
Abstract
Background
Padel has spread rapidly in several countries around the world. Although this racket sport seems to have several health benefits, the number of scientific papers on this sport is still very few. This scoping review aimed to systematically map the evidence regarding injuries in Padel players by identifying, synthesizing, and assessing the studies currently existing in the scientific literature.
Methods
This scoping review was conducted following the guidelines provided by the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews and the Population, Concept, Context framework was adopted. Articles were collected from PubMed, Web of Science, and Scopus.
Results
A total of seven studies were included in this review. The most frequent injury location is in the elbow, followed by shoulder, and low back. As for lower limbs, knee represents the most affected body region. Although not all the studies included described the type of injuries, tendon, joint, and muscle are the body structure most injured.
Conclusion
This scoping review can aid in a better comprehension of the location and type of injuries that occur in Padel players. However, it is worth noting that all the studies existing concerns nonprofessional athletes. Hence, these findings could be useful to coaches as they add knowledge on the risk of injury in padel that can allow the planning of suitable training programs for amateur and recreational players in order to prevent injuries.
Introduction
Padel, initially called Paddle or Paddle Tennis, is a racket sport born in Mexico in 1962. 1 This sport has spread rapidly in Spain over the last few decades and is now becoming one of the most popular sports in several countries around the world. 2 As a matter of fact, currently more than 60 federations have been founded and recognized all over the world. 3 The growing interest in this sport is also accentuated by the great popularity that national and international circuits for professional athletes are gaining (first of all the World Padel Tour).
Padel is played in doubles on a court with size of 20 m in length and 10 m in width and on a ground surface that can be composed of artificial grass, synthetic material, or cement. 4 The court is enclosed by metal fences on the sides and glass walls at the end and at the corners of the court. The rules are almost the same as tennis with the difference that it is possible to play the ball after it bounces off fences or walls. Additionally, in padel is used a shorter racket with an unstrung but flat head perforated by cylindrical holes and made of foam, fiberglass, or carbon fiber and of different shape (i.e., diamond, drop, and round).
Padel is a high-intensity intermittent sport which combines high-frequency and low-intensity athletic actions and requires specific physical demands, similar to tennis, as well as related technical–tactical characteristics to obtain the highest performance possible and to prevent the risk of injury.5–8 However, compared to tennis as neither high physical fitness level nor high technical–tactical skills are required to start playing padel. A recent narrative review reported that the physiological demands to which Padel players are subjected during a match are lower than tennis players showing a mean oxygen consumption (VO2) of approximately 40–50% of the VO2 max and a mean heart rate (HR) of between 140 and 160 beats/min (70–80% of the HR max). However, the authors pointed out that different intensity patterns may exist depending on the level of players. 9 Moreover, the long length of rallies makes the practice of padel enjoyable.10,11 As a result, this racket sport is widely practiced also in amateur and recreational form, and it seems to have several health benefits.12–14 For example, middle-aged adult women who practice padel regularly show greater physical fitness conditions than sedentary and better physical characteristics such as lower waist and hip circumferences and a lower thigh skinfold. 12 However, the risk of injury is, per se, intrinsic to sports practice at any level and it is influenced by several factors such as physical fitness and the level of practitioners. As a consequence, the risk of injury can be higher in recreational contexts among amateur players, especially with a low experience of practice. In itself, the repetition of unilateral gestures, typical of padel, could lead to asymmetries or overuse injuries. 9 Moreover, it seems that there is a higher incidence of injuries in those amateur players who do not perform joint mobility exercises, stretching, or specific strength exercises. 15 A recent overview of the literature, which summarized some aspects of padel, suggested that in Padel players most injuries affect the lower limbs (ankle sprains are the most common injuries) followed by upper limb injuries (shoulder and elbow are the most affected regions with rotator cuff syndrome, subacromial impingement, bursitis, and epicondylitis as the most common injuries). 5 Of interest, the association between some risk factors such as the use of padel-specific footwear or the type of racket and the risk of injury is not well understood.16,17
The growing interest in padel has led some research groups to conduct studies in order to better understand different aspects of this sport including performance,8,18 injury,16,17 biomechanics, 19 match analysis,11,20 and physical, physiological, and psychological profile of players.14,21,22 Since this sport has become very popular first in Spain, to date most of the research has been developed in this country and some of these studies are in Spanish language.23–25 However, the number of scientific papers on this sport science area is still very few, and based on these premises, the following research question was formulated: what are the scientific knowledge on injuries in Padel players?
Hence, this scoping review aimed to systematically map the evidence regarding injuries (location and type) in Padel players by identifying, synthesizing, and assessing the studies currently existing in the scientific literature. This scoping review could be useful to coaches in order to prevent injury in this emerging racket sport.
Materials and methods
This scoping review was conducted following the guidelines provided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR). 26
Eligibility criteria
The Population, Concept, Context (PCC) framework was adopted to select the studies for this scoping review.27,28 In particular, the following eligibility criteria were used: (1) Padel players as population; (2) any information on injury in Padel players (incidence/frequency of injury, type of injury, location of injury, risk of factors) as concept; and (3) Padel players of any level/age/gender as context.
Studies were eligible if they were original articles written in English and published from inception to January 2023. Studies were excluded if they were reviews, meta-analyses, conference proceedings, opinion pieces, letters, editorials, commentaries, and books.
Search strategy
The databases searched to identify potentially relevant studies were PubMed, Web of Science, and Scopus using the search field “title” in each database. The search strategy matched the terms “padel” and “paddle tennis” with the term “injur*” using the Boolean operator “AND.” In detail, “padel” AND “injur*”, “paddle tennis” AND “injur*.”
Study selection
The list of studies from each database was exported into EndNote X8 software for removing all duplicate records. Then, two independent investigators worked independently for screening records by title and abstract. Hence, studies were examined by full text to assess their eligibility for inclusion. In case of disagreement on study selection between the investigators, a third investigator was involved if needed.
Data extraction
Data regarding “first author and year of publication, aim of the study, sample size, number of males and females, participants’ age, participants’ level, participants’ practice/week, participants’ experience, methods for injury data collection, and main outcomes” were extracted by one reviewer and inserted into a Microsoft Excel (Microsoft Corp, Redmond, Washington) spreadsheet. Data extracted were synthesized and presented as a “map” in a table and a descriptive narrative synthesis was used to discuss the results.
Results
Study identification
A total of 31 records were identified through searching multiple databases and after duplicates removed a total of 16 records were identified. Based on title and abstract screening, three records were excluded (two of them were reviews and one because it investigates injury in padel coaches). Hence, 13 full-text articles were retrieved and assessed for eligibility. Of these, six were excluded for the following reasons: two were conference proceedings and four were articles in other languages (i.e., three in Spanish and one in Sweden). The remaining seven studies were included in this review (Figure 1).
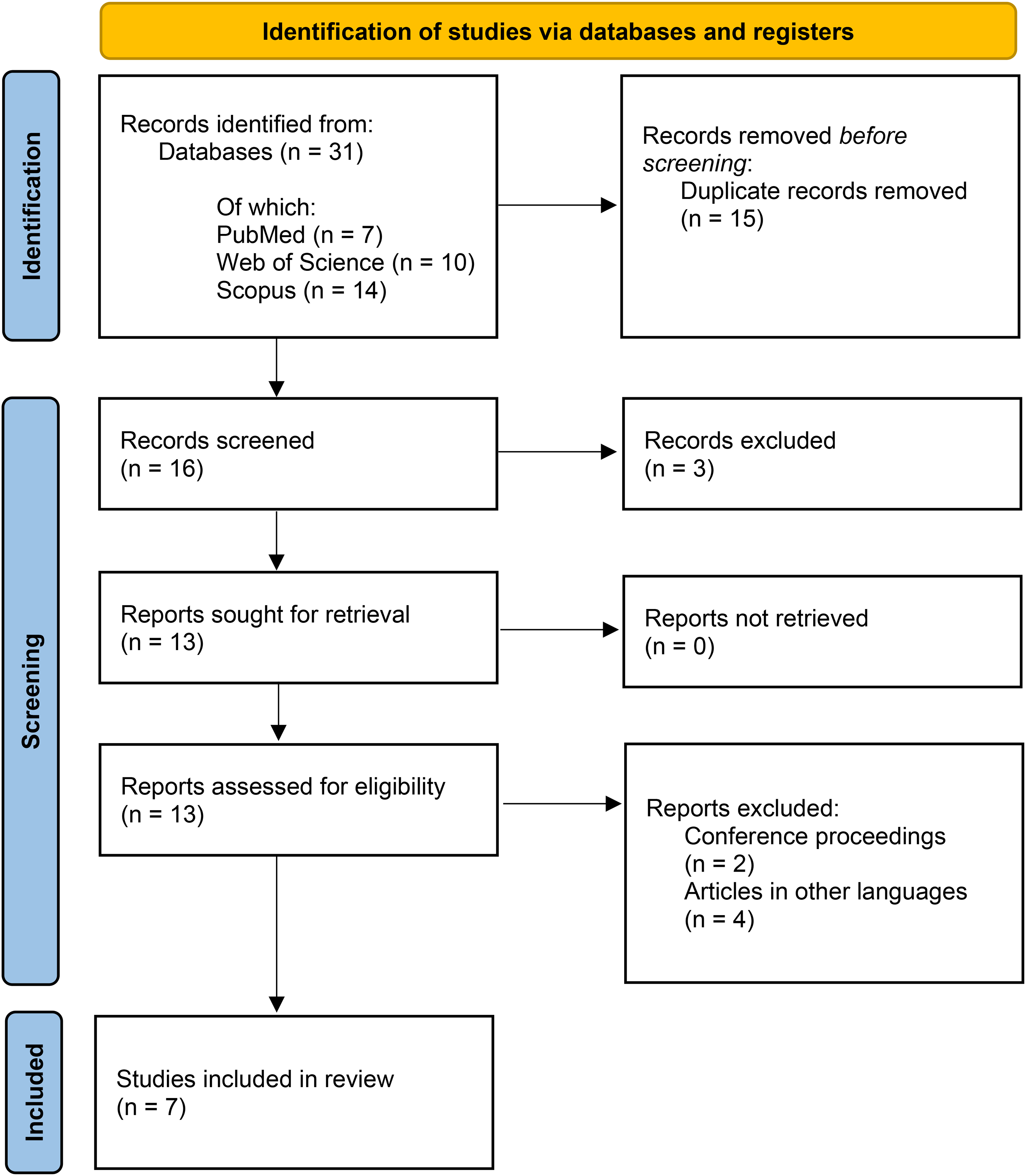
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases and registers only. From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71. For more information, visit: http://www.prisma-statement.org/.
Study characteristics
Characteristics of the studies included in this review are reported in a table (Table 1).
Characteristics of the studies included.
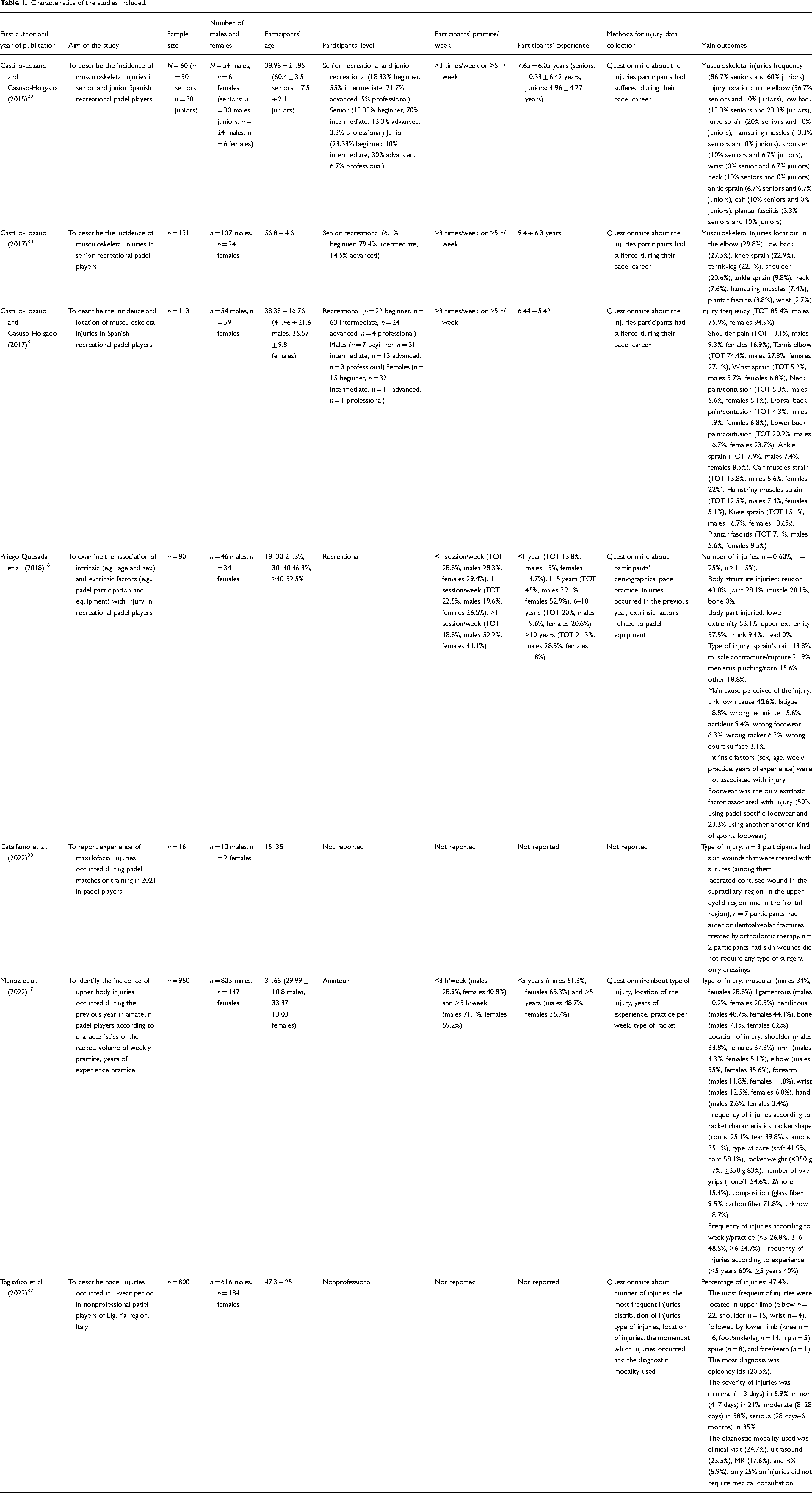
Among the studies identified, n = 5 were epidemiological, observational, descriptive, retrospective cross-sectional studies,16,29–32 n = 1 was a cases report, 33 and n = 1 adopted an empirical methodology. 17
Studies considered represented data from 2150 participants (male = 1690, female = 460) ranging from junior to senior (age range from 15 to 60 years). Across studies, participants’ level was amateur/recreational/nonprofessional. In the studies by Castillo-Lozano et al., details about recreational players were provided by specifying that participants included beginner, intermediate, advanced, and professional players.29–31 Participants’ practice/week and participants’ experience were not reported in all the studies considered. Apart from the study by Catalfamo et al. which was a case report, 33 all studies employed the use of questionnaires to collect information about injuries.
Study outcomes
Injury location
In all, almost all studies suggest that the most frequent injuries were located in the elbow. In detail, the study by Castillo-Lozano et al. showed that injuries frequency in the elbow was the 74.4% in a sample of n = 113 Spanish recreational Padel players followed by low back pain (20.2%). 31 Similar results were found by the same authors in another research in which the most frequent musculoskeletal injuries in senior recreational Padel players were located in the elbow (29.8%) followed by low back pain (27.5%). 30 This trend is confirmed by another work involved senior and junior recreational Padel players in which the authors reported that the most frequent body region injured was the elbow (36.7%), followed by knee sprain (20%), and low back pain (13.3%) in senior players; low back pain (23.3%), followed by elbow injuries (10%), and knee sprain (10%) in junior players. 29 Similarly, Munoz et al. found that the frequency of injuries in the elbow has been reported in 35% of male amateur Padel players, representing the most frequent body region injured followed by shoulder injuries (33.8%); the reverse order of location of injury for female amateur Padel players was detected showing shoulder as the most injured body region and elbow as second, although the percentage difference was almost equivalent (37.3% and 35.6%, respectively). 17 Tagliafico et al. reported that the most frequent of injuries were located in upper limb (with the majority of them referred to elbow followed by shoulder) and lower limb injuries being after with the knee as the most affected body part. 32 Contrarily, the only study that found results not in consistent with the previous studies was that of Priego Quesada et al. in which authors found in the lower limbs the highest percentage of injuries followed by those in the upper limbs (53.1% and 37.5%, respectively), although details on upper and lower limbs regions are not reported. 16 As for the study by Catalfamo et al., regarding maxillofacial injuries in Padel players, authors reported n = 5 cases of skin wounds and n = 7 participants with anterior dentoalveolar fractures. 33
Injury type
Although not all the studies included described the type of injuries, Munoz et al. reported tendinous and muscular were the most frequent in both male and female players (48.7% and 34% vs. 44.1% and 28.8%, respectively). 17 Similarly, Priego Quesada et al. found the same results with the joint as another body structure most injured (tendon 43.8%, joint 28.1%, muscle 28.1%). 16 Tagliafico et al. reported the epicondylitis as the most frequent diagnosis (20.5%). 32
Injury factors
Only two studies examined the association between extrinsic and intrinsic risk factors and injuries in Padel players. Priego Quesada et al. found that intrinsic factors such as sex, age, practice/week, and experience were not associated with injury and, among the extrinsic factors, footwear was the only associated with injury. 16 Particularly, the authors found the highest frequency of injuries in Padel players wearing padel-specific footwear than those who wore another kind of sports footwear (50% vs. 23.3%, respectively). Moreover, the authors detected that the type of racket used was not a risk factor for injury. This last outcome is in disagreement with the study by Munoz et al. in which authors found differences in frequency of injuries according to racket shape (round 25.1%, tear 39.8%, diamond 35.1%), type of core (soft 41.9%, hard 58.1%), racket weight (<350 g 17%, ≥350 g 83%), number of over grips (none/1 54.6%, 2/more 45.4%), and composition (glass fiber 9.5%, carbon fiber 71.8%, unknown 18.7%). 17 Furthermore, the authors determined differences on frequency of injuries according to practice/week (<3 26.8%, 3–6 48.5%, >6 24.7%) and experience (<5 years 60%, ≥5 years 40%).
Discussion
Considering the rapidly growing popularity of padel, the aim of this scoping review was to systematically map the evidence regarding location and type of injuries in players of this sport. In fact, as with other racket sports, padel also seems to have several health benefits.12–14 However, since padel is a relatively recently born sport, there is a need to understand the epidemiology of the type and location of injuries that occur in padel.
The first important evidence to highlight is that there are no studies that have examined the injuries that occur in professional Padel players, and this suggests that it is not possible to have complete knowledge about injuries in this sport.
Moreover, it should be noted that considering all the studies, the percentage of amateur/recreational/nonprofessional female players is much lower than that of males, limiting the possibility of defining specific gender differences on injuries in padel because female players cannot be completely representative.
Other aspects to be noted are that most of the studies are retrospective cross-sectional, one study is a case report, and one study adopted an empirical methodology. This means that no experimental studies have been conducted on Padel players for investigating injury but, to date, only observational studies exist. Furthermore, except for that of Catalfamo et al., 33 all the studies used a questionnaire to collect data about injuries increasing the risk of reporting bias. Indeed, the study by Catalfamo et al. reported case reports on maxillofacial injuries that occurred during padel matches or training. 33 The authors indicate that these injuries occurred due to the impact of the racket bouncing against the glass wall of the padel court. Indeed, during the game, the bounce of the racket occurs mainly because the players try to hit the ball close to the glass wall.
In all, evidence suggests that the most frequent injury location is in the elbow (mainly epicondylitis). Results of the present review indicate that also in padel, as with other racket sports, the elbow represents the most affected injury location. 34 This finding is in line with several studies conducted in tennis, where it has been found that epicondylitis (or tennis elbow) is the main overuse injury of the upper limbs, due to the repetitive forces, loads, and motions to which the elbow is subjected while playing tennis, particularly in recreational players.35,36 Lateral epicondylitis (tennis elbow) is seven times more frequent than medial epicondylitis (golfers elbow) and up to 50% of all regular tennis players suffer from this overuse injury. 37 This occurs because of, in biomechanical analysis, the elbow plays a central role in the kinetic chain of the strokes in racket sports linking the body with the racket. 35 In fact, it allows the transfer of kinetic energy from the body to the racket. 35
Subsequently, the other frequent injuries in Padel players are located in the shoulder. In padel, this is particularly emphasized in power strokes, which are overhead (e.g., smash and tray). 18 The shoulder is particularly involved during the strokes in all the overhead sports such as in tennis. 38 Indeed, among the specific tennis injuries, the prevalence of shoulder injuries is also common due to repetitive use, as occurs for the elbow injuries. 34 As reported in the review by Abrams et al., it seems that shoulder injuries are related to a subtle instability in younger players while the rotator cuff injuries are more common in older player. 34 In a recent review, a research group found that the rotator cuff injuries are caused by microtrauma and internal impingement in younger players leading to tearing in older players. 38
Based on the studies included in this review, other injuries in Padel players are in the low back and, as for the lower limbs, the knee (mainly knee sprain) is the most affected body region. Also, for analyzing these injuries, the tennis’ kinetic chains associated with the repetitive strokes should be taken into account. In fact, there are two types of kinetic chains in tennis which, in our opinion, given the similar nature of these two sports, can also be transposed to padel. These are related to the different strategies of body segments coordination used according to the strokes. 39 In detail, in power strokes and groundstrokes, a higher number of body segments are required to be coordinated in order to produce a high racket speed at impact. 39 In particular, this kinetic chain required leg drive and trunk rotations. Contrarily, in precision strokes such as the volley at the net, a lower number of body segments are required. 39 Moreover, knee injuries in padel could be explained by the sudden running inversions, rotation, and stopping that occur at a high frequency in this racket sport. 16 Moreover, it should be mentioned that the ground surface, which can be composed of artificial grass, synthetic material, or cement, can influence on these types of injuries.
Conclusion
This scoping review systematically mapped the evidence regarding injuries in Padel players. Results suggest that the most frequent injuries were located in the elbow followed by shoulder and low back. As for lower limbs, knee represents the most affected body region. As for the type of injuries, tendons, joints, and muscles seem that are the body structures most injured.
Strengths and limitations
The main strength is that, to the best of our knowledge, this is the first scoping review that systematically mapped the evidence regarding injuries in Padel players.
It is worth noting that all the studies existing and included in this scoping review concern nonprofessional athletes and that the percentage of female players is much lower than that of males. These aspects limit the possibility to analyze in depth and determine specific level and gender differences in injuries in padel. Moreover, it should be noted that most of the studies included are retrospective cross-sectional, one study is a case report, and one study adopted an empirical methodology. Further studies should, therefore, focus on these aspects as the literature is lacking.
Practical implications
Since this racket sport is widely practiced in amateur and recreational form, the results of this scoping review could be useful to coaches as they add knowledge on the risk of injury in padel that can allow the planning of suitable training programs for amateur and recreational players in order to prevent injuries.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.