
Abstract
Background:
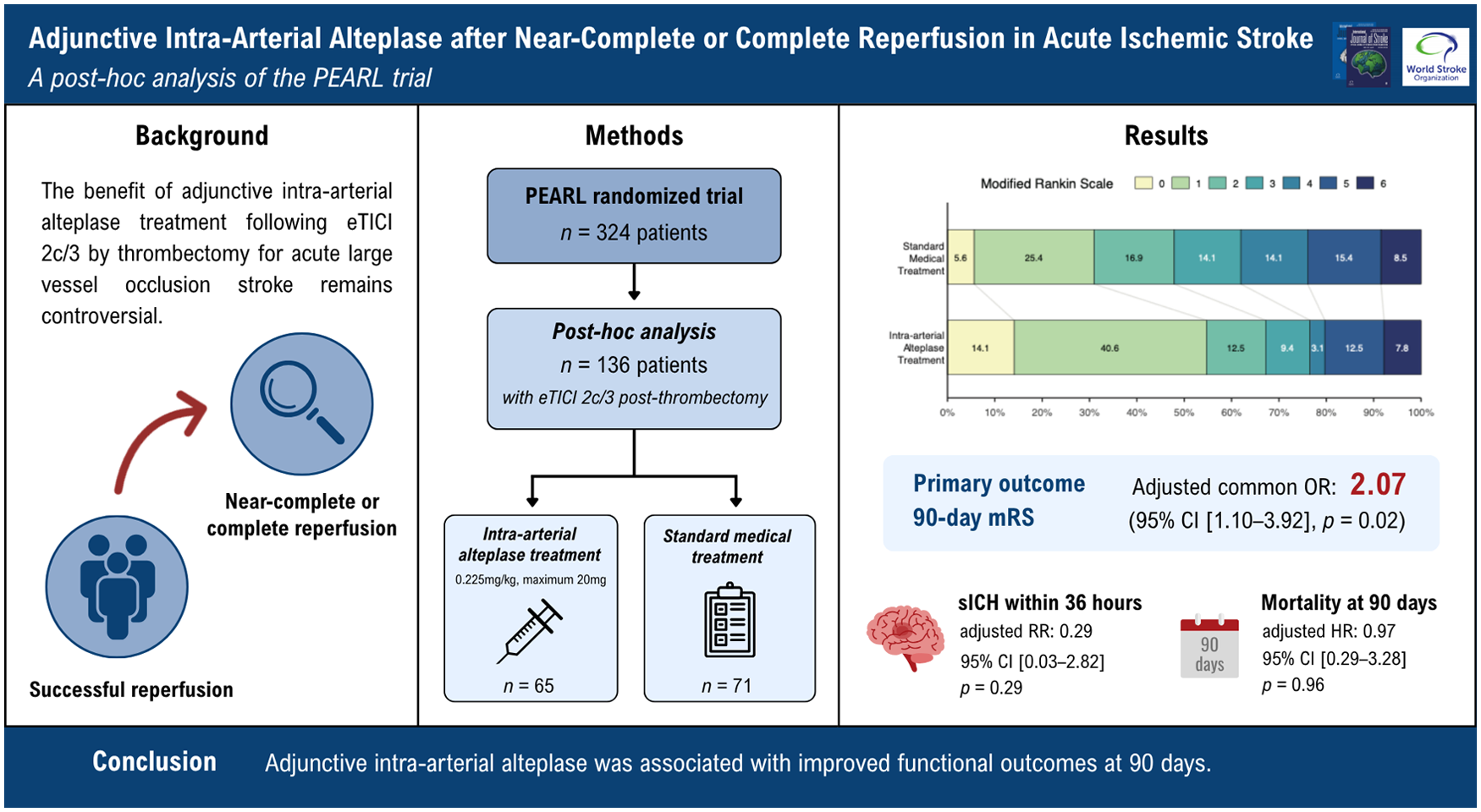
The benefit of adjunctive intra-arterial alteplase treatment following near-complete to complete reperfusion (expanded thrombolysis in cerebral infarction (eTICI) scale of 2c to 3) by mechanical thrombectomy for acute large vessel occlusion stroke remains controversial.
Aims:
The study aimed to explore whether intra-arterial alteplase was associated with improved outcomes in patients with eTICI 2c/3 after thrombectomy compared with standard treatment.
Methods:
This post hoc analysis used data from the PEARL (Intra-arterial Alteplase for Acute Ischemic Stroke After Mechanical Thrombectomy) randomized controlled trial conducted at 28 sites in China. Patients with anterior circulation large-vessel occlusion who achieved eTICI 2c/3 reperfusion after mechanical thrombectomy were included. Patients were randomized to intra-arterial alteplase or standard medical treatment. The primary outcome was the distribution of modified Rankin Scale (mRS) scores at 90 days. Safety outcomes included intracranial hemorrhage and symptomatic intracranial hemorrhage within 36 h and mortality at 90 days.
Results:
Of 324 randomized patients in the PEARL trial, 136 were included in this analysis, with 65 assigned to intra-arterial alteplase and 71 to standard medical treatment. Compared with standard medical treatment, intra-arterial alteplase was associated with a favorable shift in 90-day functional outcome (common odds ratio, 2.07 [95% confidence interval (CI), 1.10–3.92]; P = 0.02). Rates of intracranial hemorrhage (adjusted risk ratio, 1.06 [95% CI, 0.62–1.83]; P = 0.82), symptomatic intracranial hemorrhage within 36 h (adjusted risk ratio, 0.29 [95% CI, 0.03–2.82]; P = 0.29), and mortality at 90 days (adjusted hazard ratio, 0.97 [95% CI, 0.29–3.28]; P = 0.96) did not differ significantly between groups, although the number of safety events was low.
Conclusion:
Among patients in the PEARL trial who achieved near-complete to complete reperfusion after mechanical thrombectomy, adjunctive intra-arterial alteplase was associated with improved functional outcomes at 90 days. Owing to the small sample size of this study, a pooled analysis of intra-arterial alteplase in patients with eTICI 2c/3 is needed to confirm these results.
Registration:
Clinicaltrials.gov identifier: NCT05856851.
Keywords
Introduction
Acute ischemic stroke caused by large vessel occlusion (LVO) remains a leading cause of disability worldwide.1–4 Although endovascular thrombectomy (EVT) achieves high rates of successful reperfusion (defined as expanded thrombolysis in cerebral infarction (eTICI ⩾ 2b50, about half of treated patients regain functional independence at 90 days.5–9 This disparity highlights the limitations of angiographic recanalization alone and suggests that persistent microvascular dysfunction,10,11 such as distal microthrombi, endothelial injury, and the no-reflow phenomenon, may play a significant role even after successful recanalization of large arteries.12,13
To address residual microvascular obstruction following EVT, adjunctive intra-arterial thrombolysis has been proposed as a strategy to enhance downstream reperfusion. Early evidence from the CHOICE trial (Chemical Optimization of Cerebral Embolectomy) suggested that intra-arterial alteplase administered after successful reperfusion (eTICI score of 2b–3) improved excellent functional outcomes at 90 days without increasing the risk of symptomatic intracranial hemorrhage, although the trial was terminated early. 14 Subsequently, the PEARL trial (Intra-arterial Alteplase for Acute Ischemic Stroke After Mechanical Thrombectomy) further demonstrated functional benefit associated with adjunctive intra-arterial alteplase in patients achieving successful reperfusion after mechanical thrombectomy. 15
However, trials specifically focusing on patients with near-complete or complete reperfusion (⩾90% reperfusion) have reported neutral findings. Both the POST-TNK trial (Adjunctive Intra-arterial Tenecteplase Following Near-Complete to Complete Reperfusion for Large Vessel Occlusion Stroke) and POST-UK trial (Adjunctive Intra-Arterial Urokinase After Near-Complete to Complete Reperfusion for Acute Ischemic Stroke) failed to show a statistically significant improvement in disability-free survival at 90 days.16,17 Consistent with these findings, recent meta-analyses indicate that the potential benefit of adjunctive intra-arterial thrombolysis may differ according to the degree of angiographic reperfusion, with more consistent signals observed in patients with incomplete reperfusion (eTICI 2b), whereas the role of adjunctive intra-arterial thrombolysis in patients achieving near-complete or complete reperfusion (eTICI 2c/3) remains unclear.18,19 Although trials using tenecteplase and urokinase yielded neutral results in this population, there is currently no dedicated evidence assessing the efficacy and safety of adjunctive intra-arterial alteplase in patients with eTICI 2c/3 reperfusion.
This post hoc analysis of the PEARL trial was, therefore, designed to evaluate whether adjunctive intra-arterial alteplase is associated with improved functional outcomes and acceptable safety among patients achieving near-complete or complete reperfusion after mechanical thrombectomy.
Methods
Data availability
The data that support the findings of this study are available from the corresponding authors.
Study design and participants
The PEARL trial was approved by the ethics committee at Sun Yat-sen Memorial Hospital (SYSKY-2023-390-02) and all participating centers. The trial was a multicenter, prospective, open-label, blinded endpoint, randomized clinical trial conducted at 28 hospitals in China between August 1, 2023, and October 16, 2024.
Eligibility criteria included adults aged 18 years or older with an ischemic stroke due to occlusion of the internal carotid or M1 or M2 segment of the middle cerebral artery (MCA), an Alberta Stroke Program Early CT Score (ASPECTS; range, 0–10; lower scores indicate more severe infarction) of 6 or greater based on results from a CT scan or a diffusion-weighted magnetic resonance imaging scan, who achieved successful reperfusion defined as an eTICI score of 2b50 to 3 after mechanical thrombectomy, and could be randomized within 24 h from last known well. Further details regarding inclusion and exclusion criteria, as well as detailed trial protocol and primary results, are published elsewhere. 15 All patients or their surrogates provided written informed consent. Patients were randomized to receive intra-arterial alteplase treatment (0.225 mg/kg; maximum dose, 20 mg) or standard medical treatment, using a web-based centralized system, stratified by study centers and receipt of intravenous thrombolysis. All patients received standard medical management, including intravenous thrombolytics if eligible according to the clinical guidelines. However, for patients randomized to the intra-arterial alteplase group who achieved recanalization within 60 min of treatment initiation with intravenous alteplase, the site investigators were permitted to determine whether and when to discontinue the intravenous infusion. Mechanical thrombectomy procedures were limited to a maximum of 6 passes and prohibited after randomization. For this post hoc analysis, only patients who achieved near-complete or complete reperfusion (⩾90% macrocirculatory reperfusion) after mechanical thrombectomy were included. This study followed the Consolidated Standards of Reporting Trials (CONSORT) reporting guideline.
Data collection
The baseline, procedural, and outcome variables for this study, including demographic information, premorbid modified Rankin Scale (mRS) scores, medical history, admission National Institutes of Health Stroke Scale scores (NIHSS; range, 0–42, with higher scores indicating greater stroke severity), laboratory and imaging results, procedural details, periprocedural management, time metrics, and mRS scores at 90 days, were prospectively collected. The 90-day mRS scores were followed up blindly by trained independent interviewers via telephone. 20 An independent imaging core laboratory, blinded to clinical data, reviewed all imaging, including the baseline ASPECTS, infarct volume, eTICI grade, and intracranial hemorrhage. The baseline infarct volume was automatically measured using electronic stroke assessment software (NeuBrainCARE version 1.0, Neusoft). Preintervention and final reperfusion quality were assessed via catheter angiograms based on eTICI score: eTICI grade 0 is equivalent to no reperfusion or 0% filling of the downstream territory, eTICI 1 reflects thrombus reduction without any reperfusion of distal arteries, eTICI 2a is reperfusion in less than half or 1% to 49% of the territory, eTICI 2b is 50% to 89% reperfusion, eTICI 2c is 90% to 99% reperfusion, and eTICI 3 is complete or 100% reperfusion. 21
Study outcomes
The primary outcome was a shift in the distribution of scores on mRS at 90-day follow-up. Secondary clinical outcomes included freedom from disability (mRS score of 0 or 1), functional independence (mRS score of 0–2), independent ambulation (mRS score of 0–3), early neurological improvement (defined as improvement of ⩾8 points on NIHSS at 24 h of presentation or an NIHSS of 0–1), and severe disability or death (mRS score of 5–6) at 90-day follow-up. Safety outcomes included intracranial hemorrhage within 36 h, symptomatic intracranial hemorrhage (per the Heidelberg criteria) within 36 h, and mortality (mRS score of 6) within 90 days.
Statistical analysis
Categorical variables were summarized as counts and percentages and compared using the chi-square or Fisher’s exact tests, as appropriate. Continuous variables were presented as medians with interquartile ranges (IQR) and compared using the Wilcoxon rank-sum test. For the shift analysis of the 90-day mRS distribution, ordinal logistic regression was performed, and the common odds ratio (OR) with 95% confidence intervals (CIs) was reported when the proportional odds assumption was satisfied. Treatment effects of intra-arterial alteplase on binary secondary efficacy outcomes and safety outcomes were evaluated using generalized linear models with log link using binomial distribution, incorporating random effects for study centers (the centers with <20 enrolled patients were pooled). The Cox proportional hazards model was used to estimate hazard ratios with 95% CIs for death within 90 days. All adjusted models included prespecified covariates (age, sex, and intravenous thrombolysis before EVT).
Sensitivity analyses additionally adjusted for eTICI grade (2c versus 3) and time from last known well to randomization, with multiple imputation for missing mRS values. A per-protocol analysis was also conducted among participants without major protocol deviations, as defined in the original trial protocol. This analysis used the same covariate adjustment as the sensitivity analysis but was performed without multiple imputation. An additional exploratory analysis stratified by final eTICI grade after thrombectomy (eTICI 2c versus eTICI 3) was performed. Treatment-by-eTICI grade interaction was assessed by adding an interaction term to the corresponding regression model where applicable. All analyses were performed according to randomized treatment assignment. Statistical analyses were conducted using R version 4.4.2 (R Foundation). All hypothesis tests were two-sided, and a P value < 0.05 was considered statistically significant.
Results
Baseline characteristics
A total of 1879 patients were screened, of whom 324 met the inclusion and exclusion criteria and were randomized in the PEARL trial. Among these patients, 136 (42.0%) achieved eTICI 2c/3 reperfusion after mechanical thrombectomy and were included in the present post hoc analysis (107 (78.7%) with eTICI 2c and 29 (21.3%) with eTICI 3). There were 65 participants assigned to the intra-arterial alteplase treatment (intervention) group and 71 assigned to the standard treatment (control) group (Figure 1). The median age was 69 years (IQR, 59–76), and 35 (25.7%) were female. Two participants in the intra-arterial alteplase group and four participants in the standard treatment group were excluded from the per-protocol analysis due to protocol deviations or were lost to follow-up.
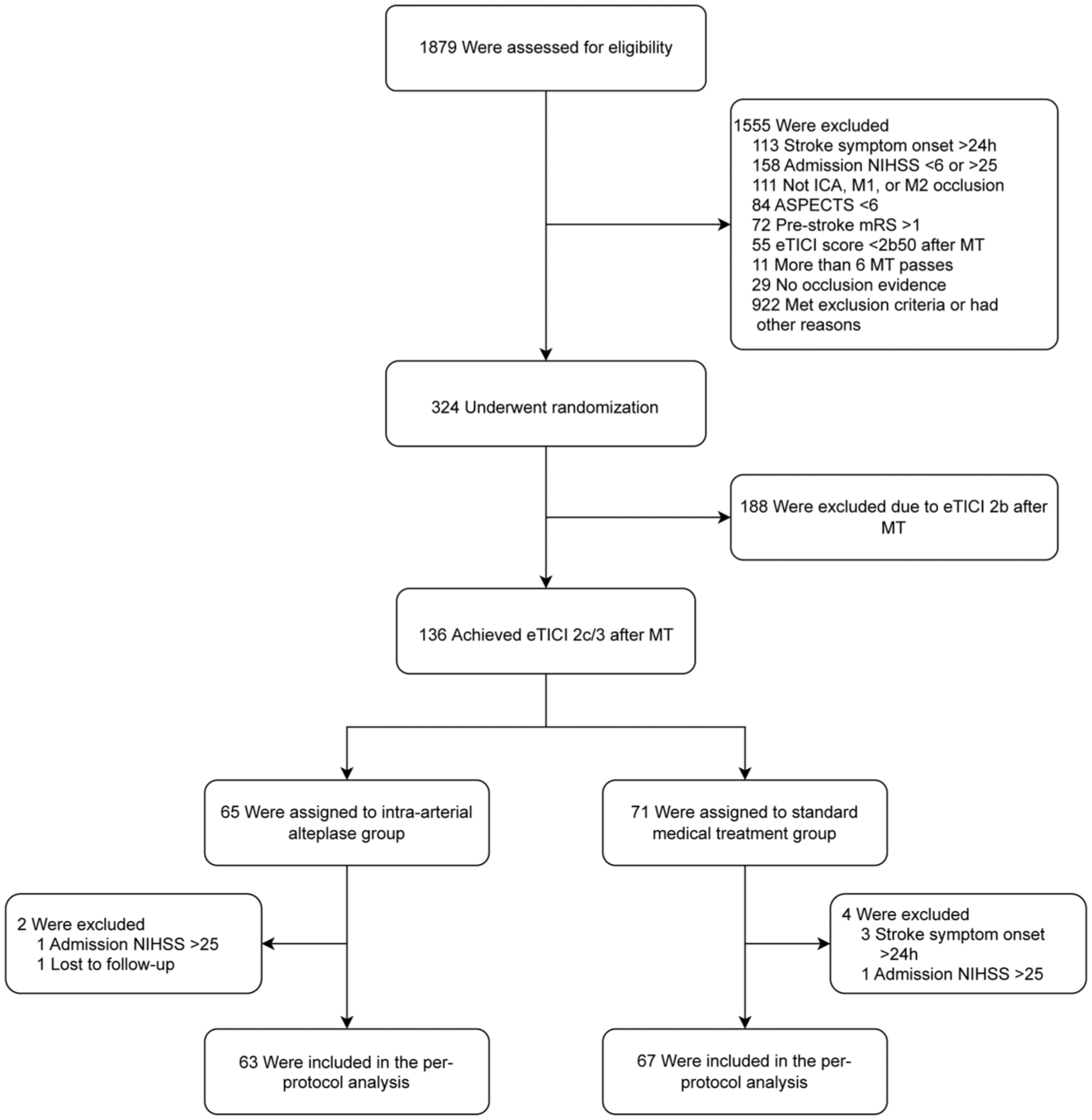
Flowchart. The selection of participants included in this post hoc analysis is shown. Abbreviation: ASPECTS, Alberta Stroke Program Early CT Score; eTICI, expanded thrombolysis in cerebral infarction; ICA, internal carotid artery; mRS, Modified Rankin Scale; MT, mechanical thrombectomy; NIHSS, National Institutes of Health Stroke Scale.
The baseline characteristics for the eTICI 2c/3 population are shown in Table 1, and detailed characteristics of endovascular therapy are available in Supplemental Table S1. The patients in each treatment group were generally well-matched on baseline characteristics, including age, sex, medical history, NIHSS, use of intravenous thrombolysis pretreatment, and ASPECTS (Table 1). The distribution of occlusion sites differed significantly between the two groups (P = 0.01), with M1 segment occlusion of the MCA being more common in the control group (83.1% versus 63.1%) and M2 segment occlusion of the MCA more frequent in the intervention group (4.2% versus 18.5%). Patients in the control group had a higher proportion of eTICI 3 grade (28.2% versus 13.9%; P = 0.07) and a longer time interval from last known well to randomization (429 min [IQR, 335–660] versus 356 min [IQR, 244–622]; P = 0.10), which were included as additional covariates in sensitivity analyses.
Baseline characteristics between intra-arterial alteplase and standard treatment in eTICI 2c/3 population.
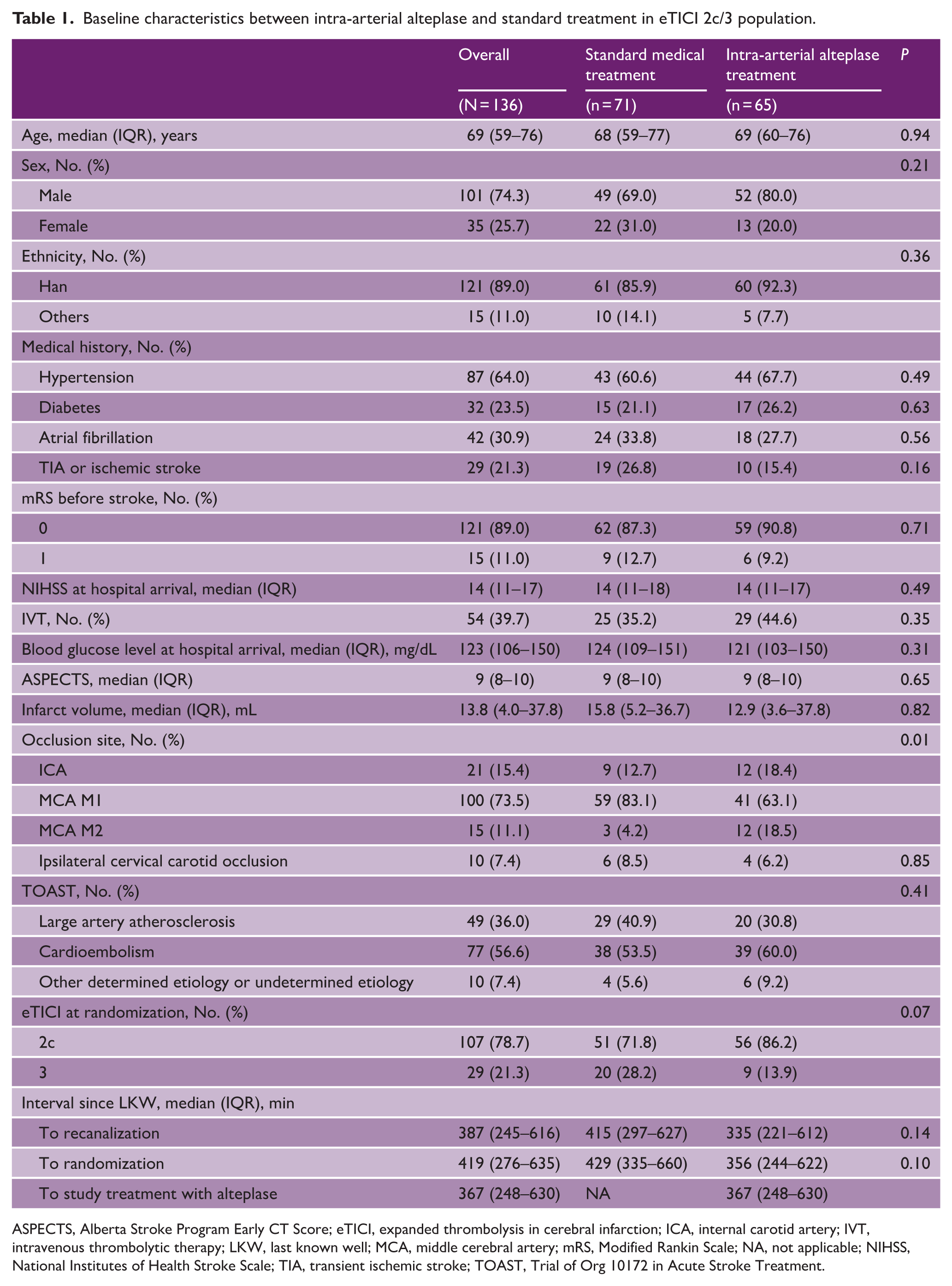
ASPECTS, Alberta Stroke Program Early CT Score; eTICI, expanded thrombolysis in cerebral infarction; ICA, internal carotid artery; IVT, intravenous thrombolytic therapy; LKW, last known well; MCA, middle cerebral artery; mRS, Modified Rankin Scale; NA, not applicable; NIHSS, National Institutes of Health Stroke Scale; TIA, transient ischemic stroke; TOAST, Trial of Org 10172 in Acute Stroke Treatment.
Clinical outcomes
In the eTICI 2c/3 population, intra-arterial alteplase was associated with a favorable shift in the distribution of 90-day mRS scores compared with standard medical treatment (adjusted common OR, 2.07 [95% CI, 1.10–3.92]; P = 0.02). The distribution of mRS scores by treatment arm is shown in Figure 2. Similarly, when evaluated as a dichotomized outcome, patients treated with intra-arterial alteplase more frequently achieved freedom from disability at 90 days (mRS 0–1; adjusted risk ratio, 1.81 [95% CI: 1.14–2.87]; P = 0.01) and functional independence (mRS 0–2; adjusted risk ratio, 1.41 [95% CI: 1.02–1.95]; P = 0.03). For independent ambulation (mRS 0–3), the proportion of patients achieving this outcome was numerically higher in the intra-arterial alteplase group, but the difference was not statistically significant (adjusted risk ratio, 1.20 [95% CI: 0.97–1.48]; P = 0.09). Early neurological improvement at 24 h (NIHSS score of 0 or 1 or a reduction of ⩾8 points) occurred in 22 of 65 patients (33.9%) in the intra-arterial alteplase group and in 14 of 71 patients (19.7%) in the standard treatment group (adjusted risk ratio, 1.63 [95% CI: 1.00–2.66], P = 0.051). Complete dependence or death (mRS 5–6) at 90 days did not differ between treatment groups (adjusted risk ratio, 0.95 [95% CI: 0.41–2.20]; P = 0.91). The unadjusted results are presented in Table 2. Sensitivity analyses incorporating additional covariate adjustment for eTICI grades and time from last known well to randomization, as well as analyses based on multiple imputation for missing 90-day mRS values, yielded similar results. The per-protocol analysis among participants without major protocol deviations also showed a consistent association between intra-arterial alteplase and a favorable shift in 90-day mRS distribution (adjusted common OR, 2.23 [95% CI, 1.16–4.36]; P = 0.02) (Supplemental Table S2).
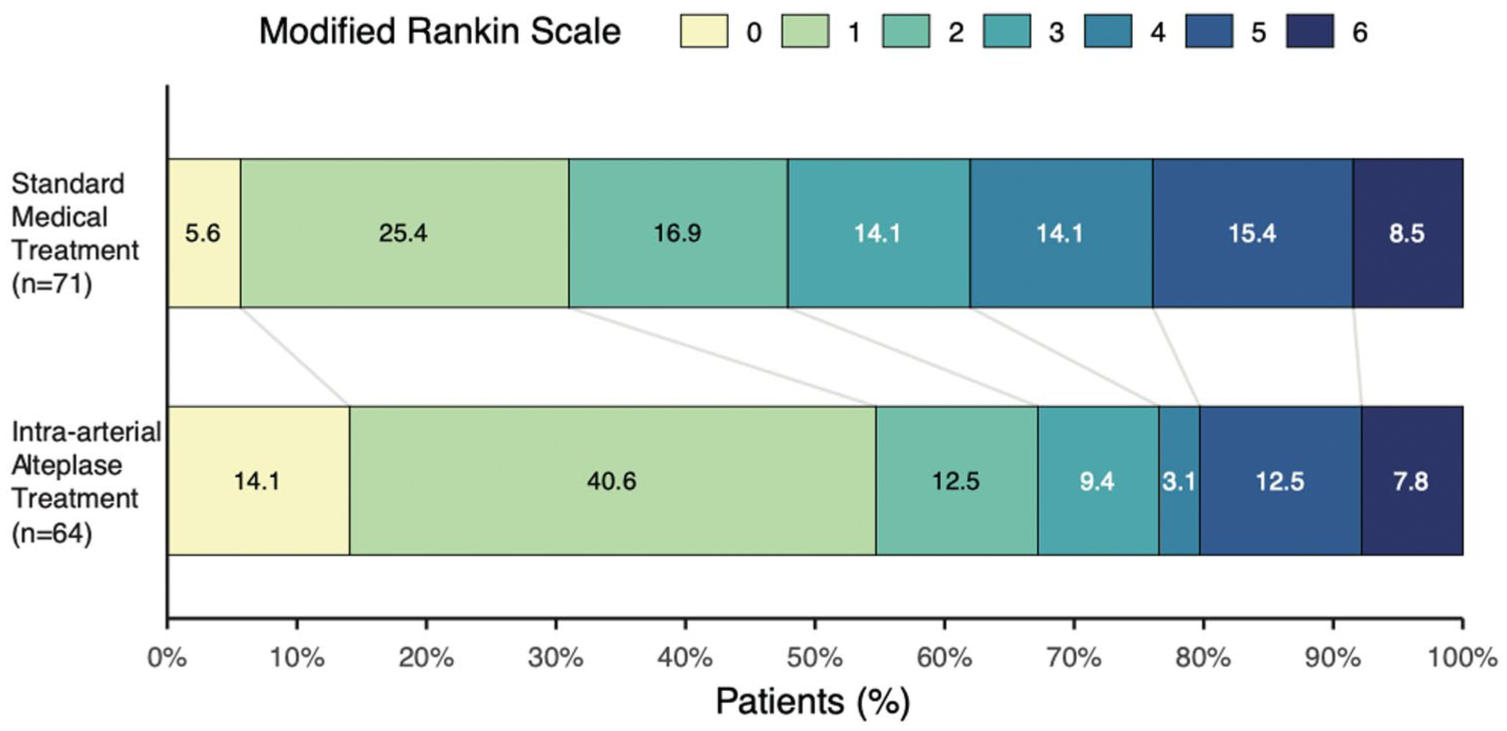
Distribution of 90-day modified Rankin Scale outcomes following near-complete or complete reperfusion, stratified by treatment assignment. The distribution of modified Rankin Scale (mRS) scores at 90 days is shown for patients who achieved near-complete or complete reperfusion and were assigned to intra-arterial alteplase treatment or standard medical treatment. The percentage of participants achieving each mRS score from 0 (no symptoms) to 6 (death) is presented for the intra-arterial alteplase group (bottom row) and the standard treatment group (top row), with values in each bar indicating the proportion of patients in the corresponding outcome category.
Effect of intra-arterial alteplase versus standard treatment in eTICI 2c/3 population.
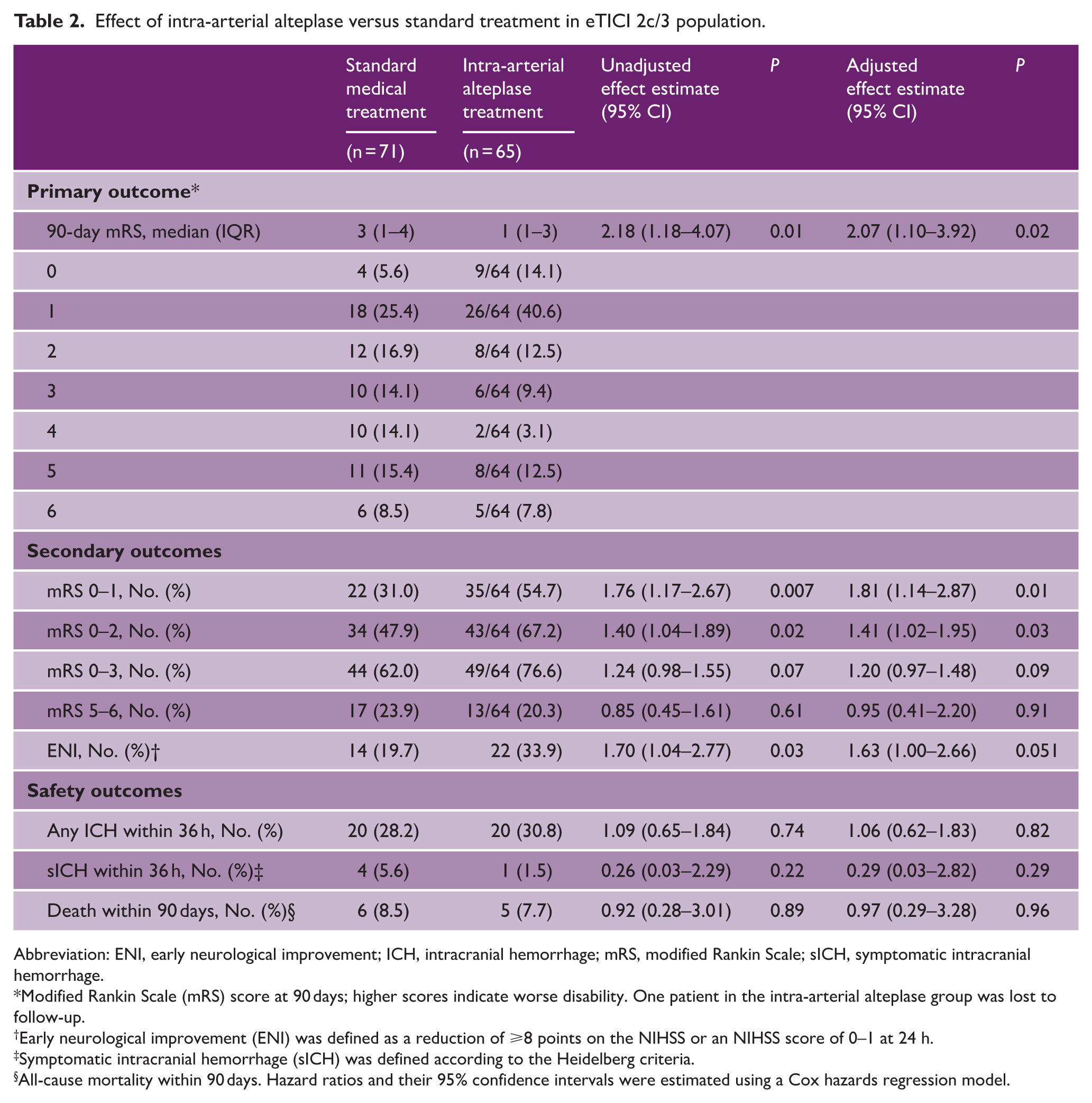
Abbreviation: ENI, early neurological improvement; ICH, intracranial hemorrhage; mRS, modified Rankin Scale; sICH, symptomatic intracranial hemorrhage.
Modified Rankin Scale (mRS) score at 90 days; higher scores indicate worse disability. One patient in the intra-arterial alteplase group was lost to follow-up.
Early neurological improvement (ENI) was defined as a reduction of ⩾8 points on the NIHSS or an NIHSS score of 0–1 at 24 h.
Symptomatic intracranial hemorrhage (sICH) was defined according to the Heidelberg criteria.
All-cause mortality within 90 days. Hazard ratios and their 95% confidence intervals were estimated using a Cox hazards regression model.
For safety outcomes, the incidence of any intracranial hemorrhage within 36 h did not differ significantly between the intra-arterial alteplase group and the standard treatment group (30.8% vs. 28.2%; adjusted risk ratio, 1.06 [95% CI: 0.62–1.83]; P = 0.82). Symptomatic intracranial hemorrhage within 36 h occurred in 1 of 65 patients (1.5%) in the intra-arterial alteplase group and in 4 of 71 patients (5.6%) in the standard treatment group, with no significant between-group difference (adjusted risk ratio, 0.29 [95% CI: 0.03–2.82]; P = 0.29). The distribution of intracranial hemorrhage subtypes according to the Heidelberg bleeding classification is shown in Supplemental Table S3. Hemorrhagic infarction (HI)2 and parenchymatous hematoma (PH)1 were among the most frequently observed hemorrhage subtypes in both groups. Death within 90 days occurred in five patients (7.7%) in the intra-arterial alteplase group and in six patients (8.5%) in the standard treatment group (adjusted hazard ratio, 0.97 [95% CI: 0.29–3.28]; P = 0.96).
In the additional exploratory analysis stratified by final eTICI grade, intra-arterial alteplase treatment was associated with a favorable shift in the 90-day mRS distribution in patients with eTICI 2c reperfusion. Among the 29 patients with eTICI 3 reperfusion, no clear treatment effect was observed. No statistically significant interaction was detected for dichotomized 90-day mRS outcomes or for any intracranial hemorrhage within 36 h (Supplemental Table S4).
Discussion
In this post hoc analysis of the PEARL randomized clinical trial restricted to patients achieving near-complete or complete reperfusion (eTICI 2c/3) after mechanical thrombectomy, adjunctive intra-arterial alteplase was associated with improved functional outcomes at 90 days, with no statistically significant difference in symptomatic intracranial hemorrhage or mortality. These exploratory findings suggest that angiographically successful reperfusion does not necessarily equate to complete tissue-level reperfusion, and that residual microvascular obstruction may continue to limit neurological recovery even in patients with optimal eTICI grades. Adjunctive intra-arterial alteplase may partially mitigate this residual microcirculatory impairment and thereby confer additional clinical benefit.
The present results are consistent with evidence from the CHOICE trial, which reported a higher rate of excellent functional outcome (mRS 0–1) with adjunctive intra-arterial alteplase after successful reperfusion. More recently, results of the CHOICE-2 trial presented at the International Stroke Conference 2026 strengthened the evidence that intra-arterial alteplase after successful thrombectomy can improve recovery. 22 Subgroup analyses stratified by final eTICI grade after thrombectomy in both CHOICE and CHOICE-2 demonstrated a consistent treatment effect, with adjunctive intra-arterial alteplase being associated with improved functional outcomes even among patients achieving near-complete or complete reperfusion (eTICI 2c/3).14,22
The POST-TNK and POST-UK trials, explicitly designed to enroll only patients with eTICI 2c/3 reperfusion treated with intra-arterial tenecteplase or urokinase, respectively, did not demonstrate statistically significant improvements in the primary outcome, although numerical trends favored the adjunctive therapy.16,17 A subsequent post hoc pooled individual patient data analysis from POST-TNK and POST-UK, however, revealed significantly better function outcomes with intra-arterial thrombolysis, suggesting that limited statistical power rather than absence of efficacy may partly explain the neutral primary results. 23 Findings from the ANGEL-TNK trial (Intra-arterial Tenecteplase for Acute Stroke After Successful Endovascular Therapy) further highlight the complexity of treatment effects across reperfusion grades. 24 While intra-arterial tenecteplase improved excellent outcomes in the overall population achieving eTICI ⩾ 2b reperfusion, subgroup analyses demonstrated that the benefit was more pronounced among patients with incomplete reperfusion (eTICI 2b), whereas no statistically significant benefit was observed in those achieving eTICI 2c/3. 24
Differences in thrombolytic agents and dosing strategies may partly account for the heterogeneity observed across trials. The PEARL, CHOICE, and CHOICE-2 trials used intra-arterial alteplase at 0.225 mg/kg. The POST-TNK trial administered intra-arterial tenecteplase at 0.0625 mg/kg. In the ANGEL-TNK, intra-arterial tenecteplase at 0.125 mg/kg appeared to show greater benefit primarily in patients with incomplete reperfusion grades. 24 The POST-UK employed a fixed single dose of intra-arterial urokinase (100,000 IU), which represents a different dosing strategy from the alteplase and tenecteplase trials. 17 Such differences may be particularly relevant in eTICI 2c/3 reperfusion, where the remaining thrombotic burden is likely to be small, distal, and partly microvascular, and intra-arterial thrombolytic therapy may help target residual distal microthrombi. Treatment response may depend on drug-specific pharmacologic properties, dose-selection strategies, and the extent and location of residual thrombotic burden. In addition, the phase 1/2 dose-escalation trial (DATE) evaluated intra-arterial tenecteplase administered after successful reperfusion across doses ranging from 0.0313 to 0.125 mg/kg. 25 The 0.0313 and 0.0625 mg/kg regimens were reported to an acceptable safety profile, but intra-arterial tenecteplase at 0.125 mg/kg was associated with an increased risk of symptomatic intracranial hemorrhage. In this study, the absolute rates of symptomatic intracranial hemorrhage and mortality were numerically low in both groups. According to the Heidelberg bleeding classification, HI2 and PH1 were among the most common subtypes, with no apparent shift toward more severe hemorrhagic patterns in the intra-arterial alteplase group. These present studies do not allow direct comparisons across thrombolytic agents or dosing regimens, but they highlight the need for future studies to determine the optimal intra-arterial thrombolytic agent, dose, and target population after near-complete or complete reperfusion.
The current analysis raises the possibility that eTICI 2c/3 may not always represent the therapeutic ceiling after mechanical thrombectomy. While achieving near-complete or complete angiographic recanalization is strongly associated with a favorable prognosis, it does not ensure complete microvascular reperfusion or maximal clinical benefit. This discordance between macrovascular recanalization and tissue-level reperfusion likely contributes to the substantial heterogeneity in clinical outcomes observed among patients achieving eTICI 2c/3 reperfusion. The observed association between adjunctive intra-arterial alteplase and improved functional outcomes may, therefore, represent a rational approach to bridging this gap and extending the benefits of thrombectomy beyond large-vessel recanalization alone. Separately, in the additional analysis stratified by final eTICI grade, the treatment effect was not clear in the subgroup of 29 patients with eTICI 3 reperfusion, but the result showed no evidence of treatment effect modification between eTICI grade strata. The observed treatment effect should be interpreted with caution and considered exploratory.
These findings further support the hypothesis that residual microvascular dysfunction remains a therapeutically targetable barrier even after high-grade macrovascular recanalization.12,14,26–28 Distal microthrombi, endothelial injury, edema-related microvascular compression, and microvascular no-reflow phenomena are increasingly recognized as critical contributors to incomplete tissue reperfusion following endovascular therapy.10,12,29–31 These microcirculatory disturbances can persist despite restoration of proximal arterial patency and may substantially undermine the prognostic gains expected from achieving eTICI 2c/3 reperfusion. In this context, adjunctive intra-arterial alteplase may facilitate dissolution of residual distal thrombus burden and improve capillary-level flow, thereby enhancing tissue salvage and functional recovery.
Emerging evidence of radiographic markers of microvascular no-reflow also underscores that a substantial proportion of patients with eTICI 2c/3 reperfusion may harbor clinically meaningful downstream obstruction that limits recovery. 32 In a post hoc pooled analysis of the EXTEND-IA and EXTEND-IA TNK trials, despite angiography showing near-complete or complete reperfusion, about 20% of patients still exhibited persistent tissue-level hypoperfusion, and the no-reflow phenotype was associated with poorer functional outcomes and larger infarct volumes. 33 Integration of such advanced imaging modalities into future trial designs could enable more precise identification of patients likely to benefit from adjunctive therapies. These findings suggest that achieving eTICI 2c/3 reperfusion may not be sufficient to ensure optimal neurological recovery in all patients. Adjunctive intra-arterial alteplase may offer additional benefit by targeting residual microvascular pathology that persists beyond successful mechanical thrombectomy. Future prospective randomized trials are warranted to validate these exploratory observations, and the underlying mechanisms could be explained by incorporating image-based assessments of microvascular perfusion.
Limitations
This study has some limitations. First, this was an exploratory post hoc analysis that was not prespecified in the original trial protocol and was conducted in a relatively small subgroup. Given the relatively large observed treatment effect and wide CIs for the primary outcome, these findings should be interpreted cautiously in view of the risks of multiple testing, inflated type I error, and possible overestimation. Second, although multivariable adjustment was performed for key baseline covariates, residual confounding cannot be fully excluded, including potential heterogeneity in reperfusion quality within the eTICI 2c/3 grades. Third, because the number of safety events was low (particularly for symptomatic intracranial hemorrhage), this analysis had limited statistical power and precision to assess safety outcomes. It is possible that small differences went undetected owing to the limited sample size of this study. Moreover, this post hoc analysis did not include a detailed imaging-based assessment, which limited further mechanistic interpretation of the findings. Finally, because the trial enrolled patients exclusively from centers in China, the generalizability of these findings to populations with different genetic backgrounds, stroke etiologies, or healthcare systems may be limited.
Conclusion
In this post hoc analysis of the PEARL trial restricted to patients achieving near-complete or complete reperfusion (eTICI 2c/3) after mechanical thrombectomy, adjunctive intra-arterial alteplase was associated with better 90-day functional outcomes with no statistically significant difference in symptomatic intracranial hemorrhage or mortality. These findings should be considered hypothesis-generating, and a pooled analysis of intra-arterial alteplase in patients with eTICI 2c/3 reperfusion is needed to confirm these results.
Supplemental Material
sj-docx-1-wso-10.1177_17474930261461367 – Supplemental material for Adjunctive intra-arterial alteplase after near-complete or complete reperfusion in acute ischemic stroke: A post hoc analysis of the PEARL Trial
Supplemental material, sj-docx-1-wso-10.1177_17474930261461367 for Adjunctive intra-arterial alteplase after near-complete or complete reperfusion in acute ischemic stroke: A post hoc analysis of the PEARL Trial by Mingyi Bao, Chunnuan Chen, Haoyang Sun, Zhenhong Deng, Yanting Chen, Ruiqi Xue, Baixuan He, Xinguang Yang, Yi Li, Songhua Xiao, Yamei Tang and Yongteng Xu in International Journal of Stroke
Footnotes
Author contributions
Y.T. and Y.X. had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. M.B., C.C., and H.S. contributed equally to the study. Y.L., S.X., Y.T., and Y.X. were co-senior authors and contributed equally to the study.
Concept and design: Y.T., M.B., and Z.D.
Acquisition, analysis, or interpretation of data: M.B., H.S., Y.C., R.X., and Y.X.
Critical review of the article for important intellectual content: Z.D., M.B., X.Y., B.H, and Y.X.
Statistical analysis: M.B., Z.D., and C.C.
Obtained funding: Y.T., Y.X., and S.X.
Administrative, technical, or material support: Y.T., C.C., and Y.L.
Supervision: Y.T., Y.X, S.X., and Y.L.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Brain Science and Brain-like Intelligence Technology–National Science and Technology Major Project (2022ZD0211600), the National Natural Science Foundation of China (82330099, 82530100), the Key-Area Research and Development Program of Guangdong Province (2023B0303040003), Science and Technology Program of Guangzhou (2023A03J0708), and the Sun Yat-sen Memorial Hospital Clinical Research 5010 Program (SYS-5010Z-202302) to Y. Tang; the National Natural Science Foundation of China (82473563) and Guangzhou Science and Technology Program (2024A03J0911) to Y. Xu; and the National Natural Science Foundation of China (81872261) to S. Xiao.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.