
Abstract
Background:
Endovascular thrombectomy (EVT) is the standard of care for large-vessel occlusion stroke. Medium distal vessel occlusions (MDVO) account for 25–40% of acute ischemic stroke cases, but recanalization rates with intravenous thrombolysis (IVT) are often less than 50%. Recent randomized trials have failed to show better outcomes after EVT versus best medical management in MDVO stroke. The main research question of the study: Is the addition of EVT to IVT associated with benefits or harm when treating patients with MDVO stroke?
Methods:
We performed a retrospective observational study of patients in the Safe Implementation of Treatments of Stroke International Stroke Treatment Registry (SITS-ISTR) 2016–2023, treated with IVT or IVT + EVT for occlusion of the anterior cerebral artery (ACA), posterior cerebral artery (PCA) or distal middle cerebral artery (MCA; M3 and more distal). Only patients with available occlusion data from computed tomographic angiography (CTA) or magnetic resonance angiography (MRA) were included. Patients with M2 occlusions or those treated with EVT only were excluded. Outcomes were acute post-treatment hemorrhage, 3-month modified Rankin Scale (mRS) score, and death at 3 months. Propensity score matching was performed due to baseline imbalances (age, National Institutes of Health Stroke Scale [NIHSS], and occlusion site).
Results:
Of 2198 included patients, 295 (13%) were treated with IVT + EVT, and 1903 (87%) received IVT alone. IVT + EVT patients were younger (73 vs. 75) and had higher median NIHSS: 10 (interquartile range [IQR]: 6–15) versus 8 (5–12), p < 0.001. More IVT + EVT patients were functionally independent (mRS 0-1) before stroke at 91.8% versus 83.0% (p < 0.001). For the IVT + EVT group, PCA occlusion was the most common (n = 179, 60.7%), and distal MCA (n = 1140, 59.9%) in the IVT group. After propensity score matching, IVT + EVT was associated with worse 3-month outcomes compared to IVT alone: mRS 0-1 (35.8% vs. 47.0%, p = 0.016, mRS 0-2 52.4% vs. 63.4%, p = 0.017, and death 21.4% vs. 11.8%, p = 0.005). Symptomatic intracerebral hemorrhage rates were higher in the IVT + EVT group according to European Collaborative Stroke Study II (ECASS II): 6.5% versus 2.4%, p = 0.043, but were similar according to National Institute of Neurological Disorders and Stroke (NINDS): 8.2% versus 4.2%, p = 0.095, and Safe Implementation of Thrombolysis in Stroke Monitoring Study (SITS-MOST): 0.6% versus 1.2%, p = 0.825.
Conclusions:
IVT + EVT for MDVO was associated with worse functional outcomes compared to IVT alone. Our results support recent publications but should be interpreted with caution due to the retrospective observational design, warranting further RCTs.
Introduction
Endovascular thrombectomy (EVT) has been well established in randomized controlled trials as treatment in acute ischemic stroke caused by proximal large-vessel occlusion, both in the anterior and posterior circulation.1–3 Medium distal vessel occlusions (MDVO), however, account for around 40% of ischemic stroke cases, and treatment with intravenous thrombolysis (IVT) is often insufficient for recanalization. 4 Recently, two randomized controlled trials have shown no benefit of EVT in addition to best medical therapy (BMT). Despite methodological differences in inclusion criteria (dominant/non-dominant M2, A1/P1 segments), as well as time window (12 h vs. 24 h), neither trial demonstrated statistically significant benefit nor harm in patients treated with EVT.5,6 The majority of patients had an MCA occlusion, and the most common site was M2 for both trials. Previously, several observational studies have shown conflicting results for EVT in MDVO. Three recent studies on isolated posterior cerebral artery (PCA) occlusion have compared EVT to best medical treatment (BMT), which may or may not include IVT in either group. Two studies have shown an association with better functional outcomes for those treated with EVT without an increased risk for intracerebral hemorrhage.7,8 However, the third study, with a sub-analysis comparing EVT ± IVT versus IVT alone, showed a higher mortality and risk of symptomatic intracranial hemorrhage (SICH) in the EVT group, without a difference in mRS.9,10 In comparisons of EVT with BMT for MDVO, including the anterior circulation, results have similarly varied between lower risk of SICH without higher odds of better functional outcome, or better functional outcome without any differences in risk of SICH or death.11,12 Further randomized controlled trials comparing EVT to BMT in MDVO are ongoing.13,14 In addition, one was recently terminated following a lack of efficacy of EVT for MDVO. 15 In a recent systematic review and meta-analysis comparing EVT with BMT over RCTs and observational studies, the authors found a higher risk of hemorrhage and no evidence of benefit after EVT treatment. 16 The question remains whether there is a selected group of patients with MDVO stroke that benefit from EVT. The aim of this study is to compare the safety and outcomes of treatment with EVT in addition to IVT to IVT alone in MDVO stroke, excluding M2 occlusions.
Methods
The corresponding author had full access to the data in the study and takes full responsibility for its integrity and the data analysis. Access to the anonymized data for this study will be available from the corresponding author upon reasonable request from qualified researchers, contingent on approval by the SITS Scientific Committee. All patients treated with IVT recorded in the SITS International Stroke Treatment Register (SITS-ISTR) between 2016 and 2023, with available occlusion data from CTA or MRA imaging, were considered for this study. MDVO was defined as any isolated occlusion in the anterior cerebral artery (ACA), PCA, or distal segments of the MCA (M3 or more distal). Patients treated only with IVT formed the IVT group, whereas those treated with both IVT and EVT formed the IVT + EVT group. Patients treated only with EVT (without IVT) were not included in the study. Treatment decisions were made at the discretion of physicians at the participating centers.
The SITS-ISTR is an ongoing, prospective, Internet-based, academic-driven, multinational, observational monitoring register for clinical centers using thrombolysis for the treatment of acute ischemic stroke. The methodology of the SITS-ISTR, including procedures for data collection and management, patient identification, and verification of source data, has been described previously.17–19
We used collected data on baseline and demographic characteristics, stroke severity per the standard 15-item, 42-point National Institutes of Health Stroke Scale (NIHSS), time logistics, medication history, and imaging data on admission and follow-up, as well as modified Rankin Scale (mRS) at 3-month follow-up.
Outcomes
Efficacy outcomes were the full range of the mRS, as well as the standard dichotomizations functional independence (mRS 0-2) and excellent functional outcome (mRS 0-1). Safety outcomes were any post-treatment intracerebral hemorrhage, subdivided into hemorrhagic infarction (HI), parenchymal hematoma (PH), as well as SICH per the SITS-MOST, European Collaborative Stroke Study II (ECASS II), and National Institute of Neurological Disorders and Stroke (NINDS) definitions. 20 Death at 3 months was also assessed as a safety outcome. Recanalization per modified treatment in cerebral infarction (mTICI) score was collected for IVT + EVT patients but was not compared as this data was not available in the IVT group. All SICH events were adjudicated centrally by the SITS International Coordination Office based on submitted clinical and imaging reports; images were not available for review.
Statistical analysis
We performed descriptive statistical analyses for baseline demographic, clinical, and imaging data, as well as outcomes, comparing the IVT and IVT + EVT groups. For continuous variables, median and interquartile range (IQR) values were calculated. For categorical variables, percentage proportions were calculated by dividing the number of events by the total number of patients, excluding missing or unknown cases, according to the standard SITS methodology.21,22 Calculations of significance of difference between proportions were performed using the Pearson χ2 method. p Values less than 0.05 (two-tailed) were considered significant.
Outcome analysis was performed with propensity score matching (PSM) analysis to account for clinically and statistically significant baseline differences between the two treatment groups. Age, sex, minor stroke (NIHSS ⩽ 6), and occlusion site (MCA, ACA, or PCA) were chosen as variables after univariate baseline comparison. The propensity score for treatment with IVT + EVT was calculated for each patient, and a nearest neighbor algorithm was used with a ratio of 1:2 and a caliper of 0.1 to compare the two groups. Absolute standardized mean differences were calculated before and after matching to ensure balance in the PSM model (Online Supplemental Figure 1). Binomial logistic regression was performed for the outcomes after matching. Subgroup analyses were performed for occlusions in the anterior (any ACA, M3, or more distal) and posterior circulation (any PCA) separately. Due to residual imbalances, a sensitivity analysis for the outcomes was performed using binomial logistic regression after PSM, with pre-stroke mRS and the full range of the NIHSS added as additional covariates. Statistical analyses were performed in R 4.3.1 (https://www.R-project.org/). Results are reported according to STROBE. 23
Ethics approval and data monitoring
Ethics approval was obtained from the Stockholm Regional Ethics Committee for this project as a part of the SITS-MOST (Safe Implementation of Thrombolysis in Stroke Monitoring Study) II framework (registration number 2022-01157-02). The latest amendment was approved by the Swedish ethics review authority. Ethics approval and patient consent for participation in the SITS-ISTR were obtained in countries where required; the remaining countries approved the register for anonymized audit. The SITS International Coordination Office monitored the SITS-ISTR data online and checked individual patient data monthly to identify errors or inconsistencies.
Results
From the SITS-ISTR, we identified a total of 84,605 patients treated with IVT between 2016 and 2023 from 237 centers in 31 countries. We included 2198 patients with an MDVO stroke, of which 1903 were treated with IVT alone, and 295 were treated with IVT + EVT between 2016 and 2023 (see Figure 1). Table 1 shows a comparison of characteristics between the two treatment groups before and after PSM. Patients in the IVT + EVT group were more commonly male (60.3% vs. 51.2%), younger (median 73 vs. 75 years), had higher baseline stroke severity (median NIHSS 10 vs. 8), as well as different distributions of occluded arteries (PCA: 60.7% vs. 30.4%; distal MCA: 24.1% vs. 59.9%; ACA: 15.3% vs. 9.7%), all p < 0.001. There was also a higher proportion of patients with a baseline mRS score of 0-1 before stroke in the IVT + EVT group (91.8% vs. 83.0%, p < 0.001). Other baseline characteristics were similar between the two groups. After PSM analysis, the effective sample size was 187 in the IVT + EVT group and 355 in the IVT-only group (see Figure 1 and Table 1). Baseline characteristics after PSM had no statistically significant differences in age, sex, proportion of patients with minor stroke, and occlusion site (Table 1). Residual imbalances remained in the proportion of patients with pre-stroke mRS 0-1 (IVT: 82.9% vs. IVT + EVT: 93.5%), as well as the full range of NIHSS score at baseline (IVT: 8, IQR 5–11 vs. IVT + EVT: 10, IQR 6–15). Absolute standardized mean differences after PSM are presented in Supplemental Figure 1.
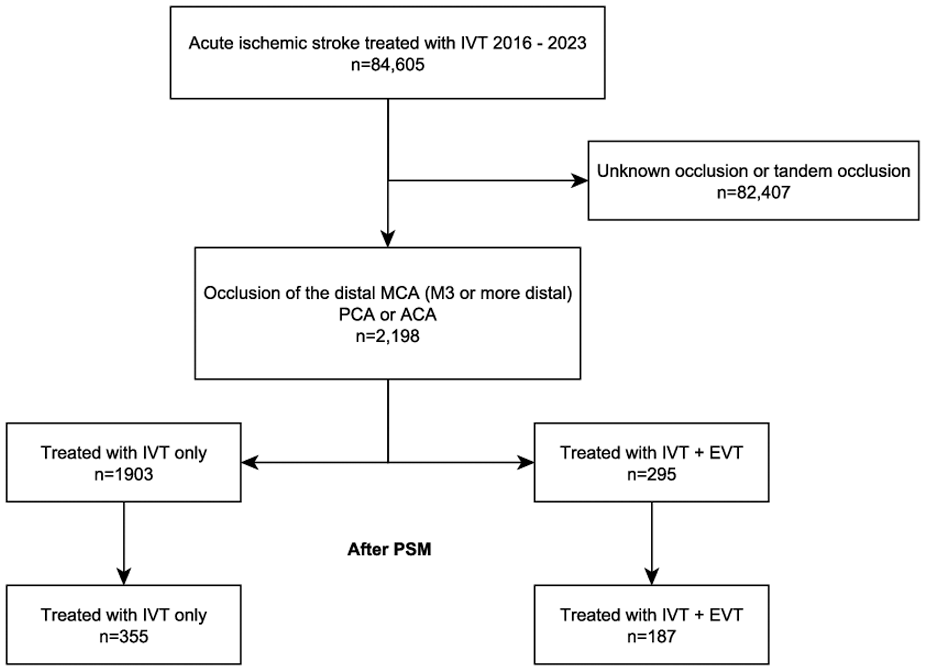
Patient flow diagram. IVT, intravenous thrombolysis; MCA, middle cerebral artery; PCA, posterior cerebral artery; ACA, anterior cerebral artery; EVT, endovascular thrombectomy; PSM, propensity score matching.
Univariate comparison of characteristics between treatment groups before and after propensity score matching.
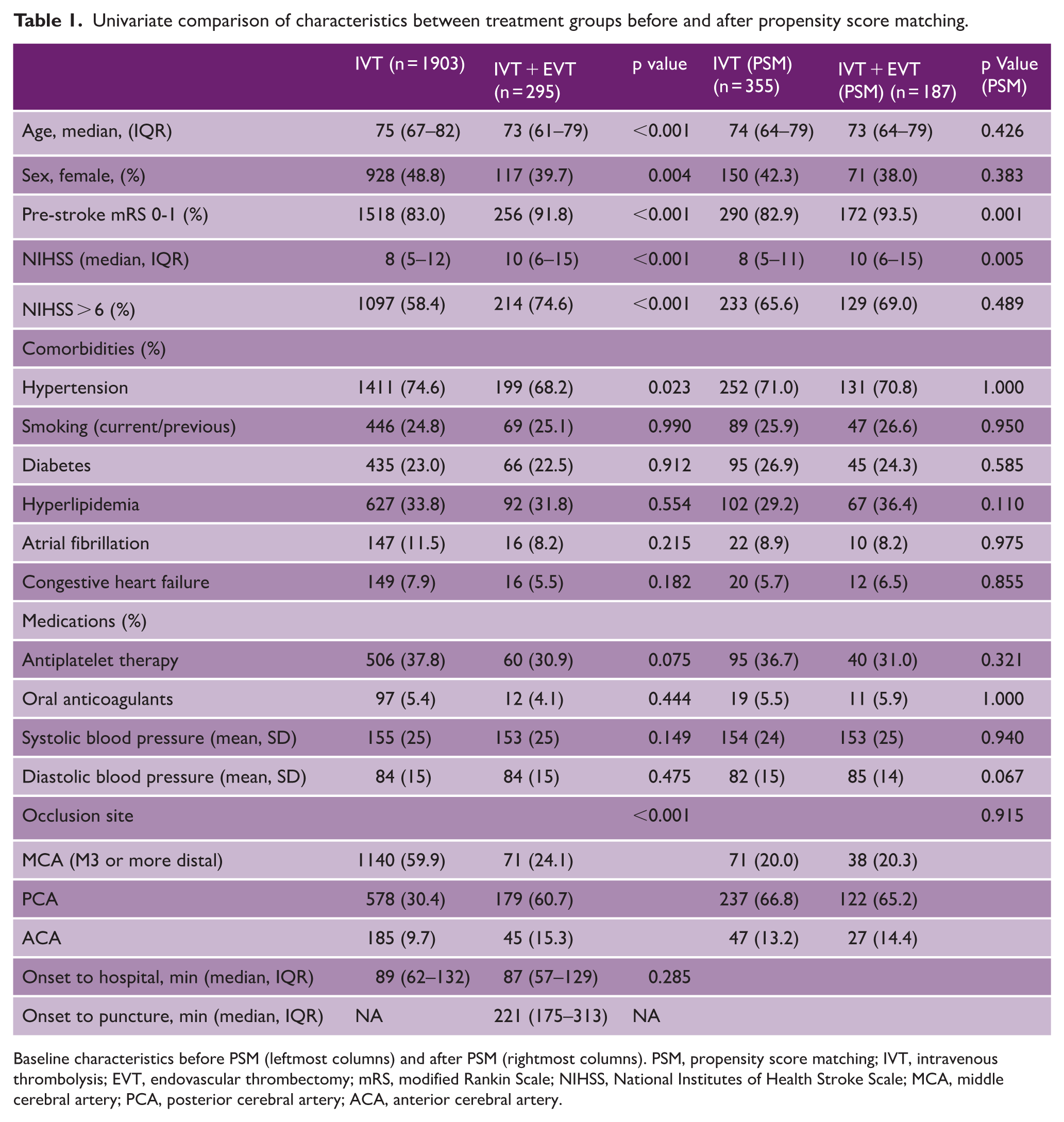
Baseline characteristics before PSM (leftmost columns) and after PSM (rightmost columns). PSM, propensity score matching; IVT, intravenous thrombolysis; EVT, endovascular thrombectomy; mRS, modified Rankin Scale; NIHSS, National Institutes of Health Stroke Scale; MCA, middle cerebral artery; PCA, posterior cerebral artery; ACA, anterior cerebral artery.
Table 2 shows comparisons of outcomes between the two groups after PSM, as well as logistic regression (see Supplemental Table 1 for unadjusted comparisons before PSM). At 3-month follow-up, fewer patients treated with IVT + EVT achieved functional independence (52.4% vs. 64.4%, p = 0.016) or excellent functional outcome (35.8% vs. 47.0%, p = 0.017). More patients in the IVT + EVT group died within 3 months, 21.4% versus 11.8%, p = 0.005. The full range of mRS scores at 3-month follow-up after PSM is shown in Figure 2 (see Supplemental Figure 2 for mRS at 3 months before PSM). For acute bleeding complications, more patients treated with IVT + EVT had a SICH per ECASS II (6.5% vs. 2.4%, p = 0.043), but differences in the rates of PH (4.6% vs. 4.3%), SICH per NINDS (8.2% vs. 4.2%), and SICH per SITS-MOST (0.6% vs. 1.2%) were not statistically significant.
Outcomes after propensity score matching.
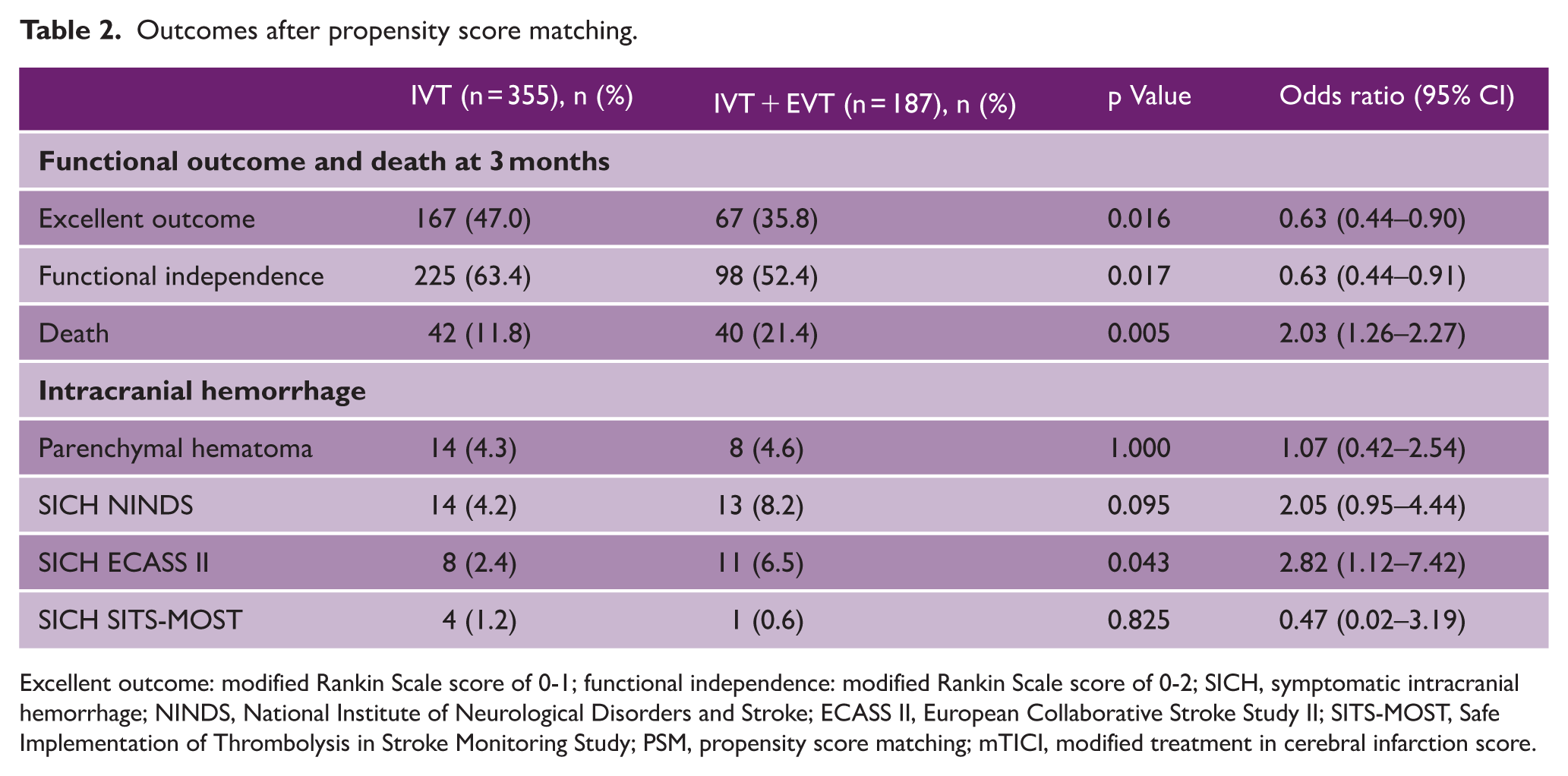
Excellent outcome: modified Rankin Scale score of 0-1; functional independence: modified Rankin Scale score of 0-2; SICH, symptomatic intracranial hemorrhage; NINDS, National Institute of Neurological Disorders and Stroke; ECASS II, European Collaborative Stroke Study II; SITS-MOST, Safe Implementation of Thrombolysis in Stroke Monitoring Study; PSM, propensity score matching; mTICI, modified treatment in cerebral infarction score.
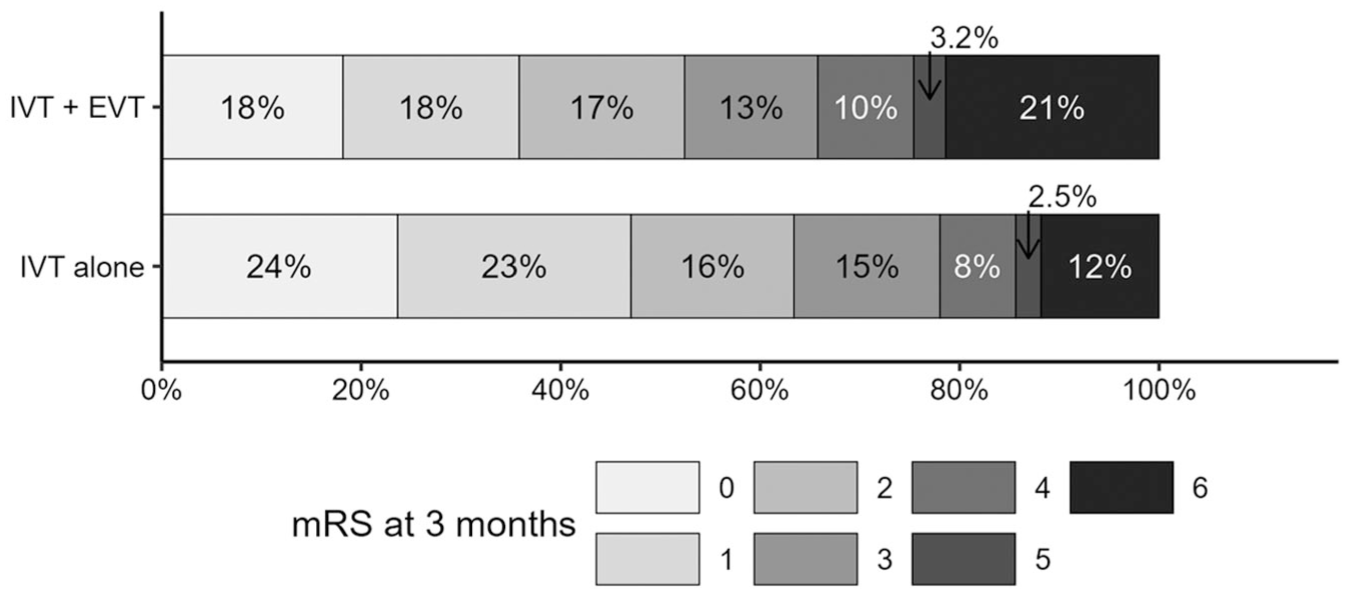
Comparison of mRS distribution after propensity score matching at 3-month follow-up. IVT, intravenous thrombolysis; EVT, endovascular thrombectomy; mRS, modified Rankin Scale score.
Logistic regression after PSM, showed lower odds ratios of excellent outcome (0.63, 95% CI: 0.44–0.90), functional independence (0.63, 95% CI: 0.44–0.91) and a higher odds ratio of death (2.03, 95% CI: 1.26–2.27) at 3 months for the IVT + EVT group. For bleeding outcomes, there were higher odds ratios of SICH per ECASS II (2.82, 95% CI: 1.12–7.42), but not for PH, SICH per SITS-MOST or SICH per NINDS. The sensitivity analysis using multivariate binomial logistic regression after PSM showed similar results (Supplemental Table 2). Subgroup analysis comparing outcomes separately for anterior and posterior circulation stroke after PSM are presented in the Online Supplemental Material. Patients treated with IVT alone had a lower rate of death at 3 months in the posterior circulation subgroup (9.3% vs. 21.0%, p = 0.004; Supplemental Table 3) and had a higher proportion with excellent outcome in the anterior circulation subgroup (55.1% vs. 33.3%, p = 0.012; Supplemental Table 4).
Discussion
This observational study, performed on a large, international stroke registry, found that treatment of patients with MDVO stroke using IVT + EVT was associated with worse outcomes compared to IVT. These results further strengthen the findings of two recently published randomized controlled trials showing no benefit of added EVT compared to BMT alone and highlight the need to evaluate which patients are appropriate for endovascular treatment.5,6
Since the first positive trials in 2015, several studies have widened the indications for EVT, opening possibilities for treatment in previously excluded groups such as those with symptom onset >6 h earlier, basilar artery occlusion, and large infarctions on baseline imaging.2,24–27 Meanwhile, other studies have shown that there may be a limit to the effectiveness of EVT in certain populations, such as those with minor stroke.28,29 In light of these findings, routine use of EVT has expanded dramatically, impacting the inclusion of patients in randomized trials. When compared to the patients included in the HERMES collaboration, patients included in the DISTAL, ESCAPE-MEVO, and DISCOUNT trials were older (median age 74–77 vs. 68), had lower stroke severity (median NIHSS 6–8 vs. 17), and were less often treated with IVT (ranging from 57% to 71% vs. 85%), as well as being randomized at later time-points (234–261 vs. 196 min).1,5,6 Our study, with slightly higher stroke severity, may be more representative of the patients treated for MDVO in routine clinical practice. One explanation for the worse outcomes in our study compared to the recent randomized trials may be the exclusion of all M2 occlusions, some of which may have a more favorable response to treatment with EVT as shown previously. 30
While previous observational studies have compared EVT to BMT for MDVO, this is, to our knowledge, the only study where the entire cohort has been treated with IVT. The added benefit of this methodology is the possibility to compare the addition of EVT for patients with active reperfusion treatment in both groups. We used PSM to increase the comparability of the treatment groups, accounting for clinically relevant baseline differences, as well as a sensitivity analysis using multivariate logistic regression after PSM including pre-stroke mRS and the full range of the NIHSS, which both showed similar results.
This study has several limitations, including those inherent in a retrospective, observational registry-based design, such as risk of bias and missing data. The term MDVO has been used heterogeneously in previous studies, specifically in the categorization of M2, A1, and P1 occlusions. Non-dominant or distal M2 occlusions could not be included in our study, as detailed information of M2 occlusion status was not available in the SITS registry. To avoid proximal or dominant M2 segment occlusions, conditions more similar to proximal large vessel occlusion (LVO) stroke in terms of treatment response, all M2 occlusions were excluded. 30 This limited the comparability of this study to the recent RCTs but allowed for a stronger focus on occlusion sites with a greater clinical uncertainty regarding EVT. Despite the larger lumen of the A1 and P1 segments, they were included as MDVOs based on previous definitions and their use in the DISTAL and DISCOUNT trials.4,5,31 A further limitation was the high proportion of patients with PCA occlusions treated with IVT + EVT at 60.7%, which may limit the generalizability to all MDVO patients. However, the sensitivity analysis with separate comparisons of anterior and posterior circulation occlusions showed similar results. Information on mRS at 3 months was missing in 40% of patients (34% for IVT + EVT and 41% in IVT). However, there was no indication of systematic bias in the missingness of this data. Meanwhile, data availability was over 90% for acute bleeding complications in both groups, showing a higher rate of SICH per ECASS II after IVT + EVT, in line with the functional outcomes. Comparability of the two groups is complicated due to confounding by indication, and the possibility of different levels of care available in a thrombectomy-capable stroke center versus a center only offering thrombolysis. Furthermore, patients treated with IVT + EVT had more severe strokes (median NIHSS 10 vs. 8), which may have been offset by other favorable baseline characteristics: a higher proportion of pre-stroke mRS 0-1 and younger age. However, after PSM, differences in both acute bleeding outcomes and functional outcomes remained statistically significant in favor of treatment with IVT only.
Conclusion
The results from this observational, retrospective study show that treatment with IVT + EVT for MDVO stroke is associated with worse functional outcomes compared to treatment with IVT alone. Future randomized trials should be carefully designed to improve patient selection and choice of endovascular devices and techniques since the risk-to-benefit ratio of IVT + EVT in MDVO may be different compared to that in LVO.
Supplemental Material
sj-docx-1-wso-10.1177_17474930261455992 – Supplemental material for Endovascular thrombectomy in addition to intravenous thrombolysis versus intravenous thrombolysis alone in medium distal vessel occlusions: Results from the SITS International Stroke Treatment Register
Supplemental material, sj-docx-1-wso-10.1177_17474930261455992 for Endovascular thrombectomy in addition to intravenous thrombolysis versus intravenous thrombolysis alone in medium distal vessel occlusions: Results from the SITS International Stroke Treatment Register by Boris Keselman, Michael V Mazya, Daniel Strbian, Ana Paiva Nunes, Andrea Naldi, Danilo Toni, Marco Petruzzellis, Giovanni Frisullo, Dalius Jatuzis, Silvia Strumia, Niaz Ahmed and Tiago Moreira in International Journal of Stroke
Footnotes
Acknowledgements
We thank all SITS-ISTR investigators and their centers for their participation. We also pass on our thanks to all patients who participated in SITS-ISTR. The SITS registry is developed, maintained, and upgraded by Zitelab, Copenhagen, Denmark, in close collaboration with SITS.
Author contributions
The study protocol was drafted by BK, TM, NA, and MVM. It was reviewed and commented upon by all co-authors as well as the members of the SITS Scientific Committee. DS, APN, AN, DT, MP, GF, DJ, and SS were coordinators of data collection at major recruiting centers or countries. Data analysis was carried out by BK with input from TM and NA. BK wrote the final draft of the manuscript. All authors reviewed and made important intellectual contributions to the final draft.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Niaz Ahmed is the chairman of SITS International which received funding from the source described under funding.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Author BK received support from the Swedish Stroke Association (Strokeförbundet) for analysis and writing of the manuscript. SITS-ISTR is financed directly and indirectly by grants from Karolinska Institutet, Stockholm County Council, the Swedish Heart-Lung Foundation, as well as from an unrestricted sponsorship from Boehringer-Ingelheim. SITS is currently conducting studies supported by Boehringer-Ingelheim and Astra Zeneca. SITS has previously received grants from the European Union Framework 7, the European Union Public Health Authority, Ferrer International, EVER Pharma, and Biogen and conducted study in collaboration with Karolinska Institutet, supported by Stryker, Covidien, and Phenox.
Ethical approval
Ethics approval was obtained from the Stockholm Regional Ethics Committee for this project as part of the SITS-MOST (Safe Implementation of Thrombolysis in Stroke Monitoring Study) II framework.
Informed consent
Ethics approval and patient consent for participation in the SITS-ISTR were obtained in countries that required this; other countries approved the register for anonymized audit.
Data availability statement
Access to the anonymized data for this study will be available from the corresponding author upon reasonable request from qualified researchers, contingent on approval by the SITS Scientific Committee.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.