
Abstract
Background:
Atrial fibrillation and atrial flutter (AF/AFL) are major contributors to ischemic stroke, heart failure, disability, and mortality worldwide.
Objective:
To provide a descriptive global analysis of AF/AFL burden using Global Burden of Disease (GBD) 2023 estimates, with emphasis on incidence, prevalence, deaths, disability-adjusted life years (DALYs), and their distribution by sex, age, and socio-demographic index (SDI).
Methods:
We performed a descriptive epidemiological analysis using direct extractions from the Institute for Health Metrics and Evaluation Global Burden of Disease 2023 Results Tool for the cause category “atrial fibrillation and atrial flutter.” We assessed incidence, prevalence, deaths, DALYs, and selected rates globally and according to sex, quinquennial age group, and SDI. Temporal trends were examined using available historical series, and the 2023 burden was summarized across major demographic and SDI strata.
Results:
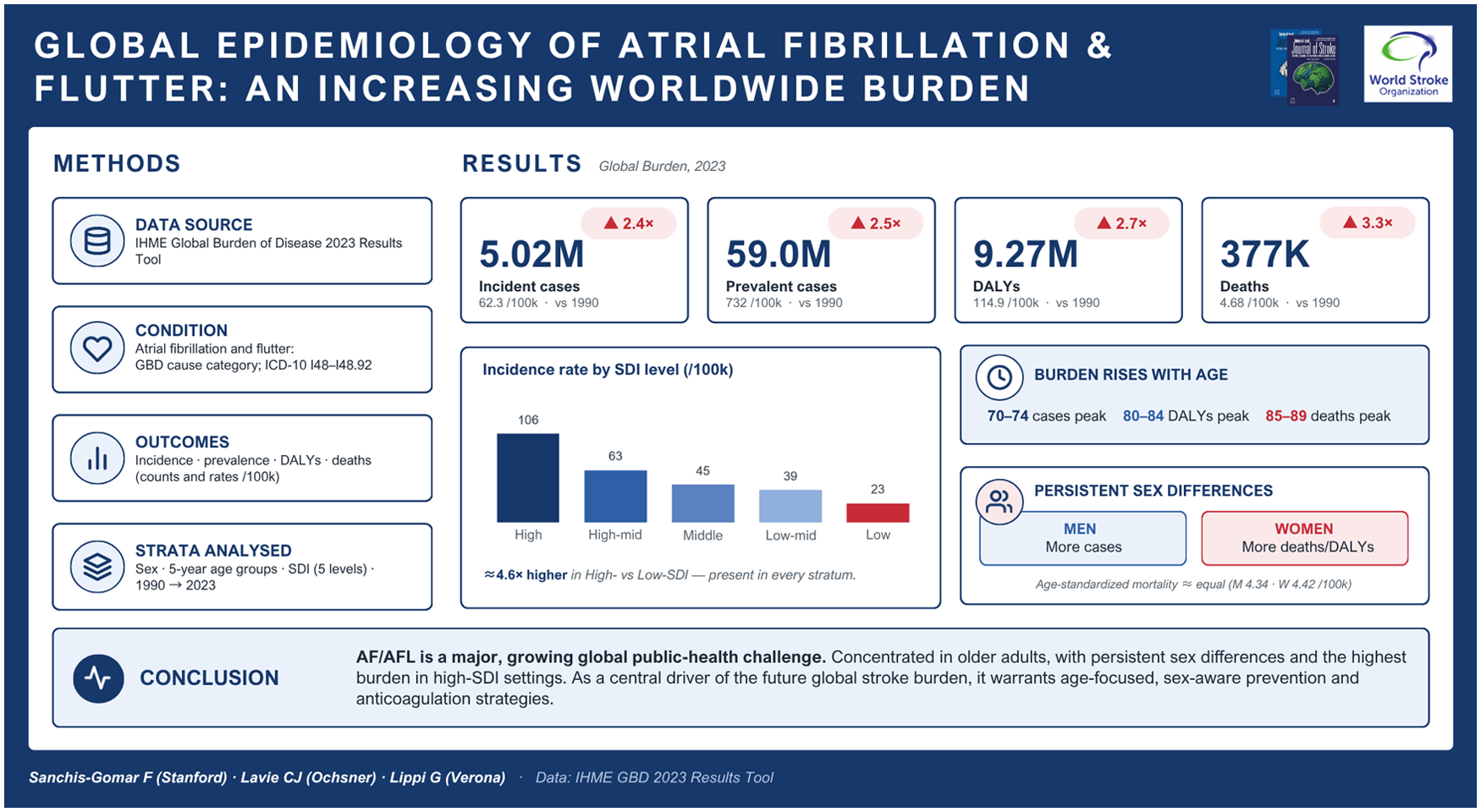
In 2023, AF/AFL accounted globally for 5,021,980 incident cases, 59,045,058 prevalent cases, 9,265,726 DALYs, and 377,258 deaths. Compared with 1990, the global burden increased substantially in absolute terms. It was substantially higher in older adults, with the highest observed counts of incident and prevalent cases in the 70- to 74-year age group, the highest DALY counts in the 80- to 84-year age group, and the highest death counts in the 85- to 89-year age group. Men accounted for more incident and prevalent cases in absolute terms, whereas women accounted for more deaths and DALYs; age-standardized rates indicated higher male incidence, prevalence, and DALYs, but essentially equivalent mortality between sexes. High-SDI settings carried the largest absolute burden and the highest rates across all major metrics. Overall, the findings indicate a marked expansion in the global AF/AFL burden, with important heterogeneity by age, sex, and socio-demographic development.
Conclusion:
AF/AFL remains a major and growing global public health challenge. The burden is increasingly concentrated in older populations, shows persistent sex differences, and remains greater in high-SDI settings. These findings reinforce the relevance of AF/AFL to stroke prevention, health-system planning, and long-term cardiovascular care worldwide.
Keywords
Background
Atrial fibrillation (AF) is the most frequent sustained cardiac arrhythmia and an important cause of ischemic stroke, heart failure (HF), hospitalization, disability, healthcare expenditure, and premature death.1–3 Its growing worldwide burden has made AF a major public health concern, especially in aging populations and in health systems increasingly challenged by chronic cardiovascular disease (CVD).2,4,5
In recent years, the epidemiological context of AF has evolved in several important ways. First, Global Burden of Disease (GBD) estimates now extend through 2023, enabling a contemporary assessment of AF and atrial flutter (AFL) using a consistent international framework. Recent GBD-based analyses have highlighted the continuing expansion and changing age profile of AF/AFL burden.1,6 Second, the burden continues to increase in absolute terms, but its interpretation is more complex than simple numeric expansion alone. Population aging, improved survival from CVD, and broader detection through contemporary monitoring pathways and wearable devices may contribute to the observed increase.2,4,7 Third, modern AF/AFL care increasingly incorporates screening, digital detection, and risk-factor management, reinforcing the need to interpret epidemiological patterns through both clinical and health-system perspectives.2,4
A thorough reassessment of the worldwide epidemiology of AF/AFL is hence necessary. Specifically, current data enable a contemporary descriptive analysis of temporal trends, sex differences, age distribution, and socio-demographic factors, as well as the distinction between absolute burden and rate-based burden in the current era of demographic aging and expanding AF/AFL detection. Accordingly, this study aimed to provide a contemporary global analysis of AF/AFL burden using GBD 2023 data, with emphasis on incidence, prevalence, disability-adjusted life years (DALYs), and mortality, and their distribution by sex, age, and the socio-demographic index (SDI).
Methods
Data source
We conducted a descriptive epidemiological study using direct extractions from the Institute for Health Metrics and Evaluation (IHME) GBD Results Tool, focusing on the cause category “atrial fibrillation and atrial flutter” (AF/AFL). 6 The GBD platform provides standardized estimates of disease burden across countries, years, sexes, age groups, and socio-demographic strata. The exact extraction settings used for the main analyses, including cause category, measures, metrics, sex, age grouping, location, year range, and SDI filters, are provided in Supplementary Table S1.
Case definition
AF/AFL burden estimates were retrieved from the IHME GBD Results Tool using the predefined cause category “atrial fibrillation and atrial flutter.” Recent GBD-based AF/AFL analyses indicate that this category corresponds to the relevant International Classification of Diseases codes, including ICD-9 427.3–427.32 and ICD-10 I48–I48.92. Additional technical details regarding GBD case definitions and modeling procedures are available in the corresponding GBD methodological documentation.
Outcomes and metrics
The primary outcomes of interest were incidence, prevalence, deaths, and DALYs. For each outcome, we extracted absolute counts and, where available, rates per 100,000 population together with lower and upper uncertainty intervals. DALYs were used as a summary measure of health loss, consistent with the GBD framework. The rates reported in the main manuscript correspond to crude all-age rates per 100,000 population derived from the selected GBD extracts, unless otherwise specified. In addition, to address sex differences observed in absolute counts, we extracted age-standardized rates per 100,000 population by sex for 2023 from the IHME/GBD Results Tool, using the GBD world standard population.
Study strata
Analyses were performed at several levels. First, we summarized the global AF/AFL burden in 2023 using extracts restricted to the global region, both sexes, and all ages. Second, we assessed sex-specific burden using direct 2023 global extracts for male, female, and both-sex categories. Third, we evaluated age-specific burden using direct 2023 global extracts for quinquennial age groups. Fourth, we analyzed burden across the five standard SDI strata: high, high-middle, middle, low-middle, and low. This analytic structure was designed to examine AF/AFL burden by sex, age, and socio-demographic characteristics.
Temporal analyses
To characterize long-term patterns, we used author-generated GBD 2023 series exports covering the widest available historical ranges for the selected outcomes. Global temporal series were examined from 1990 onward for incidence and prevalence and from the longest available downloaded series for deaths and DALYs. For contextual comparison, selected historical burden estimates from earlier reference years were retained in the Supplementary Material, whereas the main analysis focused on the contemporary GBD 2023 dataset.
Analytical approach
The aim of the analysis was to describe the magnitude, distribution, and patterning of AF/AFL burden worldwide. We summarized 2023 global estimates, compared burden between men and women, identified the age groups with the highest burden for each outcome, and quantified gradients across SDI strata using both counts and rates. Because the purpose of the study was to provide a clinically interpretable global epidemiological analysis, emphasis was placed on descriptive burden assessment rather than on formal age–period–cohort modeling, joinpoint regression, attributable risk estimation, or long-term forecasting. These approaches were used in the recent Europace GBD 2023 study, which addressed a different research question focused on age-specific and income-stratified trends.
Data handling
The authors reviewed and consolidated all extracted CSV files into a final dataset for analysis and tabulation. When more than one extract was available for the same domain, values were taken from a single internally consistent set of downloads used for the final tables. Sex-specific burden estimates for incidence, prevalence, DALYs, and deaths were all based on direct 2023 IHME/GBD extracts.
Ethical considerations
The study relied exclusively on publicly available, de-identified, aggregate burden estimates obtained from the IHME GBD Results Tool; therefore, it did not require institutional ethics approval. This approach is consistent with the methodological approach to publicly accessible GBD-derived data used in prior AF/AFL burden reports.
Results
Global burden of AF/AFL in 2023
In 2023, AF/AFL accounted globally for 5,021,980 incident cases, 59,045,058 prevalent cases, 9,265,726 DALYs, and 377,258 deaths. The corresponding global rates per 100,000 population were 62.26 for incidence, 732.04 for prevalence, 114.88 for DALYs, and 4.68 for deaths. These data confirm that AF/AFL represents a substantial worldwide burden in contemporary populations (Table 1).
Global AF/AFL burden in 2023 (both sexes, all ages).
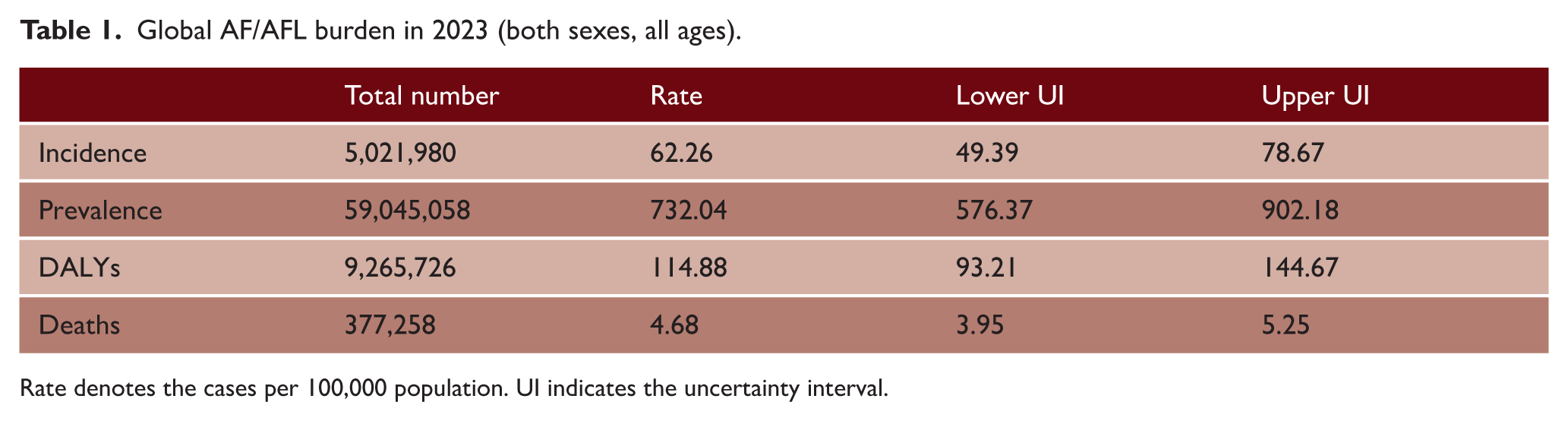
Rate denotes the cases per 100,000 population. UI indicates the uncertainty interval.
Temporal patterns in global burden
The global burden of AF/AFL increased markedly in absolute terms over time. Using the current GBD 2023 series, the worldwide burden rose from approximately 2.09 million incident cases, 23.36 million prevalent cases, 3.43 million DALYs, and 114,969 deaths in 1990 to substantially higher levels in 2023. For contextual comparison, selected historical values from earlier worldwide reports are shown in Supplementary Table S2.
Sex-specific burden
Sex differences remained clinically relevant in 2023. Men accounted for more incident and prevalent AF/AFL cases than women, with 2,645,944 (52.7%) incident cases and 32,000,021 (54.2%) prevalent cases in men compared with 2,376,036 incident cases and 27,045,037 prevalent cases in women. In contrast, women accounted for more fatal and disability-related burden in absolute terms, with 4,770,942 (51.5%) DALYs and 229,482 (60.8%) deaths, compared with 4,494,784 DALYs and 147,776 deaths in men. However, age-standardized rates refined this pattern: men retained higher incidence, prevalence, and DALY rates than women (61.83 vs. 48.16, 776.33 vs. 541.85, and 114.42 vs. 94.38 per 100,000, respectively), whereas age-standardized death rates were essentially equivalent between sexes (4.42 in women vs. 4.34 in men per 100,000), with widely overlapping 95% uncertainty intervals. These findings suggest that the greater female burden of DALYs in absolute terms is largely explained by the older age structure of women globally. In contrast, the absolute female excess in deaths reflects predominantly the same age-structure effect. Of note, the parity in age-standardized mortality despite considerably higher male incidence and prevalence indicates that, on a per-case basis, the mortality impact of AF/AFL is at least as high in women as in men (Table 2).
Sex-specific global AF/AFL burden in 2023.
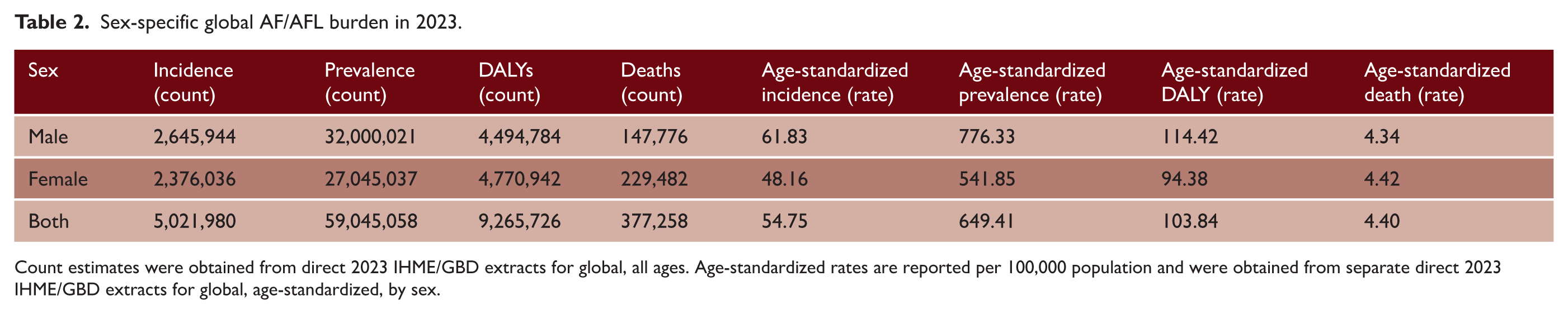
Count estimates were obtained from direct 2023 IHME/GBD extracts for global, all ages. Age-standardized rates are reported per 100,000 population and were obtained from separate direct 2023 IHME/GBD extracts for global, age-standardized, by sex.
Age-specific burden
The burden of AF/AFL was substantially higher in older adults. Within the quinquennial age categories examined, the highest observed counts of both incident and prevalent cases were found in the 70- to 74-year age group, with 851,122 incident cases and 9,698,152 prevalent cases. The highest DALY counts were observed in the 80- to 84-year age group, reaching 1,472,608, while the highest death counts were observed in the 85- to 89-year age group, with 89,150 deaths. These findings indicate that although AF/AFL incidence and prevalence are already substantial in the early elderly population, the heaviest fatal and disability-related consequences are concentrated at more advanced ages (Table 3 and Figure 1).
Age groups with the highest AF/AFL burden in 2023 (both sexes).
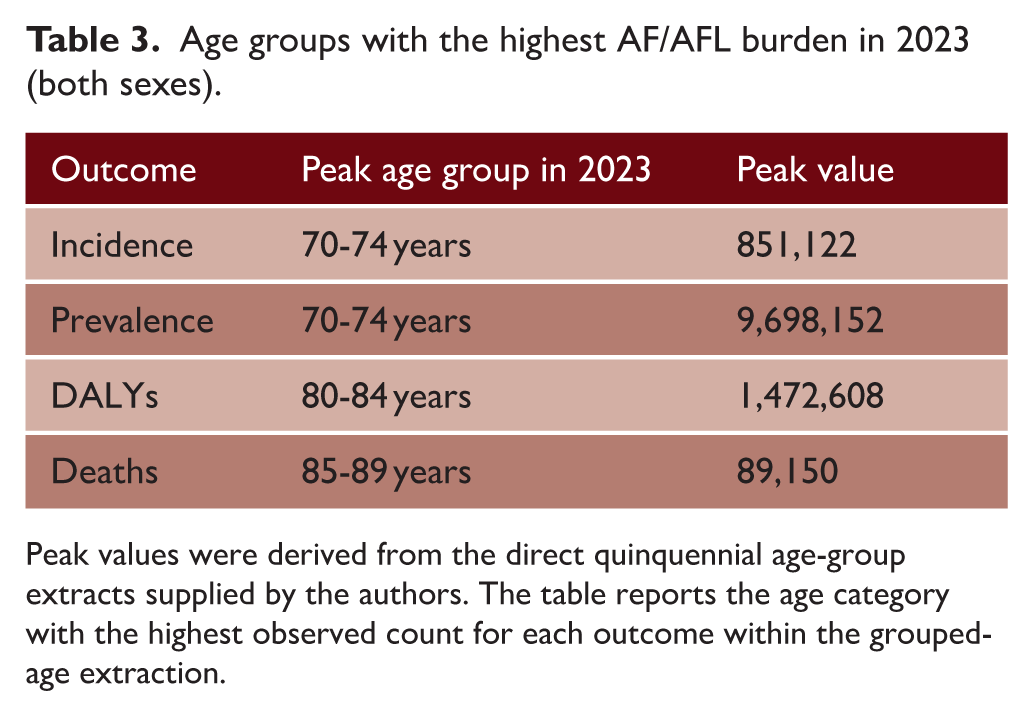
Peak values were derived from the direct quinquennial age-group extracts supplied by the authors. The table reports the age category with the highest observed count for each outcome within the grouped-age extraction.
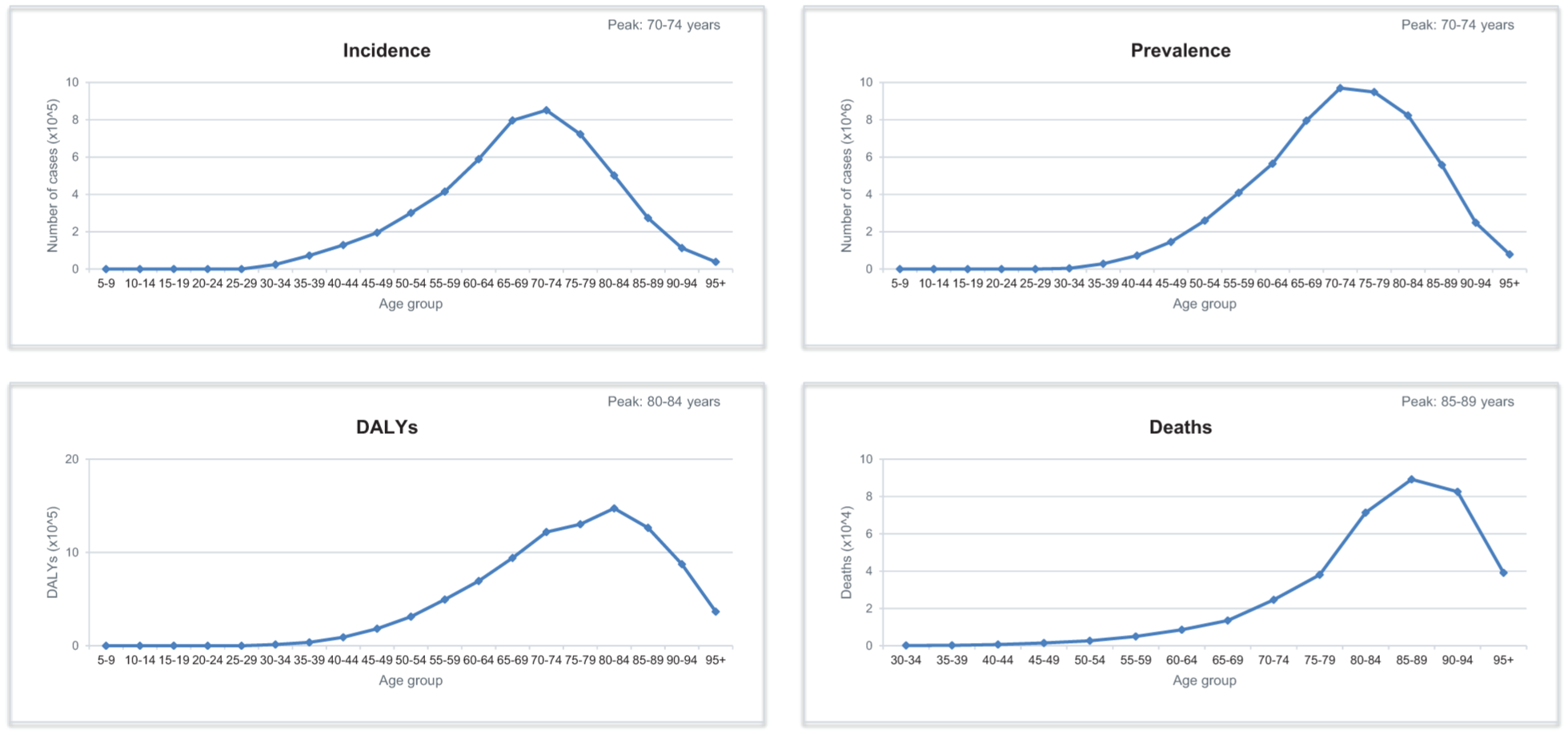
Age-group distribution of global AF/AFL burden in 2023. Distribution of incident cases, prevalent cases, disability-adjusted life years (DALYs), and deaths due to atrial fibrillation and atrial flutter across the quinquennial age groups extracted from the IHME/GBD 2023 Results Tool (Global, both sexes).
Socio-demographic gradients
Marked gradients were observed across the SDI strata. High-SDI settings carried the greatest absolute burden across all major metrics, with 2,692,607 incident cases, 33,178,730 prevalent cases, 5,245,463 DALYs, and 230,354 deaths in 2023. The burden decreased progressively across the remaining SDI strata. High-middle SDI settings accounted for 1,027,941 incident cases, 11,854,640 prevalent cases, 1,762,262 DALYs, and 65,649 deaths, whereas low-SDI settings accounted for 396,934 incident cases, 4,187,064 prevalent cases, 736,841 DALYs, and 27,679 deaths (Table 4).
AF/AFL burden in 2023 by socio-demographic index (counts).
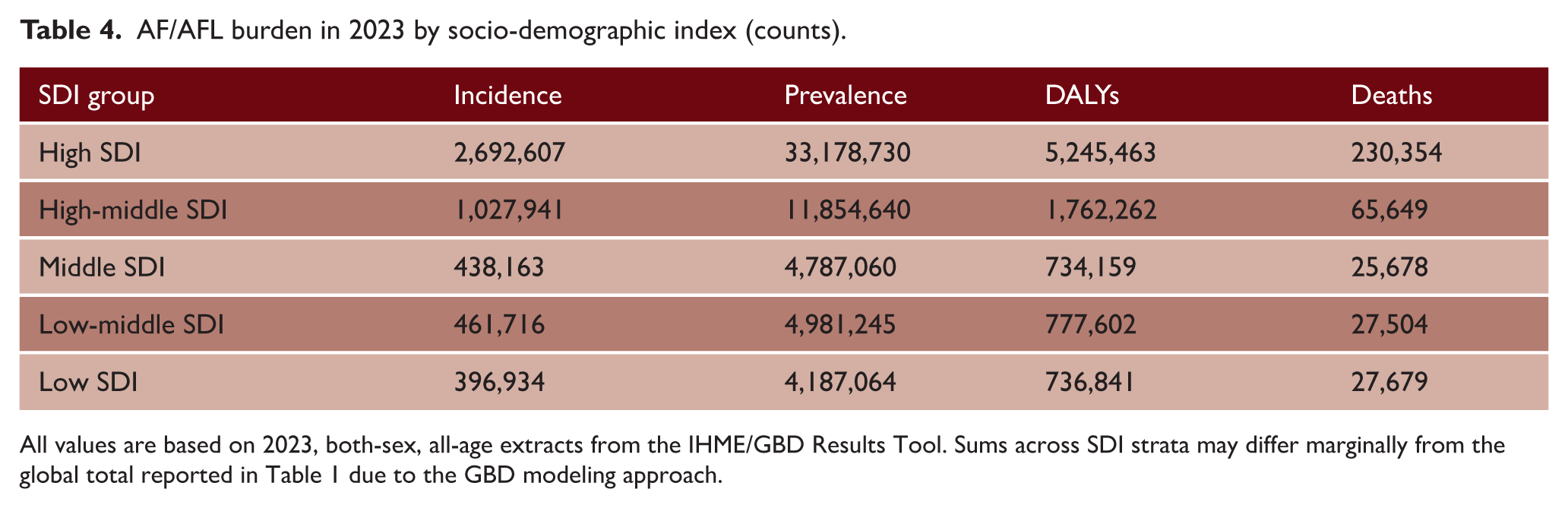
All values are based on 2023, both-sex, all-age extracts from the IHME/GBD Results Tool. Sums across SDI strata may differ marginally from the global total reported in Table 1 due to the GBD modeling approach.
A similar pattern was evident for rates. High-SDI settings showed the highest incidence, prevalence, DALY, and death rates, at 105.94, 1305.46, 206.39, and 9.06 per 100,000 population, respectively. By contrast, the corresponding rates in low-SDI settings were 22.93, 241.91, 42.57, and 1.60 per 100,000 population. Overall, these findings indicate that AF/AFL is a global condition, but its greatest measured burden remains substantially higher in the most socio-demographically developed settings (Table 5).
AF/AFL burden in 2023 by socio-demographic index (rates per 100,000).
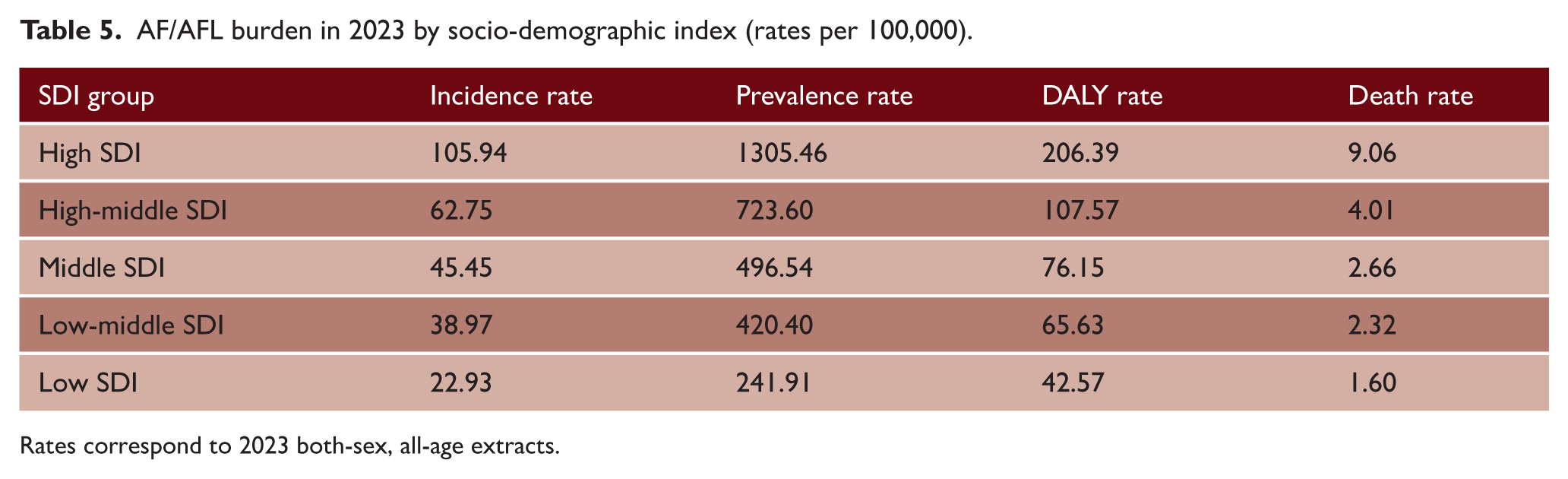
Rates correspond to 2023 both-sex, all-age extracts.
Interpretation of absolute versus rate-based burden
Taken together, the findings show that the contemporary burden of AF/AFL cannot be reduced to a simple increase in counts. The absolute burden has risen sharply over the period covered by GBD 2023, but the current distribution also reflects substantial heterogeneity by age, sex, and socio-demographic development. In particular, the substantially higher burden of incident and prevalent cases among adults aged 70–74 years, the shift of DALY and mortality peaks toward older age groups, the persistence of sex-specific differences, and the high burden observed in high-SDI settings all point to a more complex epidemiological picture than crude global growth alone would suggest. These results should be interpreted in the context of population aging and improved survival, while broader ascertainment through electrocardiographic, wearable, and digital detection remains a plausible but untested contributor in the present dataset.2,4,7
Discussion
Several findings warrant emphasis. First, the global burden of AF/AFL has continued to rise markedly in absolute terms. Second, the burden remains substantially higher in older adults, particularly for deaths and DALYs. Third, AF/AFL shows clear socio-demographic patterning, with the largest measured burden concentrated in high-SDI settings. Together, these observations reinforce that AF/AFL remains a major global public health challenge rather than a narrowly specialist arrhythmia problem.1,2,7
The current estimates also suggest that the contemporary epidemiological interpretation of AF/AFL is more complex than simple numeric growth alone. The rising absolute burden should not be automatically interpreted as a uniform increase in disease frequency across all ages. Population aging and improved CVD survival likely contribute importantly to the observed expansion. Broader ascertainment through opportunistic electrocardiographic recording, handheld devices, patch monitoring, implanted devices, and consumer-facing wearables may represent an additional contributing factor, although ascertainment mode was not directly assessed in the present study.2,4 Thus, the modern epidemiology of AF/AFL reflects both underlying biology and changing surveillance intensity.
The age distribution is especially noticeable. Within the quinquennial age categories examined, the highest counts of incident and prevalent AF/AFL cases were observed in the 70- to 74-year age group, whereas the highest DALY and death counts were observed in older age strata. This pattern suggests that AF/AFL is not only common in later life but also becomes progressively more consequential as patients age and accumulate frailty, multimorbidity, and competing CVD risk. This interpretation is supported by recent GBD-based work focusing specifically on older adults, which confirmed that AF remains a major public health concern in people aged 60–89 years and that incident cases, deaths, and DALYs increased globally between 1990 and 2019. 8 This distinction has practical clinical relevance. A rise in prevalence may reflect not only new disease occurrence but also greater longevity with AF/AFL and more prolonged exposure to complications such as stroke and HF.2,9 From a stroke perspective, this pattern suggests that an increasing proportion of future cardioembolic stroke burden may occur in patients with long-standing AF/AFL, advanced age, and accumulated multimorbidity. Contemporary United States (US) data reinforce this age gradient, with AF prevalence increasing from 0.26% in adults younger than 50 years to 24.58% in those aged 90 years or older. 10 These observations are consistent with the broader understanding that age is one of the strongest determinants of AF burden and its downstream consequences.2,9
The persistence of sex differences also deserves attention. In 2023, men accounted for more incident and prevalent AF/AFL cases in absolute terms, whereas women accounted for more deaths and DALYs. To clarify the contribution of age structure to this pattern, we examined age-standardized rates. Men retained higher age-standardized incidence, prevalence, and DALY rates than women, indicating that the greater absolute female burden of DALYs largely reflects the older age structure of women in the global population. In contrast, age-standardized mortality rates were essentially equivalent between sexes (4.34 in men vs. 4.42 in women per 100,000), despite men presenting considerably higher age-standardized incidence and prevalence. This parity in age-standardized mortality suggests that, on a per-case basis, female AF/AFL is associated with at least comparable mortality risk to male AF/AFL. This pattern is consistent with sex-related differences in frailty, comorbidity burden, anticoagulation patterns, stroke vulnerability, and post-stroke outcomes.7,9 A contemporary US cohort similarly showed higher AF prevalence in men than in women (4.87% vs. 3.11%). 10 From a stroke perspective, the greater absolute mortality and disability burden in women, together with the comparable age-standardized mortality despite lower female incidence, support a neurological interpretation of this gradient. Recent Advancing Knowledge in Ischemic Stroke Patients on Oral Anticoagulants Retrospective (ASPERA-R) cohort data further reinforce this view, showing worse 90-day outcomes and higher ischemic recurrence in women after breakthrough ischemic stroke on oral anticoagulation for AF. 11 Although the present analysis was not designed to identify the mechanisms underlying these differences, the sex gradient was sufficiently pronounced to support its continued inclusion in epidemiological and clinical reporting.
The SDI findings provide further insight into the global burden of AF/AFL. High-SDI settings carried the greatest absolute burden and the highest rates, likely reflecting a combination of older population structures, better survival, more intensive diagnosis, and greater data completeness.2,7 From a cerebrovascular perspective, these patterns may also reflect better survival after stroke and other cardiovascular events in high-SDI settings, allowing accumulation of chronic AF/AFL populations at ongoing risk of recurrent cardioembolic complications. Accordingly, the observed SDI gradient may reflect not only differences in AF/AFL occurrence and detection but also differences in survival, continuity of care, and recurrent cerebrovascular risk. At the same time, AF/AFL was measurable across every SDI stratum, underscoring that it is now a genuinely global condition. These findings also point to important health-system implications. In lower-resource settings, under-recognition of disease may coexist with limited access to long-term anticoagulation, rhythm evaluation, and chronic CVD follow-up, potentially amplifying preventable disability and mortality.2,4,7
An additional point of interest is the comparison between the present 2023 estimates and previously published future projections. In an earlier linear extrapolation based on historical trends, AF/AFL was projected to reach 4.950 million incident cases, 62.510 million prevalent cases, 10.080 million DALYs, and 427.000 deaths by 2050. 9 By contrast, the current 2023 estimates already show 5.022 million incident cases, 59.045 million prevalent cases, 9.266 million DALYs, and 377,258 deaths worldwide. Thus, incident cases have already slightly exceeded, and prevalent cases have nearly reached the earlier theoretical 2050 projections, while DALYs and deaths have also approached them substantially. These comparisons suggest that the contemporary expansion of AF/AFL burden may have progressed faster than previously anticipated, especially in case occurrence and accumulation (Supplementary Figure S1). By comparison, more recent projection studies based on GBD 2023 have mainly forecast future age-standardized rates rather than absolute global counts, reporting modest declines in age-standardized prevalence, stable age-standardized incidence, and increasing age-standardized mortality and DALY rates through 2048. 1 Therefore, direct numerical comparison with the absolute burden reported here should be interpreted cautiously.
Another recent projection study based on GBD 2019 also supports the expectation that the global burden of AF/AFL will continue to rise over the coming decades. Using Nordpred and Bayesian age–period–cohort models, Ma et al. 12 projected continued increases through 2044, including approximately 0.78–0.83 million deaths and 17.31–17.58 million DALYs worldwide. In comparison, the present 2023 estimates already show 377,258 deaths and 9,265,726 DALYs, indicating that although the future projected burden remains higher than the current one, a substantial proportion of that anticipated burden has already been reached. Direct comparison should nevertheless be interpreted with caution, as the study was based on GBD 2019, whereas the present analysis uses GBD 2023; differences between database releases may affect absolute estimates, particularly for prevalence.
The clinical and public health implications are straightforward. AF/AFL should be viewed not only as an arrhythmia but also as a systems-level chronic disease challenge closely linked to aging, multimorbidity, stroke prevention, and healthcare delivery.1,2,4 Given the central role of AF/AFL in cardioembolic stroke, the observed age, sex, and SDI patterns are likely to have direct implications for the future distribution of stroke burden worldwide. Prevention strategies should remain centered on modifiable cardiometabolic risk factors, while the growing role of digital detection means that future epidemiological interpretation will increasingly depend on how, where, and in whom AF/AFL is sought.2,4 At the same time, sex-aware and stroke-aware management strategies may become increasingly important, particularly in older women and other high-risk groups. In that sense, the contemporary epidemiology of AF/AFL is shaped by both biology and surveillance.
This study has limitations. First, it relies on descriptive use of model-based GBD estimates, which are necessarily dependent on the quality and completeness of the underlying data sources and modeling assumptions. 6 Second, different IHME queries may yield small numerical differences according to the combination of measure, metric, year range, and strata selected for download; to minimize inconsistency, the manuscript relies on a single internally consistent set of author-generated extracts for the final tables. 6 Third, the present analysis is descriptive and does not include age–period–cohort modeling, forecasting, or risk-attribution analysis. This limits mechanistic inference, but it does not diminish the value of a clinically interpretable global burden analysis focused on magnitude, distribution, and public health relevance. 6
Conclusion
AF/AFL remains a major and growing global public health challenge. In 2023, the worldwide burden was substantial and continued to be substantially higher in older adults, with the greatest mortality- and disability-related burden occurring at advanced ages. Men accounted for more incident and prevalent cases in absolute terms, whereas women accounted for more deaths and DALYs; age-standardized rates indicated higher male incidence, prevalence, and DALYs but essentially equivalent mortality between sexes, while high-SDI settings carried both the greatest absolute burden and the highest rates. These findings underscore that the contemporary epidemiology of AF/AFL must be interpreted not only in terms of rising case counts but also in light of population aging, improved CVD survival, and broader contemporary detection pathways. AF/AFL should hence be regarded as both a clinical arrhythmia syndrome and a system-level chronic disease challenge with major implications for stroke prevention, long-term CVD care, and health-system planning worldwide. Future trends in obesity, cardiometabolic abnormalities, physical inactivity, and alcohol consumption are likely to influence the trajectory of this epidemic.
Supplemental Material
sj-docx-1-wso-10.1177_17474930261464877 – Supplemental material for Global epidemiology of atrial fibrillation and atrial flutter: An increasing worldwide burden
Supplemental material, sj-docx-1-wso-10.1177_17474930261464877 for Global epidemiology of atrial fibrillation and atrial flutter: An increasing worldwide burden by Fabian Sanchis-Gomar, Carl J Lavie and Giuseppe Lippi in International Journal of Stroke
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability
Public underlying estimates are accessible through the IHME GBD Results Tool.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.