
Abstract
Background:
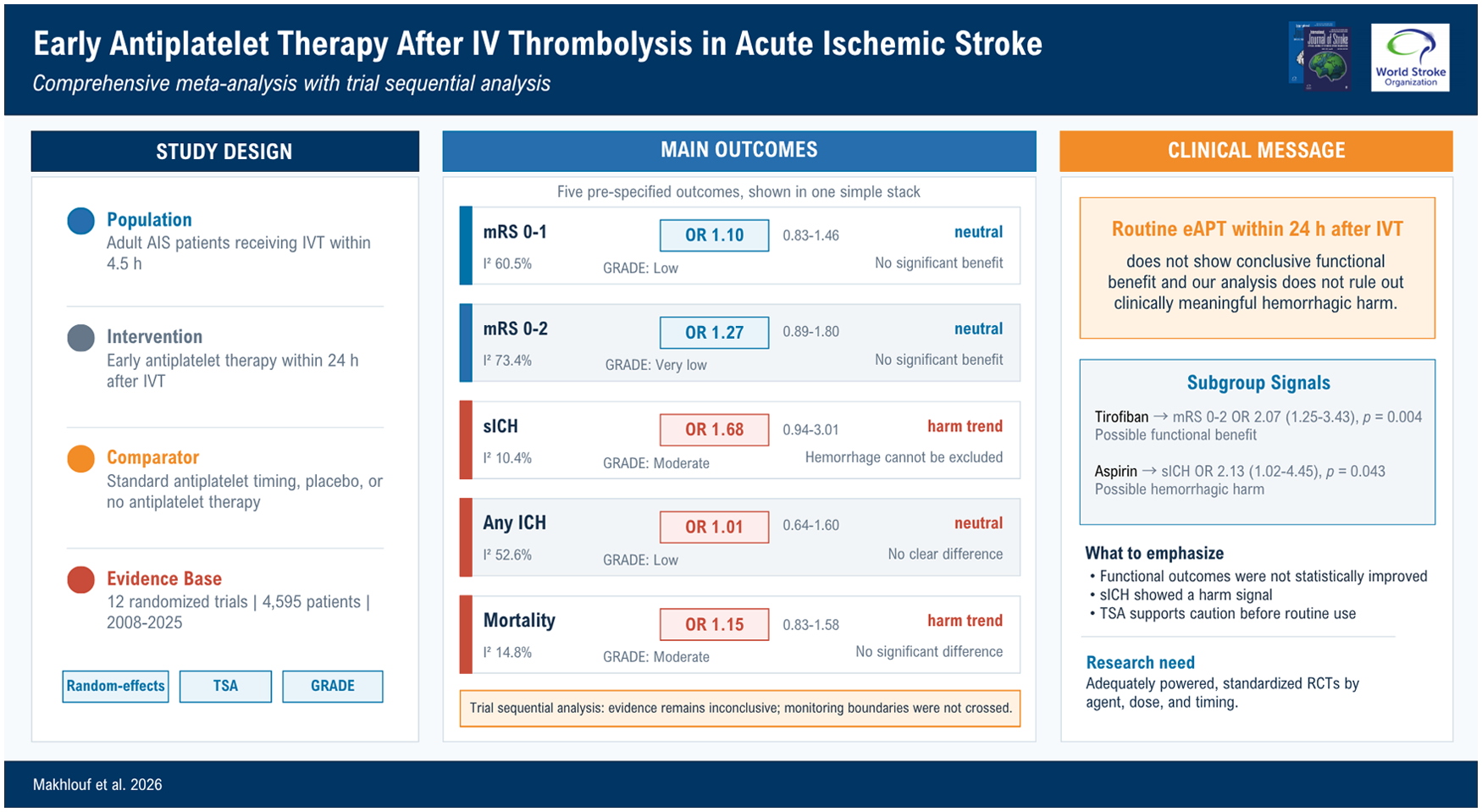
Early antiplatelet therapy after intravenous thrombolysis (IVT) in acute ischemic stroke (AIS) patients may prevent re-occlusion and early neurological deterioration, but it could increase hemorrhagic transformation. Evidence remains conflicting, particularly with emerging contemporary trials.
Methods:
We conducted a Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA)-guided systematic review of randomized controlled trials (RCTs) comparing early antiplatelet therapy (eAPT) initiated within 24 h after IVT (with or without thrombectomy) versus standard timing (>24 h), placebo, or no antiplatelet therapy (CRD420251276445). Random-effects models were used to estimate odds ratios (ORs) and mean differences (MDs) with 95% confidence intervals (CIs). Trial sequential analysis, subgroup analyses, meta-regression, and Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) certainty ratings were performed.
Results:
Twelve RCTs with 4595 patients were included. Early antiplatelet therapy led to higher non-significant odds of symptomatic intracranial hemorrhage (sICH; OR = 1.68, 95% CI = 0.94–3.01; I2 = 10.4%; GRADE moderate), and mortality (OR = 1.15, 95% CI = 0.83–1.58; I2 = 14.8%; GRADE moderate) but not intracranial hemorrhage (OR = 1.01, 95% CI = 0.64–1.60; I2 = 52.6%; GRADE low). Functional outcomes were not improved: Modified Rankin Scale (mRS) 0–1 (OR = 1.10, 95% CI = 0.83–1.46; I2 = 60.5%; GRADE low) and mRS 0–2 (OR = 1.27, 95% CI = 0.89–1.80; I2 = 73.4%; GRADE very low). Trial sequential analysis indicated evidence remains inconclusive. Agent-specific subgroup analyses suggested higher sICH with early aspirin (OR = 2.13, 95% CI = 1.02–4.45) and possible benefit for mRS 0–2 with tirofiban (OR = 2.07, 95% CI = 1.25–3.43).
Conclusion:
Routine early antiplatelet therapy within 24 h after IVT does not provide conclusive functional benefit, and our analysis cannot exclude clinically meaningful hemorrhagic harm. Further adequately powered RCTs are needed to define whether any selected regimen—especially tirofiban—has a favorable risk–benefit profile.
Keywords
Introduction
Acute ischemic stroke (AIS) is one of the most common leading causes of death and disability worldwide. 1 Therefore, effective management is essential to reduce complications and long-term disability. The main pathophysiology of AIS is sudden blockage of cerebral blood flow due to arterial occlusion, most commonly from thromboembolism from atherosclerotic plaques in large arteries or cardiac sources such as atrial fibrillation, resulting in ischemia and brain tissue infarction.2,3
Current guidelines recommend intravenous thrombolysis (IVT) with recombinant tissue plasminogen activator (rtPA) or tenecteplase to treat AIS within 4.5 h of symptom onset, to improve clinical and functional outcomes without increasing overall mortality or systemic bleeding.4–6 A limitation of IVT is that it can initially yield recanalization but then re-occlusion may occur due to ongoing platelet activation, endothelial injury, and the inflammatory cascade that follows fibrinolysis and reperfusion, leading to poor clinical outcomes. 7
Antiplatelet therapy (APT) was suggested as an adjunct to maintain recanalization integrity by inhibiting platelet activation triggered by endothelial injury and post-reperfusion inflammation. 8 This helps maintain continuous blood flow and reduces the risk of recurrent arterial blockage, although it carries a potential risk of intracranial bleeding. 9 Current stroke management recommends starting APT like aspirin, clopidogrel, or a combination of aspirin/dipyridamole not earlier than 24 h after IVT, following confirmation of the absence of intracranial hemorrhage (ICH) on imaging due to the expected potential risk of systemic bleeding and other complications. 10 Recent studies investigated the feasibility and safety of initiating APT within the first 24 h after thrombolysis in patients with AIS and found signals of efficacy.11–13 So, the optimal timing of antiplatelet initiation after IVT remains uncertain, and current evidence is inconsistent.
A previous meta-analysis by Kelani et al, 14 including both randomized and observational studies, reported improved excellent functional outcomes (Modified Rankin Scale (mRS), 0–1) with early APT, with a non-significant increase in sICH and no effect on mortality. However, a more recent trial by Chen et al. 12 found no difference in functional outcomes between early APT and placebo. Furthermore, recent trials of tirofiban have shown mixed results, with potential functional benefit alongside increased bleeding risk. 11 Given these conflicting results, there is a need for an updated meta-analysis to clarify the benefits and risks of early APT.
This meta-analysis aims to determine whether initiating APT within 24 h of IVT (with or without mechanical thrombectomy) is safe and more effective than standard-timing initiation. By including only RCTs, integrating evidence from the most recent studies, and analyzing additional outcomes and subgroups, we aim to provide clear, evidence-based guidance for clinicians on the balance of benefits and harms.
Methods
Protocol registration
This review followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines and the Cochrane Handbook for Systematic Reviews (Supplemental Table S1).15,16 Our protocol was prospectively registered on the International Prospective Register of Systematic Reviews (PROSPERO) by CRD420251276445.
Literature search
We did a thorough literature search in the subsequent databases (PubMed, Scopus, Embase, and Web of Science) up to September 2025 using terms “stroke,” “intravenous thrombolysis,” “alteplase,” “antiplatelet,” “tirofiban,” and “early initiation” to identify studies of interest. (View Supplemental Table S2 for the detailed search strategy). A full citation analysis was also performed using the included studies and previous meta-analyses for additional citations. Duplicate records were identified and removed using EndNote software.
Selection and exclusion criteria
We selected the included studies based on this Population, Intervention, Comparator, Outcome, Study design (PICOS) criteria: Population: Adult AIS patients who received IVT within the time window specified in individual trials (mostly up to 4.5 h after symptom onset), either IVT alone or for bridging to endovascular thrombectomy (EVT), Intervention: antiplatelet therapy administrated within 24 h within intravenous thrombolysis, Comparator: patients receiving the standard protocol of antiplatelet treatment (after 24 h of IVT), no antiplatelet therapy or placebo, only randomized controlled trials (RCTs) with published English full text were included in our study. Studies were excluded if they addressed the effect of EVT without rtPA, studied late initiation of IVT (after 24 h) against placebo, were non-English, or were animal or in vitro studies.
Data extraction
Two reviewers independently extracted study and participant data (study ID, design, sample size, IVT and antiplatelet agents/doses, follow-up, age/sex, prior stroke, pre-stroke antiplatelet use, baseline mRS, and the Trial of Org 10172 in Acute Stroke Treatment (TOAST) Classification for subtyping ischemic stroke. 17 Disagreements were resolved by a third reviewer.
Risk-of-bias assessment
The risk-of-bias assessment process of the included studies was carried out according to the Cochrane Risk of Bias (RoB2) tool for RCTs and was later independently judged and appraised by two reviewers. 18 ROB2 enables the authors to categorize RCTs as low risk of bias, high risk of bias, or some concern. Any disagreements between reviewers were discussed and resolved with the assistance of a third reviewer to ensure accuracy and minimize bias in the evaluation process.
Outcomes of interest
The safety outcomes were the incidence of symptomatic or asymptomatic ICH and mortality, while the measured efficacy outcomes were the change in the National Institutes of Health Stroke Scale (NIHSS) in 90 days and the number and percentage of patients with a Modified Rankin Scale (mRS) score of 0–1 (freedom-from-disability; excellent functional outcomes), 0–2 (functional independence; good functional outcomes), and 3–6 at 90 days.19,20
Data synthesis and statistical analysis
Statistical analyses were performed in R (RStudio, v4.5) using metafor for meta-analyses and ggplot2 for figures. Dichotomous outcomes were pooled as odds ratios (ORs) and continuous outcomes as mean differences (MDs) and 95% confidence interval (CI) using a random-effects model. Heterogeneity was assessed with Higgins’ I2 (0–25% minor; 25–50% moderate; >50% considerable); when present, we ran leave-one-out sensitivity checks. 21 Also, prespecified subgroup analyses examined control type (placebo/open-label standard therapy/active control), baseline severity (NIHSS ⩾5 vs. <5), antiplatelet agent (e.g. aspirin, glenzoclimb, and tirofiban), and timing (<2 h vs. 2–24 h). Meta-regressions tested effects of mean age and prior-stroke prevalence, and we reported τ2 and I2 before/after covariates. We used trial sequential analysis (TSA; α = 0.05, 80% power, 20% relative risk reduction) to assess the conclusiveness of the evidence. We conducted a separate analysis comparing low-dose rtPA + early APT versus standard-dose rtPA.
Publication bias
Publication bias was assessed using the Doi plot and quantified with the Lafuente, Ferreira, and Kairalla (LFK) index. 22 Values closer to 0 indicate minimal bias, while negative values beyond −1 and positive values beyond 1 suggest a likelihood of bias.
Certainty of the evidence
We assessed the certainty of evidence for each outcome using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) framework.23,24 GRADE assesses risk of bias, inconsistency, indirectness, imprecision, and publication bias, and rates evidence as high, moderate, low, or very low. Reasons for downgrading were reported with the pooled estimates.
Results
Literature search results
We obtained 3060 reports from the initial systematic search. After removing 943 duplicates, 2117 titles and abstracts were screened, of which 2032 were excluded. Eighty-five full texts were assessed, and 12 RCTs met the inclusion criteria and were included in the quantitative meta-analysis (Figure 1).
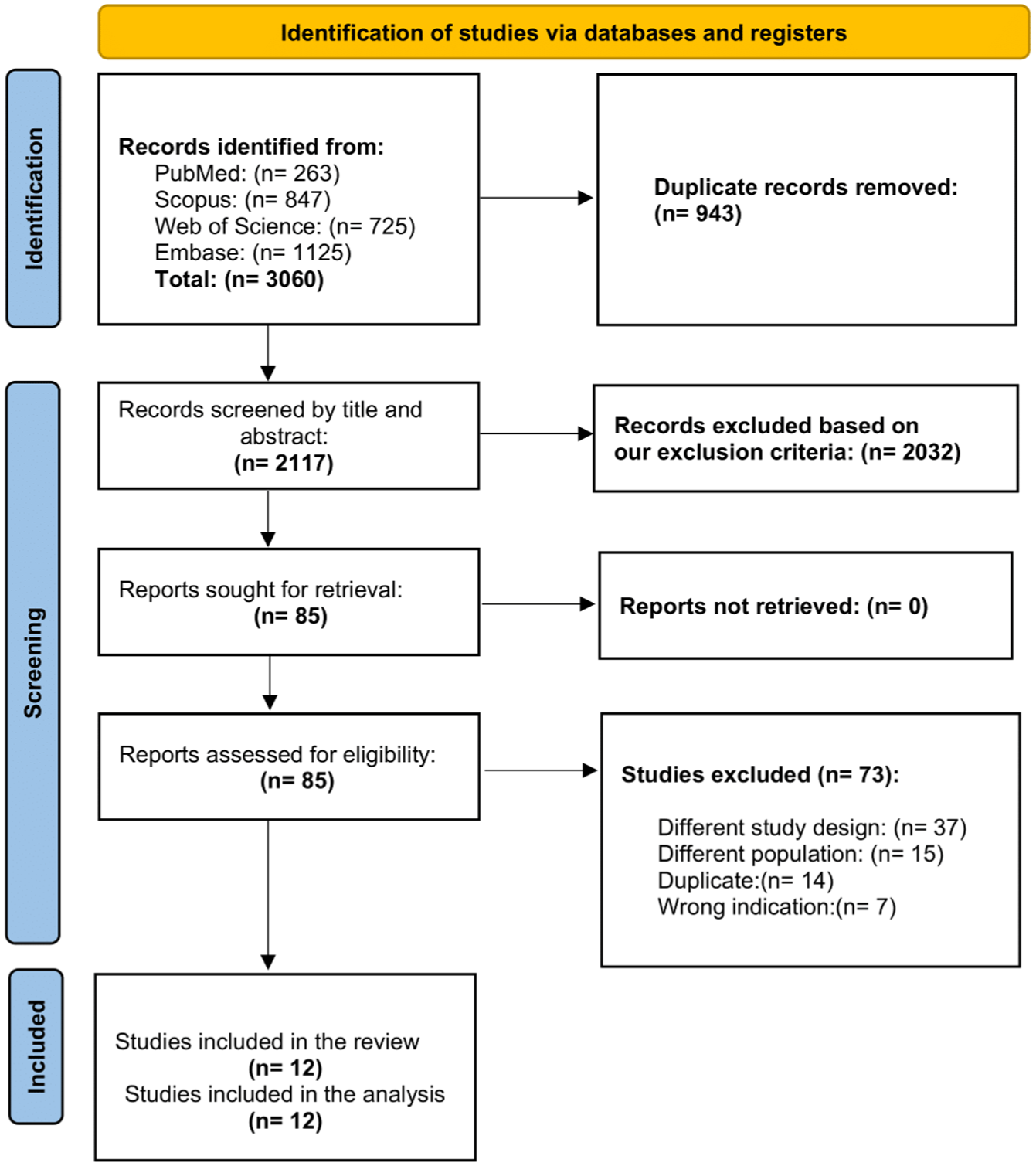
PRISMA flow diagram of the included studies.
Characteristics of the included studies
Twelve RCTs published between 2008 and 2025, involving 4595 adult patients with AIS, were included in our review.11,12,25–34 Five trials were conducted in China, three in the United States, and one each in South Korea, the Netherlands, and a multinational European consortium. All studies had a 90-day follow-up duration. Early antiplatelet therapy varied: eight trials used glycoprotein IIb/IIIa inhibitors (tirofiban or eptifibatide), two used aspirin, one used dual therapy (aspirin plus clopidogrel), and one used glenzocimab. Mean age ranged from the mid-60s to mid-70s, and male participants comprised ~50–73% of patients. Detailed characteristics are presented in Supplemental Tables S3 and S4.
Risk-of-bias assessment
A summary and graph of the risk of bias for the RCTs according to ROB2 are shown in Figure 2. Five RCTs yielded an overall low risk of bias. Six studies raised concerns, primarily regarding deviations from intended interventions (D2). The remaining study demonstrated a high overall risk of bias due to problems with randomization and the lack of allocation concealment.
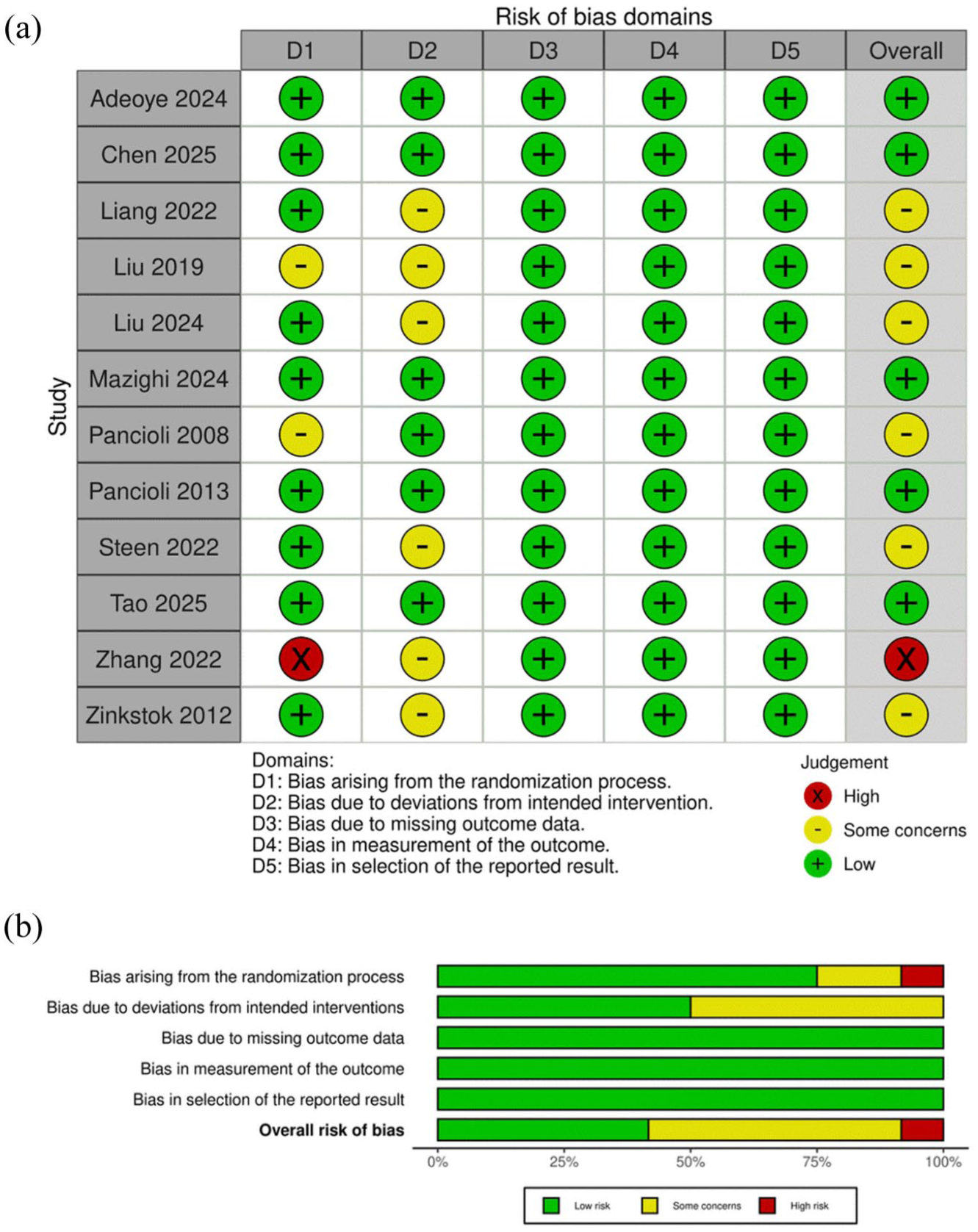
(a) Quality assessments according to risk of bias for each study. (b) Quality assessment according to risk of bias as a percentage.
Meta-analysis results for primary efficacy outcomes
mRS (0–1) at 90 days
The pooled analysis of excellent outcome (mRS 0–1) at 90 days incorporated seven studies with 3324 patients. The overall effect indicated no statistically significant difference between the eAPT and control groups (OR = 1.10, 95% CI = 0.83–1.46, p = 0.509); the heterogeneity was substantial (I2 = 60.5%, p = 0.019 (Figure 3(a)) with minor asymmetry (LFK index = 1.86), and the TSA confirmed that the available evidence remains inconclusive (Supplemental Figure S1, Figure 3(b)). Leave-one-out analyses showed the pooled estimate became significant after removing Adeoye 2024, Chen 2025, Mazighi 2024, or Zinkstok 2012, so the result is not robust (Supplemental Figure S2). Meta-regression did not identify significant associations with age or prior-stroke prevalence (Supplemental Table S6, Supplemental Figure S3) Subgroup analyses did not demonstrate any statistically significant differences (Figure 3(c)).
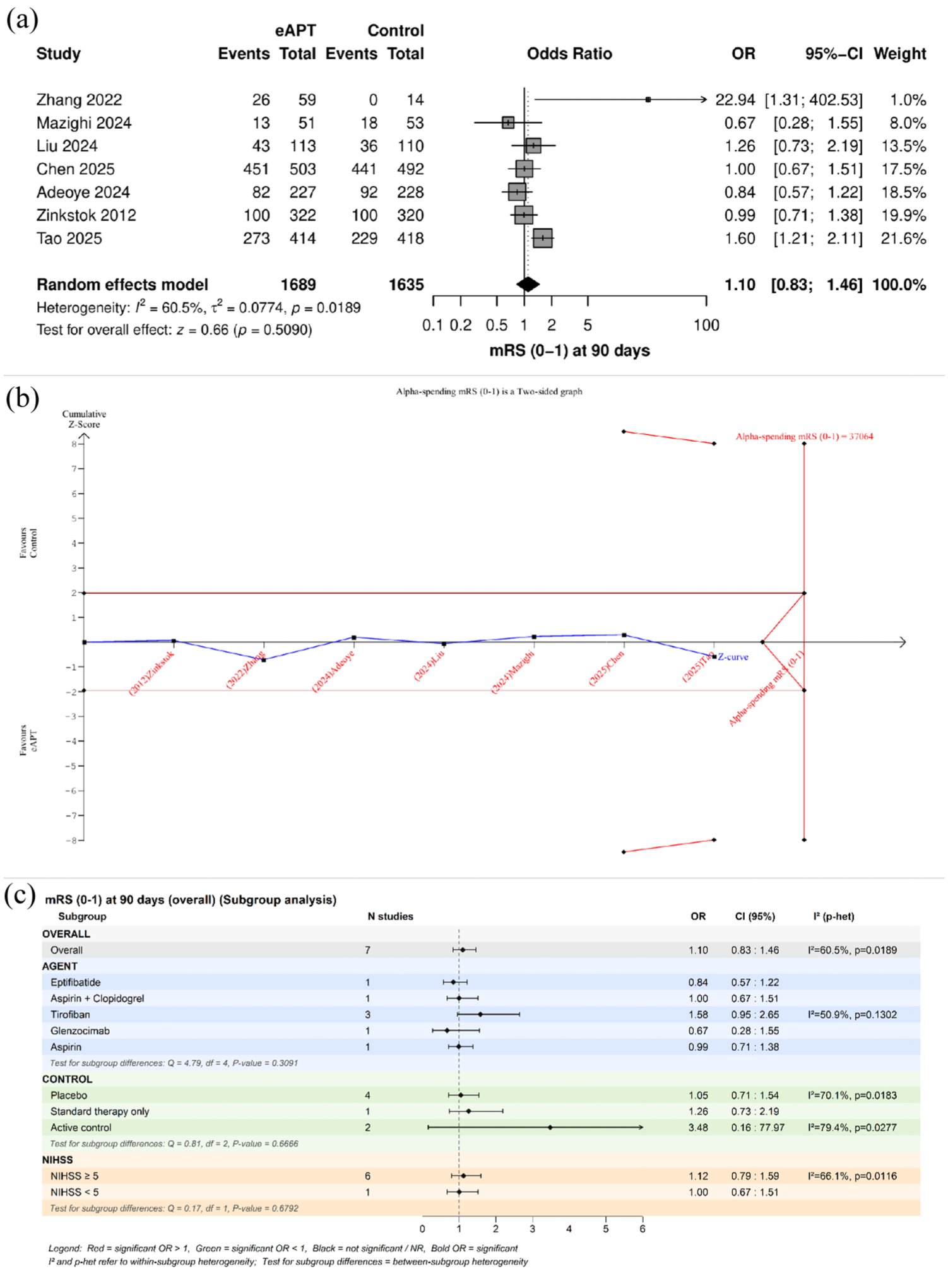
(a) Forest plot of the meta-analysis for mRS (0–1) at 90 days. (b) Trial sequential analysis monitoring plot. (c) Subgroup analyses.
mRS (0–2) at 90 days
The pooled analysis for functional independence (mRS 0–2) across eight studies (3564 patients) showed no significant difference between eATP and control groups (OR = 1.27, 95% CI = 0.89–1.8, p = 0.19), with significant heterogeneity (I2 = 73.4%, p = 0.0004; Figure 4(a)). Publication bias assessment indicated major asymmetry (LFK index = 3.05), and TSA indicated that the evidence remains inconclusive (Supplemental Figure S4, Figure 4(b)). Leave-one-out sensitivity analyses showed that this null result was unstable, as removing Adeoye 2024, Chen 2025, Mazighi 2024, or Zinkstok 2012 shifted the pooled effect to a statistically significant benefit of eAPT. (Supplemental Figure S5). Meta-regression found no significant correlation with patient age or the prevalence of previous stroke (Supplemental Table S6 and Supplemental Figure S6). Subgroup analyses demonstrated a significant difference between antiplatelet agents (p = 0.034), with the tirofiban subgroup showing a significant benefit of eAPT (OR = 2.07, 95% CI = 1.25–3.43, p = 0.004), and by control type, with benefit observed in standard therapy only comparator (Figure 4(c)).
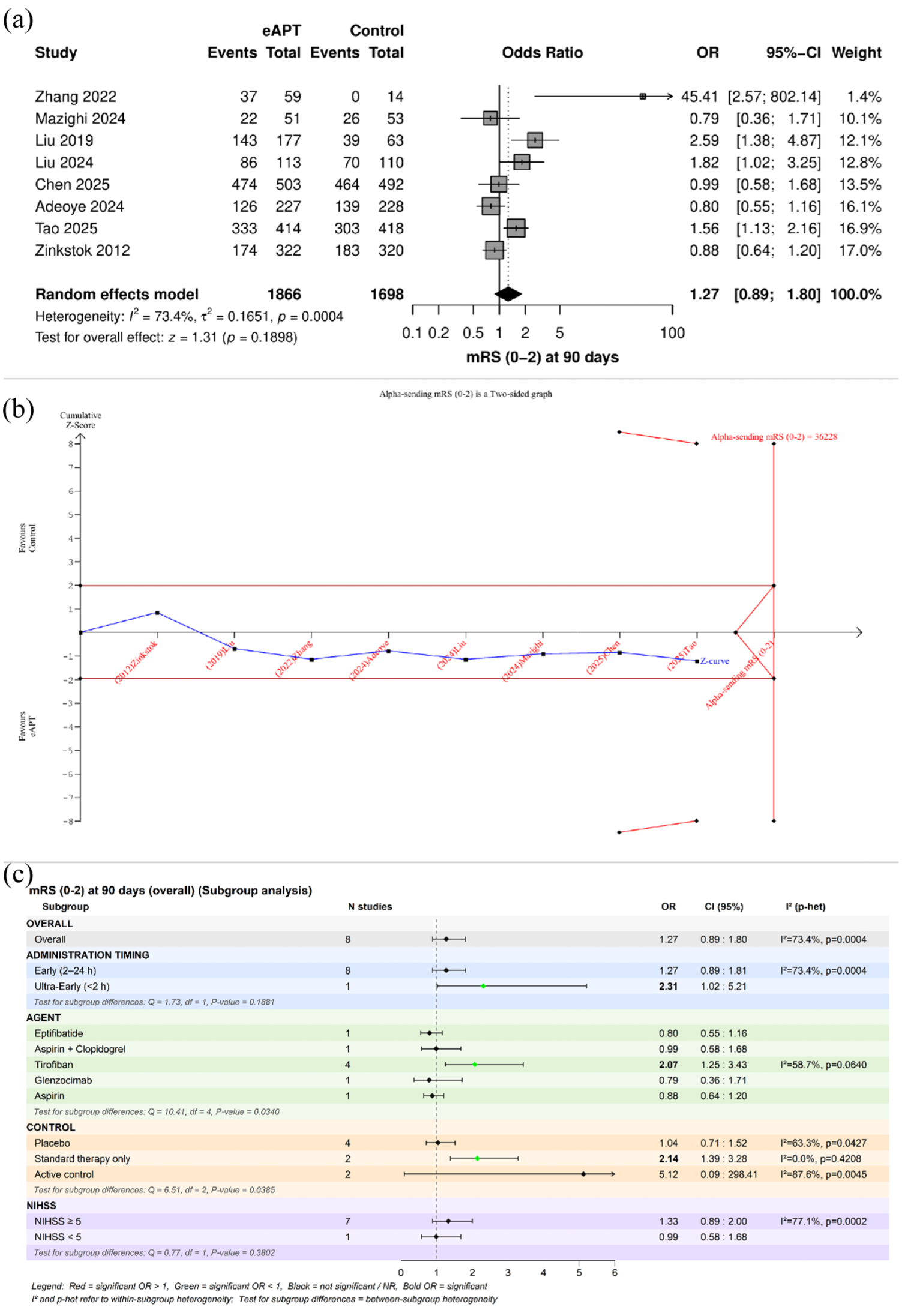
(a) Forest plot of the meta-analysis for mRS (0–2) at 90 days. (b) Trial sequential analysis monitoring plot. (c) Subgroup analyses.
Meta-analysis results for primary safety outcomes
Symptomatic intracranial hemorrhage (sICH)
Across nine trials (n = 3773), eAPT was not associated with a statistically significant increase in sICH compared with control (OR = 1.68, 95% CI = 0.94–3.01; p = 0.081), and between-study heterogeneity was low (I2 = 10.4%, p = 0.35; Figure 5(a)). Visual inspection of the Doi plot and an LFK index of −1.59 suggested only minor asymmetry, while TSA found the accrued evidence inconclusive (required information size = 5852; Figure 5(b), Supplemental S7). Meta-regression found no significant correlation with patient age or the prevalence of previous stroke (Supplemental Table S6 and Supplemental Figure S8). No significant subgroup differences were detected by administration timing, baseline NIHSS, or control group type (Figure 5(c)). However, a significant increase in sICH was observed specifically in the aspirin subgroup (OR = 2.13, 95% CI = 1.02–4.45, p = 0.043); the test for subgroup differences across all agents was not significant (p = 0.31; Figure 5(c)).
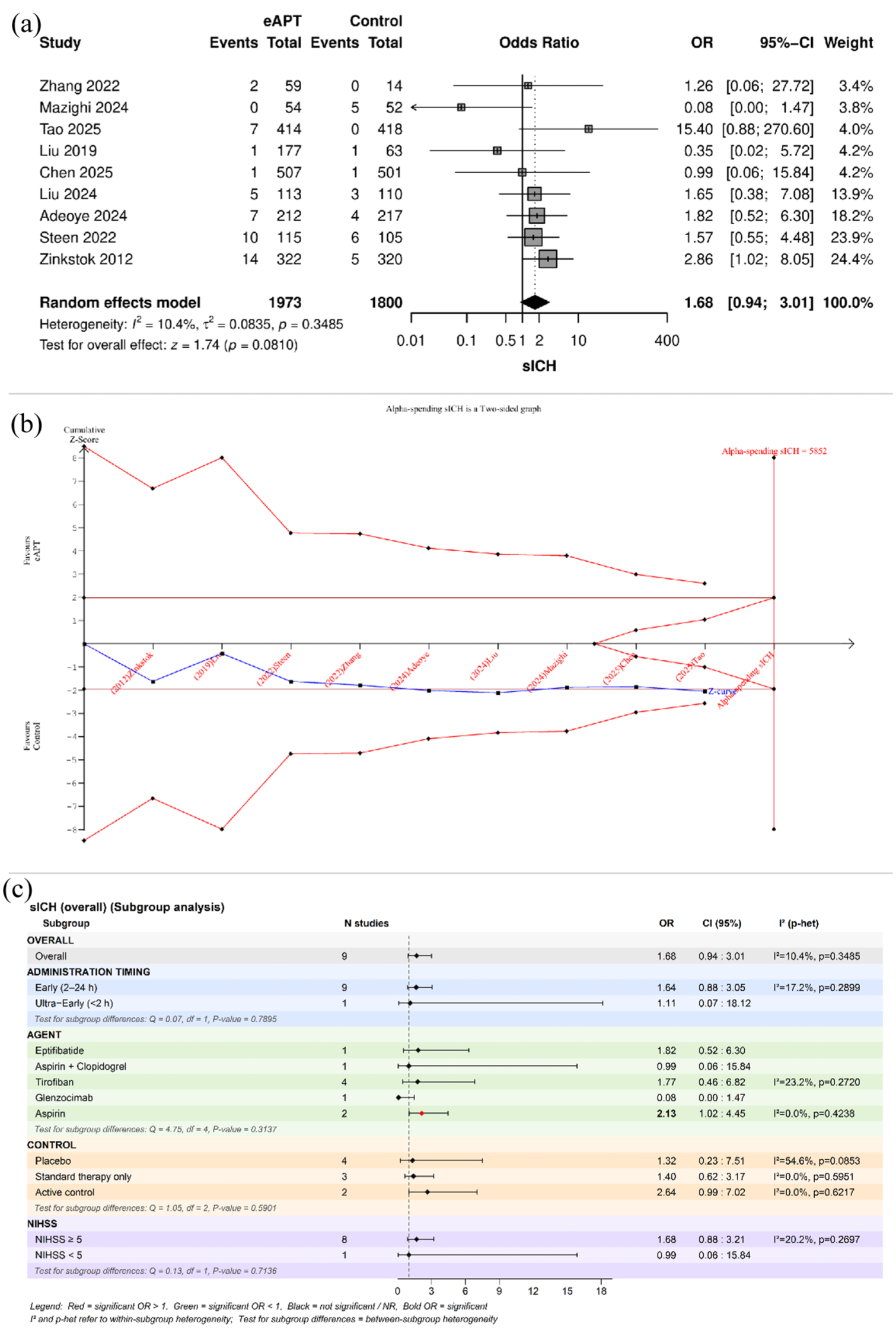
(a) Forest plot of the meta-analysis for symptomatic intracranial hemorrhage. (b) Trial sequential analysis monitoring plot. (c) Subgroup analyses.
Any intracranial hemorrhage (ICH)
The pooled analysis of seven trials (n = 3480) showed no significant difference in the risk of any ICH (OR = 1.01, 95% CI = 0.64–1.6, p = 0.97), with moderate heterogeneity (I2 = 52.6%, p = 0.049; Figure 6(a)). The null result remained stable on sensitivity analysis, and the TSA similarly suggested that the current evidence is still inconclusive (Supplemental Figure S9, Figure 6(b)). No publication bias asymmetry was detected (LFK index = 0.07; Supplemental Figure S10). Meta-regression revealed a significant inverse correlation between treatment effect and patient age (β = −0.1563, p = 0.015, R2 = 85.5%), with no association found for prior-stroke prevalence (Supplemental Table S6, Supplemental Figure S11). Subgroup analyses indicated a significant difference across antiplatelet agents (p = 0.029), but this should be interpreted cautiously because the apparently favorable estimate for glenzocimab (OR = 0.34, 95% CI = 0.15–0.75) was based on a single study (Figure 6(c)). No significant subgroup effects were found for administration timing, baseline stroke severity, or control type (Figure 6(c)).
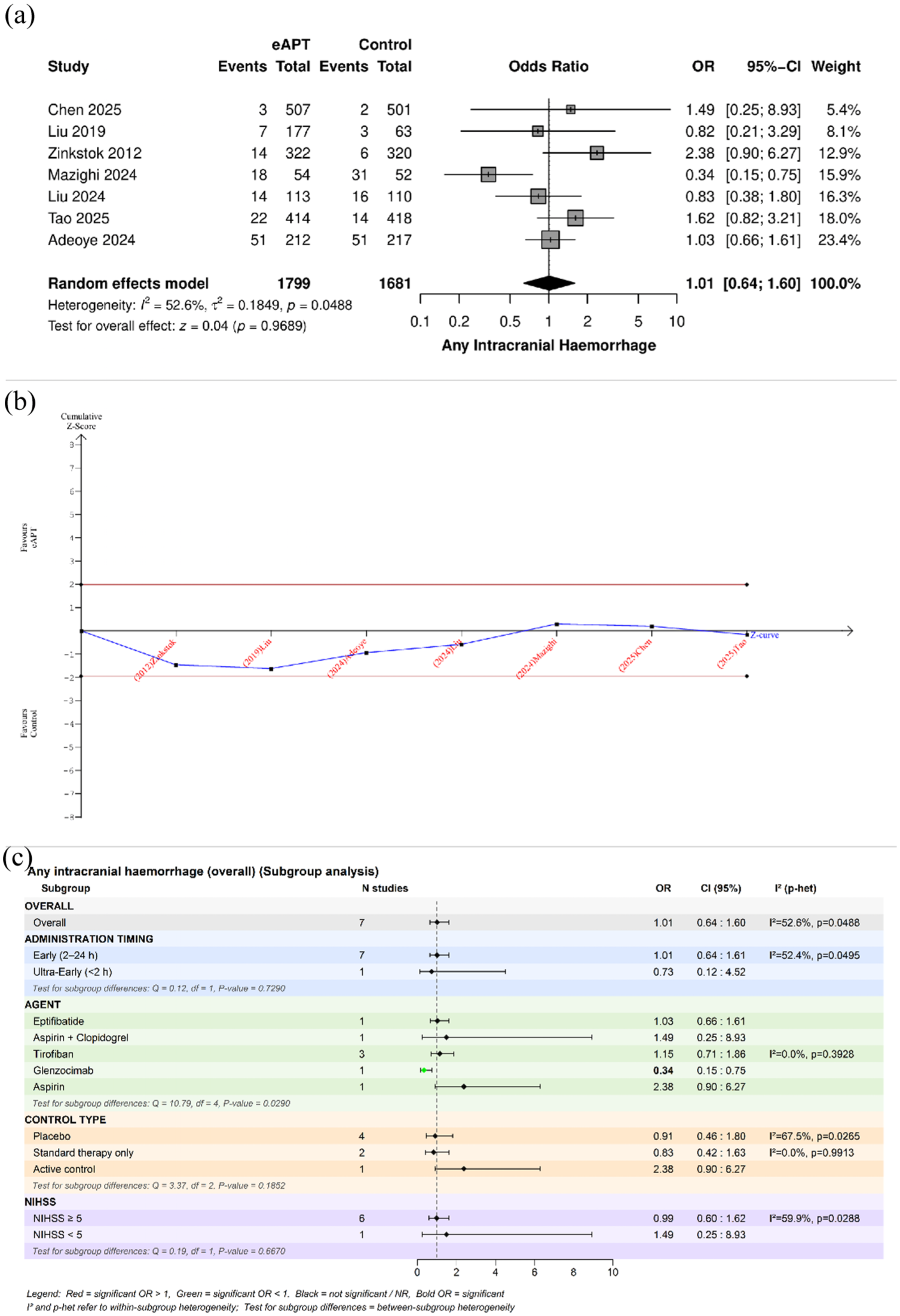
(a) Forest plot of the meta-analysis for any intracranial hemorrhage. (b) Trial sequential analysis monitoring plot. (c) Subgroup analyses.
Mortality
Across six studies involving 3224 patients, mortality risk did not differ between the eAPT and control groups (OR = 1.15, 95% CI = 0.83–1.58, p = 0.399), with minimal non-significant heterogeneity (I2 = 14.8%, p = 0.319; Figure 7(a)). Also, we summarized study-level mortality rates, showing variable event rates with several trials showing low or zero mortality (Supplemental Table S5). Publication bias assessment suggested minor asymmetry (LFK index = −1.05), and the TSA indicated that the evidence remains inconclusive (Supplemental Figure S12, Figure 7(b)). Meta-regression demonstrated no significant association with patient age or the prevalence of prior stroke (Supplemental Table S6, Supplemental Figure S13). Subgroup analyses showed no significant differences (Figure 7(c)).
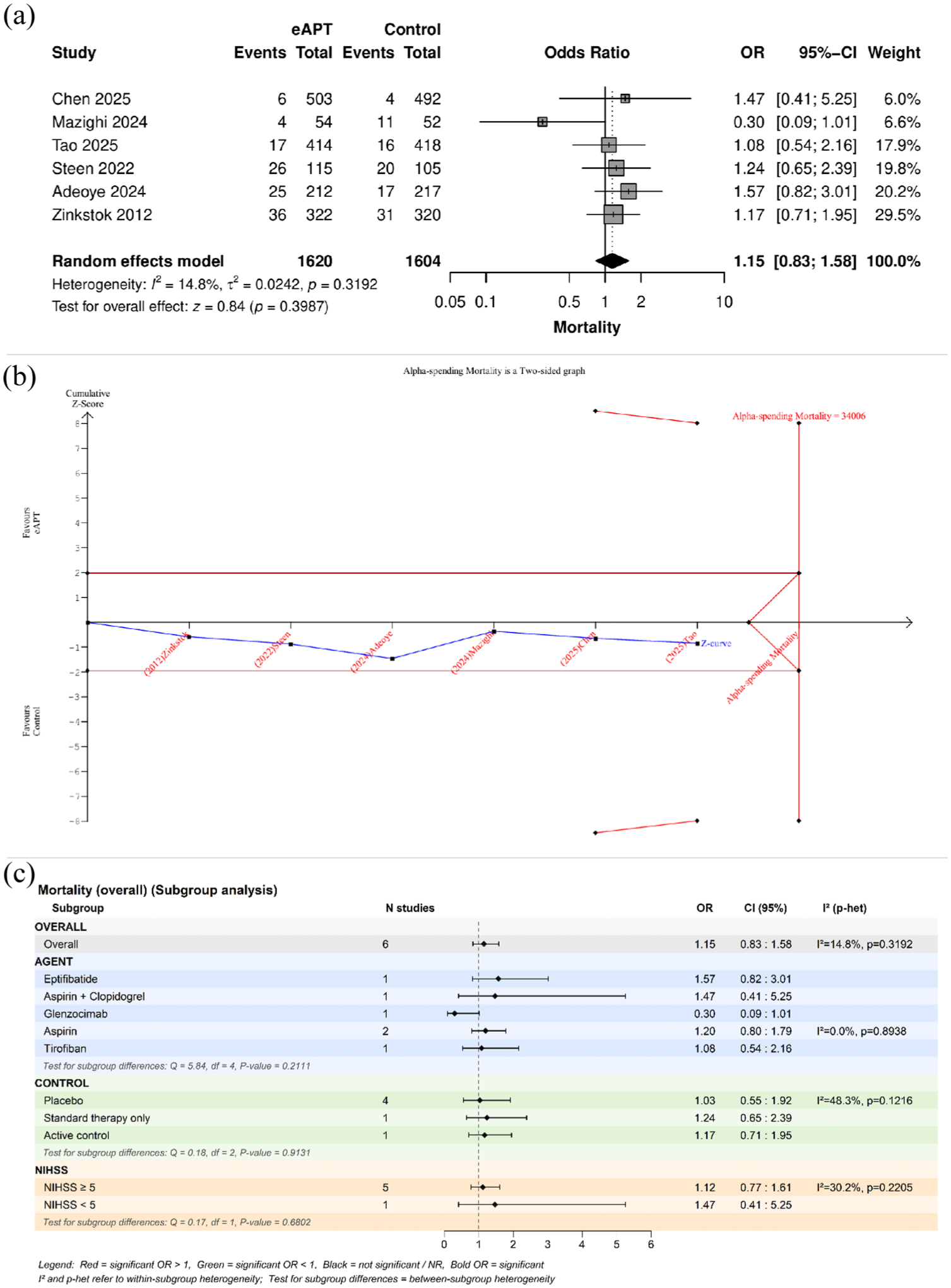
(a) Forest plot of the meta-analysis for mortality. (b) Trial sequential analysis monitoring plot. (c) Subgroup analyses.
Meta-analysis results for secondary outcomes
Regarding secondary efficacy outcomes, the pooled analysis for poor functional outcome (mRS 3–6) showed no significant difference between the two groups (OR = 0.69, 95% CI = 0.40–1.20, p = 0.188), with significant heterogeneity (I2 = 79.8%, p < 0.001; Supplemental Figure S14). Regarding the NIHSS, no significance between-group difference in neurological improvement was detected (MD = −0.5, 95% CI = −1.17 to 0.16, p = 0.135; I2 = 72.6%; Supplemental Figure S15). Subgroup analyses by assessment time showed no significant effect of eAPT (Supplemental Figure S16). Similarly for secondary safety outcomes, there was no significant difference between the eAPT and control group for parenchymal hemorrhage (OR = 1.70, 95% CI = 0.83–3.45, p = 0.146, Supplemental Figure S17), asymptomatic ICH (OR = 0.73, 95% CI = 0.48–1.12, p = 0.153, Supplemental Figure S18), or extracranial bleeding (OR = 0.86, 95% CI = 0.48–1.12, p = 0.639, Supplemental Figure S19), all without heterogeneity. Detailed results of secondary outcomes, including the number of studies and participants for each analysis, are summarized in Supplemental Table S7.
Early antiplatelet therapy plus low-dose intravenous thrombolysis versus standard-dose rtPA
We compared the outcomes between low-dose rtPA plus eAPT (LD-rtPA + eAPT) and standard-dose rtPA (SD-rtPA). The pooled analysis did not improve functional outcome at 90 days (mRS 0–1; OR = 1.24, 95% CI = 0.45–3.37; I2 = 67.7%; Supplemental Figure S20(a)). However, this finding was not robust in leave-one-out analysis, with exclusion of Pancioli 2008 showing a significant benefit (OR = 2.07, 95% CI = 1.02–4.22; I2 = 0%; Supplemental Figure S20(b)). LD-rtPA + eAPT significantly reduced sICH (OR = 0.16, 95% CI = 0.04–0.68; I2 = 0%; Supplemental Figure S20(c)); no significant differences were observed for any ICH or mortality (Supplemental Figure S20(d) to (e)). These comparisons were based on a limited number of studies (two to three trials) with relatively small sample sizes (~220–280 patients), which may limit the precision and generalizability of these findings (Supplemental Table S7).
GRADE certainty of evidence
Overall, the GRADE assessment indicates greater confidence in safety estimates than in efficacy estimates, with functional outcome data remaining highly uncertain (Table 1).
Summary of analyses and certainty of outcomes (GRADE).
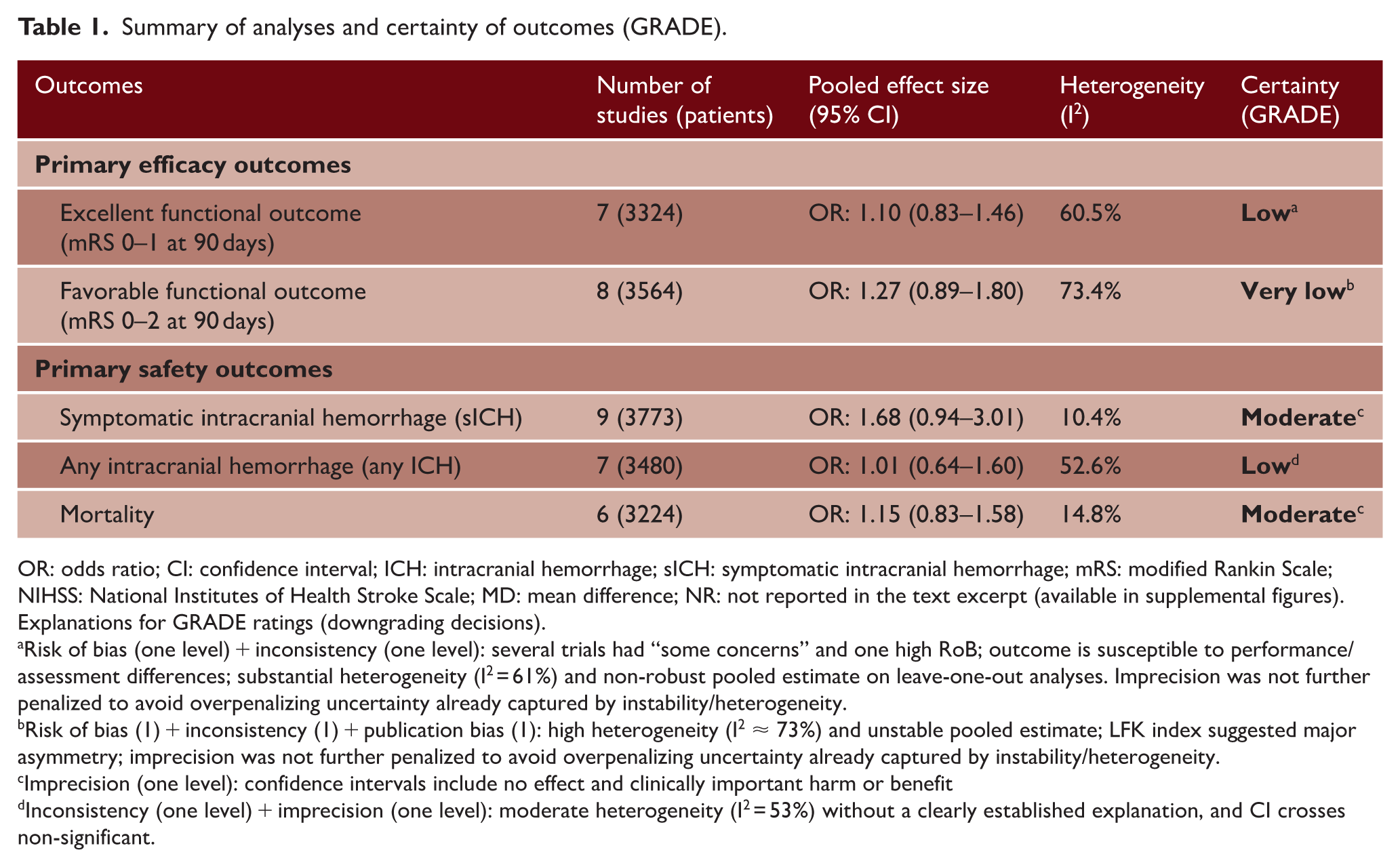
OR: odds ratio; CI: confidence interval; ICH: intracranial hemorrhage; sICH: symptomatic intracranial hemorrhage; mRS: modified Rankin Scale; NIHSS: National Institutes of Health Stroke Scale; MD: mean difference; NR: not reported in the text excerpt (available in supplemental figures).
Explanations for GRADE ratings (downgrading decisions).
Risk of bias (one level) + inconsistency (one level): several trials had “some concerns” and one high RoB; outcome is susceptible to performance/assessment differences; substantial heterogeneity (I2 = 61%) and non-robust pooled estimate on leave-one-out analyses. Imprecision was not further penalized to avoid overpenalizing uncertainty already captured by instability/heterogeneity.
Risk of bias (1) + inconsistency (1) + publication bias (1): high heterogeneity (I2 ≈ 73%) and unstable pooled estimate; LFK index suggested major asymmetry; imprecision was not further penalized to avoid overpenalizing uncertainty already captured by instability/heterogeneity.
Imprecision (one level): confidence intervals include no effect and clinically important harm or benefit
Inconsistency (one level) + imprecision (one level): moderate heterogeneity (I2 = 53%) without a clearly established explanation, and CI crosses non-significant.
Discussion
In this comprehensive RCT-only meta-analysis, initiating antiplatelet therapy within 24 h after IV thrombolysis did not yield a consistent net clinical benefit compared with standard initiation after 24 h, placebo, or no antiplatelet treatment. Across primary safety outcomes, early APT was associated with a non-significantly higher incidence of sICH and mortality and no differences in any ICH. For efficacy, early APT did not significantly improve the proportion of excellent disability outcomes (mRS 0–1) or functional independence (mRS 0–2) at 90 days in the overall analyses, with substantial heterogeneity and sensitivity to excluding several influential contemporary trials. Subgroup signals suggested harm with early aspirin for sICH, whereas a possible functional benefit emerged in the tirofiban subgroup for mRS 0–2 and in trials using open-label standard therapy controls; however, these findings should be interpreted cautiously given the small number of studies in some of the groups. In a separate comparison of low-dose thrombolysis plus early antiplatelet therapy versus standard-dose rtPA, a significant reduction in sICH was observed, whereas other outcomes were similar, again with limited information size.
The substantial heterogeneity observed for functional outcomes, particularly mRS 0–1 (I2 = 60.5%) and mRS 0–2 (I2 = 73.4%), is plausibly explained by both clinical and methodological diversity across trials. Clinically, studies included various interventions and control arms and mixed IVT-only and IVT plus thrombectomy populations. However, we conducted subgroup analyses and meta-regression, as well as sensitivity analyses, which partially resolved these heterogeneities. For mRS 0–1, the overall null effect became statistically significant after excluding Adeoye 2024, Chen 2025, Mazighi 2024, or Zinkstok 2012, indicating that between-trial differences in population, intervention class, and care pathway meaningfully affected the pooled estimate. A similar pattern was observed for mRS 0–2, in which omitting the same influential studies shifted the pooled effect toward significance, consistent with small-study effects and the significant asymmetry detected by the Doi plot (LFK 3.05). Adeoye 2024 was a large, multicenter, US adjunctive-antithrombotic trial in which the early strategy was intravenous eptifibatide or argatroban administered soon after IVT (including alteplase and tenecteplase), with a utility-weighted mRS primary endpoint and a contemporary care pathway, making it less comparable to trials evaluating routine early secondary-prevention aspirin or tirofiban. 26 Chen 2025 (EAST) enrolled minor stroke patients with very high baseline rates of excellent outcome, used early dual oral antiplatelet therapy (aspirin + clopidogrel), and, therefore, had a strong ceiling effect that limits detectable improvement in mRS 0–1. 12 Mazighi 2024 (ACTIMIS) was an early-phase European trial of glenzocimab (Glycoprotein VI (GPVI) inhibition) with dose cohorts and safety focus, enrolling an older, more heterogeneous population and assessing a mechanistically distinct antiplatelet pathway that is not directly comparable to aspirin or GPIIb/IIIa inhibition. 33 Zinkstok 2012 tested very early intravenous aspirin within 90 min of alteplase versus delayed aspirin. In contrast, safety outcomes were more stable: sICH showed low heterogeneity (I2 = 10.4%) with a consistent directional trend toward harm, and mortality also showed low heterogeneity (I2 = 14.8%). “Any ICH” displayed moderate heterogeneity (I = 52.6%), and meta-regression suggested that differences in mean age across trials accounted for a large proportion of this variability (R2 analog = 85.5%).
Importantly, the TSA for the key outcomes did not cross the trial sequential monitoring boundaries, confirming that the cumulative evidence remains inconclusive even after the inclusion of recent large trials. For sICH, the cumulative Z-curve remained consistently below zero, suggesting a persistent directional signal toward higher bleeding risk with early antiplatelet therapy; however, the accrued information size (3773 patients) remains below the required information size (RIS) = 5852 to detect a 20% OR change, indicating that studies to date have enrolled two-thirds of the patient numbers needed before TSA can provide a more definitive conclusion. This is especially important as the higher probability of sICH overcome the possibly-to-remain inconclusive evidence in efficacy outcomes as the RIS for the remaining outcomes is substantially larger (on the order of tens of thousands), implying that huge additional trial populations would be required to confirm or confidently exclude small-to-moderate effects in other outcomes and that the findings are mostly expected to remain non-significant in further trials for these outcomes.35,36
Compared with the prior meta-analysis by Kelani et al. (search through May 2024; eight studies, 2134 participants; pooled RCTs and observational designs) that concluded early antiplatelet therapy after IV thrombolysis is “safe” and improves excellent functional recovery, our updated and methodologically stricter synthesis (search through September 2025; 12 RCTs totaling 4595 participants) supports a different interpretation. Kelani et al. 14 reported significantly higher odds of mRS 0–1 with early therapy and noted heterogeneity, with no risk of sICH. Our RCT-only analyses, strengthened by incorporating multiple recent large, randomized trials, found no consistent overall functional benefit (mRS 0–1 or mRS 0–2, low and very low certainty). At the same time, the safety point estimates consistently favored harm, with higher odds of sICH (OR = 1.68; moderate certainty) and mortality (OR = 1.15; moderate certainty). Agent-stratified results further refined interpretation by identifying early aspirin as the regimen most consistently associated with increased risk of sICH. However, other agents showed similar trends. At the same time, any potential functional signal appeared to be confined to specific non-aspirin strategies (notably tirofiban) and control contexts and remained sensitive to influential trials. Overall, the combination of a larger randomized evidence base, exclusion of confounding-prone observational data, and the addition of TSA and GRADE explain why our conclusions differ from those of Kelani et al.
Importantly, we should clarify a common misunderstanding of “safety” in prior meta-analyses, which interpret eAPT as safe when there is no statistically significant difference. Absence of statistical significance does not equal absence of clinical significance.37,38 A high risk of 1.77, for example, remains important to consider even in the absence of statistical significance, and conclusions about “safety” should be revised. This is further highlighted when GRADE is used to assess the certainty of findings, as recommended.
Tirofiban, a short-acting, reversible GPIIb/IIIa inhibitor, offers rapid platelet inhibition during the high-risk window for re-occlusion and microembolization while allowing quick offset if bleeding occurs. 39 In our subgroup analysis (four trials), tirofiban was the only agent associated with improved favorable outcome (mRS 0–2: OR = 2.07, 95% CI = 1.25–3.43) while showing a non-significant signal toward higher sICH (OR = 1.77, 95% CI = 0.36–6.82). The preponderance of evidence derives from Tao et al, 11 a major multicenter trial (ASSET-IT) that found that early IV tirofiban significantly increased excellent functional outcomes (mRS 0–1) in non-thrombectomy patients but also showed a higher risk of ICH compared with placebo, underscoring a critical safety trade-off. Also, extended infusion was reported beneficial in one cohort. 25 Most studies used a 0.4 µg/kg/min loading dose more than 30 min followed by maintenance infusion, regarded as the safest regimen, whereas combined intra-arterial and intravenous approaches have been explored with suggested better outcomes.40,41 That said, interpretation of the tirofiban data must be cautious, as our pooled estimates are derived from subgrouping and most trials were conducted in Chinese populations, which limits generalizability; however, a previous meta-analysis of three RCTs supports these findings.42,43 Overall, tirofiban may represent a promising adjunctive option, but adequately powered and geographically diverse trials are required to establish its benefit-to-risk profile before it can be considered for routine use in the early post-thrombolysis setting.
Implications and future directions
Current evidence does not support routine initiation of APT as a broad class within 24 h after IVT, especially given the tendency toward higher sICH risk and the low-to-very low certainty for functional benefit. Clinically, antiplatelets should remain deferred until post-thrombolysis imaging excludes hemorrhage, and “early” strategies should be considered agent- and context-specific (early aspirin appears least favorable; non-aspirin approaches, for example, tirofiban, merit further study). Future work should prioritize adequately powered, multicenter RCTs that standardize agent, dose, timing, and hemorrhage definitions; prespecify enrichment strategies (large-artery disease, incomplete reperfusion, early deterioration); stratify by thrombolytic and thrombectomy status; and incorporate imaging biomarkers. Dose optimization and selection for tirofiban should be prioritized, given signals of potential efficacy coupled with a concern for increased sICH. Moreover, verification in ethnically and geographically diverse cohorts is essential, as most current tirofiban data originate from Chinese populations. Individual-participant data meta-analysis and head-to-head trials of promising agents (notably tirofiban) are needed to determine net clinical benefit in targeted subgroups.
Limitations
This study provides the most up-to-date synthesis of randomized evidence on the use of eAPT in AIS, supported by advanced methodology, including subgroup analyses, meta-regression to explore key baseline moderators, TSA to assess whether evidence is sufficiently accrued, and GRADE to communicate certainty in a decision-relevant manner. However, the eAPT strategy was heterogeneous across trials (agent class, dose, route, and start time), limiting the transportability of pooled averages despite subgroup analyses exploring these modifiers. Efficacy outcomes showed substantial between-study heterogeneity and instability in leave-one-out analyses, warranting cautious interpretation of the results. Some trials had “some concerns” or a high risk of bias, and study-level meta-regression cannot substitute for patient-level effect-modification analyses. Finally, TSA indicated that the available information remains insufficient to draw firm conclusions, particularly regarding efficacy, and clinical benefit is hard to conclude, while clinical harm can be concluded with the few additional large trials.
Conclusion
In this RCT-only meta-analysis, early antiplatelet therapy within 24 h after intravenous thrombolysis did not improve 90-day functional outcomes (mRS 0–1 or 0–2), and TSA indicated that evidence remains inconclusive. Although pooled safety outcomes were not statistically different, effect estimates for symptomatic ICH and mortality trended toward harm, and GRADE assigned moderate certainty to these outcomes, suggesting that a clinically significant bleeding risk cannot be excluded. Early aspirin use appeared most consistently associated with a higher risk of sICH. However, a potential benefit was observed for tirofiban. Overall, current evidence does not support routine early initiation of antiplatelet therapy after thrombolysis, and further adequately powered RCTs are needed to determine whether any selected regimen—especially tirofiban—or subgroup has a favorable risk–benefit profile.
Supplemental Material
sj-docx-1-wso-10.1177_17474930261458007 – Supplemental material for Safety and efficacy of early antiplatelet therapy after intravenous thrombolysis for acute ischemic stroke: A comprehensive meta-analysis with trial sequential analysis
Supplemental material, sj-docx-1-wso-10.1177_17474930261458007 for Safety and efficacy of early antiplatelet therapy after intravenous thrombolysis for acute ischemic stroke: A comprehensive meta-analysis with trial sequential analysis by Hamdy A. Makhlouf, Ahmed Harb, Moaz Elsayed Abouelmagd, Anas Mansour, Ahmed S.A. Osman, Nada Mosad, Ahmed H. Abdelaal, Omar Kassar and Jeffrey L. Saver in International Journal of Stroke
Footnotes
Acknowledgements
Not applicable.
Author Contributions
H.A.M. contributed to study conception and design, data collection, data analysis, drafting of the original manuscript, and critical revision of all tasks. A.H. contributed to the literature review, data extraction, risk-of-bias assessment, and data analysis. M.E.A. contributed to writing the discussion and critical review. A.M., A.S.A.O., N.M., A.H.A., and O.K. contributed to the literature review, data extraction, risk-of-bias assessment, and manuscript writing. J.L.S. contributed to Supervision, Writing – review and editing. All authors revised and approved the final manuscript and any concerns about the integrity or accuracy of any part are duly investigated and addressed. The authors confirm that no paper mill or artificial intelligence was used.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Saver reported receiving consulting fees from Biogen, Boehringer Ingelheim, Genentech, Johnson and Johnson, Phenox, Phillips, Rapid Medical, and Roche for advising on rigorous and safe clinical trial design and conduct outside the submitted work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Not applicable. This study is a systematic review and meta-analysis of previously published randomized controlled trials and did not involve the collection of new human or animal data.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.