
Abstract
Background:
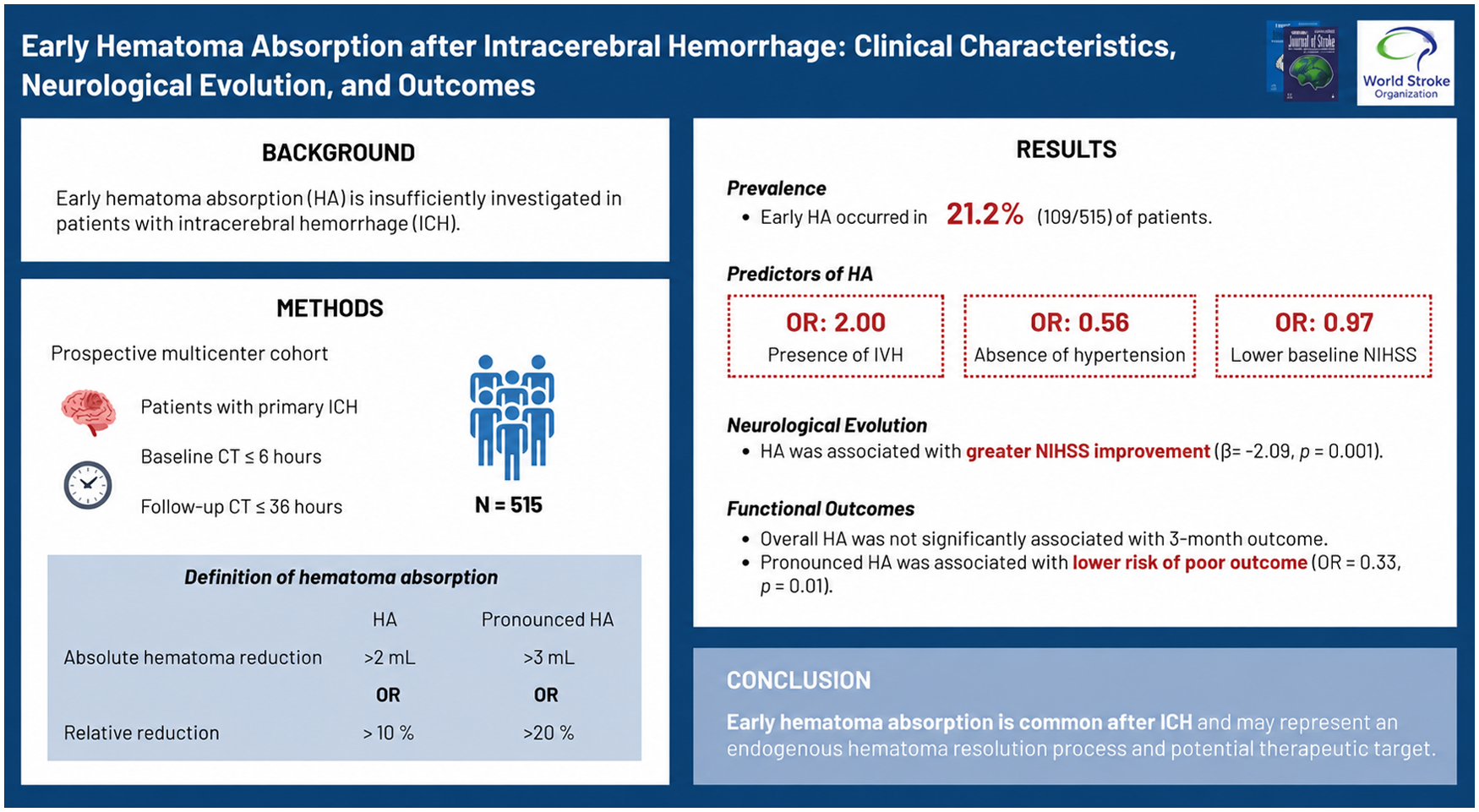
Early hematoma absorption (HA) has been insufficiently investigated in patients with intracerebral hemorrhage (ICH). This study aimed to determine the prevalence of HA and to evaluate its association with neurological and functional outcomes.
Methods:
We analyzed prospectively collected data from patients with primary ICH. Eligible patients underwent baseline computed tomography (CT) within 6 h of symptom onset and follow-up CT within 36 h. HA was defined as an absolute reduction in hematoma volume > 2 mL or a relative decrease > 10%. Pronounced HA was defined as an absolute reduction > 3 mL or a relative decrease > 20%. Early neurological deterioration (END) and early neurological improvement (ENI) were defined as an increase of ⩾ 4 points and a decrease of ⩾ 2 points in the National Institutes of Health Stroke Scale (NIHSS), respectively. Functional outcomes at 3 months were assessed using the modified Rankin Scale (mRS), with poor outcome defined as mRS 4–6.
Results:
Among 515 patients (median age, 60 years; 31.7% female), 109 (21.2%) exhibited early HA. END occurred in 65 patients (12.6%), and ENI in 93 patients (18.1%). In multivariable analyses, HA was independently associated with the absence of hypertension and with the presence of intraventricular hemorrhage (odds ratio (OR), 2.00; 95% confidence interval (CI), 1.19 to 3.36; p = 0.009). HA was also significantly associated with greater neurological improvement, reflected by a larger reduction in NIHSS score (β = −2.093; 95% CI, −3.369 to −0.816; p = 0.001) in adjusted linear regression models. While HA was not associated with 3-month functional outcome overall, pronounced HA was independently associated with a reduced risk of poor outcome (OR, 0.325; 95% CI, 0.133 to 0.795; p = 0.014).
Conclusion:
Early hematoma absorption occurs in approximately one-fifth of patients with acute ICH and is associated with favorable early neurological evolution. These findings suggest that HA may reflect endogenous hematoma resolution processes and represent a potential therapeutic target in ICH.
Introduction
Intracerebral hemorrhage (ICH) is the second most common subtype of stroke and the most lethal form, accounting for approximately 23–29% of all incident stroke cases.1,2 Despite advances in critical care, ICH remains associated with high mortality and disability. 3 Accumulating evidence indicates that dynamic hematoma expansion (HE) during the acute phase of ICH plays a pivotal role in brain injury and is strongly correlated with early neurological deterioration, increased mortality, and unfavorable long-term functional outcomes.4–6 Substantial research efforts have focused on elucidating the prevalence, imaging markers, clinical predictors, and prognostic implications of HE, with the aim of identifying high-risk patients and developing targeted interventions.7,8
In contrast, early hematoma absorption (HA), reflecting the natural process of hematoma clearance and degradation of blood breakdown products, has received comparatively less attention, particularly in relation to early neurological evolution and subsequent clinical outcomes. Prior observational studies have examined early hematoma retraction and suggested that such radiographic changes may not predict long-term functional outcomes.9–11 Notably, its relationship with early neurological changes and short-term clinical trajectories remains unclear. A more comprehensive understanding of early HA may provide important insights into endogenous repair mechanisms, improve prognostic stratification, and inform the development of therapeutic strategies aimed at promoting hematoma clearance while mitigating secondary brain injury. In experimental models of ICH, hematoma resolution is primarily driven by complement-mediated erythrocyte lysis and progressive erythrophagocytosis by activated macrophages. 12 These processes facilitate hemoglobin degradation and iron redistribution, contributing to clot resolution, but may also exacerbate secondary oxidative injury through iron-dependent mechanisms. 13
Accordingly, this study aims to: (1) determine the prevalence of hematoma absorption and identify its predictors; and (2) evaluate the association between hematoma absorption and subsequent neurological and functional outcomes.
Methods
Study population
In the present study, we conducted a retrospective analysis of prospective data derived from 2887 consecutive patients with ICH enrolled in the PRICH (Prognosis and Risk Factors of IntraCerebral Hemorrhage) study. 14 This cohort comprised patients with ICH who were admitted to the Second Affiliated Hospital of Anhui Medical University between August 2022 and March 2025, and to the First Affiliated Hospital of Chongqing Medical University between January 2016 and December 2022. Patients were eligible if they underwent baseline computed tomography (CT) within 6 h of symptom onset and a follow-up CT within 36 h. Exclusion criteria were as follows: (1) intracerebral hemorrhage secondary to identifiable causes (e.g. trauma, vascular malformation, tumor, or hemorrhagic transformation of infarction); (2) primary intraventricular hemorrhage or subarachnoid hemorrhage; (3) poor imaging quality or hematoma evacuation surgery performed before follow-up CT, precluding accurate hematoma volume quantification; and (4) incomplete clinical or follow-up data. Informed consent was obtained. The study protocol was approved by the Institutional Review Boards of the Second Affiliated Hospital of Anhui Medical University and the First Affiliated Hospital of Chongqing Medical University. This study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Clinical variables
Demographic characteristics (age and sex), medical history (including hypertension, diabetes mellitus, and prior stroke), baseline Glasgow Coma Scale (GCS) score, timing of baseline and follow-up CT examinations, hematoma location (lobar, deep, cerebellum, brainstem), and the presence of IVH were systematically collected. Stroke severity was evaluated using the National Institutes of Health Stroke Scale (NIHSS) at admission and 24 h thereafter. Neurological evolution was quantified as the change in NIHSS from baseline to 24-h follow-up. Early neurological improvement (ENI) was defined as a reduction of ⩾ 2 points in the NIHSS score, whereas early neurological deterioration (END) was defined as an increase of ⩾ 4 points in the NIHSS score between baseline and 24-h follow-up. 15 Functional outcomes were assessed at 3 months using the modified Rankin Scale (mRS). Functional independence was defined as a mRS score of 0–2, whereas poor functional outcome was defined as a mRS score of 4–6.
Image acquisition and analysis
All patients underwent baseline and follow-up non-contrast CT with axial reconstruction of 5 mm slice thickness. Hematoma volume was calculated using the edge-detection tool in Analyze 12.0 (Mayo Clinic, Rochester, MN), with semi-automated volumetric quantification applying attenuation thresholds of 44–100 Hounsfield units, followed by visual inspection and manual correction. Measurements were performed by trained clinicians with expertise in neuroimaging analysis, who were blinded to clinical characteristics and study outcomes and demonstrated excellent agreement prior to formal assessment (two-way random-effects intraclass correlation coefficient [ICC] for absolute agreement = 0.993; 95% confidence interval [CI] = 0.983–0.998). Hydrocephalus was defined as ventricular dilatation without corresponding enlargement of the cisternal or sulcal spaces, including dilation of the temporal horns, unilateral or bilateral lateral ventricles, or the third or fourth ventricle caused by intraventricular clot obstruction or mass effect from ICH. 16 Hematoma expansion was defined as an absolute increase in hematoma volume > 6 mL or a relative increase > 33% compared with baseline.17,18 Early hematoma absorption was defined as an absolute reduction in hematoma volume > 2 mL or a relative decrease > 10% (Supplemental Figure S1). These thresholds were informed by analyses using stepwise cut-offs for both absolute (>1, >2, >3, and >4 mL) and relative (>5%, >10%, >20%, and >30%) hematoma reduction. Among these, thresholds of >2 mL and >10% demonstrated the strongest and statistically significant associations with neurological evolution in adjusted models (Supplemental Tables S1 and S2). Pronounced hematoma absorption was defined as an absolute reduction >3 mL or a relative decrease >20%.
Statistical analyses
Continuous variables were presented as mean (standard deviation (SD)) or median (interquartile range (IQR)), as appropriate based on data distribution, and were compared using the Student’s t test or the Mann–Whitney U test, respectively. Categorical variables were expressed as counts (percentages) and were compared between patients with and without hematoma absorption using the χ2 test or Fisher’s exact test, as appropriate. Multivariable logistic regression models were constructed to identify factors independently associated with hematoma absorption. Covariates were prespecified a priori based on clinical relevance, biological plausibility, and prior literature on intracerebral hemorrhage severity and hematoma evolution. The model included age, hypertension, baseline NIHSS score, baseline hematoma volume, presence of IVH, hematoma location, study center, hydrocephalus, time from symptom onset to baseline CT, and the interval between baseline and follow-up CT.11,19 The associations between hematoma absorption, hematoma change rate, and hematoma expansion and clinical outcomes were evaluated using linear regression models for changes in NIHSS scores between baseline and 24 h; binary logistic regression models for END, ENI, functional independence, and poor functional outcome; and ordinal logistic regression models for the distribution of mRS. Model 1 was unadjusted. Model 2 was adjusted for age, baseline NIHSS, baseline hematoma volume, presence of IVH, study center, infratentorial hemorrhage, time from symptom onset to baseline CT, and time interval between baseline and follow-up CT. 20 Multicollinearity was assessed using the variance inflation factor (VIF), and no evidence of significant multicollinearity was observed (all VIF values < 2, Supplemental Table S3). Sensitivity analyses were conducted in patients without baseline IVH and using pronounced hematoma absorption as an alternative exposure. All statistical analyses were conducted using SPSS version 21.0 (IBM Corp., Armonk, NY, USA). A two-sided p value < 0.05 was considered statistically significant.
Results
Baseline characteristics
A total of 515 patients who met the inclusion criteria were included in the final analysis (Figure 1), of whom 109 (21.2%) exhibited hematoma absorption on follow-up CT. The baseline characteristics of included and excluded patients are presented in Supplemental Table S4. Compared with excluded patients, those included in the analysis had a shorter interval from symptom onset to baseline CT (2.33 vs. 15.78 h, p < 0.001), a higher prevalence of hypertension (78.1% vs. 66.6%, p < 0.001), and greater baseline stroke severity, as reflected by higher NIHSS scores (median 11.0 vs. 6.0, p < 0.001). The distributions of absolute and relative changes in hematoma volume are presented in Figure 2. The median age of the study population was 60.0 (IQR, 51.0–70.0) years, and 31.7% were female. The baseline characteristics of the overall cohort and comparisons between the HA and non-HA groups are presented in Table 1. END occurred in 65 patients (12.6%), and ENI in 93 patients (18.1%), with no significant differences observed between the two groups. Compared with patients without HA, those with HA had a lower prevalence of hypertension (69.7% vs. 80.3%, p = 0.018), lower 24-h NIHSS scores (median 8 vs. 11, p = 0.008), a longer interval from symptom onset to baseline CT (2.74 vs. 2.21 h, p = 0.011), and a higher prevalence of hydrocephalus (19.3% vs. 11.8%, p = 0.043) and baseline IVH (41.3% vs. 28.6%, p = 0.011). The median baseline hematoma volume was 10.94 mL and the median baseline IVH volume was 5.59 mL; no significant differences were observed between the two groups in baseline hematoma volume (p = 0.450), IVH volume (p = 0.518), or hematoma location (p = 0.162).
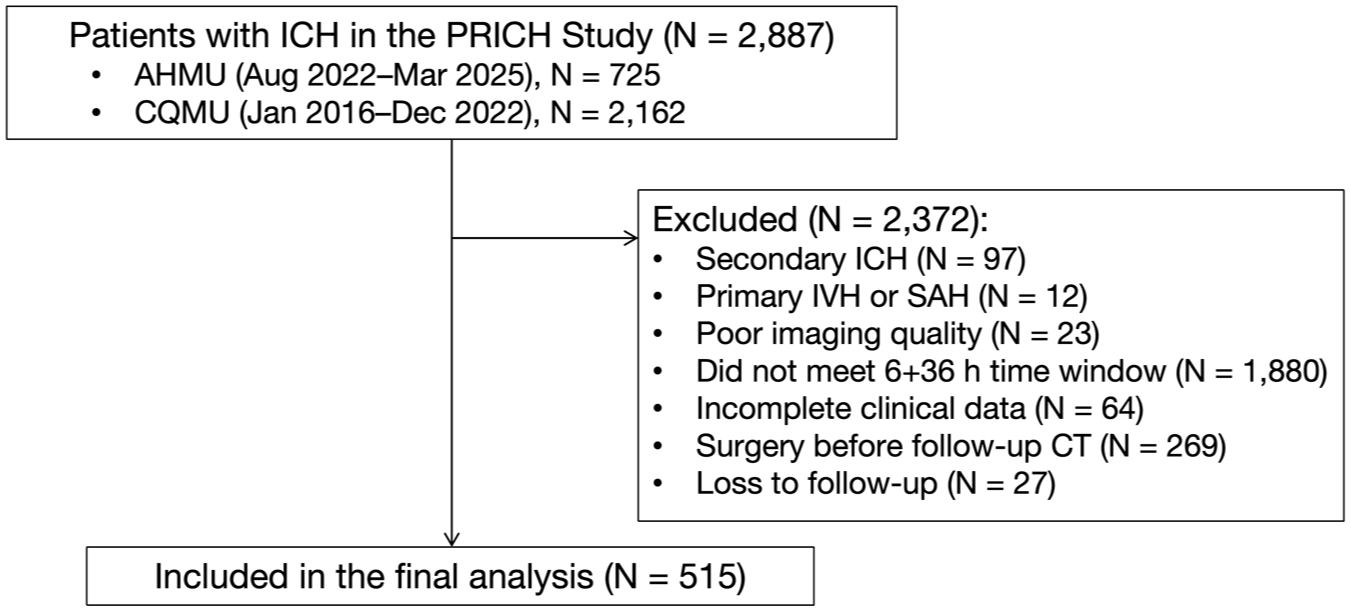
Flowchart of patient selection.
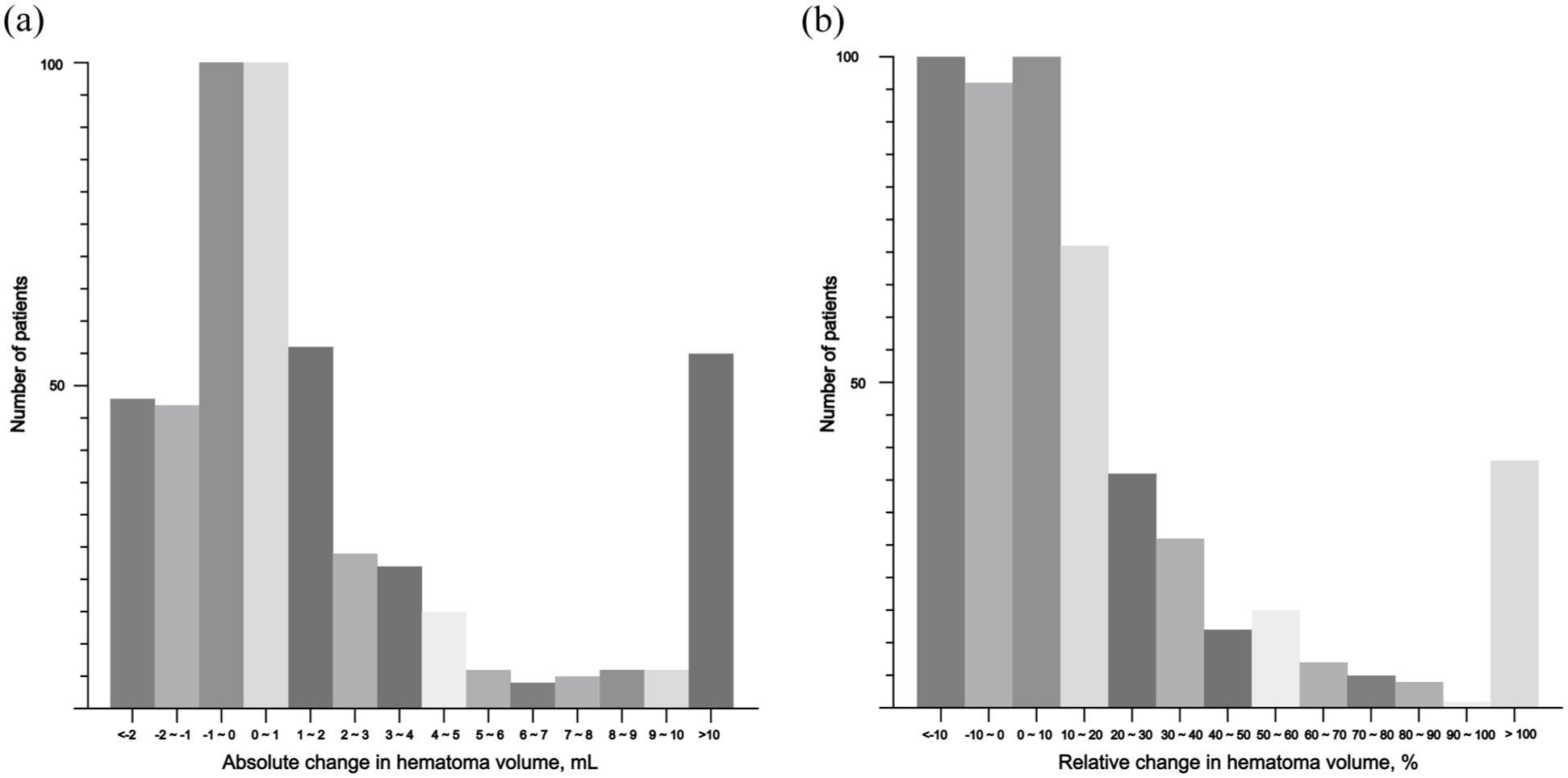
Distribution of absolute and relative hematoma volume changes between baseline and follow-up CT. (a) Absolute volume change: Frequency distribution of the absolute change in hematoma volume. The x-axis represents the change in volume (mL), and the y-axis represents number of patients. Median (interquartile range [IQR]) values were 0.35 mL (−0.61 to 2.43) for all included patients, −1.69 mL (−3.49 to −0.95) for the hematoma absorption (HA) group, and 0.94 mL (0.05 to 3.79) for the non-HA group. (b) Relative volume change: Frequency distribution of the percentage change in hematoma volume relative to baseline. The x-axis represents the relative change (%), and the y-axis represents number of patients. Median (IQR) values were 5.5% (−7.5% to 23.5%) for all included patients, −16.1% (−22.2% to −12.5%) for the HA group, and 11.46% (1.3% to 32.2%) for the non-HA group.
Baseline characteristics.
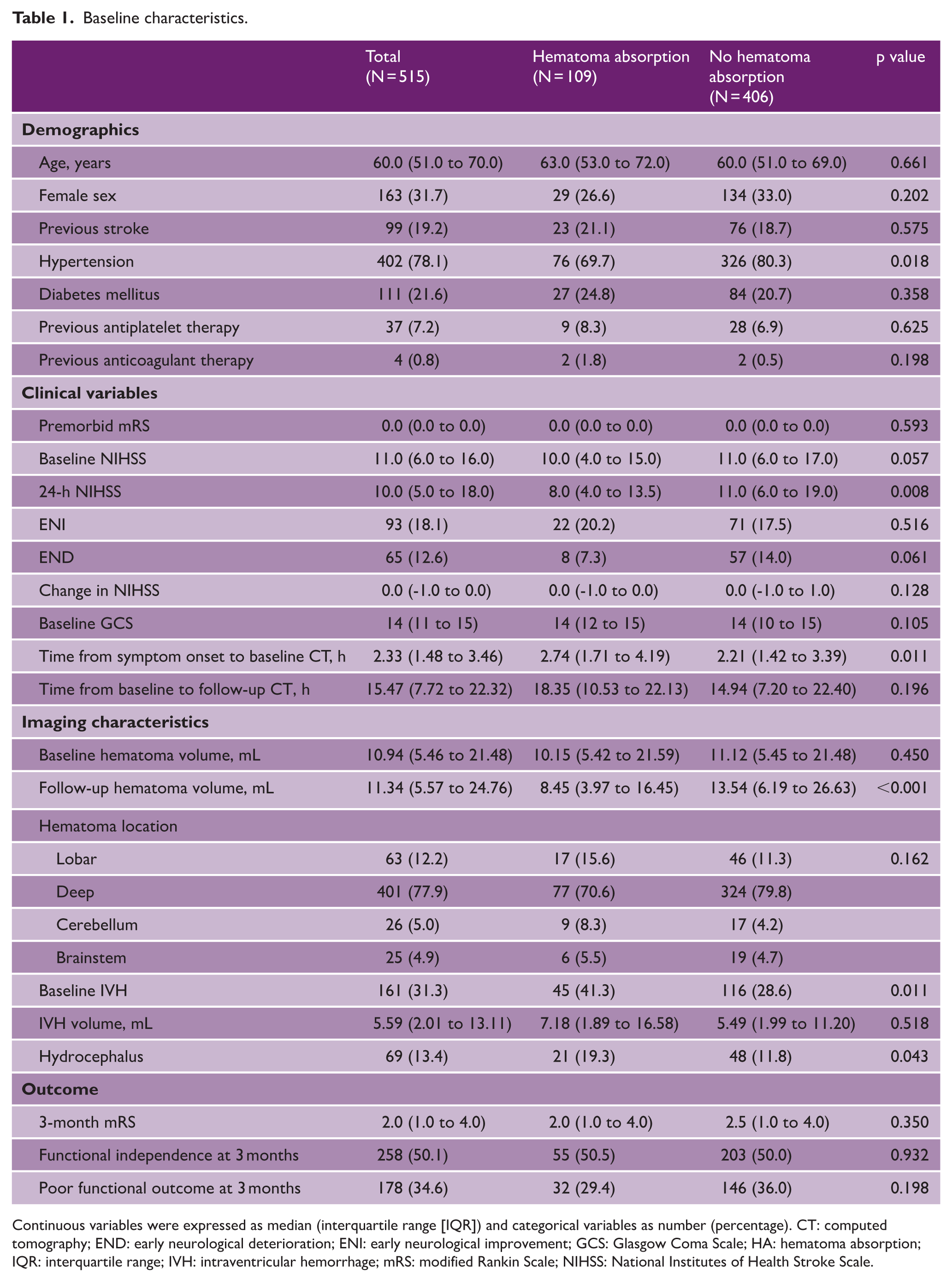
Continuous variables were expressed as median (interquartile range [IQR]) and categorical variables as number (percentage). CT: computed tomography; END: early neurological deterioration; ENI: early neurological improvement; GCS: Glasgow Coma Scale; HA: hematoma absorption; IQR: interquartile range; IVH: intraventricular hemorrhage; mRS: modified Rankin Scale; NIHSS: National Institutes of Health Stroke Scale.
Additional analyses were conducted using pronounced hematoma absorption as the stratification variable (Supplemental Table S5). Consistent with the primary analysis, a lower prevalence of hypertension and a longer interval from symptom onset to baseline CT were observed in patients with pronounced HA (p = 0.005 and p = 0.045, respectively). However, in the subgroup of patients without baseline IVH, no significant differences in clinical and imaging characteristics were identified (Supplemental Table S6).
Predictors of hematoma absorption
Multivariable logistic regression models were constructed to identify independent predictors of hematoma absorption using prespecified covariates selected based on clinical relevance and prior literature. In the overall cohort, absence of hypertension (OR, 0.56; 95% CI, 0.34 to 0.93; p = 0.024), presence of IVH (OR, 2.00; 95% CI, 1.19 to 3.36; p = 0.009) were associated with hematoma absorption after adjustment for age, baseline NIHSS score, baseline hematoma volume, hematoma location, study center, hydrocephalus, and CT timing variables. Lower baseline NIHSS was also independently associated with HA, although the association was modest (OR, 0.97; 95% CI, 0.94 to 1.00; p = 0.044). In addition, lower baseline NIHSS score (OR, 0.95; 95% CI, 0.91 to 0.99; p = 0.009), larger baseline hematoma volume (OR, 1.03; 95% CI, 1.00 to 1.05; p = 0.022), and presence of hydrocephalus (OR, 3.75; 95% CI, 1.73 to 8.16; p = 0.001) were related to pronounced hematoma absorption in the adjusted model (Table 2). In contrast, among patients without baseline IVH, no clinical or radiological factors were independently associated with hematoma absorption (Supplemental Table S7).
Multivariable logistic regression models for predicting hematoma absorption.
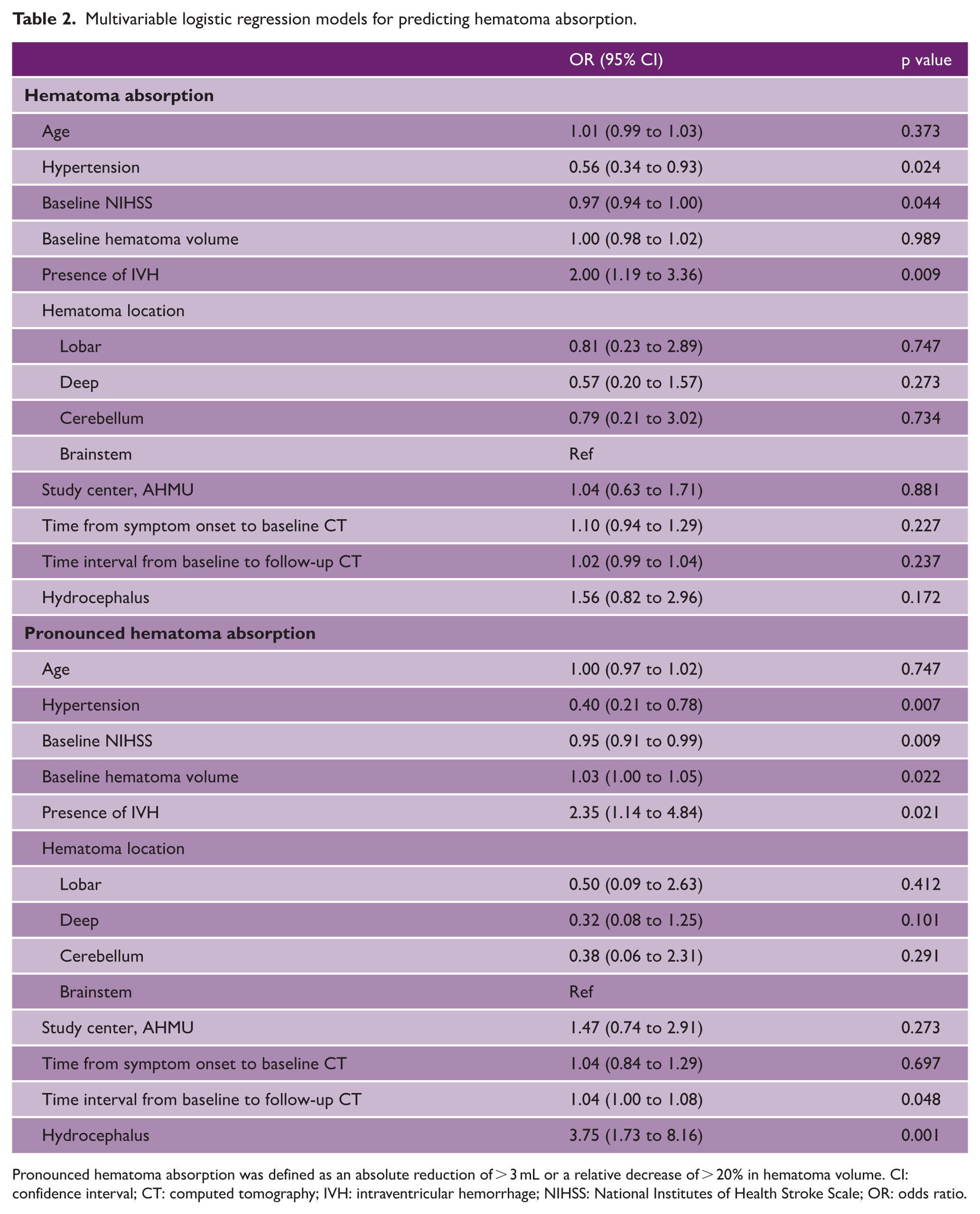
Pronounced hematoma absorption was defined as an absolute reduction of > 3 mL or a relative decrease of > 20% in hematoma volume. CI: confidence interval; CT: computed tomography; IVH: intraventricular hemorrhage; NIHSS: National Institutes of Health Stroke Scale; OR: odds ratio.
Associations between early hematoma absorption and clinical outcomes
Figure 3 illustrates the distribution of mRS scores between the HA and non-HA groups. Hematoma absorption was significantly associated with greater improvement in NIHSS scores from baseline to 24 h in both unadjusted and fully adjusted models (Model 1: β = −1.827, 95% CI −3.152 to −0.503, p = 0.007; Model 2: β = −2.093, 95% CI −3.369 to −0.816, p = 0.001; Table 3). In the subgroup of patients without baseline IVH, hematoma absorption showed a marginal association with NIHSS change (Model 2: β = −1.278, 95% CI −2.710 to 0.153; p = 0.080; Supplemental Table S8). While in the subgroup of patients with IVH, HA was still strongly correlated with reduction in NIHSS score (Model 2: β = −3.701, 95% CI −6.211 to −1.190; p = 0.004; Supplemental Table S9). No significant associations were observed between hematoma absorption and ENI, END, or 3-month functional outcomes (Table 3). However, when pronounced hematoma absorption was considered, a significant association emerged, with a lower risk of poor functional outcome (OR, 0.325; 95% CI, 0.133–0.795; p = 0.014; Supplemental Table S10).
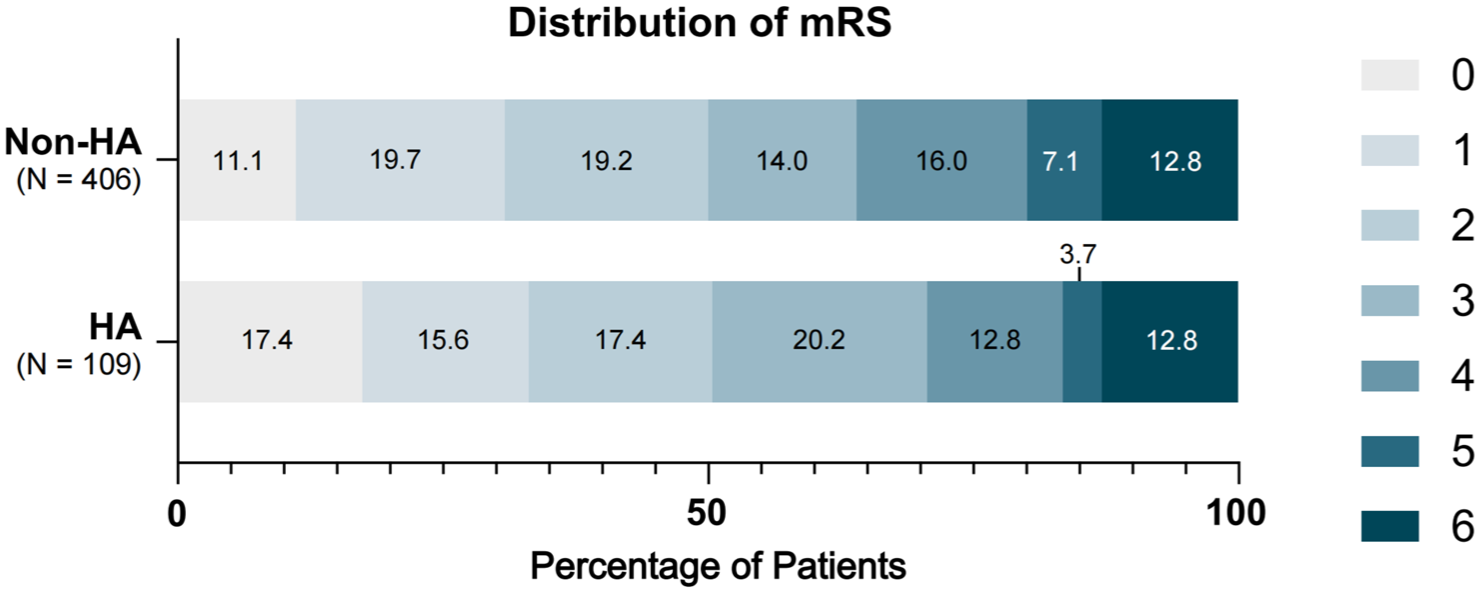
Ordinal distribution of 3-month modified Rankin scale scores according to hematoma absorption.
Association between hematoma absorption and clinical outcomes.
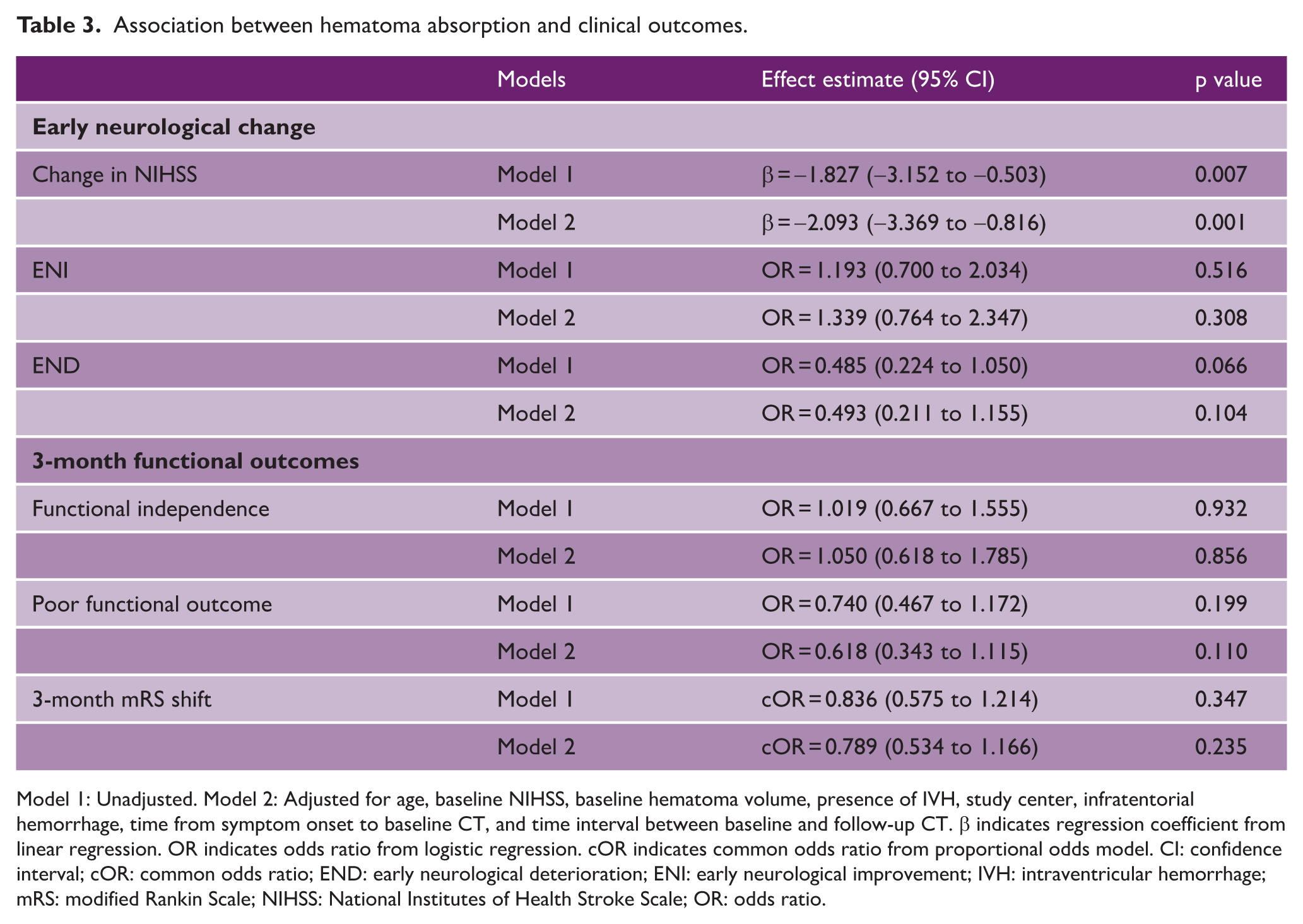
Model 1: Unadjusted. Model 2: Adjusted for age, baseline NIHSS, baseline hematoma volume, presence of IVH, study center, infratentorial hemorrhage, time from symptom onset to baseline CT, and time interval between baseline and follow-up CT. β indicates regression coefficient from linear regression. OR indicates odds ratio from logistic regression. cOR indicates common odds ratio from proportional odds model. CI: confidence interval; cOR: common odds ratio; END: early neurological deterioration; ENI: early neurological improvement; IVH: intraventricular hemorrhage; mRS: modified Rankin Scale; NIHSS: National Institutes of Health Stroke Scale; OR: odds ratio.
We further examined the associations of hematoma change rate and HE with neurological and functional outcomes using fully adjusted models (Supplemental Table S11). Hematoma change rate was significantly associated with a lower likelihood of ENI (OR, 0.410; 95% CI, 0.201 to 0.834; p = 0.014) and a higher risk of END (OR, 1.577; 95% CI, 1.204 to 2.064; p = 0.001). Both hematoma change rate and HE were associated with a reduced probability of 3-month functional independence and an increased risk of poor functional outcome.
Discussion
In this study, early hematoma absorption was observed in approximately one-fifth of patients with acute ICH. Absence of hypertension, lower NIHSS at baseline and presence of IVH were independently associated with hematoma absorption. Although hematoma absorption was associated with short-term neurological changes, it demonstrated only a non-significant inverse association with poor functional outcome. In contrast, both hematoma change rate and hematoma expansion were associated with short-term neurological changes as well as 3 month functional outcomes. These findings suggest that early hematoma absorption may primarily reflect short-term dynamic changes in hematoma structure and perihematomal physiology, rather than substantial reversal of structural brain injury, which is more strongly associated with long-term functional outcomes.
Hematoma absorption is a time-dependent biological process of clearing extravasated blood and degradation products from the brain. Previous studies based on animal models have demonstrated that hematoma resolution is a dynamic process that progresses from initial clot retraction and hemolysis to the active removal of red blood cells and their breakdown products.12,21,22 In the present study, hypertension and the presence of IVH emerged as independent predictors of HA within the multivariable model (Table 2). Hypertension may impair hematoma resolution through vascular instability and altered microvascular function, potentially delaying the transition from active bleeding to clot stabilization.23–26 By compromising perivascular spaces and impairing arterial pulsatility, hypertension may not only exacerbate early tissue injury but also hinder the long-term clearance of neurotoxic blood breakdown products from the brain parenchyma. 27 Although IVH is traditionally associated with poor prognosis in patients with intracerebral hemorrhage, our findings indicate that baseline IVH is independently associated with a higher likelihood of hematoma absorption. This finding may reflect the physiological role of cerebrospinal fluid (CSF) circulation in facilitating the redistribution and clearance of blood products. 28 This rapid absorption may be attributed to the high turnover of CSF and its circulation, which act as major drivers for the dilution and redistribution of blood. Unlike the dense brain parenchyma, the fluid-filled ventricular system permits a potential “washout effect,” facilitating the redistribution and transport of blood products toward CSF drainage pathways, which may lead to an apparent underestimation of parenchymal hematoma expansion. 29 In addition, hydrocephalus exhibited a trend toward a positive association with HA, which reached statistical significance when pronounced HA was used as the dependent variable (Table 2). This relationship may partly reflect the frequent co-occurrence of hydrocephalus with IVH, although no significant multicollinearity was observed between these two variables. Mechanistically, the presence of hydrocephalus may facilitate redistribution of intraparenchymal blood into the ventricular system, contributing to apparent hematoma volume reduction. 29 In the subgroup of patients without IVH, no variables maintained independent significance in the multivariable analysis (Supplemental Table S7). These results suggest that conventional clinical parameters, including age, vascular comorbidities, and stroke severity, exerted less influence on hematoma absorption compared to ventricular communication. Such findings further corroborate the hypothesis that CSF-mediated redistribution associated with IVH may play an important role in radiographic hematoma reduction. Consequently, future studies utilizing NCCT and advanced MRI markers are warranted to refine the imaging predictors of hematoma absorption and to optimize risk stratification and clinical resource allocation. 30
Our findings are consistent with a previous study showing that early hematoma reduction is not strongly associated with long-term functional outcomes, while extending these observations by demonstrating a relationship with short-term neurological changes. 11 In the present study, no significant association was observed between hematoma absorption and early neurological deterioration after adjustment, but a numerical trend toward a lower incidence of END was observed in the HA group (7.3% vs. 14.0%, p = 0.061). In contrast, hematoma absorption was consistently associated with the absolute change in NIHSS score (Table 3), indicating that HA remains independently related to early neurological trajectories even after adjustment for conventional risk factors.20,31 An inverse association between hematoma absorption and poor functional outcome was observed, although it did not reach statistical significance. This association became statistically significant when pronounced hematoma absorption was used as the exposure (p = 0.014, Supplemental Table S10), suggesting that the magnitude of hematoma reduction may be a key determinant of its clinical relevance. Furthermore, among patients without baseline IVH, only a marginally significant association was found between HA and the interval change in NIHSS from baseline to 24-h follow-up (p = 0.080, Supplemental Table S8), whereas in patients with baseline IVH, the association between HA and neurological evolution remained robust (p = 0.004; Supplemental Table S9). This observation may reflect that in the presence of IVH, hematoma volume reduction is facilitated not only by biological absorption but also by redistribution of blood into the ventricular system, thereby producing a more pronounced early improvement in neurological function. These findings indicate that hematoma absorption at minor to moderate scales may reflect limited volumetric changes that are insufficient to produce meaningful long-term functional recovery. Nonetheless, such early reductions can capture transient neurological improvement, and temporal changes in clinical status may provide valuable information for the acute management of ICH patients, including prognosis estimation and guidance for treatment decisions. Previous experimental studies have demonstrated that hematoma resolution is initiated within the first 1–3 days following ICH, with measurable reductions in iron burden observed by day 7.12,13 These observations align with our findings, which characterize hematoma absorption as an early-initiated and dynamically evolving process. A more pronounced influence of hematoma absorption on neurological outcomes may require greater reductions in hematoma volume and longer follow-up periods. Notably, its significant association with early changes in neurological deficits warrants further clinical attention.
While the impact of hematoma expansion on long-term outcomes is well established, the clinical relevance of hematoma absorption remains less clear. Previous analyses of international multicenter data indicate that only severe HE, defined by an absolute increase exceeding 12.5 mL or a relative growth of more than 66%, is independently associated with poor functional outcomes, a trend not consistently observed in mild or moderate expansion. 8 This association is particularly pronounced in the ultra-early stage of hemorrhage. 5 Furthermore, a post hoc analysis of the ATACH-2 trial demonstrated that intensive blood pressure control targeting this ultra-early expansion window was associated with improved functional outcomes. 26 Collectively, these findings suggest that the impact of hematoma volume evolution on patient prognosis is largely dependent on both the timing and magnitude of volume change. The lack of a significant association between hematoma absorption and 90-day functional outcomes may be explained by several factors. First, the magnitude of volume reduction observed in our cohort was relatively modest and may have been insufficient to offset the mass effect and biochemical toxicity induced by the primary hemorrhage. This interpretation is further supported by sensitivity analyses, in which pronounced hematoma absorption was associated with a lower risk of poor functional outcome at 3 months. Second, long-term functional outcomes are predominantly determined by baseline hematoma volume and the extent of early hematoma expansion, both of which may lead to irreversible structural injury to critical neural pathways. 32 As illustrated in Supplemental Figure S1, hematoma absorption primarily manifests as retraction of the lesion border, the pre-existing structural damage is unlikely to be reversed within such a short time frame. The discrepancy between early neurological improvement and long-term functional recovery may reflect the fact that hematoma reduction represents transient physiological processes, such as clot retraction, fluid redistribution, or early resolution of mass effect, rather than true reversal of primary structural brain injury. 33 In addition, long-term outcomes are influenced by multiple factors beyond early hematoma dynamics, including secondary injury processes, medical complications, lesion location, and post-stroke recovery and rehabilitation.34–37 Accordingly, future studies incorporating larger sample sizes and multiple predefined follow-up CT assessments are warranted to more precisely evaluate the impact of substantial hematoma absorption and to further explore its potential as a therapeutic target for improving both short- and long-term outcomes during the acute phase of ICH.22,38 Emerging evidence suggests that endogenous hematoma clearance is closely linked to phagocytic processes and the removal of toxic blood degradation products. 10 Pharmacological strategies that enhance these mechanisms may mitigate secondary injury by reducing the neurotoxicity associated with hematoma breakdown, thereby offering a promising avenue for improving clinical outcomes in patients with ICH.39,40
This study has several limitations. First, given that the objective was to investigate early hematoma absorption, only patients who underwent early follow-up CT within the predefined time window were included. This selection criterion may introduce selection bias and limit the generalizability of the findings to patients presenting at later time points. Second, patients with hematoma absorption had a longer interval from symptom onset to baseline CT, which may introduce time-to-presentation bias and influence the observed associations despite no significant association being observed between this time interval and HA in multivariate regression model. Third, secondary injury processes, such as perihematomal edema, were not systematically evaluated. Further studies are warranted to explore the interaction between edema dynamics and hematoma absorption and their combined impact on functional outcomes. Finally, given the observational design of the present study, causal relationships cannot be inferred, and future research is needed to determine whether hematoma absorption represents a modifiable and clinically viable therapeutic target. In addition, longitudinal studies with larger sample sizes are warranted to more precisely define the optimal cut-off values for hematoma evaluation in predicting long-term functional outcomes.
In conclusion, this study demonstrates that hematoma absorption is common during the acute phase of ICH. Absence of hypertension, lower baseline NIHSS, and IVH were independently associated with HA. Moreover, HA was associated with greater improvement in NIHSS scores. Further research is warranted to clarify its long-term clinical implications and to explore whether modulation of hematoma absorption may represent a viable therapeutic strategy in hemorrhagic stroke.
Supplemental Material
sj-pdf-1-wso-10.1177_17474930261457236 – Supplemental material for Early hematoma absorption after intracerebral hemorrhage: Clinical characteristics, neurological evolution, and outcomes
Supplemental material, sj-pdf-1-wso-10.1177_17474930261457236 for Early hematoma absorption after intracerebral hemorrhage: Clinical characteristics, neurological evolution, and outcomes by Xiao Hu, Zijie Wang, Min Liu, Lei Zhu, Qian Dong, Chu Chen, Juan Li, Xueyun Liu and Qi Li in International Journal of Stroke
Footnotes
Acknowledgements
We thank all the participants and professionals contributing to this study. Qi Li is acknowledged for the original observation and conceptualization of early hematoma absorption.
Author contributions
QL: Study conceptualization. XH, ZW, and ML: Manuscript drafting. XH and ZW: Statistical analysis and visualization. XH, ZW, LZ, QD, CC, JL, and XL: Data curation. QL: Critical revision of the manuscript for important intellectual content and funding acquisition. All authors: Data interpretation and approval of the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by National Natural Science Foundation of China (No. 82471368), Excellent Research and Innovation Team Project of Anhui Province (No. 2024AH010014), Clinical and Translational Research Project of Anhui Province (No. 202427b10020090, No. 202427b10020053), and Health Research Program of Anhui (No. 2024Aa40015).
Ethical approval
The study protocol was approved by the Institutional Review Boards of the Second Affiliated Hospital of Anhui Medical University (YX2025-174) and the First Affiliated Hospital of Chongqing Medical University (2025-413-01).
Informed Consent
Written informed consent was obtained from all participants or their legal representatives prior to study enrollment.
Data availability statement
The de-identified data supporting this study’s findings will be made available upon reasonable request by the corresponding author.
Guarantor
Qi Li.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.