
Abstract
Elbow tendinopathy injuries are very common in tennis players. One of the commonly accepted theories describing the development of elbow tendinopathy in tennis is based on stiffness of the forearm skeletal muscle units and their repetitive overuse in the forehand stroke. Our objective was to use a novel microcontroller based wearable device to compare the influence of different forehand spin levels (flat, topspin and lob) and ball exit speed on forearm muscle activity in the potential onset of elbow tendinopathy in experienced adult tennis players. Peak normalised extensor carpi radialis (ECR) and flexor carpi radialis (FCR) muscle activity corresponding to each forehand shot and ball exit speed were determined and analysed. For the ECR shots (flat = 121, topspin = 272 and lob = 273) by 8 players, Kruskal-Wallis test (p < 0.001) and Post-Hoc tests revealed a significant difference between the flat and topspin spin levels (p < 0.01) and flat and lob spin levels (p < 0.001). For the FCR shots (flat = 125, topspin = 301 and lob = 303) by 9 players, Kruskal-Wallis test showed no significant difference between the three spin levels. For the corresponding ball speed, the Kruskal-Wallis (p < 0.001) and subsequent Post-Hoc (p < 0.001) showed that flat hits had the significantly highest ball speed followed by topspin then lob accordingly for both muscles included shots. Our results suggest that coaches could consider recommending players to hit forehands with topspin in order to potentially reduce the risk of developing lateral elbow tendinopathy.
Keywords
Introduction
Between 40-50% of tennis players experience elbow symptoms throughout their career.1,2 Lateral elbow tendinopathy (LET) or “tennis elbow” is more common in recreational players, while medial elbow tendinopathy (MET) or “golfer’s elbow” is more common in advanced players.3,4 The repetitive overload nature of the forehand stroke on the forearm musculature has been implicated in the development of elbow tendinopathy in tennis players.5,6 The forehand stroke is complex and can be divided up into three phases: (1) the preparation phase characterized by the first movement of the backswing to the first forward movement of the racket (2) the acceleration phase characterized by the first forward movement of the racket to the point of ball impact and (3) the follow-through phase that starts at the point of impact and finishes with completion of the stroke. 7 Regarding the development of MET, the forehand stroke is thought to play a main role due to valgus overload during the acceleration phase, especially among tennis players who often hit the ball with topspin. 6 Because the forehand is the groundstroke most frequently hit by professional players 8 it is likely a significant contributor in the onset and progession of elbow injuries.
Players often hit the ball with varying levels of spin and ball exit speed depending on their playing ability and desired playing style (tactical situations). 9 In the context of recreational tennis, although topspin is the most effective method for controlling the ball in the court, recreational players will typically first learn to hit the ball flat before they learn topspin. 10 There are three levels of spin in a forehand stroke; minimal ball rotation (flat), moderate level of forward rotation (topspin) and high level of topspin (lob). 11 Topspin is generated on the ball by the racket following a low-to-high path (wrist abduction) through the impact zone, while faster racket head velocity results in greater ball exit speed during the forehand stroke. 12 Kinematic studies have shown a decrease in horizontal and increase in vertical racket head velocity between the flat and topspin forehand strokes.9–11 This movement involves wrist abduction which uses both the extensor carpi radialis (ECR) and the flexor carpi radialis (FCR) muscles. 13 However, a study by Rota et al. 14 found no significant difference in ECR and FCR activity levels for flat forehands hit at a range between 60–100% of player’s maximal velocity. Differences in movement patterns between flat and topspin forehands suggest that the upper limb muscle activation patterns will be different. 15
To date, there is no consensus as to the main etiology of elbow tendinopathy, although it has been suggested to be multifactorial 16 and non-gender specific. 17 One of the most commonly accepted theories to describe the development of elbow tendinopathy in tennis players is based on the stiffness of the skeletal muscle units and their repetitive overuse in tennis strokes. When the skeletal muscles stiffen near maximum contraction, the vibrations from impact are transferred efficiently and directly to the myotendinous junction causing repeated microtrauma.18,19 LET is typically associated with overuse of the extensor carpi radialis brevis (ECRB) muscle, 20 while MET is commonly associated with overuse of the FCR muscle. 6 A study by Wei et al. 21 found that higher levels of forearm electromyographic (EMG) activity corresponded with more impact vibrations transferred to the elbow joint on the backhand stroke. These observations underpin the rationale for the current study.
The majority of biomechanics research in tennis has been carried out in a research laboratory environment with multiple high speed cameras linked to a computer to produce 3 D displacement data of the player. 22 However, recent revolutions in computational hardware and software has resulted in microcontrollers and low-cost inertial sensors (such as gyroscopes and accelerometers) that allow rapid prototyping for personalized applications and ergonomic experimentation. Due to their small size, inertial sensors are providing new ways to conduct of motion analysis research either on court or even under tournament conditions. 22 The Babolat Play® tennis racket and the Head Tennis Sensor® are examples of commonly available commercial devices for tennis which use algorithms to estimate the number of strokes, swing type, impact location, ball spin level and ball exit speed under playing conditions. These types of devices typically use an accelerometer to analyze the direction of the racket, a gyroscope to analyze the rotation of the racket and a piezoelectric sensor that analyzes the vibration of the racket to identify the location of the ball on the racket strings at impact. 23 However, the technical specifications of the sensors and software are not publicly available and there is no requirement to conform to technical quality control of data standards, thus the accuracy of these commercially available tennis sensors is currently unknown. 24
The ability to easily visualize the player technique and relate this to the influence of forehand topspin on forearm muscle activity is important tool when tennis coaches and clinicians instruct players on their best playing style to prevent the potential onset of elbow injury.
Based on the need for reliable real-time data acquisition during tennis play, the primary aim of our study was to develop and test a novel microcontroller based wearable device that could measure racket movement and the EMG activity of the forearm muscles. The second aim of the study was to determine the influence of different forehand spin levels (flat, topspin and lob) and corresponding ball exit speeds on forearm extensor and flexor muscle activity in order to test the hypothesis that the spin level and ball exit speed during the forehand stroke have a significance influence on the level of maximal forearm extensor and flexor muscle activity.
Materials and methods
To measure the player’s forearm electromyographic activity, we designed, developed and tested a prototype device we called Tennis Racket Accelerometer MyoWare Wearable Device (TRAM). TRAM consisted of a microcontroller (Teensy 3.6, PJRC, Oregon, USA) attached to the handle of the racket, two EMG Muscle Sensors (MyoWare® AT-04-001, Advancer Technologies, Raleigh, USA) which were positioned over the main forearm muscles associated with the development of elbow tendinopathy (ECRB and FCR) together with a 3-axis digital accelerometer (ADXL345 (±16 g), Adafruit, New York, USA) attached to the throat of the tennis racket (Figure 1(a)). The device was powered through a 1.2 meter Micro-USB cable (Belkin Micro-USB), taped onto the player’s arm and connected to a portable power bank (Cygnett, 3000 mAh) in their pocket.
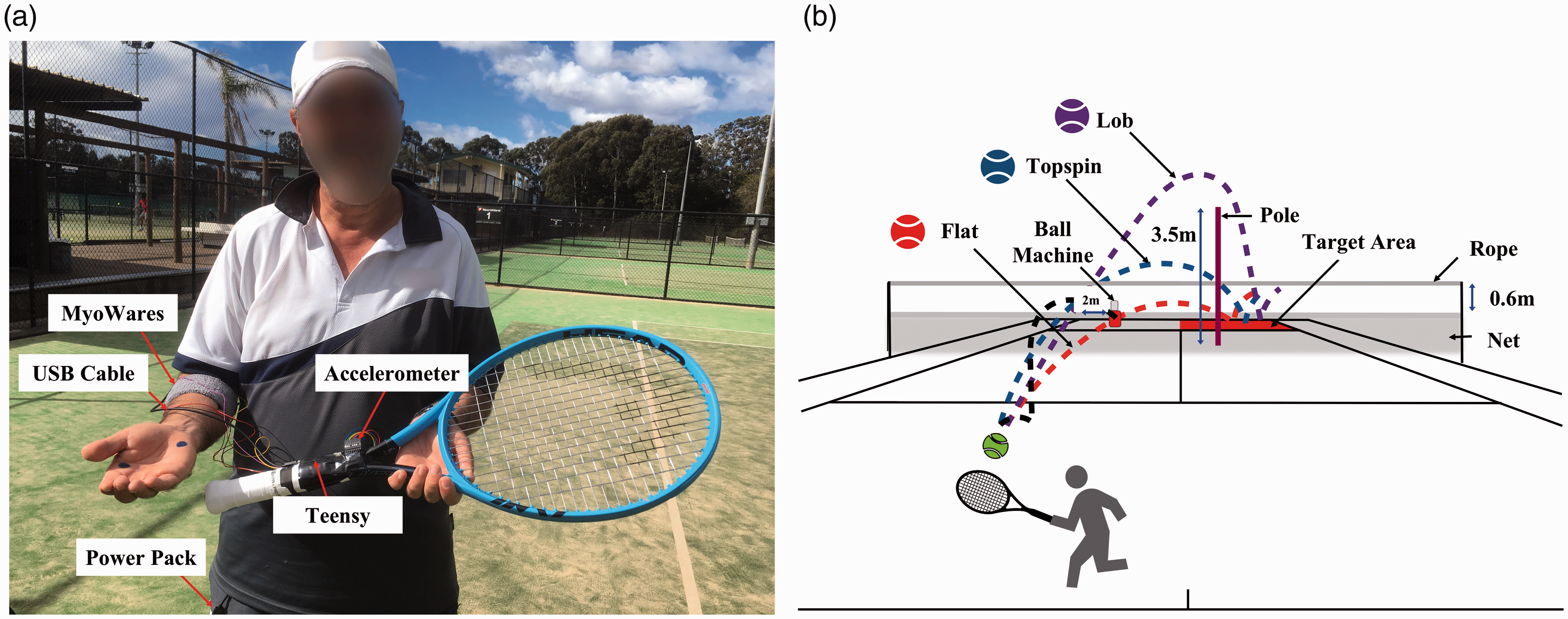
Experimental TRAM set-up and on-court testing protocol. (a) The placement of TRAM on a player as marked. (b) For the shot to be include for analysis, players must have hit the ball from the ball machine into the target area, following the correct ball spin height guideline as indicated for either the flat, topspin or lob spin level.
TRAM simultaneously collected data from all three sensors at 3200 samples per second and which were stored on a micro SD card (SanDisk Ultra microSDHD UHS-I 16GB Card) on the Teensy. To reduce data latency and increase the accuracy of data collection the sampling rate of the accelerometer was used to trigger the collection of the MyoWare® data. Each time the accelerometer produced a signal, the MyoWare® sensors were triggered to collect data. The microcontroller packaged the data points with a modified version of an open access low latency data-logging Teensy 3.6 SDIO SD code 25 and sent them to the microcontroller SD card for storage. Therefore, each data point from the sensors had the same timestamp which enabled continuous time domain analysis of the MyoWare® data to be matched to the different phases of the forehand stroke as determined by the accelerometer data. The device was then tested on experienced players through an on-court testing session. Raw TRAM data were retrieved during rest periods from the SD card for later processing using MATLAB (R2018b).
Ten male right-handed tennis players (39.2 ± 10.0 years old, 180.9 ± 6.2 cm in height, 80.4 ± 10.1 kg in mass and 31 ± 8.9 years of experience playing tennis) were enrolled in this initial study. Because this was a novel experimental design, a power analysis could not be reliably performed due to the unavailability of an estimate of variation from previous research. 26 However, having 10 players in the study means that each player was required to hit 40 balls for each spin level, thus providing ∼120 forehand strokes per player for device functionality and potentially 1200 forehand strokes for EMG comparison. For this reason, the number of subjects was deemed suitable for this study. To qualify, the players must have either been ranked internationally within the top 200 nationally or have obtained a professional coaching qualification, be over 18 years of age and not experienced any dominant sided, upper limb pain in the 6 months prior to testing. All players gave written consent for participation in the study. Ethical approval was obtained from The University of Sydney (Protocol 2019/434). All testing was performed by the same researcher at local tennis clubs.
Players were required to hit forehand strokes following the height guideline of three ball spin levels (flat, topspin and lob) 11 during an on-court testing session (Figure 1(b)). For flat, the ball must have travelled under a rope placed 0.6 m above the height of the net. For topspin, the ball must have travelled over this rope. For the lob, the ball must have travelled over the height of a 3.5 m pole positioned 2 m behind the opposite side of the net to the player, in a straight line between the hitting and target zone. Before the hitting phase, players were instructed to perform 10 air swings mimicking their forehand technique for each spin level. The air swings were collected to act as a base-line control for comparison with the data when the ball was hit. The impact point for each forehand stroke was determined by the rapid saturation in the Z-axis in the accelerometer trace.
The ball exit speed (in this study defined as vectorial sum of the horizontal and vertical velocities) corresponding to each hit was measured using a Head Tennis Sensor® (Head/Penn Racquet Sports, Arizona, USA) which replaced the butt cap of the tennis racket (Head Graphene 360 Instinct MP, 4 3⁄8 inches, 300 g). The recorded speed (kph) was displayed on the accompanying mobile phone application after each hit and was later used for statistical analysis. The player’s forehand must have landed in the target area (back diagonal cross-court square) and have correctly followed the height guideline to have been included for analysis (Figure 1(b)).
New tennis balls (Wilson Tour Premier) were ejected from a ball machine (Lobster Elite Three, Lobster Sports, California, USA) (80 kph) every 8 seconds during the warm-up and 12 seconds during testing. The ball machine was located on the opposite baseline to the participant and 2 meters towards the center mark from the singles line (Figure 1(b)).
All players were required to complete a guided 10 minute warm-up of hitting forehands at different spin levels, using testing height conditions. For the testing phase, each player was required to hit 4 series each comprising 10 cross-court forehand strokes using their preferred forehand grip position. This was repeated for the flat, topspin and lob spin levels in a randomized order between players. The tester stood next to the ball machine and noted for each hit whether it would be included for analysis and its corresponding ball speed. When hitting the ball, the players were asked to hit at a pace that was realistic of match conditions with increased accuracy (i.e. hitting with control over the ball instead of trying to hit winners). There was a 30 second rest between each series and a 5 minute rest between each spin level.
Different forehand grip positions influence the alignment of the wrist at impact and the kinematics of the forehand stroke. 27 Therefore, the forehand grip position of the player was determined by marking the player’s dominant hand in two positions (base knuckle of the index finger and the heel pad of the palm) 28 (Figure 2(a)) and observing where they held the racket during the forehand stroke. Depending on which racket handle bevel number (Figure 2(b)) the marks rubbed off onto during testing, the player’s grip position was determined 28 (Figure 2(c)). The original manufacturer replacement grip was replaced with a Babolat® leather replacement grip on the handle of the racket and a new white Wilson Pro Overgrip® was placed over this for each player. When uncertainty occurred, the bevel of the mark associated with the base of the index knuckle was used. Of the ten players, four players used an eastern forehand grip, four players a semi-western grip and two players a continental grip.
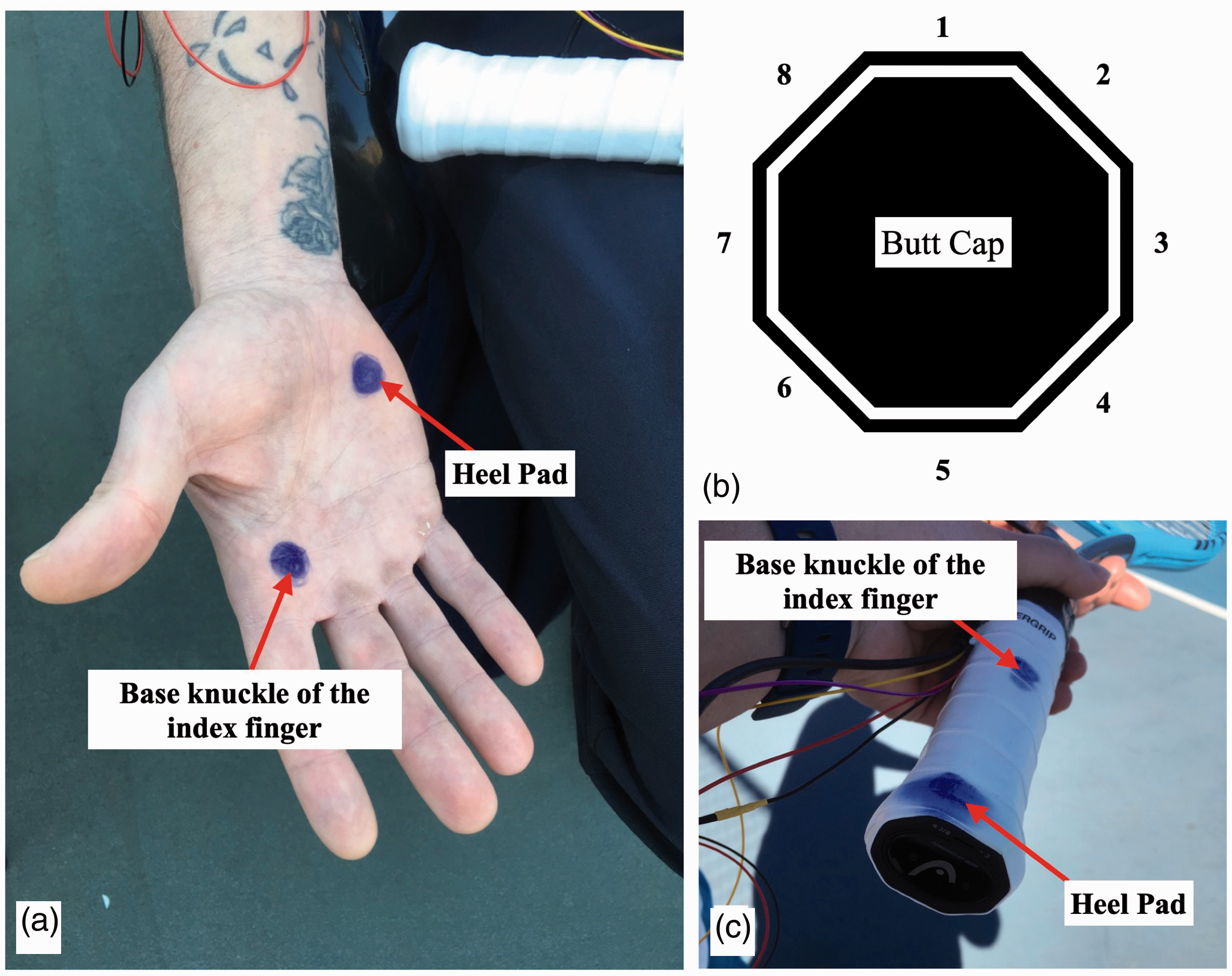
The preferred forehand grip position of the player was determined by marking the player’s dominant hand in two locations – at the base knuckle of the index finger and the heel pad (a) prior to the commencement of testing. Depending on the racket bevel number (b) associated with the marking location observed after testing (c), the player’s grip position was determined. The bevel number associated with the different forehand grips are continental (2, 1–2), eastern (3, 2–3), semi-western (4, 4) and western (5, 5) for the base knuckle of the index finger and heel pad markings respectively.
The ECRB and FCR forearm muscles were isolated through palpation and all skin areas were prepared (shaving, skin abrasion with gel and alcohol). 29 The MyoWare® sensors and electrodes (Kendallä Medi-Trace® hydrogel foam electrode, 1 1⁄4 in diameter, Ag/AgCl) were then individually placed over the muscle belly and parallel to the line of the muscle fibers of the ECRB muscle and the FCR muscle according to European standards recommendations. 29 A wristband was then placed over the sensors to additionally secure them. The MyoWare® ground electrodes were extended and placed over the lateral and medial epicondyle for the ECRB and FCR muscle respectively. TRAM’s recording functionality and appropriate MyoWare® placement were verified on each player using guided wrist extensor and flexor manual muscle tests. This verification focused on accurate TRAM sampling rates and increased levels of recorded muscle activation during these movement tasks.
Although the MyoWare® has been shown to be a cost-effective way of collecting EMG data compared with commercially available systems during both isometric and dynamic muscle contraction tasks,30,31 it is not clear how accurate they are in delineating precisely between the individual forearm extensor and flexor muscles. This could potentially be due the interelectrode distance. 32 Therefore for our analysis we accepted that our measurements were detecting components of all forearm extensor and flexor muscle activity when reporting the ECRB and FCR MyoWare® data respectively.
The EMG signal was processed by applying a Butterworth Filter order 8 (high-pass (10 Hz) and low-pass (10 Hz) frequency cut-off) to the extensor and flexor data. The 10 Hz high-pass filter was applied to the muscle data using the zero-phase digital filter MATLAB command “filtfilt”. The low-pass filter was then applied to the absolute value (full wave rectification) of the high-pass filtered data (again using the command “filtfilt”) to smooth the EMG data after rectification. These processing steps created a filtered envelope of data over time at 10 Hz which provided the EMG signal amplitude over a the given time period.
Maximum Voluntary Isometric Contraction (MVC) values were used to normalize the EMG signals. In order to determine MVC, players were seated with their backs straight on a chair feet on the floor and their dominant arm bent at 90 degrees with their fingers straight and forearm resting on a box or the arm of the chair. The height of the box was adjusted to enable the players to rest their dominant forearm on the box and maintain the bent angle of their arm at 90 degrees during the isometric contractions. In this position the players were asked to maximally flex their wrist upwards against resistance applied by the tester to their fingers and hand for 5 seconds. Following a 15 second rest, the players were then required to extend their wrist upwards against resistance for 5 seconds. The 5 seconds of contraction force consisted of a build-up of 1 second from the tester’s instruction “go”, then the tester yelled “push” 3 times at a one second interval while the player pushed against the tester at their maximum force while the tester matched their force level. This was followed by a “relax” instruction where the player relaxed their muscles. The tester’s goal was to push the player’s hand towards the ground and for the player to resist the force. No instructions were provided for players to try and maintain a certain wrist joint angle during the isometric contractions. There was a 2 minute rest between each test and the test was repeated 3 times for each muscle.
Normalization of the EMG signal was performed by dividing the recorded EMG signals during the specific testing task by the reference EMG MVC value obtained from the same muscle. 32 As a result, the peak MVC value corresponding to the low-pass filtered data of the three MVC attempts for each player was used as a reference measurement to normalize the low-pass filtered extensor and flexor data for each spin level. 32 The normalized EMG data were then expressed as a percentage of MVC for each player and spin level. For each player the peak %MVC values corresponding to the correctly hit shots (matched to the accelerometer data for timestamp conformation) were recorded and used in the subsequent statistical analysis.
Identical statistical and graphical analysis was performed on EMG and ball speed data for all three spin levels using MATLAB (R2018b). As analysis was between the three different spin levels, it was an inclusion criterion that each spin level was recorded for the players data to be included for statistical analysis. Following initial screening of the data, valid peak extensor and flexor %MVC values were available for eight and nine players respectively.
All observations were considered independent as the data were from different hits by separate players. For each muscle, the EMG data was grouped into the three different spin levels to assess the effect of the level of forehand ball spin on maximal extensor and flexor EMG activity. Similarly, the ball speed corresponding to these included extensor and flexor muscle shots were grouped into the three different spin levels for each muscle. This enabled a comparison between either the effect of the ball spin level and/or ball exit speed on the level of maximal muscle activity for each ball spin level. Initial analysis using the Lilliefors test for normality showed that the parametric normality assumption was not met for all groups therefore, non-parametric Kruskal-Wallis statistical tests and associated Multiple Comparison tests were performed. All statistical tests had a significance level of p < 0.05.
Results
The first step was the testing of TRAM using accelerometer and EMG data collection of all 10 players under realistic playing conditions. Importantly, players reported no issues with the device interfering with their technique during testing. An example of the processed TRAM accelerometer data for one player’s topspin forehand stroke when they performed an air swing and when they hit the ball can be seen in Figure 3(a) and (b) respectively. The impact point is seen in Figure 3(b) where rapid saturation in the Z-axis in the accelerometer trace compared with Figure 3(a). Accelerometer saturation can also be seen in Figure 3 due to only data within the accelerometer’s dynamic range (± 157 m/s2) being recorded. An example of the different phases of processing TRAM EMG data for finding the players peak MVC value is shown in Figure 4. For the extensor and flexor muscle activity, the peak %MVC values corresponding to the correctly hit shots (Figure 5) were recorded and used in the subsequent statistical analysis.
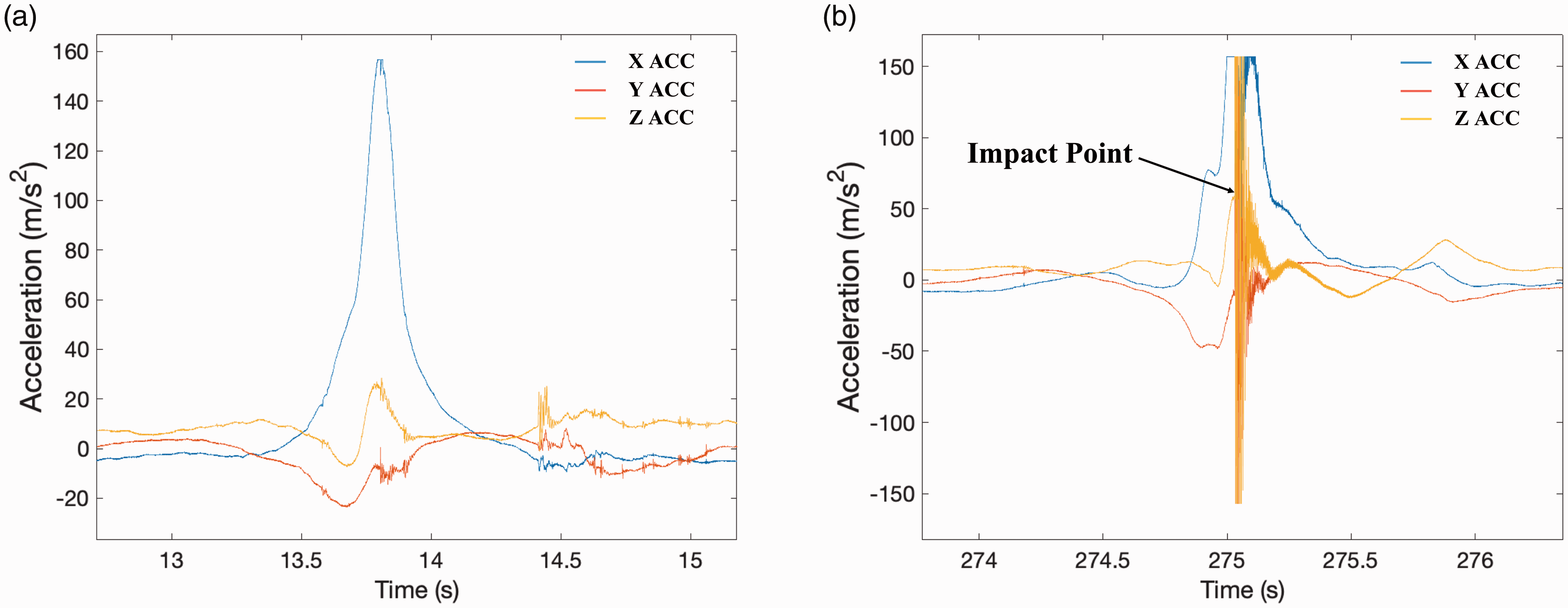
An example of processed TRAM accelerometer data for one player’s topspin forehand stroke when they performed an air swing (a) and when they hit the ball (b). The impact point is seen in (b) where rapid saturation in the Z-axis in the accelerometer trace compared with (a). Relative to the racket, the X-axis of the accelerometer was the direction along the racket from the tip to the handle, the Y-axis was the direction across the string bed and the Z-axis was perpendicular to the string bed.
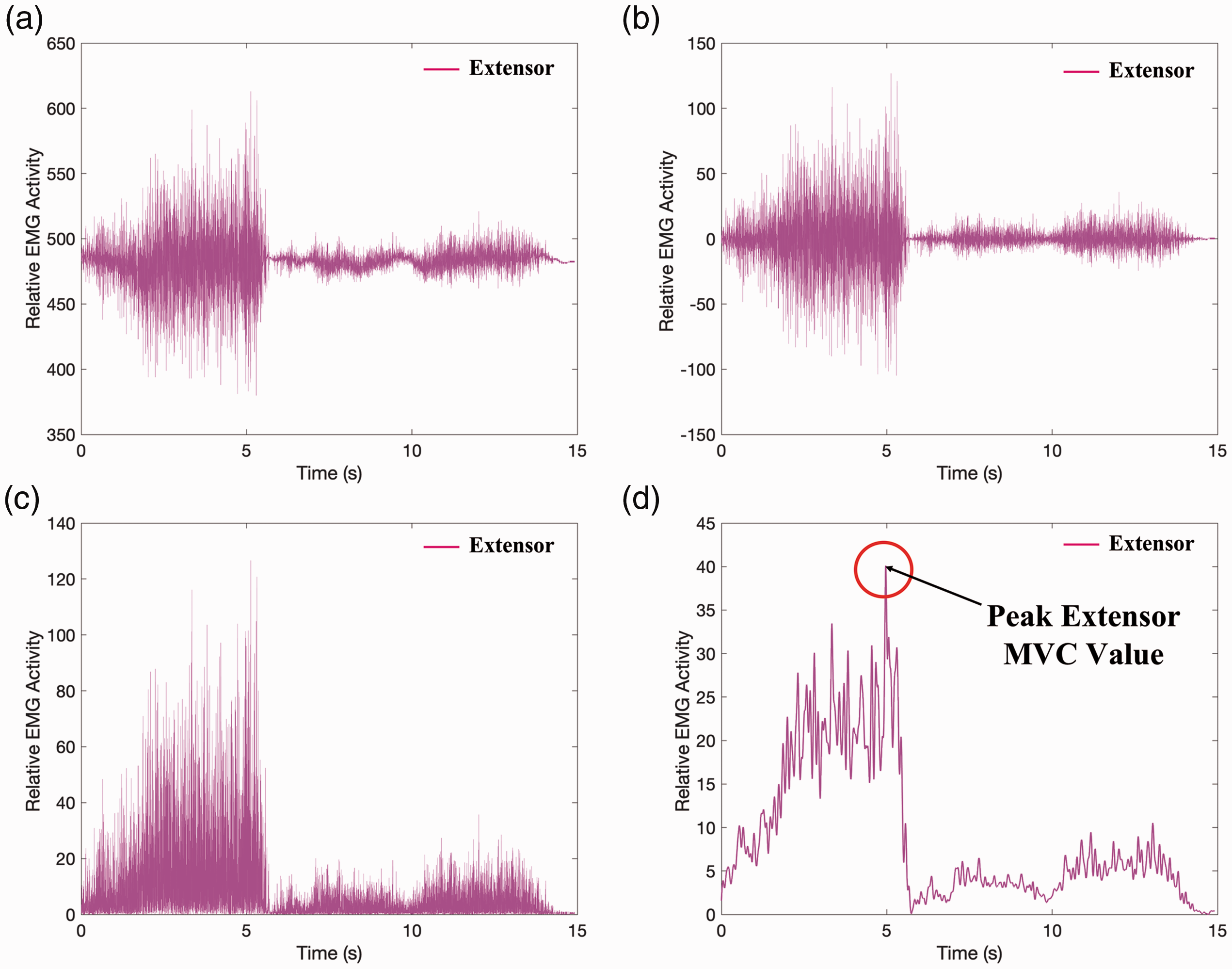
Figure showing the different phases of processing the EMG data for finding the peak MVC value. (a) Raw MyoWare® Extensor MVC data for one attempt. (b) The high-pass filtering of 10 Hz attenuates signals with a frequency lower than 10 Hz (including the direct current voltage) and changes the data to oscillate around zero. (c) The absolute value of the high-pass filtered data, converts all negative amplitudes are into positive amplitudes. (d) The low-pass filter smooths the curve by attenuates signals with a frequency higher than 10 Hz. The highest peak value from this curve for the three MVC attempts were used to normalize the player’s hitting data.
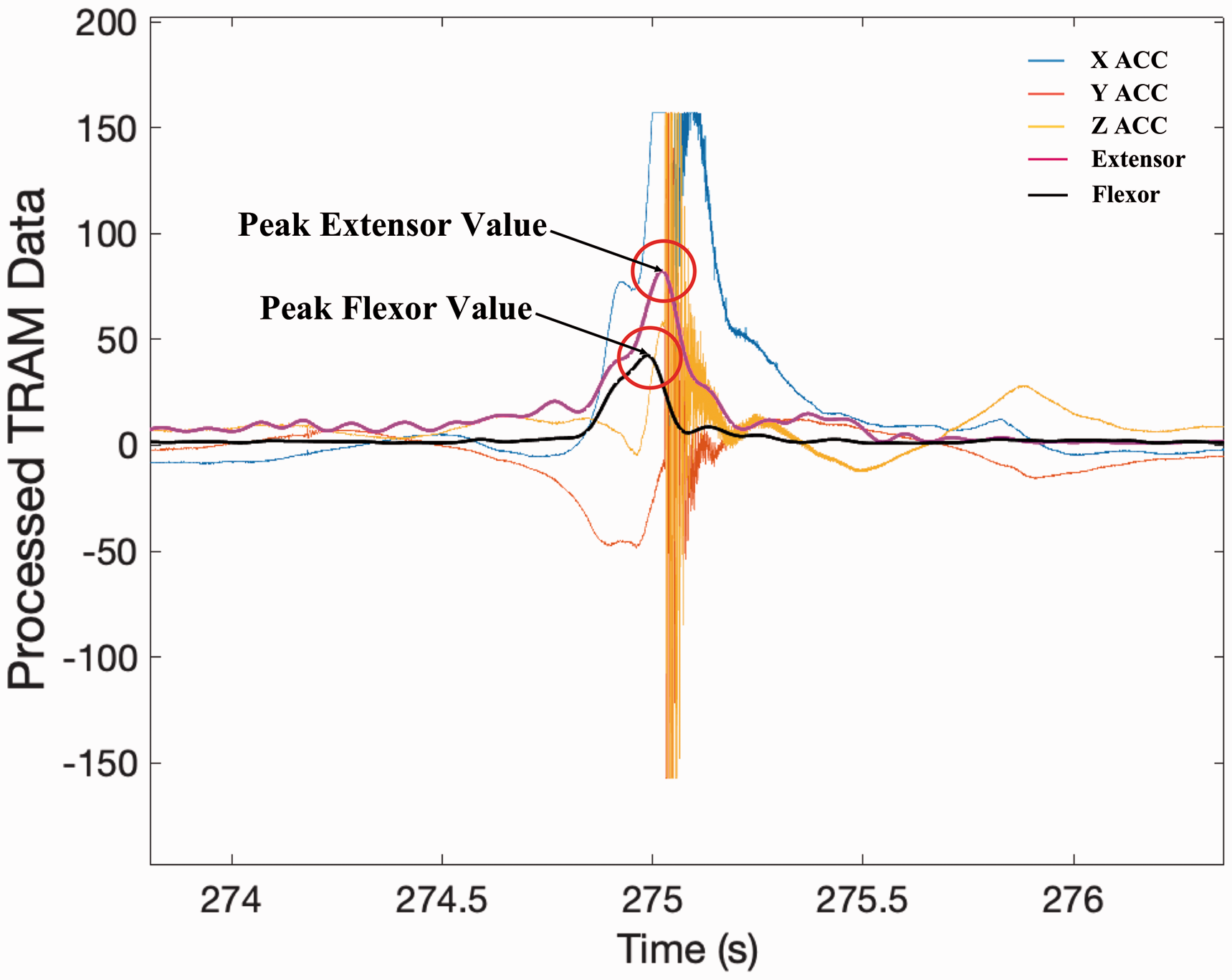
An example of processed TRAM data and normalized EMG values for one player’s topspin forehand stroke. Corresponding peak extensor and flexor values are also indicated on the trace.
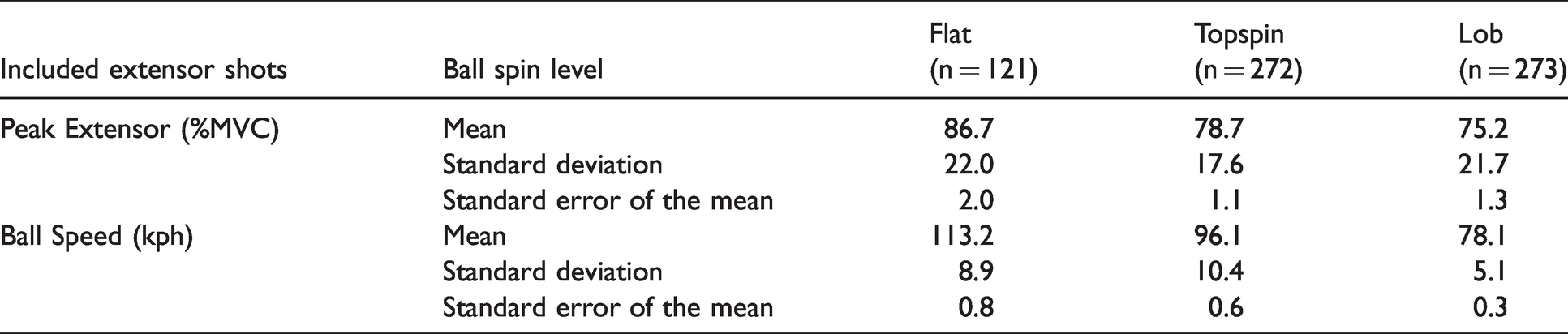
We first analyzed the peak extensor %MVC values corresponding to the correctly hit shots (flat = 121, topspin = 272 and lob = 273) by 8 players (Table 1). The Kruskal-Wallis test showed significance (p < 0.001) between all three spin levels. The Post-Hoc test showed there were significant differences between the flat and topspin spin levels (p < 0.01) and flat and lob spin levels (p < 0.001). Importantly, we found that hitting the ball flat corresponded with a significantly higher level of extensor maximal activity when compared with hitting the ball with either the topspin or lob spin levels (Figure 6(a)). In contrast, when we analyzed the peak flexor %MVC values corresponding to the correctly hit shots (flat = 125, topspin = 301 and lob = 303) by 9 players (Table 2), the Kruskal-Wallis test showed there were no significant difference between the three spin levels (Figure 6(a)).
Peak extensor %MVC and ball exit speed values corresponding to the correctly hit shots for each spin level (n = 8).
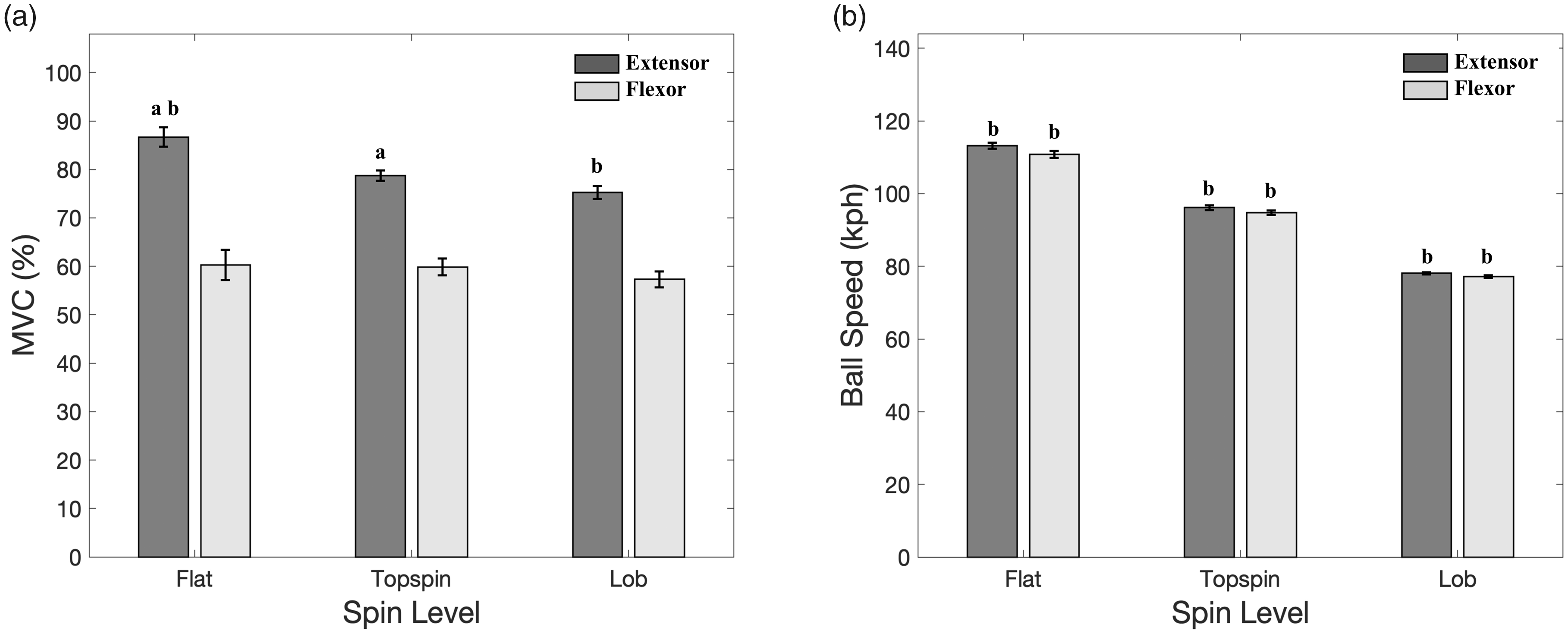
Statistical and graphical analysis of peak EMG values and ball speed data for included shots. (a) Peak extensor (n = 8) and flexor percentage MVC (n = 9) values corresponding to correctly hit shots for all three spin levels. (b) Ball speed for correctly hit shots corresponding to successfully recorded extensor (n = 8) and flexor (n = 9) values for all three spin levels. Bars represent mean ± SEM. Corresponding letters represent significant level between the different spin levels: a(p < 0.01) and b(p < 0.001).
Peak flexor %MVC and ball exit speed values corresponding to the correctly hit shots for each spin level (n = 9).
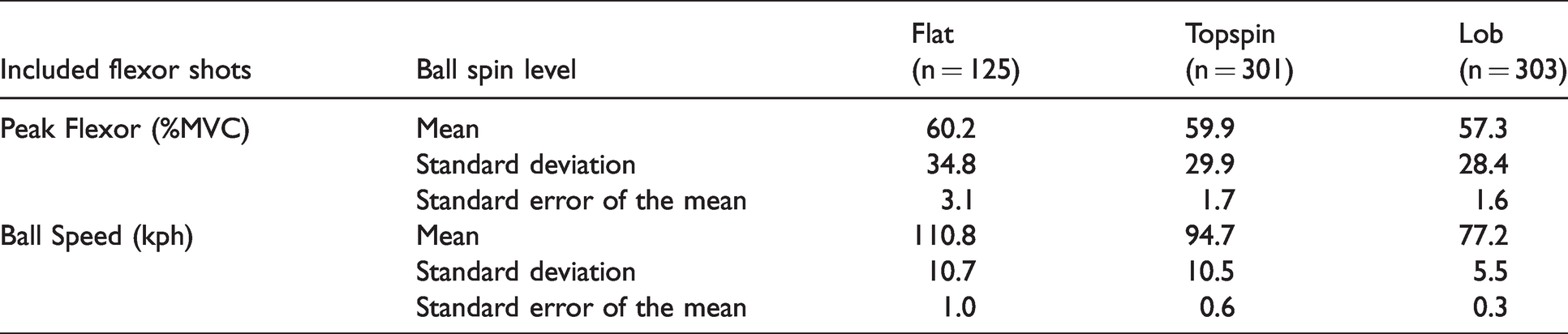
We then examined for each muscle the effects of ball speed corresponding to the included shots for the three different spin levels (Tables 1 and 2). Kruskal-Wallis tests showed significance (p < 0.001) for the ball speed corresponding to the included shots for each muscle group. The Post-Hoc tests also showed there were significant differences between the ball speed for the flat and topspin (p < 0.001), flat and lob (p < 0.001) and the topspin and lob (p < 0.001) spin levels. The flat hits had the highest ball speed, followed by the topspin with then lob having the lowest speed (Figure 6(b)).
Discussion
Due to the repetitive nature of the forehand stroke, professional and recreational tennis players are at significant risk of developing elbow tendinopathy. Higher levels of forearm muscle activity leads to increased vibrational transfer from impact being transferred efficiently and directly to the myotendinous junction causing repeated microtrauma and increased risk of elbow tendinopathy development in tennis players. Our results revealed that spin level did have a significant effect on the level of maximal extensor activity in the flat stroke compared with the topspin and lob spin levels. This suggests that potentially players who prefer hitting the ball with topspin may be at reduced risk of developing LET compared with those who prefer hitting flat. Additionally, although the ball speed associated with these correctly hit forehand shots was highest with the flat spin level followed by topspin and lob, this trend was not observed across all three corresponding spin levels for both muscles. This suggests that decreased ball speed when combined with increased levels of topspin does not affect the level of maximal extensor or flexor activity in experienced tennis players.
A previous study by Rogowski et al. 15 reported a significant decrease in ECR and FCR activity between flat and topspin inside-out forehands in junior players hitting both flat and topspin spin levels. Our extensor results are in agreement, however we did not observe any difference in flexor activity between any of the three spin levels (flat, topspin and lob). This difference may be due to kinematic differences associated with the different forehand spin levels, ball placement or muscle cross-talk. For example, the wrist joint remains hyperextended at impact9,11,12 while the peak palmer flexion angular velocity increases from flat to topspin to lob spin levels for the forehand stroke. 9 The ball is also required to be hit further forward when hitting the forehand cross-court 12 and with less wrist abduction when compared with hitting an inside-out forehand. 33 Both of these effects would result in different forearm muscle activation patterns. Furthermore, the study by Rogowski et al. 15 was performed on junior players who would have had less developed muscle groups compared with the adult players in the current study. In the case of less developed muscle groups, it is known that significant EMG signals produced by neighboring muscles can influence the recorded electrode readings, an effect referred to as physiological crosstalk. 34
Our finding that flat forehands have a significantly higher ball speed than topspin forehands is in agreement with a study by Genevois et al. 10 Although faster racket head velocity results in a greater speed of the ball leaving the racket, 12 as mentioned previously, the study by Rota et al. 14 found no significant difference in ECR and FCR activity levels for flat forehands hit at different speeds. This is somewhat surprising given the key role of FCR activation in wrist flexion, 13 the motion players report to use intentionally in order to increase ball speed 35 and topspin on the forehand stroke. 9 Although high levels of forearm muscle activity occur during the forehand stroke to stabilize the wrist, 7 differences in kinetic energy transfer may potentially not lead to significant changes in muscle activity in this case.
Although coaches often encourage players to use the forehand grip position which feels most comfortable, other injuries in the wrist and hand have been associated with the different forehand grip styles. A study by Tagliafico et al. 28 found lateral-side wrist injuries have been associated with the eastern grip, while medial-sided wrist injuries have been associated with the western and semi-western grip. They also found a significant difference in the age of the players with the wrist injuries, with the older players having used the eastern grip while the younger players having used semi-western or western, reflecting generational changes in techniques. A study by Balius et al. 36 found stress fractures of the second metacarpal in the hand were associated with increased tennis playing intensity and may be associated with use of the semi-western or western forehand grip. Although previous studies typically grouped the different forehand grip positions together,10,14 the separate analysis of the different forehand grip positions on the potential development of elbow tendinopathy could provide vital information for coaches when recommending the different forehand grip positions.
There are some limitations with the current study. For example, the EMG data was normalized to a standardized isometric MVC task. Although this is an acceptable method of normalization, it may present as a potential limitation given the accuracy of whether the participants performed their true maximum MVC is unknown.37,38 This limitation can potentially be address in future studies through a normalization reference measurement being obtained by players hitting forehand strokes at their maximum speed and spin for each ball spin level condition.
Additionally, previous MyoWare® validation studies were performed on the quadricep muscles of the leg which have a much larger muscle belly than the forearm muscles.30,31 Crosstalk between the two MyoWare® sensors would be minimal as suggested by a study from Mogk and Keir 39 which found that gripping tasks with forearm rotation resulted in minimal crosstalk between forearm extensor and flexor electrode pairs. However, the significance of the size of the muscle belly is that physiological crosstalk is commonly associated with surface EMG studies when smaller muscles (such as muscles in the forearm) are being studied due to the importance of the interelectrode distance. Although the commonly used European standard recommendations suggest that the interelectrode distance should be 20 mm, 29 the MyoWare® has a fixed interelectrode distance of 30 mm. This limitation can be address in future studies through the addition of the MyoWare® sensor cable electrode pads which can then be adjusted to the recommended interelectrode distance.
Another limitation of TRAM was the saturation of the accelerometer due to the measured g forces associated with impact being larger than the accelerometer’s dynamic range (Figure 3). Although previous forehand studies using low-cost accelerometers (±8 and 16G) did not appear to show saturation, this difference could potentially be due to their lower sampling rates (200 - 833 samples per second).40,41 It has been suggested that frequencies in the range of 80-200 Hz are likely to contribute to the development of elbow injuries in tennis. 18 Future studies using an accelerometer with a higher g force range will enable us to do a Fast Fourier Transform on the data of the vibrational components from impact.
In conclusion, this study is the first to develop a novel wearable device to investigate the difference in forearm extensor and flexor activity between the three spin levels on the forehand stoke. We found a significant difference in extensor activity between flat versus topspin and flat versus lob spin levels but no significant difference in flexor activity between all three spin levels. However, despite significant difference in the ball speeds between all three spin levels, these differences were not reflected in the level of extensor and flexor maximal muscle activity. Although this is a preliminary study and further work is required, this study shows that wearable devices can be used to allow coaches to customize the training program for each individual player and identify facets of the players playing style that could predispose to long term injury. For example, our current data suggests that regardless of the player’s preferred playing style or speed they hit the ball, coaches and clinicians should recommend tennis players to hit their forehands with topspin, to reduce their maximal level of extensor activity and hence less vibrational transfer to the elbow. This could potentially reduce the player’s risk of developing LET.
Footnotes
Acknowledgements
The authors would like to thank all players who participated in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.