
Abstract
Athletes’ optimal training progression can be supported by reliable and valid monitoring tools. This systematic review aims to investigate tools that have been most frequently in the field used by coaches and practitioners of sports of any level. PyscINFO, Scopus, MEDLINE and SPORTDiscus databases were searched. Search terms used include: overreaching, overtraining, recover, fatigue, overload, train; monitor, athlete monitor, train monitor and coach, sport scientist, or performance coach. From the 1982 search results retrieved, seven articles met the inclusion criteria. The inclusion criteria required articles to be descriptive or observational studies on the training monitoring of athletes, be peer-reviewed, and in English. Physiological measures (e.g. heart rate) and measures of performance and workload (e.g. tests including sprints; global positioning system variables) were most frequently used. Psychological self-reported questionnaires, such as ratings of perceived exertion and mood inventories, were also frequently used in the field. The results indicated that only a few biochemical measures (blood and urine analysis) were regularly used outside of a laboratory. Easily implemented measurements were more commonly used than more advanced ones, indicating that the tools valued by practitioners are those that are time efficient, easy to administer and are non-fatiguing and non-invasive. Knowing what tools are currently used in the field is the first step in knowing what is practical and usable for coaches in the field, where after coaches and practitioners collaborating with sport scientists can develop and implement tools that are both useable and easily administered.
Introduction
Elite athletes perform regular training at differing volumes and intensities to improve competitive performance. 1 When balanced by sufficient recovery, athletes achieve improved performance, which is in line with the supercompensation principle. 2 However, if training and recovery are not appropriately balanced, maladaptive effects like prolonged fatigue, injuries, illness and overtraining syndrome can occur. This maladaptive response can lead to deterioration of an athlete’s performance, and endanger their overall mental and physical health. 3 To minimise the risk of potentially negative consequences of training, appropriate monitoring of an athlete’s training is required. Adequate monitoring may also be useful to identify fatigue, inform training prescription, and improve practitioners’ understanding of individual adaptations and responses to training.3–5
Training can be monitored by systematically recording via external and internal load. External training loads are a measure of the work completed by the athlete. 6 External load are measures specific to the training completed and can be measured via the duration of training, distance completed, volume and weight, for example. 7 The internal load is the stress an athlete may experience during training or competition. 4 Internal load can be measured differently including through psychological states (e.g. mood questionnaires or perceptions of effort), 8 physiological responses (e.g. heart rate), 9 and individual biomarkers (e.g. blood or saliva analyses). 10 However, as no single marker can accurately detect overtraining in athletes, it is recommended that several are used simultaneously. 6 A combination of workload, physiological, psychological and biochemical markers could therefore provide multifaceted information to both athletes and coaches.
Scientific investigation and interest on athlete monitoring techniques are reported in many studies.4,11,12 However, those working across research and applied sports science settings have identified a gap between the sports science research being conducted and what is implemented into practice. 13 There are several possible reasons for this disconnection, including a lack of collaboration between researchers and applied practitioners, often increased by their different educational backgrounds and terminology used.13–15 Furthermore, laboratory research, conducted with the aim of publishing peer-reviewed studies, are laden with requirements including controlled and specific sample groups, blind or double-blind study designs and carefully controlled external variables.13,15 While this maximises internal validity, it sacrifices external validity and applicability to practice. Researchers have consequently been criticised for not asking and investigating questions that will provide practical and useful information in applied settings (e.g. training and competition environments).13–15 In contrast, coaches and athletes primarily focus on practicality, performance and outcomes. 13 The availability (or lack thereof) of resources (e.g. time, equipment and staff), the knowledge and experience of coaching or support staff in implementing and sustaining a monitoring program, collecting and interpreting the results, and staff and athlete buy-in also influences the translation of research into practice. 6 These differing objectives contribute to the gap between research and practice.
Knowledge of available athlete monitoring techniques used in applied settings is the first step of improving current practice and closing the gap between research and practice. By understanding what is valued in the field, and how it is actually implemented, researchers may work together with coaches and practitioners do develop tools that are practically useable. Furthermore, coaches will be able to see what has been done in practice and how their monitoring techniques fit in, as well as have the opportunity to discover different monitoring strategies. The aim of this review is therefore to describe what monitoring tools are used in the field and their strengths and weaknesses.
Method
Search strategy
This review was guided by the preferred reporting items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. 16 The search was completed using MEDLINE, PsycINFO, SPORTDiscus and Scopus databases. The databases were searched from the earliest available record up to 1 October 2019. The search terms were: overreach* OR ‘over-reach*’ OR ‘over reach*’ OR overtrain* OR ‘over-train*’ OR ‘over train*’ OR recover* OR fatigue OR overload OR ‘over-load’ OR ‘over load’ or train* AND monitor* OR ‘athlete monitor*’ OR ‘train* monitor*’ AND coach* OR ‘sport* scientist’ OR ‘performance coach’. Search terms were consistent across the databases, with truncation marks changed as per database requirements. Searches were limited to peer-reviewed journal articles, English language and human population groups.
Eligibility criteria and study selection
The inclusion criteria for this systematic review was observational and descriptive literature investigating the training monitoring tools (condition/factor of interest) used by practitioners (population) to monitor athlete training at any level (context). The CoCo Pop (condition, context and population) mnemonic was used to develop inclusion and exclusion criteria through which search results were screened. 17 For the purpose of the current investigation, the term ‘practitioner’ was used to refer to fitness coaches, sports science personnel, coaches and medical personnel involved in monitoring athlete training and health. All sports, genders and ages were included in the search. Intervention and review studies or studies with a non-human sample were excluded. Intervention studies were excluded as they represented researcher manipulation and would not provide an accurate representation of the tools that practitioners were choosing to use themselves. The inclusion criteria are open to articles describing training monitoring practices that have been used in the field previously, and is not restricted to any time period.
Once duplicates were removed, results were screened by title and abstract against the inclusion criteria. The full text was sought and screened against the selection criteria if it was unclear from the title or abstract whether the study met the inclusion criteria.
Figure 1 illustrates the PRISMA flow diagram depicting the number of articles retrieved from the database search, and included and excluded at each stage. A total of seven articles met the inclusion criteria and were included in the study. Six full-text articles were excluded: two articles18,19 were excluded as did not fit the design (observational/descriptive articles). Four articles20–23 were excluded as they did not fit the condition and/or context (athlete training monitoring tools used in practice) of the review.
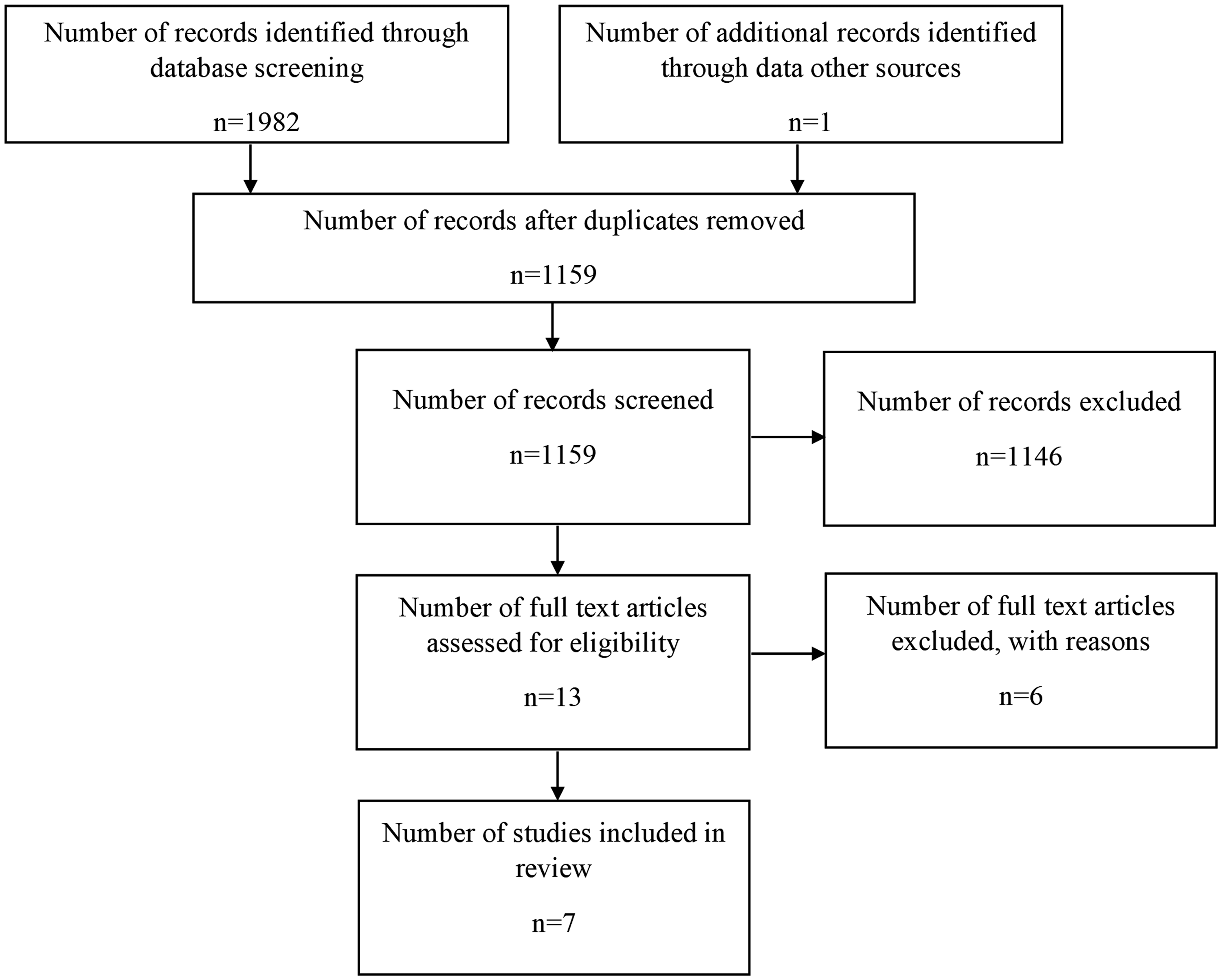
PRISMA flowchart of study selection.
Quality assessment
A quality assessment of the included studies was conducted against a version of the Joanna Briggs Institute Critical Appraisal Checklist for Studies Reporting Prevalence Data. 24 This checklist was considered the best tool available to critically assess the studies in the review. However, the first author made several modifications to make the checklist more appropriate to the scope and design of the articles included in the review. Out of the nine original items, item number five ‘was data analysis conducted with sufficient coverage of the identified sample’ and item six ‘were valid methods used for the identification of the condition’ were removed from the original checklist. These items were removed as they dealt with a specific sample population/condition rather than the broader use of monitoring tools this review is focussing on. One item assessing the quality of the descriptive data displayed, and one item assessing acknowledgement of funding source were included in the modified version. Articles were checked against nine criteria with a yes/no response. Authors H.M. and P.H. conducted the quality assessment. All articles that met the criteria were included in the study. The articles were assessed as unsuitable for meta-analysis due to the descriptive nature of the results and lack of consistent measures being evaluated.
Results
Study characteristics
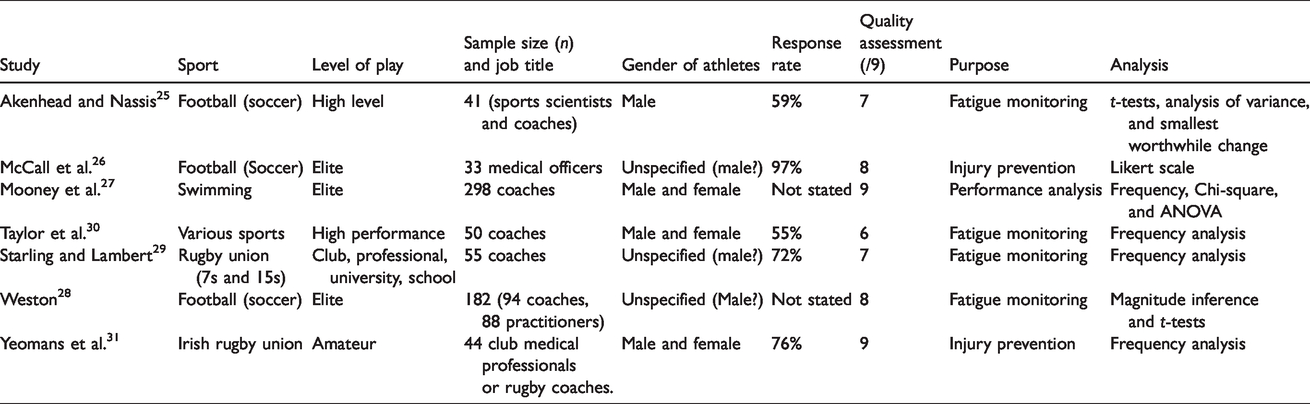
Characteristics of the included studies, including the sample size, sport and level, and purpose of each article are presented in Table 1. Field-based, invasion team-sports (e.g. football and rugby) were the most common sports sampled, with five studies25–29 solely assessing these sports, and a further study 30 assessing ‘various’ sports including field-based sports. The professional/elite level was the most common sporting level with five studies25–28,30 assessing this level of sport, the remaining studies assessed a mixture of sport levels 29 and amateur sport. 31 The purpose of the included studies could be categorised into three main concepts: monitoring for fatigue and fitness,25,28–30 injury prevention/monitoring26,31 and performance analysis. 27 All studies received a score of six or more out of a possible nine points on the critical appraisal checklist.
Study characteristics and quality assessment of included studies.
Training monitoring
Monitoring tools can be cross-disciplinary in nature; however, for the purpose of this review, they were grouped into four different categories: biochemical monitoring, physiological monitoring, external workload monitoring and psychological monitoring.
Tables 2 and 3 display the three most commonly reported monitoring tools for workload and psychological monitoring, and biochemical and physiological monitoring, respectively. The common tools reported in the studies were global positioning systems (GPS) variables and match performance to measure external training load, heart rate measures and performance tests to assess physiological responses and physical capabilities. Ratings of perceived exertion (RPE) scales to assess physiological response to training sessions, and self-report questionnaires to assess psychological aspect of training were also common.
The three most commonly reported monitoring tools and frequency of response (reported as a percentage of responses) for biochemical and physiological monitoring categories for each study.
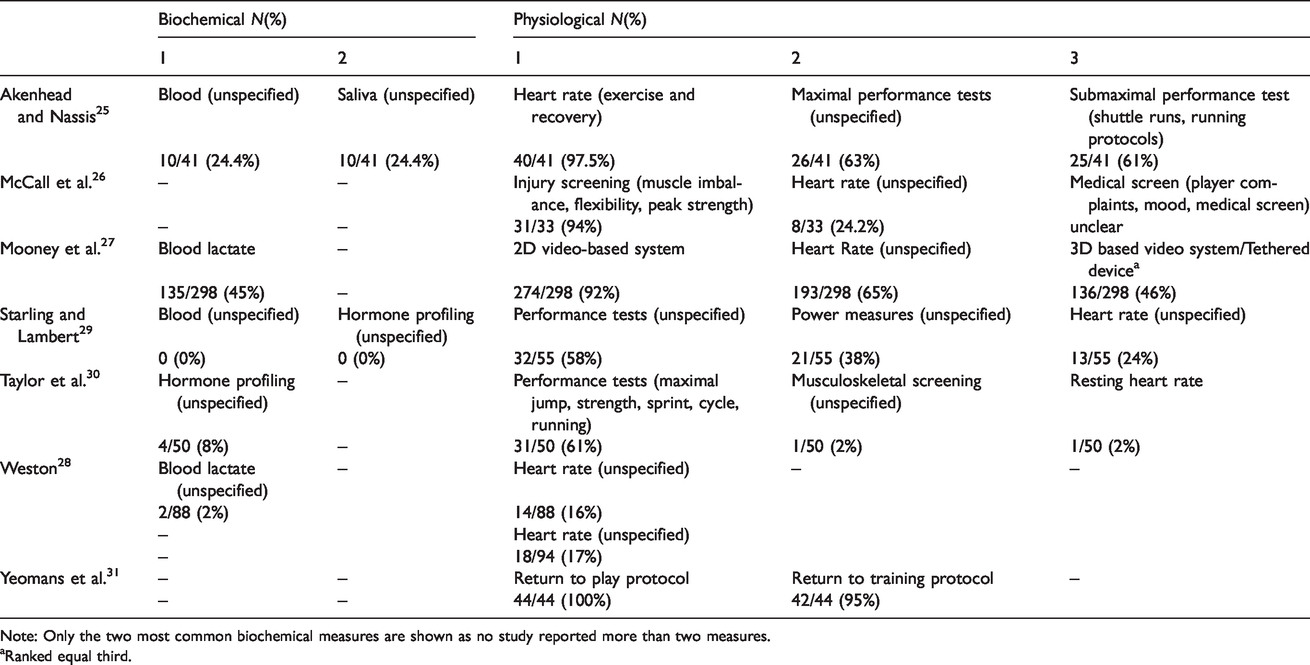
Note: Only the two most common biochemical measures are shown as no study reported more than two measures.
aRanked equal third.
The three most commonly reported monitoring tools and frequency of response (reported as a percentage of responses) for the workload and psychological monitoring categories for each study.
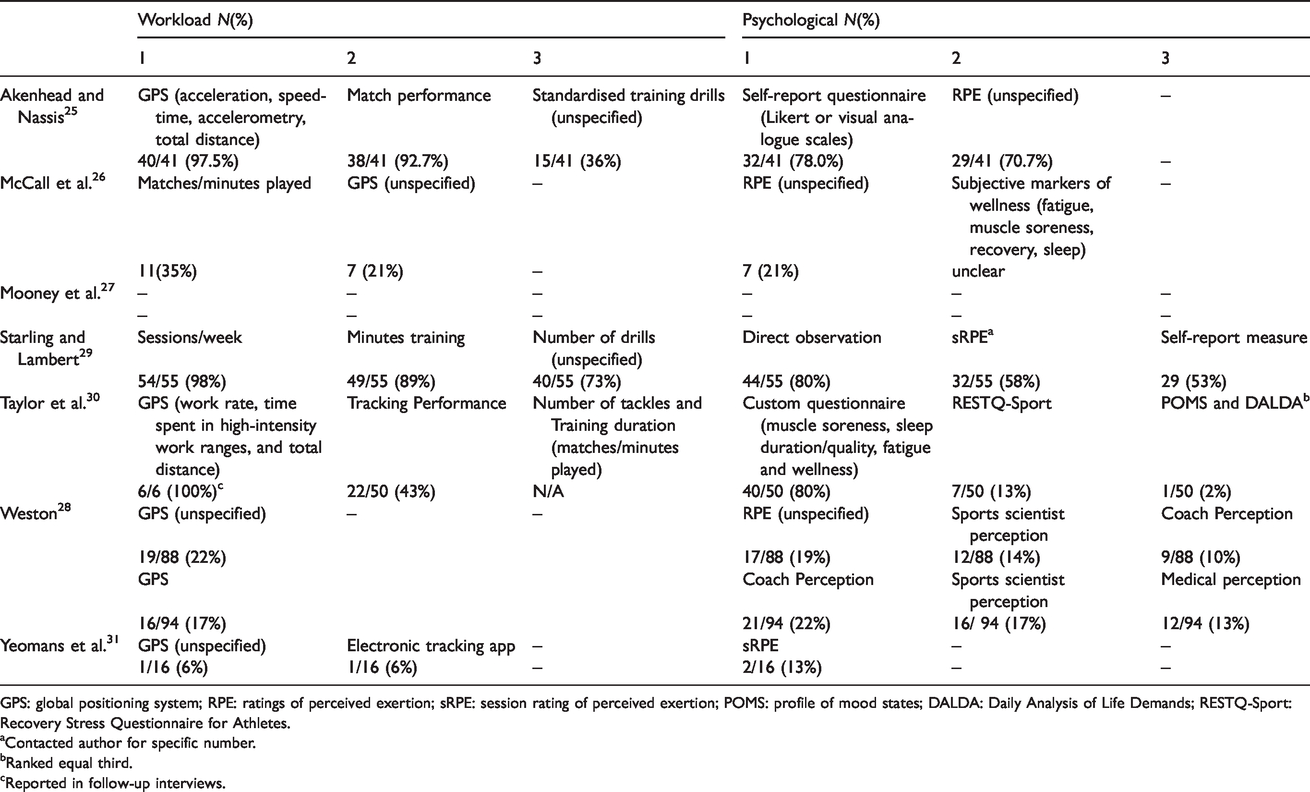
GPS: global positioning system; RPE: ratings of perceived exertion; sRPE: session rating of perceived exertion; POMS: profile of mood states; DALDA: Daily Analysis of Life Demands; RESTQ-Sport: Recovery Stress Questionnaire for Athletes.
aContacted author for specific number.
bRanked equal third.
cReported in follow-up interviews.
Biochemical monitoring
Blood analysis to monitor training was reported in three studies;25,27,28 blood lactate was reported in two studies,27,28 while the third study 25 did not specify what blood was analysed. Usage ranged from 2% 28 to 45% 27 and was commonly reported being measured monthly.25,27 The use of saliva to monitor training was reported by 10 (24%) coaches in one study. 25 It was not stated what was specifically measured. One study 30 reported the use of hormone profiling. Use was low with only 4 (8%) participants using it to monitor athletes. The type of hormone profiling was not stated.
Physiological monitoring
The collection of heart rate indices was reported in six out of the seven studies. Practitioner usage varied from 1% 30 to 98%. 25 Specifically, heart rate variability was reported by 12 (30%) practitioners involved in high-level football, 25 while resting heart rate was used by one participant to measure their athlete(s) in a study of various high-performance sports. 30 The remaining studies reporting the collection of heart rate did not state what heart rate indices were measured or when heart rate was frequently used (every session/daily).25,27,29
Performance tests of physical capabilities and characteristics were reported in three studies.25,29,30 Reported frequency of use was from 58% 29 to 61%. 30 Submaximal and maximal performance tests were both reported.29,30 Performance tests included jump tests, sport-specific test protocols, strength/power tests and running or cycling tests. 30 Submaximal performance tests were commonly used weekly or monthly.25,29,30 Maximal performance tests were used less frequently at monthly to quarterly intervals. 29
Injury screenings, medical screenings, 26 and return to training and return to play protocols were reported. 31 Injury screening tools included side-to-side muscle imbalance, flexibility, peak muscle strength evaluation and joint mobility and function. 26 Medical screenings were mainly reported in amateur rugby to assess concussion. 31 Return to play protocols were implemented in all of the amateur rugby clubs surveyed, return to training protocols were implemented in 95% of the clubs. 31
External workload monitoring
The use of GPS was reported in six of the seven studies. Usage varied from 6% 31 to 100%. 30 GPS was reported in all studies reporting on field-based sports (soccer,25,26,28 rugby29,31 and ‘various’ 30 sports). Although the majority of sports represent elite or high-performance sports, GPS was also used at the lower levels of play (although reported use was less common).29,31 GPS devices were commonly used every field-based training session. 25 Variables analysed include work rate (meters covered per minute), time spent in high-speed zones, total distance and number of tackles performed. 30
Training/match duration, such as number of matches played, minutes played or match performance 26 and training duration 25 were reported to monitor external workload. Use of training or match duration was used frequently from 35% of practitioners involved in elite soccer 26 to 98% of rugby practitioners at all levels of play 29 . These were most frequently taken into account weekly to monthly. 25
Subjective monitoring
One study reported the use of validated questionnaires in practice. 30 Across 50 participants from various high-performance sports, use of these questionnaires was low. In this study, the Recovery Stress Questionnaire for Athletes (RESTQ-Sport) 32 was used by 13% of participants; the Profile of Mood States (POMS) 33 and the Daily Analysis of Life Demands for Athletes (DALDA) 34 used by 2% of respondents each.
For the purpose of this review, self-report questionnaires are considered to be either custom designed questionnaires or questionnaires not clarified as being a validated or established questionnaire. Five studies reported self-report questionnaire use with high with usage ranging from 53% 29 to 80% 30 of participants implementing them. They were frequently used daily to weekly.25,29,30 The questionnaires covered areas including fatigue, muscle soreness, perceived recovery, sleep and mood.26,30
Athlete RPE were collected by practitioners in five of the included studies. Use ranged from 17% 28 to 71%. 25 In a comparison between coach and practitioner (specifically fitness and sports service personnel) use, RPE was used more by practitioners than coaches in elite soccer (22% vs. 12% respectively). 28 The use of session rating of perceived exertion was reported in two studies29,31 to monitor workload; however, others25,26,28 may have used RPE to calculate sRPE.
The perception and observation of coaches and practitioners to monitor athlete training was reported in two studies.28,29 Direct observation was used by 80% of coaches in various levels of rugby, with the club level using it most frequently. 29 The observation of players by staff was taken into account every session. In elite level soccer, the perception of a variety of other practitioners was also considered. Coach perception was used by 22 (22%) of coaches, and nine (10%) of practitioners, medical staff perception was taken into account by 12 (13%) of coaches and seven (8%) practitioners, sports scientist/fitness coach perception was taken into account by 16 (17%) coaches and 12 (14%) of the practitioners. 28
Discussion
The purpose of this review was to describe the tools used by coaches and practitioners to monitor the training of athletes. Seven studies were included in the review. Training load monitoring is a relatively new topic as such the articles are relatively new, with the oldest being from 2012. Therefore, by virtue, the review covers practices as published upon in the last 8 years. The majority of studies used an elite or high-performance population,25–28,30 two studies also investigated monitoring tools across lower levels of play (club, university and school; 29 amateur). 31 Physiological measures, such as the measurement of heart rate indices were common. Workload monitoring data such as GPS variables were also commonly collected within the high-performance setting on a regular basis. Subjective measures including RPE and wellness measures were commonly used by all levels of sport included in this study on a daily basis. However, many questions remain around these monitoring tools and how they are implemented in the field, and what type of data is collected, analysed and used in the decision-making process.
Biochemical analyses
There is an abundance of research on the use of biomarkers to monitor athlete training. For example, Lee 10 provides a comprehensive review with recommendations for biomarker use for athlete training and monitoring. Furthermore, a recent systematic review and meta-analysis investigating biomarker responses to intensified exercise training identified 118 individual markers used in 101 studies. 35 The biomarkers considered to offer the greatest insight into training included the athlete’s testosterone to cortisol ratio, circulating glutamine and urea concentration. 35 However, few biomarkers were reportedly used by practitioners in the studies reviewed indicating their use in practice was low. When biomarkers were reported to be used, the specific markers being analysed were often not stated. Not stating this information does not inform us of the markers that are valued by practitioners, limiting future research’s ability to approve on the practicality of collection and analysis of these markers. Blood lactate, a relatively inexpensive tool that is suitable for use in the field, was the only specific biomarker reported across the studies. Limitations to biochemical analysis, likely contributing to the low reported use include the expense of collecting and analysing samples, as well as variations that can influence the results including the athlete’s diet, hydration status, training schedule, or time of collection. 6 The lack of biomarker reference values, particularly for elite athletes, further complicates conclusions that might be drawn from such data. 10 Nevertheless, regular assessment of several purposefully selected markers for biochemical analysis, and scheduled testing, has been recommended to provide insightful and objective information about the athlete’s response to the coaching team. 10
Physiological
Physiological monitoring tools were commonly implemented into monitoring programs. Specifically, heart rate was reported as a common tool in six of the reviewed studies. Heart rate can be measured at different times (e.g. at rest, during exercise and post-exercise) and used for various purposes (e.g. as an early sign of illness, assessment of aerobic fitness, etc.). 36 However, only two studies gave more specific information on which indices were collected, which were resting heart rate 30 and heart rate variability. 25 Heart rate variability is the variation in time between each heart beat and may be used to monitor the sympathetic and parasympathetic activity and stress the body experiences during exercise, and the recovery after exercise. 37 It is most valid when collected for 5–10 min in the supine position upon waking. 36 For endurance athletes, resting heart rate monitoring is recommended at least three to four times a week and supplemented with exercise heart rate. The autonomic nervous system can be monitored via heart rate and can be used to objectively monitor the intensity of the exercise completed, or used long term to monitor the fatigues and fitness of the athlete.36,37 Team sport athletes are recommended to collect exercise heart rate and resting heart rate weekly on a standardised training day. 36 Practitioners and coaches in the reviewed studies reported collecting heart rate more frequently than these recommendations, with measures commonly collected every session/daily.25,27,29 However, it was not stated when and how often this data was analysed and if it was used to inform subsequent training prescription or recovery.
Performance tests of physical capabilities and characteristics
Performance tests were frequently reported in three of the reviewed studies.25,29,30 Improvement of competitive performance is indeed the end goal of training for many athletes and hence performance tests are a direct assessment of sport specific improvement. 38 However, they can be highly fatiguing, and may require the athlete to be fully recovered prior to starting the test, which may have a negative effect on previous and subsequent training. Prolonged decreases in performance can indicate maladaptation to the training program and are a marker of non-functional overreaching. 39 Performance tests should be easy and time-efficient to implement and incorporate into a monitoring program, and should not present any additional load to the athlete. 40 Only two studies25,30 reported the specific performance tests used. Tests such as jump tests and running or cycling drills were commonly used and reflect these requirements of being easy to implement and time-efficient.
Workload
Measures of external workload were commonly reported in every study reviewed. Measures of external workload are important to understand the work completed by the athlete, their capabilities and to prescribe future training loads. 6 The measures reported (number of sessions per week, training duration, number of drills and minutes played) are easy to document and interpret, have low associated costs, are valid and reliable and can be used with minimal technology. 4 One issue with these measurements is that they often represent a measure of training volume, while ignoring the intensity at which they are completed. Hence, coaches focussing on these metrics may be encouraged to prescribe programs high in volume at the expense of intensity. Also, if the intensity is not monitored, then sudden increases in exercise intensity may go unnoticed, increasing the risk of injury for the athlete. 12
The use of GPS to monitor training was reported by all field-based studies reviewed.25,26,28–31 Use was more frequent for team sport athletes in the professional/elite samples25,28 compared to lower levels of sport.29,31 The difference in use of monitoring tools between sporting levels could be attributed to the high expense of purchasing the GPS devices, as well as on-going software subscriptions, and employment of dedicated staff with the knowledge to monitor, analyse and summarise the large amount of data that is generated. 4 It is recommended that GPS use within a monitoring program should be easy to use with simplistic feedback, such as analysing key performance indicators (e.g. distance covered in different velocity zones, number of acceleration/decelerations or workload calculations) that have established reliability and validity, and cover different aspects of athlete performance. Finally, practitioners should take the time to set individual threshold values for their athletes, such as setting upper and lower thresholds for parameters and reference values of these training days (e.g. day before or after competition/game day). 41
Self-report measures
The use of subjective measures to monitor training was common across the reviewed studies. The RPE scale is easy and inexpensive to administer and can be used with large groups of athletes at once. Furthermore, the RPE scores are comparable with heart rate and oxygen consumption measurements due to the assumption that as physiological strain increases so does the perception of physical intensity. 42 Session RPE (sRPE), is a workload calculation based of RPE which takes into account the intensity and duration of the work completed, is also a simple tool to monitor the overall training load completed. 43 sRPE has been validated across several sports and athlete levels within the applied setting. 43 Of course, such data relies on honesty from the athlete and consistency in their reporting. None of the seven studies in the current review described how long after training cessation the athletes reported their RPE. Original guidelines for the use of sRPE suggest that data be collected 30 min after training cessation. This time-point would allow the athlete’s score to reflect the global intensity of that secession, rather than being influenced by any harder or easier bouts of work towards the end of the session. 44 Whether the time of collection impacts on the accuracy and interpretation of the data, however, is still under investigation. Recent research has suggested that the collection time does not influence RPE scores in steady state or interval exercise 45 or in boxing athletes, 46 for example. Conversely, research into recreational and competitive endurance athletes 47 and high-intensity functional training 48 found that the longer the time period between training cessation and RPE collection resulted in lower RPE values compared to time-points closer to training cessation. 47 It is recommended that the timing of collection of RPE data from the athlete should remain consistent to accurately gauge intensity and work completed. 47
A number of questionnaires have been developed and validated to assess mood, wellbeing, stress, and recovery in athletes. Validated questionnaires (such as the RESTQ-S) are sensitive to changes in training load and can help and identify changes in athlete wellbeing. 11 However, the use of validated questionnaires assessing mood and wellness was only reported in one study 30 with the majority of coaches and practitioners reporting the use of other custom-designed questionnaires or ‘self-report’ questionnaires. Respondents in Taylor et al. 30 reported the extensive nature of the established questionnaires, the time burden for the athlete to complete and for staff to analyse, and the lack of sports specificity as barriers to validated questionnaire use. Furthermore, the frequent use of these measures may lead to ‘question fatigue’ and a lack of compliance from the athlete. 49 These reasons may cause coaches and practitioners to use their own, modified questionnaires. Taylor et al. 30 reported coaches ask four to twelve questions focussing on areas of sleep (duration and quality), fatigue, and wellness. Similarly, a sample of elite soccer coaches (45%) indicated measures of fatigue, muscle soreness, perceptions of recovery and sleep were important to monitor athlete recovery. 26 However, the validity and reliability of these questionnaires have not been sufficiently assessed. Gastin et al. 50 demonstrated that common measures of subjective wellness (including fatigue, muscle soreness, pain and/or stiffness, sleep, and well-being) are sensitive to changes in training and can be useful to monitor athlete response within the Australian Football League. Further research of these wellness questions among different sports and levels of play is needed to further establish their validity and reliability.
Researchers have acknowledged the need to shorter, practical questionnaires to monitor the psychological response to training. To reduce to time burden on completion, recent recommendations from Saw et al., 11 suggest implementing particular subscales from the validated questionnaires to decrease the length and time burden of completion. To monitor acute changes, the subscales of vigour/motivation, physical symptoms/injury, training stress, fatigue, physical recovery, general health/wellbeing and being in shape should be used. For ongoing monitoring, subscales assessing the non-training stress an athlete may experience, fatigue levels, recovery, health, wellbeing, being in shape, and any conflicts/pressure are useful. Additionally, the RESTQ-Sport has been updated to include a briefer version (RESTQ-36-Sport) with 36 items in order to reduce this time burden. 51 Consistent with current recommendations, 11 most coaches and practitioners within the review implemented frequent (daily) monitoring.
Sport level
The monitoring tools implemented from amateur to elite levels of sport were simple, easy to use, and generally inexpensive. However, the high-performance/elite respondents reported using more equipment-based monitoring systems like GPS and biochemical analysis compared to the lower levels of the sport. Starling and Lambert 29 reported that school and club level participants used observation and self-report measures more frequently than the university and club respondents. The reasons for the difference in tool use may be due to the availability of resources needed to implement technology-based systems into a monitoring program and the knowledge and expertise to analyse the data which may be lacking at the lower levels of sport.6,29 However, only seven studies were analysed, with the majority being from the high-performance sport settings; therefore, comparisons between different sporting levels may need further research to support this observation.
Strengths and limitations
This review is the first to summarise and critique research surveying the training monitoring tools used in applied settings. Knowing what is used in the field can indicate what is practical and valued by coaches and associated staff. This information can be used to improve these tools and disseminate this information to those working in the field. However, this study was limited to peer-reviewed articles. As there is a disparity between preferred sources of information of researchers compared to practitioners, 14 information on training monitoring practices may be found in sources other than peer-reviewed journals. Therefore, future reports could include and analyse sources outside academic literature to better understand what is used in the field. This review has nevertheless identified gaps in previous research, in particular, many of the articles present an incomplete description of the training monitoring tools used. Specific details on frequency, timing, methodology, or even what was being monitored was not well described. Finally, an assessment of how these tools are used to inform the decision-making process would also be an interesting outcome. Knowing these details could provide researchers with information on what practitioners are most interested in when performing their training monitoring, thereby allowing researchers to ask questions that are more industry relevant.
Recommendations for future research
Future research into applied training monitoring should involve practitioner collaboration at all stages of the research process. Collaboration between practitioners and researchers will have high relevance and contribute to the practice in the field. Additionally, investigation into how these tools are used in the decision-making process is needed to greater enhance both the understanding of how these tools are used is needed. Knowing how the tools are used in the decision-making process will also aid researchers in optimising a training monitoring program.
The systematic search only retrieved seven relevant studies focussing on the training monitoring tools used in practice. One possible reason for the limited studies is that minimal research has been conducted to understand the training monitoring tools and processes used in the field. This highlights a potential disconnect between researchers and practitioners, that has been noted previously in the literature, 13 and provides an area for future research.
None of the reviewed articles compared the use of monitoring tools between male and female athletes. There is a significant underrepresentation of female participants in sport and exercise medicine research. 52 Differences in male and female physiology and biochemistry may affect the results of certain tests, for example, lower sRPE values have been reported for women, than men. 47 Additionally, the menstrual cycle phase and sex hormone fluctuations of females can affect the physiological aspects of the recovery process after exercise. 53 It is therefore important to determine whether there is a gender difference when using different tools to be able to accurately monitor training.
Conclusions
The purpose of this review was to describe which tools are used to monitor the training of athletes in the field. Seven studies met the inclusion criteria, these monitored athletes for fatigue,25,28–30 injury and prevention26,31 and performance. 27 Few biomarkers (blood and saliva) were used across the studies, indicating they are not frequently used outside laboratory research. Physiological and workload monitoring tools such as measures of heart rate and GPS were commonly used. Subjective measures such as RPE and custom-designed self-report measures (despite the availability of validated questionnaires) were also frequently used. Commonly used tools are generally inexpensive, non-invasive and can monitor multiple athletes at once. Given the associated strength and limitations of these tools, a bio-psychophysiological approach, incorporating several tools from each discipline may be considered to provide a multifaceted and more complete picture of the athlete’s health and performance status to both athletes and coaches. However, these monitoring tools should be practical to use in the field. Knowing what tools are currently used by coaches, how they are implemented in practice, and how these differ from recommendations is the first step to better monitor training in athletes. The second step should involve coaches and practitioners in all stages of the research process to develop better quality monitoring tools and improve evidence-based practice.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.