage feeding method could lead to abnormal intestinal motility patterns, changes in nutrient absorption, and overall intestinal imbalance. All of these collectively contribute to impaired intestinal control. 38
In terms of medical history, the clinical observation study found that coronary heart disease and atrial fibrillation were associated with FI after stroke, while the meta-analysis emphasized that the CCI was a related factor. CCI gathers a variety of comorbidities, reflecting the cumulative burden of systemic diseases. 39 This difference may be because the clinical study focused on specific cardiovascular and neurocognitive conditions, which were directly related to autonomic nerve or vascular dysfunction affecting intestinal motility. The meta-analysis focused on the impact of cumulative scores of multiple diseases on intestinal incontinence after stroke. In addition, diabetes mellitus and previous disability, identified as risk factors in the meta-analysis, did not show a correlation in the clinical study. This difference might be attributed to differences in the study population.
With regard to disease-related factors, the clinical study emphasized the admission NIHSS score and the high incidence of FI in the acute stage. The meta-analysis focused on mRS, hemorrhagic stroke (intraventricular or lobar hemorrhage), Barthel Index, GCS, and specific symptoms, which usually reflect more severe nervous system impairment in the acute phase.40,41 This indicated that the underlying mechanism was consistent. The neurological deficit caused by acute stroke was heavier than that in the rehabilitation stage. Acute stroke directly disrupted intestinal function, leading to intestinal incontinence. 42 Besides, the clinical study did not evaluate the potential effects of anticholinergic medications or length of hospital stay on post-stroke FI.
Objective laboratory markers provide a new insight into studying the associated risk factors of FI in stroke patients. In the clinical study, it was found that there was a correlation between post-stroke FI and white blood cell count with differential counts, as well as cystatin C, D-dimer, hs-CRP, and IL-6.
White blood cell count and differential counts (neutrophils, lymphocytes, monocytes) reflect the activation of systemic immunity. Stroke can trigger a systemic inflammatory cascade. Neutrophils release proinflammatory cytokines43–45 and reactive oxygen species, destroy the intestinal mucosal barrier, and impair intestinal motility. The disorder of lymphocytes and monocytes further indicates an immune imbalance and aggravates the disruption of intestinal homeostasis. Meanwhile, elevated hs-CRP and IL-6 as key markers of systemic inflammation strengthen the occurrence of FI after stroke.46,47 The activation of these inflammatory markers aggravates intestinal dysfunction and leads to loss of intestinal control. Cystatin C is a marker of renal function that can reflect systemic endothelial integrity. Evidence showed that impaired renal clearance in stroke patients could lead to the accumulation of uremic toxins. 48 This damages intestinal epithelial cells and disrupts their movement. D-dimer is an indicator of hypercoagulable and fibrinolytic states, which is elevated due to endothelial injury and prethrombotic state in acute stroke. 49 Intestinal microthrombosis can reduce intestinal mucosal perfusion, cause intestinal ischemia-reperfusion injury, and thereby damage intestinal function. 50 In addition, a hypercoagulable state can destroy lymphatic drainage, leading to intestinal edema and intestinal motility disorders. These findings showed that the associated risk factors of post-stroke FI were correlated with inflammation, renal endothelium, and coagulation.
Although the clinical study and meta-analysis provide complementary insights, both approaches have limitations. The clinical study provided real-time data, but it was limited by its single-center design and restricted survey location. Furthermore, potential temporal variability in assessment and documentation practices may have resulted in inconsistent data recording and introduced misclassification bias. In addition, the simplified stroke stage classification and the lack of data on rehabilitation exposure may be a potential limitation. Although the meta-analysis integrated different studies, it was limited by publication bias. In the future, multi-center research could be carried out in combination with real-world data to improve these findings.
In conclusion, this study combines clinical observation data and systematic evidence from published studies. It emphasizes the incidence and associated risk factors of FI in stroke patients. The incidence of post-stroke FI is high, which is associated with demographic data, medical history, disease-related information, treatment-related information, and objective laboratory markers. In particular, age, gender, cognitive impairment, antibiotic use, and gavage feeding are important factors. It aims to deepen the understanding of intestinal complications and risk factors after stroke. These findings provide the basis for optimizing the clinical management strategies of patients with stroke.
Supplemental Material
sj-doc-1-wso-10.1177_17474930261452825 – Supplemental material for Incidence and associated risk factors of fecal incontinence in stroke patients: From a clinical observational study to meta-analysis
Supplemental material, sj-doc-1-wso-10.1177_17474930261452825 for Incidence and associated risk factors of fecal incontinence in stroke patients: From a clinical observational study to meta-analysis by Jianxiang Li, Xiangyi Han, Wenzhe Qiu, Yuanzhu Bao, Yuanze He, Shengbo Zhang, Yingying Sun, Yuan Yuan, Tianchen Wu, Dejing Ding and Weifeng Guo in International Journal of Stroke
Supplemental Material
sj-docx-2-wso-10.1177_17474930261452825 – Supplemental material for Incidence and associated risk factors of fecal incontinence in stroke patients: From a clinical observational study to meta-analysis
Supplemental material, sj-docx-2-wso-10.1177_17474930261452825 for Incidence and associated risk factors of fecal incontinence in stroke patients: From a clinical observational study to meta-analysis by Jianxiang Li, Xiangyi Han, Wenzhe Qiu, Yuanzhu Bao, Yuanze He, Shengbo Zhang, Yingying Sun, Yuan Yuan, Tianchen Wu, Dejing Ding and Weifeng Guo in International Journal of Stroke
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Scientific Research Project of Jiangsu Commission of Health (Z2024022) and “Double Hundred Plan” for Young Teachers’ Development of Nanjing University of Chinese Medicine (NJUCM Renzi [2024] 48). The funder of the study had no role in study design, data collection, data analysis, or writing of the report.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.