
Abstract
Background:
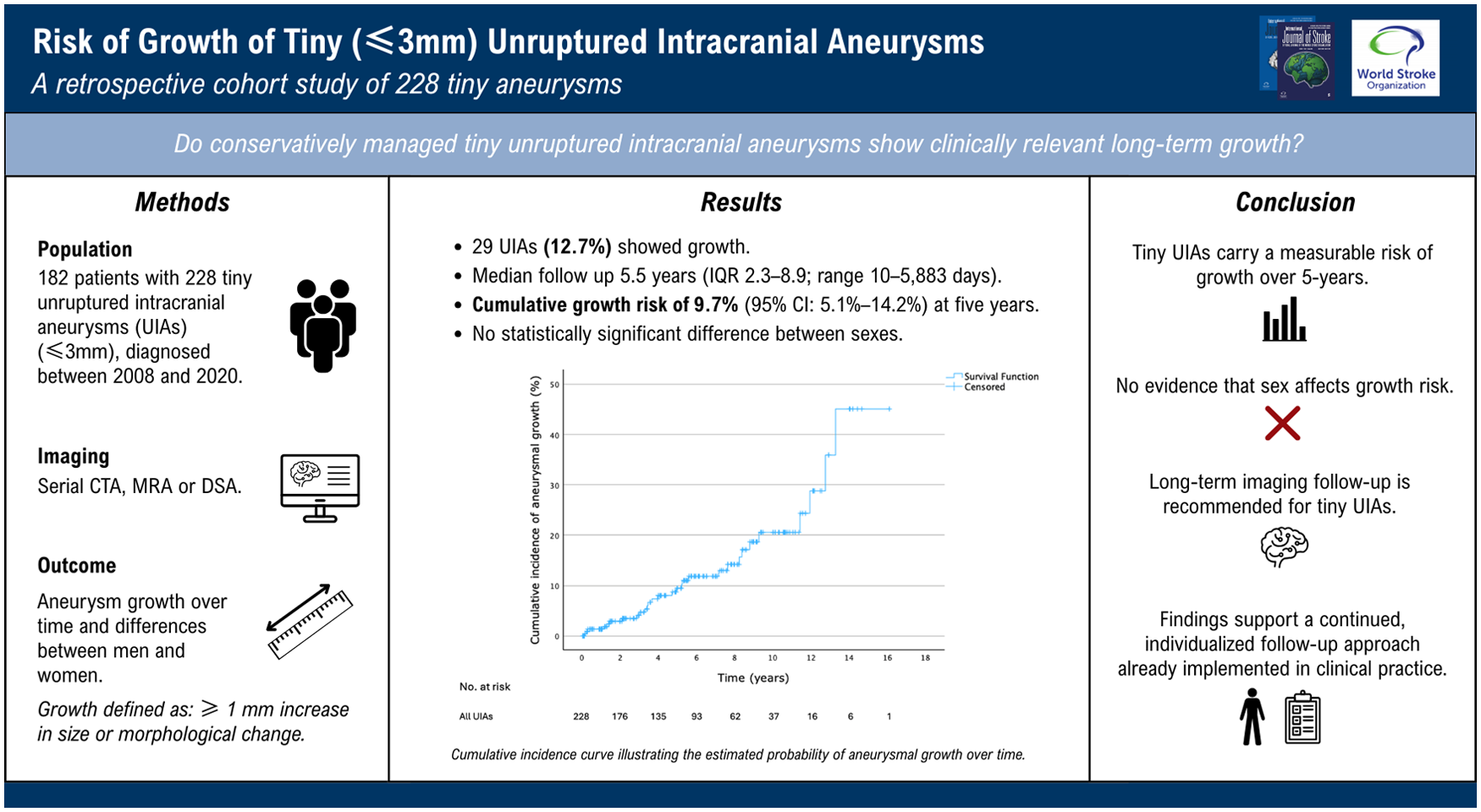
Tiny unruptured intracranial aneurysms, defined as ⩽ 3 mm, are increasingly detected due to advancements in imaging. However, the optimal management approach remains uncertain. Studies have questioned the necessity of long-term radiological monitoring because of presumed low risks of growth, yet robust data are limited.
Aims:
This retrospective cohort study aimed to estimate the 5-year growth risk of conservatively managed tiny unruptured intracranial aneurysms and assess potential differences in growth between men and women.
Methods:
We conducted a single-center retrospective cohort study including adult patients diagnosed with one or more tiny saccular unruptured intracranial aneurysms at a tertiary academic hospital between 2008 and 2020. Patients were included if at least two imaging studies (baseline and ⩾1 follow-up) were available. Growth was defined as a ⩾1 mm increase in size or a morphological change. Growth risk was calculated, and cumulative incidence was estimated using the Kaplan–Meier analysis. Sex differences were analyzed using the log-rank tests.
Results:
A total of 182 patients (142 women; median age = 54 years) with 228 tiny unruptured intracranial aneurysms were followed for a median of 5.5 years. Growth was observed in 29 unruptured intracranial aneurysms (12.7%). The Kaplan–Meier analysis showed cumulative growth of 9.7% (95% confidence interval = 5.1–14.2%) at 5 years. Growth rates were comparable between men and women (p = 0.63).
Conclusions:
Approximately one in eight tiny unruptured intracranial aneurysms demonstrated growth over long-term follow-up, indicating a clinically relevant growth risk despite small initial size. No sex-related differences in growth were observed. These findings support the importance of long-term radiological monitoring. Future studies should investigate whether tiny unruptured intracranial aneurysms may be safely followed with longer surveillance intervals than larger unruptured intracranial aneurysms.
Data access statement:
The data underlying this study are not publicly available due to institutional and ethical restrictions but may be accessed upon reasonable request and subject to approval by the appropriate review committees.
Keywords
Introduction
Unruptured intracranial aneurysms (UIAs) are estimated to occur in approximately 3% in the adult population. 1 The increasing use of advanced neuroimaging techniques has increased detection rates, especially of smaller UIAs that were previously underdiagnosed. 2 Given the potential for rupture resulting in aneurysmal subarachnoid hemorrhage (aSAH), careful monitoring is essential to detect aneurysm growth, which is associated with an increased risk of rupture.3,4 Detecting growth enables timely reassessment of treatment strategies, balancing the risks of preventive intervention against rupture risk.5–8
Current monitoring strategies are applied uniformly to all UIAs regardless of size. However, previous research suggests that tiny (⩽3 mm) UIAs differ in their natural history and treatment outcomes compared to larger ones.9,10 Despite their relatively low absolute risk of rupture, tiny UIAs account for a substantial proportion of aSAH cases. 11 This paradox highlights a persistent clinical dilemma in the management of tiny UIAs. A decision analysis using a Markov model questioned the necessity of long-term surveillance for these UIAs and suggested that routine follow-up imaging may lead to unnecessary interventions without improving patient outcomes and potentially reducing quality-adjusted life years (QALYs). 12 However, as the model was based on theoretical assumptions rather than long-term follow-up data, its conclusions underscore the need for empirical studies specifically focused on tiny UIAs.
In addition, previous studies have shown that women are at higher risk of aneurysm growth and rupture,13,14 but these findings have not been specifically examined for tiny UIAs. Understanding the potential sex-related differences for tiny UIAs could have important implications for individualized monitoring strategies.
The present study aims to estimate the 5-year growth risk of conservatively managed tiny UIAs and to explore potential sex differences.
Patients and methods
Study design and population
We performed a single-center, retrospective cohort study using data from adult patients diagnosed with one or more UIAs at the University Medical Centre Utrecht (UMCU), a tertiary academic hospital in the Netherlands. Patients were eligible if they had at least one incidental saccular UIA measuring ⩽3 mm in both width and length, diagnosed between 2008 and 2020, and if at least two imaging studies (baseline and at least one follow-up) were available. The threshold of ⩽3 mm was chosen in line with prior studies defining “tiny” UIAs12,13 and provides consistency with the literature on the definition of very small UIAs. Available imaging was obtained using computed tomography angiography (CTA), magnetic resonance angiography (MRA), or digital subtraction angiography (DSA). When patients had multiple aneurysms, only those measuring ⩽3 mm were included in the analysis. Patients with monogenetic hereditary conditions predisposing to aneurysm formation (e.g. autosomal dominant polycystic kidney disease) were excluded.
Data collection
Clinical and imaging data were extracted from electronic health records and radiology reports. The date of diagnosis was defined as the earliest scan on which the UIA could be identified. Initial UIA dimensions were remeasured by trained researchers, neurologists, or neuroradiologists using a standardized protocol. Size was defined as the maximum length or width of the aneurysm, measured on multiplanar reconstructions. Aneurysm growth was primarily determined from multidisciplinary neurovascular conference reports. If these assessments were unavailable, growth was evaluated by reviewing serial measurements reported in radiology reports, regardless of whether growth was explicitly mentioned. Follow-up duration was defined as the time from the date of diagnosis to the date of the last available imaging study, which served as the censoring point. During follow-up, the occurrence of aSAH and any preventive treatment of the UIAs were recorded.
Outcome measures
The primary outcome measure of this study was aneurysm growth, defined as an increase in aneurysm size of ⩾1 mm or a morphological change observed on follow-up imaging, including the appearance of a bleb, an aneurysm wall protrusion, or an additional lobe, in line with established recommendations. 15 Because aneurysmal growth is thought to occur in an irregular and discontinuous manner, 16 the exact timing of growth could not be established. For this study, the moment of growth was defined as the date of the first imaging study on which growth was detected.
Statistical analysis
Analyses were performed using IBM SPSS Statistics (version 30.0). The cumulative incidence of aneurysmal growth at 1, 2, and 5 years was estimated using the Kaplan–Meier analysis. If exact time points were unavailable, linear interpolation was used to estimate incidence and standard errors. Differences in time to growth between sexes were assessed using the log-rank test.
Results
Between 2008 and 2020, 990 patients were diagnosed with one or more UIAs at the UMCU, totaling 1397 UIAs. Of these, 182 patients with 228 tiny UIAs (⩽3 mm at time of diagnosis) met the inclusion criteria for this retrospective cohort study (Figure 1).
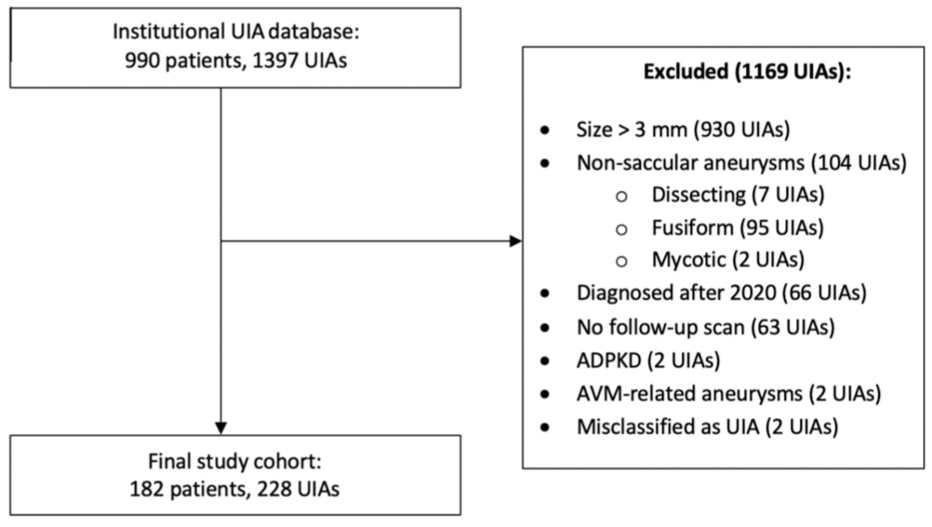
Flowchart of patient inclusion and exclusion. ADPKD = autosomal dominant polycystic kidney disease; AVM = arteriovenous malformation.
Patient and UIA characteristics
The median age of the patients was 54 years (interquartile range (IQR) = 48–64; range = 19–92 years). Baseline characteristics are shown in Table 1. In total, 180 of the included aneurysms originated from 142 women, corresponding to 78.9% of all UIAs. The median follow-up time was 5.5 years (IQR = 2.3–8.9; range = 10–5883 days). The median aneurysm size at baseline was 2.4 mm (IQR = 1.9–2.9; range = 1.0–3.0 mm). Most UIAs were located at the middle cerebral artery (n = 100, 43.9%), followed by the internal carotid artery (n = 40, 17.5%) and the vertebrobasilar arteries and their branches (n = 33, 14.5%).
Baseline characteristics.
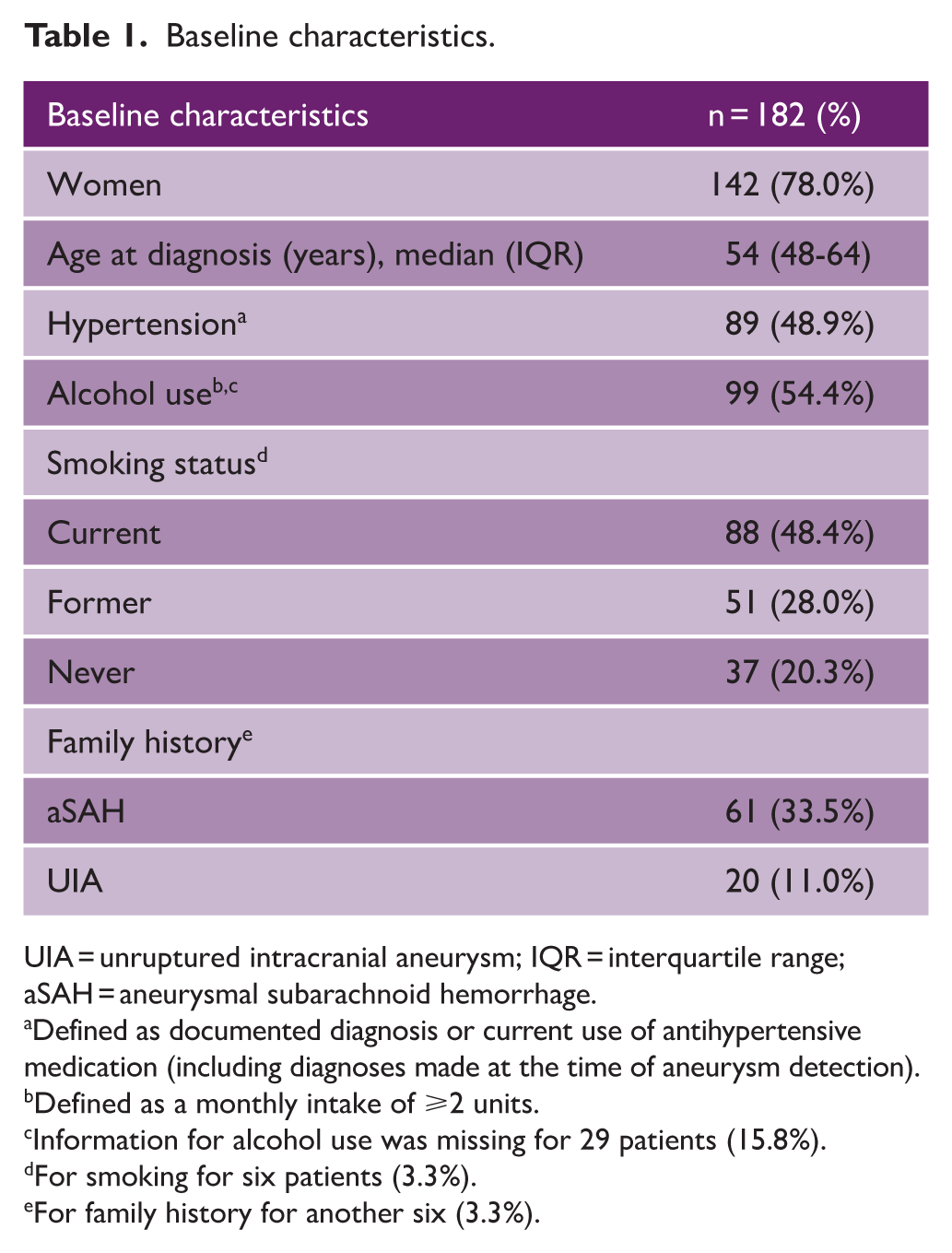
UIA = unruptured intracranial aneurysm; IQR = interquartile range; aSAH = aneurysmal subarachnoid hemorrhage.
Defined as documented diagnosis or current use of antihypertensive medication (including diagnoses made at the time of aneurysm detection).
Defined as a monthly intake of ⩾2 units.
Information for alcohol use was missing for 29 patients (15.8%).
For smoking for six patients (3.3%).
For family history for another six (3.3%).
Aneurysmal growth
A total of 29 tiny UIAs in 28 patients showed growth (12.7%) (Table 2). An example of aneurysm growth observed during follow-up is shown in Figure 2. The cumulative follow-up time until growth occurred was 1263 aneurysm-years, corresponding to an annual growth rate of 2.3% per aneurysm-year (95% confidence interval (CI) = 1.5–3.1%). Among the UIAs that grew, the median absolute increase in size was 1.90 mm (IQR = 1.55–2.24). The median follow-up duration for aneurysms that showed growth was 8.1 years (IQR = 6.3–9.5). The median follow-up duration of all UIAs, regardless of growth, did not differ between men and women (p = 0.43). Also, no association between sex and aneurysm growth rate was found: six of 48 (12.5%) UIAs in men showed growth compared to 23 of 180 (12.8%) UIAs in women (p = 0.82). The Kaplan–Meier analysis showed a cumulative aneurysmal growth rate of 1.8% (95% CI = 0.1–3.6%) at 1 year, 3.4% (95% CI = 0.9–5.9%) at 2 years, and 9.7% (95% CI = 5.1–14.2%) at 5 years (Figure 3). Stratification by sex revealed no statistically significant difference in time to growth (p = 0.63; Figure 4).
Growth characteristics and clinical outcomes of unruptured intracranial aneurysms (UIAs).
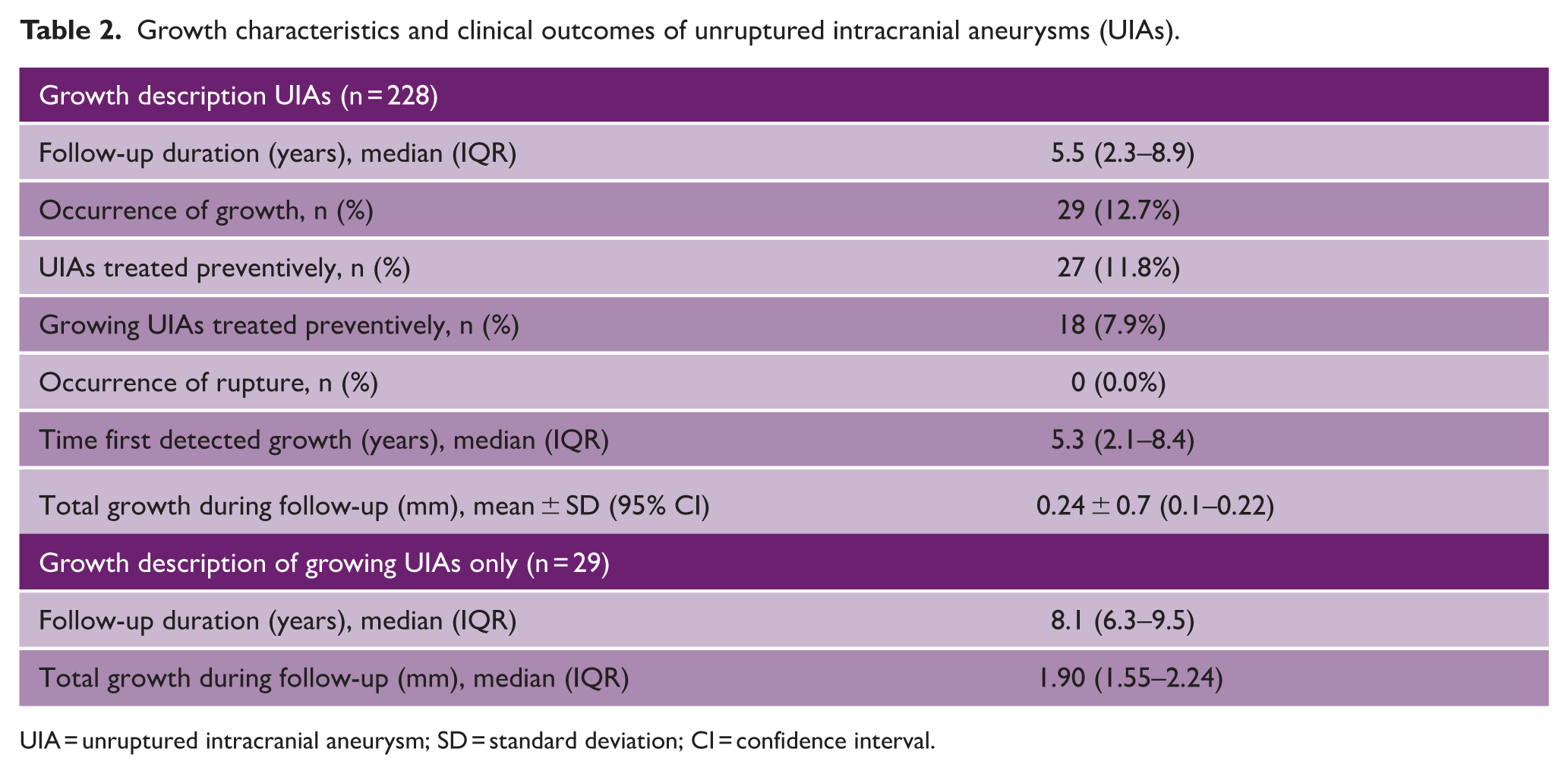
UIA = unruptured intracranial aneurysm; SD = standard deviation; CI = confidence interval.
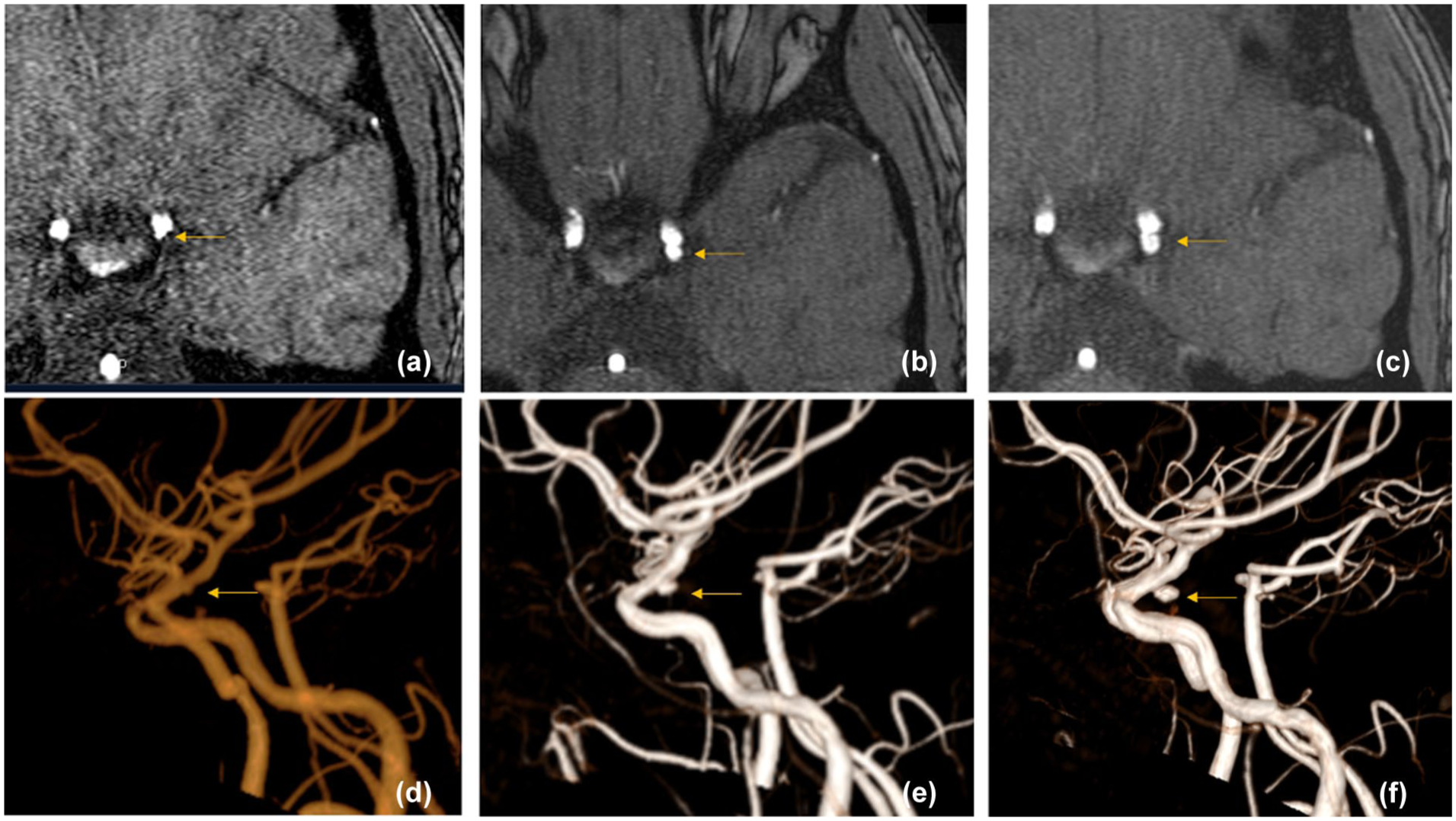
MRA-TOF images of a tiny left internal carotid artery aneurysm. Axial source images (a–c) and 3D reconstructions (d–f) show the aneurysm at baseline (a, d), after 6 years (b, e), and after 11 years (c, f), increasing in size from 1.0 × 1.4 mm to 2.0 × 2.8 mm, and 3.0 × 3.0 mm, respectively.
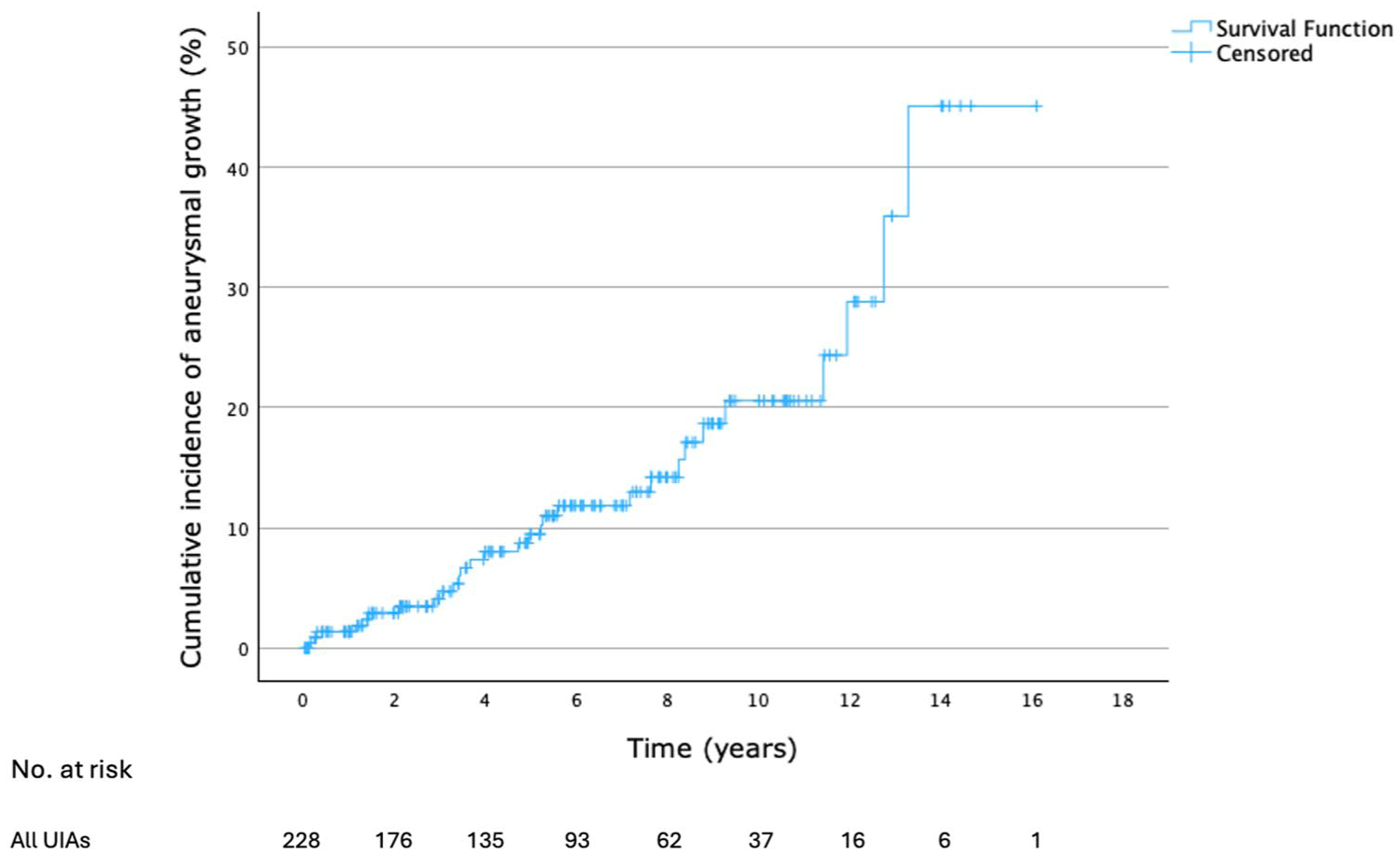
Cumulative incidence curve illustrating the estimated probability of aneurysmal growth over time.
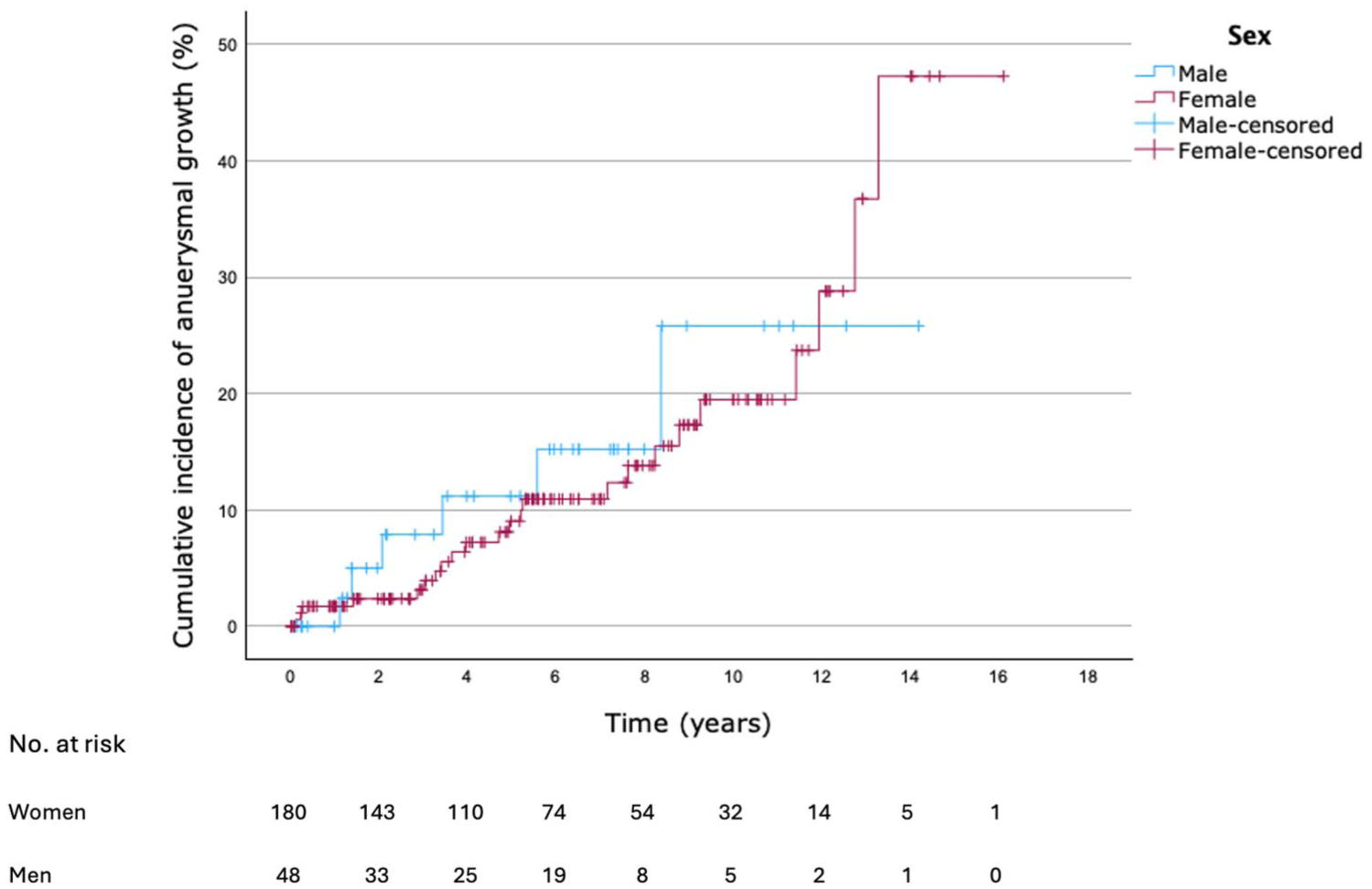
Cumulative incidence curves illustrating the estimated probability of aneurysmal growth over time stratified by sex.
Treatment
Of the 29 UIAs demonstrating growth, 18 were treated, while the remaining 11 were managed conservatively because of advanced patient age or relevant comorbidities. Across the entire cohort, preventive treatment was performed for 27 UIAs in 24 patients. The median interval between diagnosis and treatment was 4.04 years (IQR = 3.10–6.24). Growth was the indication for treatment in 18 cases, three UIAs in two patients were treated based on patient preference (e.g. positive family history), and six UIAs in four patients were treated concurrently with other larger UIAs.
Discussion
In this retrospective cohort study, aneurysm growth was observed in approximately one out of eight tiny UIAs over a median follow-up of more than 5 years, corresponding to a cumulative growth risk of 9.7% (95% CI = 5.1–14.2%) at 5 years. These findings indicate that tiny UIAs, despite their small size, exhibit a clinically relevant probability of growth over time. Growth rates were comparable between men and women, suggesting that sex-specific surveillance strategies may not be warranted for this aneurysm subgroup.
Currently, studies specifically focusing on the follow-up of tiny UIAs remain limited. Most studies on aneurysm growth focus on small UIAs up to 5 or 7 mm, with only a few reporting subgroup analyses for UIAs measuring ⩽3 mm. A systematic review included such a subgroup analysis, 17 comprising five studies that reported growth rates specifically for tiny UIAs. The estimated annual growth rates varied widely, ranging from 0.53% to 11.64%, with four of the five studies reporting growth rates below 3%. This wide range reflects substantial heterogeneity between studies and underscores the uncertainty surrounding growth estimates for tiny UIAs. Moreover, as acknowledged by the authors, the overall quality of evidence was low, owing to retrospective study designs, inconsistent definitions of growth, and limited follow-up durations. In our cohort, the annual growth rate was 2.3% per aneurysm-year (95% CI = 1.5–3.1%), which falls within the lower range of previously reported rates, providing more precise long-term data specifically for tiny UIAs.
A Markov decision model questioned the necessity of long-term surveillance for tiny UIAs. 12 This model was based on an earlier observational study of 448 UIAs smaller than 5 mm, 13 which were followed for a mean of 41.0 months. The study reported growth in 6.7% of cases, corresponding to an annual growth rate of 1.22%. However, it did not specifically include UIAs ⩽3 mm, and differences in growth definitions as well as the shorter follow-up duration may explain the lower growth rate compared with our findings.
This study provides valuable longitudinal data from one of the largest cohorts to date focusing exclusively on tiny UIAs. The relatively long median follow-up duration strengthens the reliability of our observations regarding long-term growth. Our findings indicate that growth may occur more frequently than previously assumed, suggesting that discontinuation of monitoring could result in missed growth associated with an increased risk of rupture. 5 Nevertheless, several limitations should be acknowledged. First, the retrospective design introduces potential information bias, as growth assessment relied on radiology reports and multidisciplinary documentation, which are subject to interobserver variability. Second, a relatively high proportion of patients in our cohort had a positive family history of aSAH were current or former smokers or had multiple aneurysms. This likely reflects clinical selection for follow-up, consistent with routine clinical practice in which patients with a higher perceived risk are more likely to be diagnosed with UIAs through screening and are also more likely to have multiple UIAs. 18 In addition, patients with multiple UIAs are more likely to be frequently monitored over time, which may increase the likelihood of detecting aneurysm growth. Smoking is another important risk factor associated with multiple UIAs, 19 which may contribute to the relatively high proportion of smokers in the cohort. This may have introduced selection bias into our findings. Furthermore, measurement of tiny UIAs is inherently prone to variability due to relatively greater measurement error and should be taken into account when interpreting growth rates in clinical practice. In addition, follow-up intervals were not standardized, potentially affecting the timing and detection of aneurysmal growth. Finally, the relatively small number of UIAs in men limits the statistical power to detect sex-specific differences, which should be considered when interpreting the lack of observed differences between sexes. In the absence of prospective data defining optimal surveillance intervals, our findings support a cautious, individualized, risk-adapted approach that balances the benefits of early detection against the costs and potential anxiety associated with repeated imaging. 20 Future large-scale, prospective, multicenter cohort studies with standardized imaging protocols and predefined follow-up intervals are needed to refine surveillance strategies and determine whether follow-up intervals for tiny UIAs can be safely extended compared with those used for larger aneurysms. Such studies should also incorporate health economic analyses to evaluate cost-effectiveness and further optimize follow-up strategies.
Conclusion
In conclusion, this study demonstrates that a meaningful subset of tiny UIAs exhibits measurable growth over time. These findings challenge recommendations to discontinue active monitoring of tiny UIAs and instead support a continued, individualized follow-up approach already implemented in clinical practice. Further prospective research is needed to optimize surveillance intervals and improve patient management.
Footnotes
Ethical approval
The institutional review board of the University Medical Centre Utrecht (UMCU) waived the need for ethics approval.
Informed consent statements
The institutional review board of the University Medical Centre Utrecht (UMCU) waived the need for patient consent for the collection, analysis, and publication of the retrospectively obtained and anonymized data for this non-interventional study.
Consent to participate
Not applicable.
Author contributions
I.C.v.d.S. and Y.M.R. were responsible for the study design. J.D.v.d.P., M.J.K., L.T.v.d.K., and M.D.I.V. were responsible for the data acquisition. J.D.v.d.P. and Y.M.R. were responsible for the data analysis and interpretation. J.D.v.d.P. was responsible for drafting the manuscript. I.C.v.d.S., M.D.I.V., M.J.K., L.T.v.d.K., and Y.M.R. were responsible for the critical revision of the manuscript. YMR was responsible for the supervision.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We acknowledge the support by the Dutch Heart Foundation (Dekker Established Clinical Investigator Grant 03-001-2022-0157).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data underlying this study are not publicly available due to institutional and ethical restrictions. The dataset is hosted at the UMCU and contains sensitive patient information that cannot be shared openly. Access to the data may be granted upon reasonable request and subject to approval by the appropriate institutional review board and data access committee. Requests can be directed to the corresponding author.