
Abstract
Extant research indicates that collegiate coaches often lack the knowledge or confidence required to provide their student–athletes with effective educational experiences related to eating disorders. The current study investigates the prevalence and quality of such experiences from the perspective of lean and non-lean female student–athletes at a National Collegiate Athletic Association Division III institution. Participants were asked closed- and open-ended questions in an anonymous online survey. Lean and non-lean participants reported similar rates of education despite differential risk for eating disorders. Approximately 70% of student–athletes expressed a desire for a more comprehensive and long-term program of study. Participants’ confidence in identifying an eating disorder in a peer did not differ based on type of sport or education status, but those who were educated identified more appropriate potential symptoms than did those who were uneducated. This indicates some degree of educational effectiveness. However, education status and type of sport had no bearing on the likelihood of a participant speaking with their coach about their own or a peer’s potential disorder. Educational attempts were therefore insufficient to help student–athletes overcome the shame and consequential secrecy associated with eating disorders. Our results underscore the need for effective education for at-risk student–athletes while also clarifying that both lean and non-lean student–athletes often want to receive more comprehensive education about eating disorders. Current findings highlight specific areas of student–athlete interest about the topic and could be used to help coaches revise their educational efforts to enhance engagement and long-term retention of information.
How do female collegiate athletes view their education about eating disorders?
Approximately 13.5% of female college students experience an eating disorder. 1 Participating in athletics places them at a higher risk due to pressure to conform to expressed or perceived expectations pertaining to their weight, shape, and size.2,3 Coaching staff can act as a first line of defense against these pressures. 4 Unfortunately, they are often ill-equipped to handle the complex duties associated with the prevention of and recovery from eating disorders due either to a lack of relevant knowledge or a lack of confidence in passing that knowledge to student–athletes.5–7 The current study offers an examination of female collegiate athletes’ perspectives on the quality of eating disorder education provided by their coaches including whether it was provided, its content, and desired curricular changes.
Women are at risk for eating disorders largely due to external societal pressure to conform to an unrealistic standard of attractiveness centered on thinness. 8 Participation in athletics can place additional pressures on individuals to maintain a body type that is generally viewed as appropriate for their sport. 4 Specifically, weight-related pressures are strongest when sports: (a) base scores at least partially on aesthetics or involve revealing uniforms, (b) require maintaining a certain weight, and/or (c) emphasize thinness as a performance advantage. 9 Participation in lean sports that emphasize thinness (e.g., running) is usually associated with reduced body satisfaction, lower desired body weight, and, ultimately, more eating disorders when compared to participation in non-lean sports.10,11 However, some research indicates that both lean and non-lean athletes are at risk for eating disorders due to engaging in unhealthy eating behaviors geared toward weight control.12,13 It is therefore important to educate all athletes about the risks associated with eating disorders and monitor them for associated symptoms so that high-risk athletes can be more easily identified and directed to appropriate professionals.
Given the many circumstantial stressors experienced by athletes, many seek positive feedback from others who they see as important and knowledgeable in order to maintain their self-confidence and self-esteem. 14 Coaches are often the most important of these evaluators because they tend to be viewed as authorities who share their knowledge with eager athletes who try to enhance their sporting performance to both fulfill their own athletic goals and please their coaches. 15 Some ways athletes do this include making personal sacrifices such as setting aside large amounts of time for physical training or modifying their diet in order to maintain a desired body shape—the latter of which can be perceived as advantageous in terms of both performance potential and appearance. 16 Given their close working relationship, coaches are in an excellent position to inform athletes about some of the negative side effects of eating disorders such as fatigue, anemia, and depression. 17 Unfortunately, coaches sometimes perceive the risk of eating disorders as lower than it is—particularly when working with lean athletes. 18 Coaches may also lack confidence in their knowledge of early warning signs that could signal the need for interventions. 6
Assessments of coaches’ knowledge about eating disorders typically reveal that their lack of confidence is appropriate. For example, one study found that nearly 20% of their sample of NCAA coaches had never identified an eating disorder within their teams. 19 Another found that only 17% of their sample of coaches from NCAA division I and II schools had ever attended an educational program about eating disorders. 5 As would be expected given their lack of training, a test of eating disorder etiology, identification, management and treatment, risk factors, and prevention and education revealed average accuracy across all coaches that was only marginally above chance. 5 Of greater concern, coaches were similarly confident in both correct and incorrect responses. Coaches therefore often appear to be ill-informed about the subject matter without being aware of it. 20 They need further training about eating disorders and athlete education so knowledge can be passed on in an open and supportive environment. Encouraging an open dialogue may allow a stronger bond to form between coaches and their athletes that might facilitate earlier interventions for maladaptive behaviors. 21
Effective education is a key component of eating disorder prevention and management, and numerous studies examined coaches’ effectiveness in this regard in terms of both their objective knowledge and related confidence.5,6,18,20,22,23 However, no study has yet examined these educational experiences from the perspective of the largest stakeholders in this research: student–athletes. It may be assumed that, given the sensitivity of this topic, student–athletes generally wish to avoid discussing it altogether. 24 However, even if this is accurate, they need to be educated about eating disorder symptoms, prevention, and recovery to decrease their risk of developing one. Education could also increase their chances of detecting that a peer athlete needs help, which is not an expectation that should be placed on a student–athlete by coaches but could offer another chance for intervention.
As a step in that direction, it is important to assess the quality of the education about eating disorders that they receive in the context of their sport(s). Such assessments could include (a) whether educational attempts are made by important authorities (e.g., coaches), (b) the quality of those experiences (e.g., in terms of included content and the competence with which it is related), (c) the learning outcomes associated with these educational opportunities, and (d) what other information student–athletes want to learn (e.g., how to gain and lose weight safely or how to talk to a teammate who may have an eating disorder). Although points (a) through (c) may seem obvious, point (d) is also important because it could be used to create educational interventions targeting each area of student–athlete interest. Student–athletes may be more receptive to curricula that are tailored at least somewhat to their interests, and this might increase their odds of preventing or seeking treatment for their own or a peer’s disorder.
In the current study, female collegiate athletes at an NCAA Division III institution completed an anonymous survey assessing characteristics and outcomes of educational efforts made by coaching staff regarding eating disorders. Measures were compared based upon student–athlete Sport Type (lean or non-lean) and Education (whether participants reported receiving an educational experience pertaining to eating disorders). Based on prior research, we hypothesized that overall body satisfaction would be higher for non-lean than lean student–athletes, given the pressures exerted on the latter to be thin. Second, as a validation of our Sport Type categorization, lean student–athletes were expected to report more pressure to maintain a specific weight for their sport (perhaps based on cues perceived from coach or teammate or resulting from a self-determined goal—our question did not specify a specific source) and perceive an overall higher risk of eating disorders for competitors in their sport than would non-lean student–athletes. Third, lean participants should report more frequent education than non-lean participants due to their differential risk. Educated participants were also anticipated to express dissatisfaction with their experiences (given typical coaching deficiencies mentioned previously) by reporting a greater desire for expansion than uneducated participants who may lack awareness of the topic’s complexity. Fourth, student–athletes were hypothesized to report similar subjective confidence in their ability to identify an eating disorder in a peer regardless of Sport Type or Education. Consistent with coaching research, student–athletes were expected to be unable to differentiate between accurate and inaccurate (or absent) knowledge about eating disorders when asked if they could detect one in a peer, but educated participants were expected to spontaneously report more appropriate symptoms than uneducated participants, reflecting greater objective knowledge. Fifth, educated student–athletes were expected to be more comfortable talking to a coach about eating disorders in a team setting as well as one-on-one about their or a teammate’s possible disorder.
Method
Design
This study was a 2 (Sport Type: Lean, Non-lean) × 2 (Education: Educated, Uneducated) between-subjects quasi-experimental design. Sport Type was determined by participant self-report, as described below. Educational status was determined by asking participants “has your coach attempted to educate your team on eating disorders and/or healthy eating behaviors?” This self-report measure offered more consistency than would be likely given alternative options involving the evaluation of open-ended responses related to the content of their self-reported experiences (i.e., participants’ classification could have been based on the number of responses provided, the quality of those responses, or some combination of the two).
Participants
A convenience sample of 103 female student–athletes at the University of Wisconsin—Eau Claire (UWEC) completed our survey. The participants’ average age was 19.85 years (SD = 1.26). Twenty-six participants were first-year students, 39 were sophomores, 17 were juniors, 19 were seniors, 1 was a super-senior, and 1 did not report this data. Thirty reported being active in collegiate sports for one year, 27 for two, 15 for three, and 30 for four or more years. Although only 19 reported being seniors, it is possible for 30 to have four or more years of collegiate experience because this university’s class standing is based on course credits earned, not time spent at the institution.
Our sample included 48 women in lean sports and 55 in non-lean sports. Student–athletes were categorized as lean or non-lean based on descriptions provided by Torstveit, Rosenvinge, and Sundgot-Borgen. 25 Lean sports are those “in which leanness and/or a specific body weight were considered important for performance (e.g., endurance, aesthetic, weight class, and anti-gravitation sports),” and non-lean sports are those for which “leanness was considered less important for performance (e.g., technical, ball game, and power sports)” (p. 111). 25 The lean sports represented in our sample included cross country (n = 1), gymnastics (n = 4), swim and dive (n = 5), track and field (n = 18), and volleyball (n = 6). These sports all either emphasize thinness as beneficial to performance or involve revealing team uniforms. Non-lean sports included tennis (n = 1), soccer (n = 6), golf (n = 2), hockey (n = 21), and softball (n = 25). These sports are either ball sports or do not involve revealing uniforms. Thirteen participants reported competing in both cross country and track and field (both lean sports). One reported competing in tennis (non-lean) and volleyball (lean) and was categorized as lean. Ten lean and 10 non-lean student–athletes endorsed two or more items on the SCOFF.
Procedure
Our survey was administered using Qualtrics online survey software. 26 It was distributed in two ways. First, an anonymized link to the survey was posted along with a brief request to participate in our study on each athletic team’s Facebook page. The posts specifically mentioned that participation was completely anonymous and there was no intention of linking responses to any person’s identity (which was accurate). Second, to ensure we gave every student–athlete an opportunity to participate (e.g., if they did not use Facebook) coaches were emailed the same information and asked to forward it to their team’s mailing list. Coaches were asked specifically to only mention this opportunity to participate and not to place any pressure on their team members to do so because (a) that would be highly unethical and (b) the quality of any resulting data would be suspect. If a student–athlete clicked the survey link in either the Facebook posting or coach email, they were directed to our informed consent materials which consisted of (a) reading a cover letter detailing what the study would ask about and (b) signing off (electronically) that they agreed to participate, given the benefits and risks involved (e.g., a risk of psychological upset due to questions about their eating behaviors).
After obtaining informed consent and responding to demographic measures participants answered open- and closed-ended questions related to their ability to recognize the signs of an eating disorder in a peer athlete, their comfort level talking to coaching staff about their own or a teammate’s possible eating disorder, and the educational efforts of coaching staff related to eating disorders (see the Appendix for specific questions). Finally, all participants were debriefed and thanked for their participation. The debriefing process involved reading a statement summarizing the point of the research (to assess the quality of eating disorder education in vulnerable populations) and highlighting that if they suspected that they or other persons they know might be suffering from an eating disorder that there are free and confidential resources available to them such as the university’s counseling center.
Measures
The survey included questions from a previously validated measure meant to detect a person’s risk for eating disorders and questions we generated to address the role of coaches in the prevention, development, and recovery from eating disorders. The SCOFF questionnaire is a general screening tool for eating disorders and was chosen to minimize the completion time for the survey while maintaining both validity and reliability of measurement. 27 The SCOFF involves answering five yes/no questions pertaining to their eating behaviors and beliefs; the endorsement of two or more items is indicative of either anorexia nervosa or bulimia nervosa. This threshold allows for 100% sensitivity for both eating disorders for persons identified as meeting Diagnostic and Statistical Manual of Mental Disorders–Fourth Edition (DSM-IV) criteria for either disorder based on a clinical interview at a specialist eating disorder clinic. 28 Additionally, its specificity at this threshold is approximately 87.5% (i.e., it has an approximately 12.5% false positive rate). It compares favorably to diagnoses based on clinical interviews, and high agreement exists between written and verbal administrations (κ > 0.82).
We also created a list of closed- and open-ended qualitative questions about the educational efforts of coaching staff related to eating disorders and nutrition, participants’ ability to recognize the signs of an eating disorder in a peer athlete, and their comfort level talking to others about their own or a teammate’s eating disorders. Questions were created through a collaboration with student–athletes (the coauthors of this study) and the first author. Prior to the finalization of the question list, every coach and athletic trainer at our university was contacted with a request for a brief informal interview to discuss how they approached discussions of eating disorders and nutrition with their student–athletes to get an idea of how much variability existed on campus at that time.
Six coaches of the dozens contacted responded to our request, but they provided insight into the variability in their approaches to the subject. Some, for example, discussed bringing in a nutritionist and monitoring their student–athletes carefully (e.g., a running coach), whereas others expressed interest in the topic of eating disorders but did not currently address it at all with their athletes (e.g., a basketball coach). Although we initially planned for these data to be part of the current study (we were going to send a variation of the final survey to coaches in addition to student–athletes), this was not feasible due to the small number of staff who participated in our initial interviews. Only one nonparticipating coach responded to us indicating a lack of availability, and the rest either did not receive or ignored our requests. It therefore seemed inappropriate to base any conclusions on the few coaches who might have completed the survey. The initial interviews aided the construction of our questionnaire, however, by highlighting the variability in educational experiences offered by coaching staff. Open-ended questions were written very broadly to avoid narrowing the possible range of responses (and to avoid unwarranted assumptions such as “all student-athletes receive an education of some kind about eating disorders”). Ideally, the current student–athlete data will help administrative and coaching staff see more value in their participation in research of this kind in the future.
Written responses to open-ended questions were coded by the first author and a graduate student who was unaffiliated with this project. The graduate student was familiarized with the question list and both raters independently coded the data according to standards associated with thematic analysis. 29 First, coders familiarized themselves with the data set as a whole to gather an initial impression of presented semantic themes and create response categories based on those themes. After coders agreed on the initial list of coding categories, approximately 5% of responses were selected at random and processed using that list. Similar codes were collapsed together during a subsequent discussion of findings to generate the final coding scheme for each question. All data were then coded based on that final scheme, and each participant could potentially be represented in multiple response categories depending upon the complexity of a given response. Very high interrater reliability was achieved for the final coding scheme such that coders agreed on 99.02% of cases overall, and disagreements were resolved via discussion prior to analyzing the data. Response categories are reported below only when given by at least 10% of our sample.
Results
The following results are inclusive of specific hypothesis tests and exploratory analyses intended to provide further context for our findings. Lean (63%) and non-lean (51%) participants reported similar rates of education about eating disorders or healthy eating by their coaches, χ2(1) = 1.10, p = .294, ϕ = .11. Educated participants (57% of our overall sample) reported receiving the following information as part of their education: (a) the need to stay healthy to perform well (30% of the educated), (b) presentations on basic nutrition either led by a coach (25%) or dietician/nutritionist (16%), (c) how to navigate the on-campus cafeteria (23%), (d) a coach-led presentation specifically on eating disorders, including common symptoms (14%), and (e) readings about nutrition (11%).
As one might glean from the varied response rates, large experiential disparities existed within the educated. For example, one participant stated that their coach facilitated “[a] discussion with [an] alum who is a nutritionist” and that the coach “also works with people personally when they think they are having a problem with proper nutrition.” In contrast, another stated that they only received “a packet listing healthy food options.” Lastly, some reported being educated but implied with their wording that it was inadequate. For example, “there is always a talk about nutrition but that is the end of the discussion and then it’s never brought up again.”
Educated participants suggested that coaches also: (a) talk about the qualities of eating disorders (not just general nutrition), including their prevalence, and do so more than once at the beginning of the year (41% of the educated), (b) offer to talk to student–athletes individually and emphasize that they care and want to provide help (13%), and (c) talk about the negative effects of eating disorders like poor athletic performance (11%). Thirty percent of educated participants stated that no improvements were necessary either without further elaboration or because of a feeling that, as one participant said, “I think they did an all-around great job on educating us on weight loss and management. I cannot think of any ways they could’ve done more or done better.” Others expressed thoughts such as “all you really need [are] the basics on what an eating disorder is and how to look out for them in your teammates” or “it’s not a health class; I don’t think they should have to [do more].”
Uneducated participants made up 43% of our sample. Thirty-six percent of the uneducated suggested that coaches cover point (a), and 19% wanted coaches to discuss how to gain and/or lose weight safely. Additionally, 11% stated plainly that no changes were necessary, and 17% noted that eating disorders have never been an issue on their team or that the topic had never come up before. For example, many expressed views such as “I don't think they're that prevalent in our sport, so there's never really a need to discuss them. Maybe just say something about them at our team meetings.” One also elaborated that “I don’t think [eating disorders and nutrition have] anything to do with the coaches.”
Sixty-seven percent of participants reported being able to identify an eating disorder in a peer athlete regardless of Sport Type or Education, ps > .60. Overall, participants said they would look for: (a) inadequate food consumption (educated: 70%; uneducated: 74%), (b) physical symptoms like paleness, weakness, fatigue, and looking ill (educated: 37%; uneducated: 21%), (c) gaining or losing weight very quickly (educated: 26%; uneducated: 34%), (d) throwing up often and/or going to the bathroom after meals (educated: 37%; uneducated: 18%), (e) disturbed mood (e.g., irritability or depression; educated: 20%; uneducated: 13%), (g) being very cautious about food intake (educated: 13%; uneducated: 18%), and (h) obsessing about their weight (uneducated: 21%; educated: 26%). Educated participants also cited: (a) obsessing about food (17%), (b) binge eating (15%), and (c) working out too much (13%).
Hypotheses pertaining to discussions with coaching staff were unsupported. Fifty-three percent of participants reported feeling comfortable talking to a coach about eating disorders in a team setting (e.g., by asking general questions) regardless of Sport Type or Education, ps > .60. This foreshadowed the reluctance of many participants to discuss such matters with a coach. Although a trend existed such that educated participants (84%) were more likely than uneducated participants (70%) to speak with their coach if they suspected a teammate of having an eating disorder, χ2(1) = 2.82, p = .093, ϕ = .17.
Overall, 24% of participants would not report an at-risk teammate due to: (a) a desire to avoid violating the privacy of the other person (42% of those who would not report a teammate), (b) their coach not being the right person talk to (e.g., they might not handle it delicately or the coach is a man rather than a woman; 32%), (c) a fear of being wrong (32%), and (d) a desire to talk to the person themselves without involving the coach (21%). Many participants stated something like “[I would not do so] because I would not know how to word it, it is not my business, and I wouldn’t want people to do the same if I had an eating disorder.” Regarding the roles a coach plays, one student–athlete also stated “It’s none of my coach’s business if myself or my teammates experience that. It wouldn't do anything to tell him because he can’t do anything about it.” Another simply said, “[the teammate] can figure it out themselves.”
Similarly, their willingness to talk to a coach about their own possible disorder did not vary based on Sport Type or Education (67% overall would not do so; n = 34; ps > .200). These participants cited: (a) privacy (50%), (b) embarrassment, shame, and fear of judgment (42%), (c) a lack of closeness to the coach and a preference to talk to someone else (13%), and (d) a fear they could no longer participate in their sport (13%). One response captured several common sentiments: “I don’t know … I might feel shameful for letting my issues get so bad that I would turn to an eating disorder to fix it. Or I might not want to be kicked off the team for turning to an eating disorder.” Another common theme was captured by “Not close enough to the coaches or trainers. Would talk to friends or family!”
Participants’ confidence in identifying eating disorders was unassociated with their willingness to discuss eating disorders with their coach in a team setting or discuss their own possible eating disorder with their coach in private (ps > .11). However, their confidence was associated with their willingness to discuss a peer’s possible eating disorder with their coach, χ2(1) = 4.33, p = .038, ϕ = .25. While 81% of confident participants were willing to do so, this was true of only 58% of the unconfident. Participants’ SCOFF scores were unassociated with their willingness to have either discussion, ps > .17.
Chi-square tests related to self-perceptions of weight-related issues.
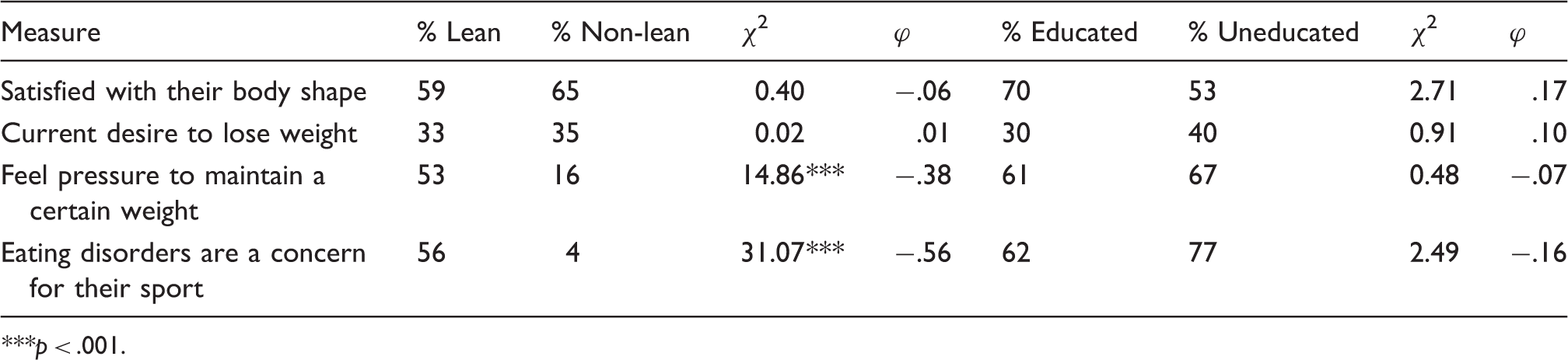
***p < .001.
Means and standard deviations of group comparisons and associated t-tests.
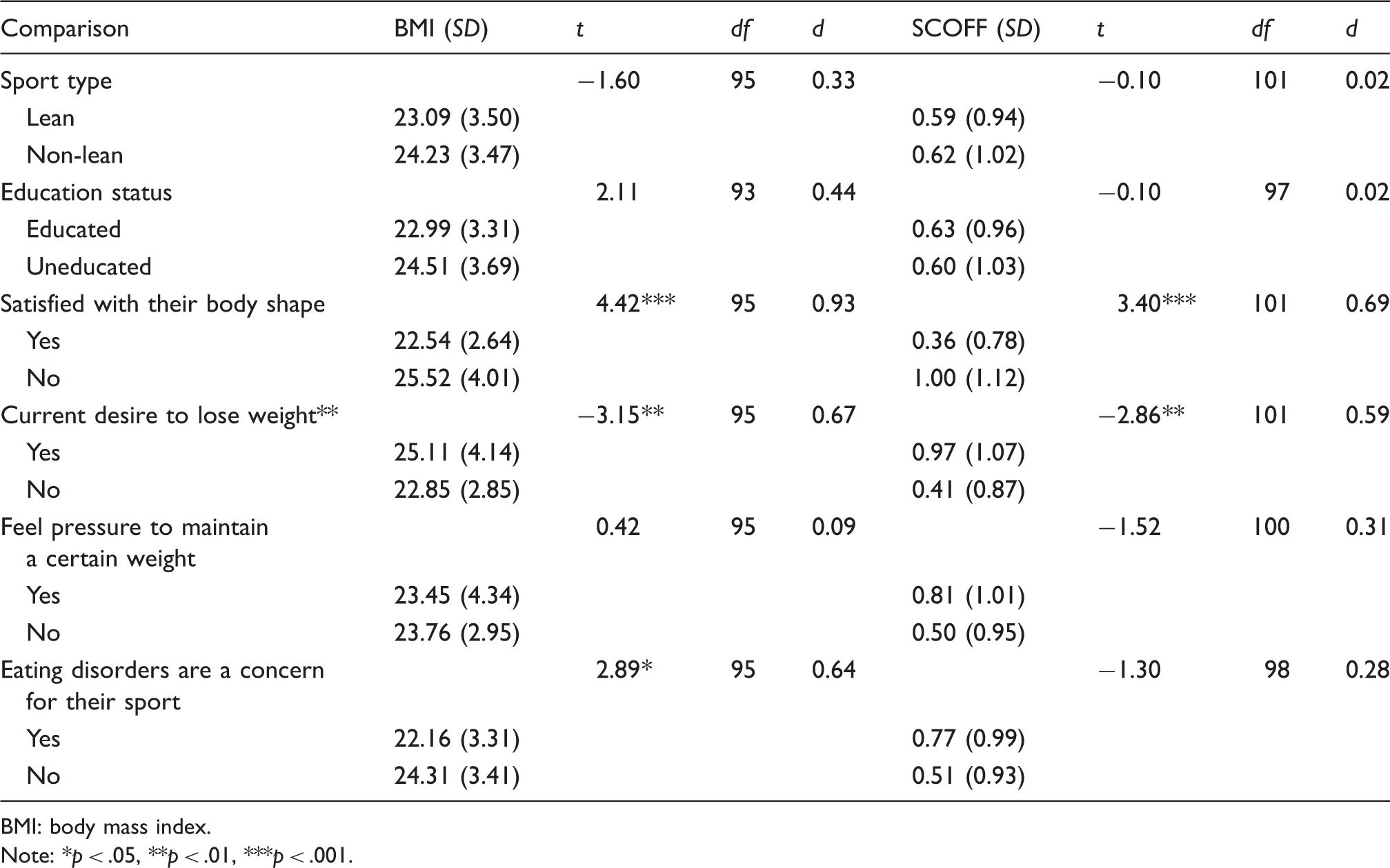
BMI: body mass index.
Note: *p < .05, **p < .01, ***p < .001.
Discussion
Our results indicate a deficiency in eating disorder education offered by coaches at this NCAA Division III institution. Lean and non-lean student–athletes reported similar rates of eating disorder education provided by coaching staff (approximately 55%) despite differential objective and subjective risks. 11 Consistent with prior research, more lean student–athletes reported pressure to maintain their weight and concern for eating disorders than did non-lean student–athletes (a 37% and 52% difference, respectively). 10 However, these differences were qualified by statistical equivalences in both their body shape satisfaction and current desire to lose weight. Although lean athletes felt more externalized pressure to maintain a certain weight in the context of their sport(s), they did not place more pressure on themselves (on average) than non-lean student–athletes. This similarity could be due to the many pressures women face outside of their sport to maintain thinness. 30 A possible interpretation would therefore be that participants felt a certain baseline level of pressure to meet society’s expectation of thinness, and this pressure was exacerbated in the context of lean-sport participation.
Student–athletes reported that their coaching staff’s educational efforts related to eating disorders included many topics examined in prior research, e.g., their negative side effects. 17 Although 30% of educated and 28% of uneducated athletes desired no changes to their curricula, most felt differently. Suggested curricular changes aligned with a comprehensive educational program suggested by the International Olympic Committee that includes long-term coverage of nutrition, eating disorders, healthy eating, and dieting, and how diet impacts performance. 31
Educated student–athletes most often requested more comprehensive and long-term curricula. One participant noted that coaches sometimes acted like they “just wanted to get it over with,” which is not likely to help emphasize the importance of provided information. Many educated student–athletes also wanted their coaches to explicitly state that they care about their athletes and are available to help them through hardships. Uneducated athletes also reported a desire for comprehensive education including, e.g., how to gain or lose weight safely. The lack of different perspectives between lean and non-lean student–athletes indicates that both groups desired relevant educational opportunities, and this aligns with prior research indicative of high-risk individuals participating in both types of sports.12,13 Also, SCOFF scores were similar among lean and non-lean as well as educated and uneducated participants, which indicates a similar distribution of vulnerable individuals in all categories—individuals who might benefit from educational (or other) interventions. Coaches should attend to these findings and become more educated about the topic so they are prepared to offer the education and services student–athletes need.
In terms of educational outcomes, student–athletes were similarly confident in their ability to identify an eating disorder in a teammate regardless of Sport Type or Education, but educated student–athletes outperformed uneducated student–athletes when asked to spontaneously report symptoms (e.g., physical symptoms such as fatigue were reported by 37% of educated student–athletes but only 21% of uneducated student–athletes). However, even educated participants failed to report many common symptoms (e.g., most of our sample neglected to mention physical symptoms), and this was not due to missing data (i.e., participants simply not providing a response).
In some cases, even participants’ basic understanding of eating disorders was flawed. For example, some endorsed the idea that a person purposely “turns to an eating disorder” even though they result from illness and not a conscious choice. 4 This belief may contribute to the shame and secrecy that often characterize eating disorders and make them harder to identify and treat. Participants also indicated a general lack of understanding of the potential consequences of an eating disorder including those that directly impact their physical and mental health as well as possible exclusion from sport participation for safety reasons. 4 Coaches should be taught to share this information with their student–athletes to help underscore the need to identify and treat eating disorders to both maintain one’s health and remain able to participate in desired activities.
Clearly, both educated and uneducated student–athletes should be provided with further opportunities to expand their knowledge of eating disorders including strategies for identifying them and intervening (or seeking help for themselves) as needed. Student–athletes cannot be expected to come up with this information spontaneously or based on “common sense.” They need to receive competent and relevant instruction from someone they trust who creates an atmosphere of concern and understanding about sensitive topics and offers help to those who may need it. This type of atmosphere could allow for an open, honest, and long-term conversation about the topic—which many student–athletes would support (based on our qualitative data). This would increase the likelihood of high-risk student–athletes being identified (regardless of sport) and directed toward personnel who could provide appropriate assessment and treatment.
Additional findings indicated that lean participants were no more confident in their ability to identify the signs of eating disorders than non-lean participants regardless of education and despite their increased risk. Also approximately half of our sample was unwilling to discuss their own or a peer’s possible eating disorder with their coach. Their reluctance was social in nature—reflecting a fear of privacy violation, lack of comfort with their coach, and a fear of embarrassment, shame, or judgment. As mentioned previously, effective education about eating disorders should increase student–athlete confidence and reduce stigma while encouraging them to be more forthcoming about their challenges. 21 This is of special importance given the low confidence many coaches have in independently identifying eating disorders in their athletes. 6
Athletes and coaches agree that the stigma surrounding mental illness is the biggest barrier to athletes seeking support.32,33 Researchers suggest that coaches emphasize open discussion and increased awareness of the issue, which align with suggestions from our participants. Although coaches in prior studies tended to favor intervention from professional clinicians (to whom they can often provide referrals), athletes thought of coaches as an asset from whom to receive direct support. This shows that coaches might offer the best care to their student–athletes by offering both personal support and by providing referrals to qualified professionals both within and outside of their academic institution.4,18,34 It is advisable for coaches to have an updated list of professionals available to help advise them how to approach each situation as it arises and connect athletes with helpful resources. 4 This may prove especially important for coaches who feel uncomfortable with the subject matter or for student–athletes who do not feel comfortable having such discussions with their coach (as was the case for many of our participants).
This study offers many opportunities for further research. First, ours was a convenience sample, which could mean that participants who responded did so due to preexisting biases that produced stronger-than-average feelings (e.g., the quality of their education). Secondly, although our Sport Type classifications were based on prior research, different sports exert different specific pressures on athletes, which was likely reflected in the large variety of responses to some open-ended questions. A larger, more representative sampling of athletes would address this concern.
We did not examine the nature of educational opportunities offered to student–athletes from a perspective other than that of the student–athletes themselves or attempt to assess coaches’ knowledge or confidence in an objective manner. Coaches could be given a variation of the survey created for the current study to compare their backgrounds and beliefs to those of their student–athletes while also revealing why they choose to educate their athletes the way they do (e.g., coaches with low confidence might not offer as thorough an education despite a desire to do so). These data would provide a more complete picture of the quality of educational experiences offered to student–athletes while also providing an opportunity for coach education. Additionally, the relationship between the educational opportunities provided by coaching staff and knowledge outcomes for student–athletes should be assessed directly. This could be accomplished by carefully examining the nature of the education received by coaching staff, the specific information they convey to their student–athletes (and the confidence with which they convey it), and the memory and confidence outcomes for athletes. Studying the process from start to finish would allow for the identification of areas in need of improvement.
Student–athletes’ desire for continued, regular conversations about eating disorders could encourage more complete learning and long-term retention of material by taking advantage of distributed practice effects in memory. 35 By offering multiple opportunities to discuss eating disorders, coaches could reinforce the learning that takes place as well as potentially making student–athletes more comfortable with such discussions by diffusing some of the associated tension (i.e., by making open discussions of taboo topics like eating disorders seem more normal and appropriate). Athletes appreciate coaches who care about them enough to approach them with a concern about their health and genuinely listened to their needs, and this conclusion could be more easily drawn by student–athletes if educational experiences were framed as something other than a presentation made due to a feeling of obligation rather than of perceived importance. 21 Finally, more studies should focus on how to engage coaching staff and administrators in the creation and management of relevant and scientifically accurate educational programs that would convey the dangers associated with eating disorders and provide student-athletes with tools needed to help avoid or resolve them.
Supplemental Material
Supplemental material for How do lean and non-lean female collegiate athletes view the eating disorder education they receive from their coaches?
Supplemental Material for How do lean and non-lean female collegiate athletes view the eating disorder education they receive from their coaches? by Jarrod C Hines, Whitney L Wendorf, Alexes N Hennen, Kelsey L Hauser, Madeline M Mitchell and Jillian M Homa in International Journal of Sports Science & Coaching
Footnotes
Authors’ note
The authors thank Samantha Korn for her help coding qualitative data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.