
Abstract
Sports coaches play a key role on sports participants’ health, due to the informal educational dimension inherent to sport, but feel limited in terms of health promotion (HP) implementation in their practices. The aim of this systematic mapping review is to identify coaches’ HP skills, which are already used in daily practice, and which they need to acquire, as well as leverages and barriers to their use. Based on PRISMA-P guidelines, six databases were searched using keywords close to sport coaching and skill and health. Inclusion criteria were 1) targeting organized grassroots sport coaches, 2) peer review English original articles, 3) discussing coaches’ skills. Among the 2485 studies found, 56 were included based on a double-blind selection. Analysis included: thematic coding of skills, followed by a categorization based on health determinants (social, environmental, economic and organizational) mobilized and an analysis of the types of health (social, physical and psychological) affected. Results identified ten coach's HP skills: sport participant management, health support, education, evaluation, motivation, cooperation, prevention, communication, role modeling and self-management. These skills are mostly targeting sport participant psychological health. Barriers included coaches’ own definition of the boundaries of their role, pressure from sport participants’ relatives. Leverages to skills use were self-confidence, attending training, getting experience, increasing knowledge or adhering to guidelines. Coaches’ HP skills are close both internal (e.g., self-management, role modeling) and external (in relations to sport participants or partners) and target mostly psychological health.
Introduction
Coach is a member of the sport club (SC) who undertakes a multitude of support activities with the role of developing and optimizing the training schedule to develop and refine physical, technical and sport participants’ tactics through communication and support in and out of the environment. 1 Scientific literature has shown that in the exercise of their main functions, coaches notably carry out tasks of conduct practices, building relationships or shape the environment which will require them to develop skills such as planning, management and even needs analysis. 2 In the present work, as specific attention will be given to grassroots coaches, as key gatekeeper to sports practice for all. Scientific literature around Health Promotion (HP) in SC has shown that grassroots coaches (i.e., more focus on recreational activities) can contribute through the informal and educational nature of sport to better physical, mental and social health.3,4 In other words, in the context of recreational training, grassroots coaches are key actors supporting sports participants “to make healthier choices, easier choice” and gain control over the health, by creating a positive health context through their interpersonal behavior's styles 5 and their practices’ management and organization. 1
This means that coaches contribute to HP, which is defined as the “process of enabling people to increase control over, and to improve their health”. 6 SC contribution to HP has been modelized through the application of the settings-based approach 7 called health promoting SC. Four types of health determinants (social, organizational, environmental, economic) act at three levels internal to SC: macro-(policies and orientations of SC’ activities), meso-(activities of club management) and micro-level (coaches’ activities in guiding, altering or supporting actions of club member coaches’ activities in guiding, altering or supporting actions of club members) to foster HP. 8
Thus, although there is no theoretical model of health-promoting sport coaches, they play an important role as health promoters, based on the delivery of their sports activities (i.e., exercises quality, rest or social cohesion), which predict sports’ participants emotional, cognitive and behavioral outcomes, such as anxiety, self-esteem or intention of drop out. In this line, HP activities by the coaches contributed to positive sport experience and perceived health. 9 Moreover, evidence of the benefits of coaches’ HP activities have been found in previous work.10–12 High scores on perceived coaches’ HP activities by sport participants have been linked with a high score of enjoyment in sport practices, low scores of drop out intentions and high scores of quality of life, both among youth and adults..10–12 Beyond studies focusing on HP as global concept, coaches have been also recognized as a major source of psychological support for sport participants, when fostering autonomy development, 13 skills development 14 or relatedness-supportive behaviours. 15 Previous research has shown that coaches focus preferentially on performance oriented actions 16 and that their focus on HP was mainly on providing fun or divert activity. 17
Despite their potential to have a positive influence on sport participants, coaches are more passive towards HP, 16 as they stated that HP could be increased in their SC, especially in regard to the organizational and economic determinants. 12 Moreover, research has shown a limited capacity to discuss and implement specific HP programs. 18 Barriers such as their volunteer status, their lack of knowledge or resources to invest in have been identified19,20
So far, coaches have been reluctant to take part to health education programs due to their limited time investment but have stated being committed to enhance their practice. 21 Particularly since with the appropriate support, coaches can foster the commitment of individuals to sport practice, 22 identify sport participants’ “warning signs” to adapt their practices 23 or respond appropriately to sport participants’ needs when they are concerned as a role model. 24 Strengthening coaches’ commitment to health promotion 7 requires providing practical support to develop their skills and knowledge in health-related issues, thereby creating a competent and empowered coaching workforce.16,25 This involves identifying key skills that need enhancement, 26 particularly in the context of sports clubs, which differs significantly from school or healthcare settings, due to their voluntary nature and informal education opportunity. Furthermore, there is a need to adapt sports policies and systems, given their often voluntary nature, to empower coaches in HP and address barriers, such as limited time, lack of knowledge, or insufficient implementation skills. 27 The primary aims of this systematic mapping review is to identify coaches’ HP skills, which are already used in daily practice, and which they need to acquire, as well as leverages and barriers to their use.
Methods
Design
A systematic mapping review was carried out to map coaches’ HP skills, their use in daily practice and the ones coaches would like to acquire, as well as leverages and barriers to their use, in order to enable the development of future HP intervention. 28 Using a systematic review is justified by the importance of comprehensive and exhaustive synthesis of the literature, coupled with a mapping review, allowing to map the identified skills, their barriers and leverages in regard to a classification.29,30 The protocol was recorded on PROSPESRO, based on PRISMA-P guidelines. 31 To review the quality of included studies, AMSTAR 2 was used to guarantee rigor and transparency. 32 Due to the broad diversity of skills, as well as the impossibility to quantify their impact, a narrative synthesis was undertaken.
Eligibility criteria
The main inclusion criteria were: (a) being published an article in peer-review English journals, (b) including grassroots organized sport coaches as population, (c) describing skills in HP. The terms competencies and skills have been used in an undifferentiated manner, as this had been found as common in the literature particularly with regard to its transferability, its application or even its development. Skills refer to “reading and understanding what is happening and adaptability to the context” 33 with “a specific cognitive or motor ability that is typically developed through training and practice, and is not context specific”. 34 As there is no theoretical model for HP skills, they will be defined as such when general skills have a direct or indirect influence on the health of sports’ participants. In the context of sport coaching skills are then defined as “the evaluations of the ability of the head coach to affect the learning and performance of sport participants and conceptualized coaching”. 35 We excluded articles that were (a) not in SC, (b) not focused on sport coaches’ behaviors/skills (c) not an original scientific article (e.g., protocol, conferences,) or in another language than English (d) focused on sport performance or rehabilitation only, (e) studies on elite sport, above regional level.
Search
Literature search was conducted in October 2023 over a time frame between 1986 (date of publication of the Ottawa Charter) and 2023 in the following electronic databases: PubMed (n = 1704) including MEDLINE, SPORTdiscus (n = 371), Embase (n = 331), Scopus (n = 205), Web of Sciences (n = 240).
The search keywords were ((“sport* coach*" OR "sport trainer*" OR "sport* volunteer*") AND ("skill*" OR "training" OR "behavior" OR "behaviour" OR "education”)) AND ("health").
Study records and selection process
The PRISMA flow diagram 36 describes the article selection process (Figure 1). The first and the last authors independently assessed titles and abstracts using Rayyan software, which “helps researchers to expedite the initial screening of abstracts and titles using a process of semi-automation while incorporating a high level of usability”. 37 In case of disagreement, a decision was made by a fore last author. Full text screening and analysis was done by the first author and verified by the last author.
PRISMA diagram for study selection. Legend: Skills that coaches want to develop (n = %/40 studies); Skills use as a strategy (n = %/16 studies); Barriers faced by coaches (n = %/37 studies); Leverages used by coaches (n = %/36 studies).
Data items
Studies content was extracted on an excel sheet to report following criteria: (a) authors; (b) country; (c) year; (d) participant characteristics (age and gender); (e) study design; (f) method and data collection tool; (g) purpose/research question; (h) type of sport (e.g., recreational, competitive, individual, collective sports); (i) key findings; (j) coaches’ HP skills; (k) leverage (i.e., what's support?) to HP skills use and barriers (i.e., what's hinder?) to HP skills use.
Study risk of bias assessment and report
The first author assessed the quality and risk of bias of the included reviews using the Measurement Tool to Assess Systematic Reviews (AMSTAR-2). 32 This specific quality assessment tool was chosen due to its applicability and has been used in numerous studies since its creation. 38 The AMSTAR-2 consists of sixteen items, each of the items are scored on a scale ranging from 0 to 10 with a score of 0 meaning “missing all required components”, and a score of 10 meaning “includes all components”.
Analysis method and grid construction
Five variables of interest were analyzed, including 1) skills, 2) skills used in daily practices, 3) skills to acquire, 4) barriers and 5) leverages to skills use. For each variable studied, three different types of analysis were undertaken. Thematic coding to highlight recurring categories within the variables (i.e., different skills, barriers or leverages); a categorization of the determinants of health (social, environmental, economic and organizational) mobilized by the variable analyzed; and finally, an analysis of the types of health (social, physical and psychological) affected by the use of the skill. The three types of health outcomes were based on the definition of health, where physical health referred at “capacity to maintain daily adequate energy level to resist at injury and diseases”, 39 social health referred at “the ability to fulfill one's obligations, develop one's potential, manage one's own life, be independent and participate in social activities” 40 and mental health referred at “a state of well-being in which the individual realizes his or her own abilities, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to his or her community”. 41
First, an inductive thematic coding of skills, barriers and leverages was done, collecting information in the results sections of the studies, the qualitative quote expressing either skills, barriers, or leverages. The inductive method is justified by the fact that although there is a model of the competencies of professionals in sport associated with performance and leisure 2 as well as a framework of competencies for health professionals, 42 no existing model organizes these two approaches together to identify the competencies of the sports coach adapted to HP.
After identifying the skills already in use and those required, a schematic representation was created to summarize the findings, ranking the skills by their current usage and desirability for acquisition. A similar approach was applied to barriers and enablers, using arrows to create a mind map highlighting the most critical aspects to address when considering coaches’ HP skills.
Secondly, a blind coding process by the first and last author was made to link the skills, barriers and leverages with the types of health determinants of the Health Promoting Sport Club Model, 43 and the type of health impacted.
Results
On the 2485 screened studies (see Figure 1), 56 studies were included in this systematic mapping review (see Table 1), targeting 6379 coaches. The studies were mainly from Australia (n = 11) and USA (n = 11), followed by United Kingdom (n = 8), Ireland (n = 5), Canada (n = 4) and 3 multi-country studies were found. Publication dates started in 2007 and proceeded thereafter with 4 studies before 2010, 34 between 2010 and 2020, and 18 since 2020. Most of studies investigated multiple-sports (n = 33) and soccer (4).
Descriptives informations about included studies.
Note: Score on a 12-points scale using adapted AMSTAR2 rating.
The results of this systematic study highlight ten key skills used and requested by coaches to promote the health of their sport participants, and which have been reported to varying degrees. The latter also reported nine barriers in the use of HP skills and five leverages to overcome them (see Figure 2).
Coaches’ skills use as strategy, wish to develop, barriers they face and leverages they use to overcome them.
HP coaches’ skills
Coaches’ identified HP skills included, described in order of their frequency in the different studies including sport participants’ management (n = 23/37 studies), health support (n = 23/37), education (n = 21/37), appraisal (n = 20/37), motivation (n = 19/37 studies), cooperation (n = 18/37), prevention (n = 13/37), communication (n = 12/37), role model (n = 12/37 studies) self-management (n = 11/37) (Table 2).
HP coaches' skills.
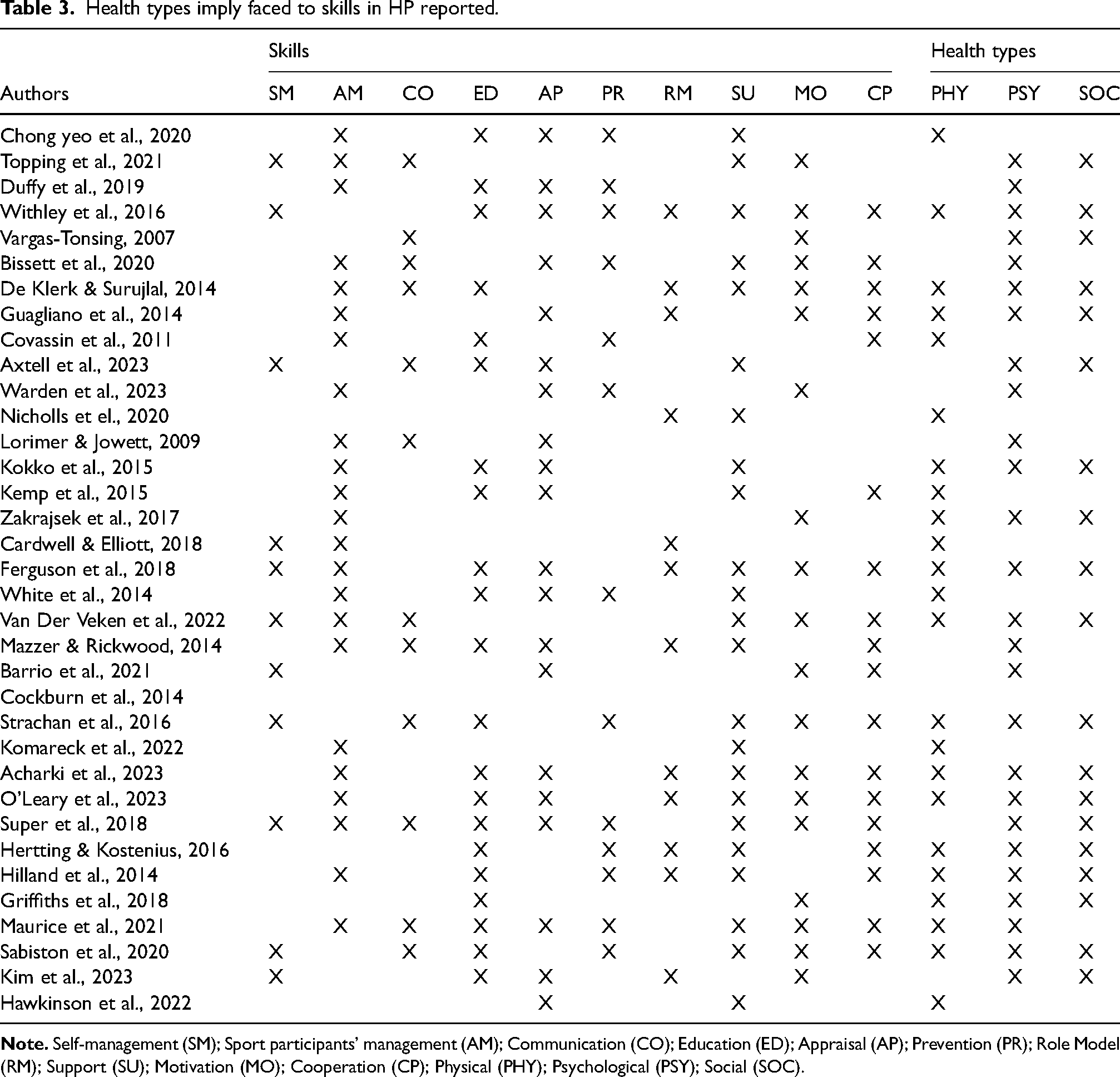
Health determinants analysis results showed that skills reported by coaches principally referred to social determinants of health (n = 29/56), before organizational determinants (n = 17/56), economic determinants (n = 16/56) and environmental determinants (n = 14/56).
Health types imply faced to skills in HP reported.
Coaches’ skills used in daily practice
To implement HP in SC, coaches use of these HP skills, which are reported in 16/56 studies, based on their frequency in analyzed studies: Motivation (n = 11/16), Sport participants’ management (n = 7/16), Self-management (n = 7/16), Health Support (n = 7/16), Communication (n = 5/16), Appraisal (n = 5/16), Role model (n = 4/16), Education (n = 3/16), Prevention (n = 3/16), Cooperation (n = 2/16).
Motivation strategy is used to put sport participants away of everyday hassles with positive and supportive atmosphere creation (i.e., healthy, safe and caring environment) and safe behaviors development through sports activities. 44 Sport participants’ management skill referred to coaches fostering sport participants’ emotion control, program adaptations (i.e., activities’ complexity or facilitation), including planning of activities depending on sports participants mental and physical state. Self-management was centered on coaches’ own emotional management, to normalize and validate sport participants’ actions and feelings in order to minimize the impact of negative emotions. 45 Health Support was used when coaches guide and advice sport participants already engaged health behavior (e.g., support in reducing smoking through advice) to maintain their efforts. 46 Communication skill is based informal conversation (e.g., around mental health, coping strategies or feedback using to increase sport participants’ behaviors with positive or negative reinforcement (e.g., personal growth, autonomy, acceptance). 47 Appraisal was used to evaluate risks of unhealthy behaviors (e.g., concussion) and encourage sports participants to take precautions, limiting the occurrences of these behaviors. 48 Role model referred to the awareness of coaches’ influential role, used as an opportunity to promoting psychological health (e.g., body image and self-esteem). 49 Education was used to limit occurrences of unhealthy behaviors through proper education. 48 Prevention was used through actions to support, influence sport participants on social (e.g., marginalization), psychological (e.g., stressed) or physical drift (e.g., concussion). Cooperation referred to the use of family (e.g., parents) to promote sports participants health. 50
Health determinants analysis results showed that skills used by coaches principally referred to social determinants (n = 14/16), organizational determinants (n = 9/16), environmental determinants (n = 2/16) and economic determinants (n = 1/16).
The HP skills of coaches were mainly used with an emphasis on psychological health (n = 12/16) through emotional connection work with sport participants, 51 promoting a moment of success or the creation of a therapeutic atmosphere, 17 followed by physical health (n = 6/16) when assessing and managing injuries; and social health (n = 7/16) in the management of communication with sport participants.
Skills to acquire by coaches
The literature also highlights coaches’ need to develop specifics skills for HP development, from most requested to least requested: Communication (n = 19/40); Sport participants’ management (n = 19/40); Health support (n = 18/40); Motivation (n = 18/40); Self-management (n = 17/40); Appraisal (n = 14/40); Prevention (n = 13/40); Cooperation (n = 11/40); Education (n = 8/40); Role model (n = 6/40).
The need in regard to Communication are principally on how to foster engagement of sport participants, on how to discuss with sports participants on the development of their personal and social skills. In regard to sport participants’ management, coaches want to learn on how to create safe and caring climate. 17 Health Support needs are on the ability to anticipate sport participants’ injuries and generate feedback to reinforce sport participants’ healthy behaviors.17,52,53 To develop Motivation, coaches want to get helped on how to foster social network positive and caring climate with and between sport participants. 54 The need to enhance Self-management is based on how to adapt their own behaviors, emotions and actions to sport participants’ health behaviors. For Appraisal needs are on detecting signs and symptoms of illness or inappropriate behavior For Prevention, needs are on how to avoid illness or inappropriate behaviors. 55 The need to enhance Cooperation is based on how to develop connections with sport participants’ entourage and confidence to offer healthy choices and reinforce health behaviors beyond sport activities. 56 Education need are on how to develop education on sport participants’ life skills through sport practices which implying also cross-sectoral knowledge.51,57 Role model needs are especially on how to develop self-confidence, and gather a positive representation by their sport participants. 16 Health determinants analysis results showed that principal skills to develop referred to social determinants (n = 24/40), organizational (n = 20/40), economic (n = 17/40) and less on environmental determinants (n = 11/40).
The skills to be developed revolve around the three aspects of overall health (i.e., physical, psychological and social) with a slight prevalence on the psychological health (n = 29/40), followed by physical health (n = 28/40), and social health (n = 24/40).
Barriers to skills use
Barriers to skills use.
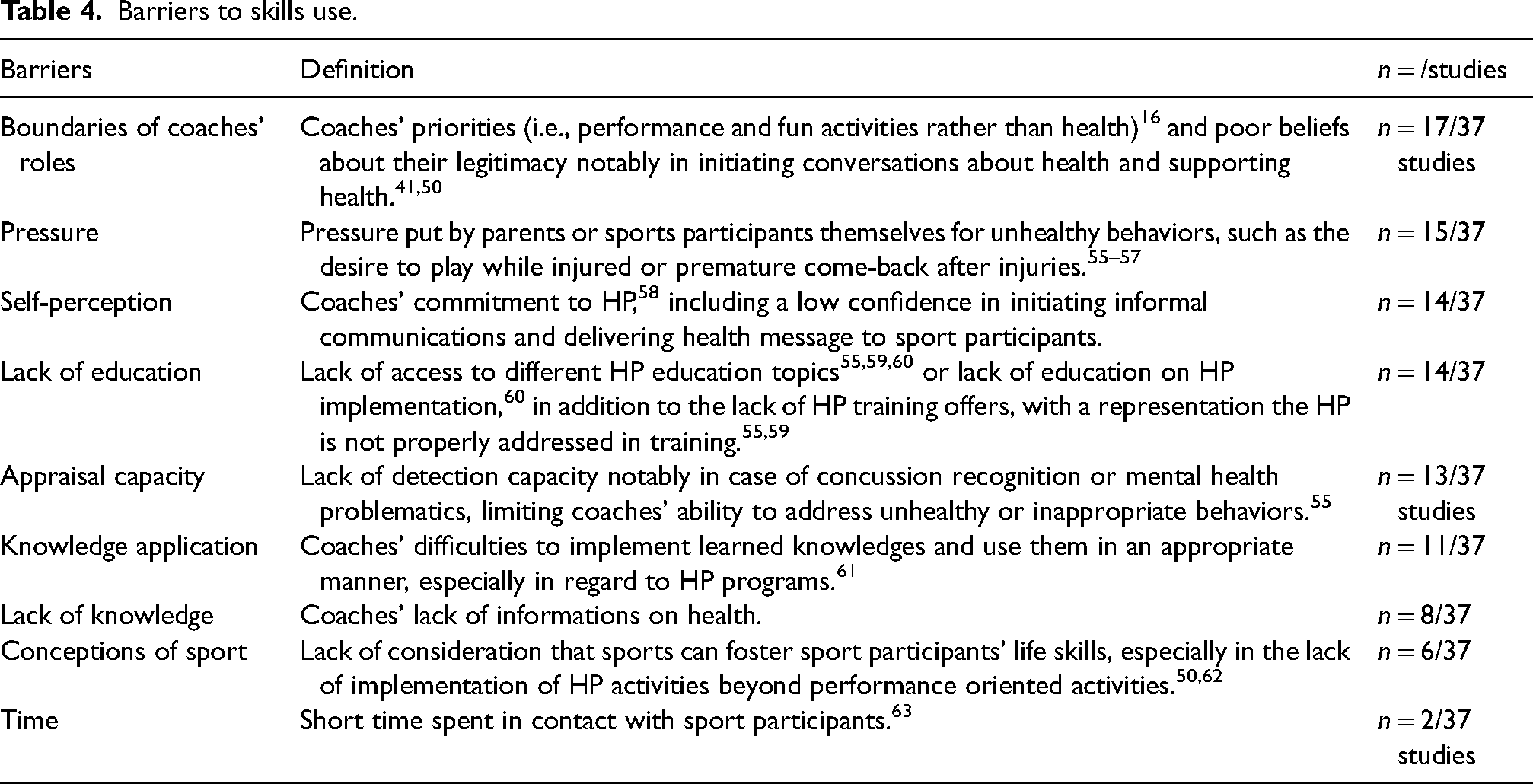
Health determinants analysis results showed that a majority of barriers are principally on social determinants (n = 21/37), followed by organizational determinants (n = 20/37), economic determinants (n = 17/37) and environmental determinants (n = 5/37).
The importance of health on coaches’ barriers felt are mostly social health (n = 19/37) with notably a non-perception of themselves as role models 66 ; followed by psychological health (n = 14/37) in recognizing the signs and symptoms of emotions and physical health (n = 11/37) with notably poorness of injury management knowledges.
Leverages to skills use
Leverages to skills use.
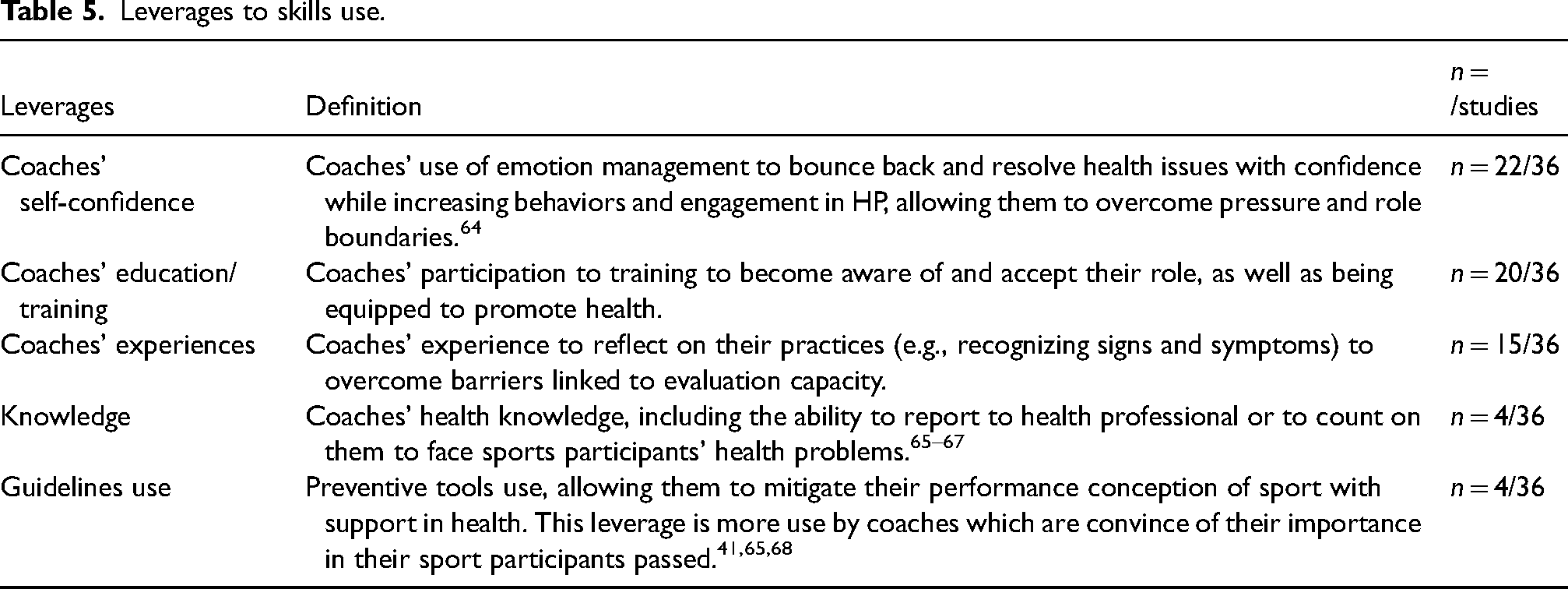
Results showed that a clear majority of leverages are coming from economic determinants (n = 30/36), followed by social determinants (n = 24/36), organizational determinants (n = 20/36), and environmental determinants (n = 5/37).
Discussion
There is a call from sports clubs and coaches themselves on capacity building to promote health in coaching practice. 7 Therefore, coaches should be guided and their motivation and commitment ensured by enhancing their knowledge and skills. 69 Aligned with previous research, the analysis and development of coaches’ skills in HP can be considered from at least two different perspectives: how are these skills related to existing coaching practice or to health professionals’ skills? As HP is seen as a continuous process and as there is currently no theoretical framework that includes both aspects. Although there is currently no theoretical framework on health coach skills, health and health inequalities are contextual and understanding contexts is central for health promoters. These health contexts influence the local setting and can go beyond it. 70 Thus, to analyze the mapping of health coach skills, we need to analyze the HP coaches’ skills with the contexts involved by these actions, namely coaching and health.
The present systematic review identified 10 coaches’ HP skills, with a different hierarchy between those used and those requested by coaches, as well as leverages and barriers to their use. Our results of HP coaches skills present similarities with those identified in the field of sports coaching, when mapping them to the International Sport Coaching Framework in 2012 (see Table 6). 2 A congruence between the functions of coaching in the context of sport and a large majority of the skills needed to promote health in this environment whether in relation to motivation (“Build relationships”), 2 education (“Be an educator”), 2 role model (“lead and influence”), 2 cooperation (“Nurture individual relationships”), 2 appraisal (“Read and react to the field"), 2 prevention (“Shape the environment function"), 2 communication (“set the vision”), 2 self-management (“Learn and reflect") 2 and sport participant's management skill (“Organize the setting and personnel"). 2 Since there is no strong dichotomy between coaching skills and HP skills, this indicates that coaches do not need to develop new concepts or explore completely unknown areas to integrate HP into their practices. It also demonstrates that these HP skills can in fact be an essential component of sports coaching that explicitly integrates HP aspects into the practice, requiring only the integration of health knowledge adapted to the sports context.
Skills link between sports coaching, HP coaches and health professionals.
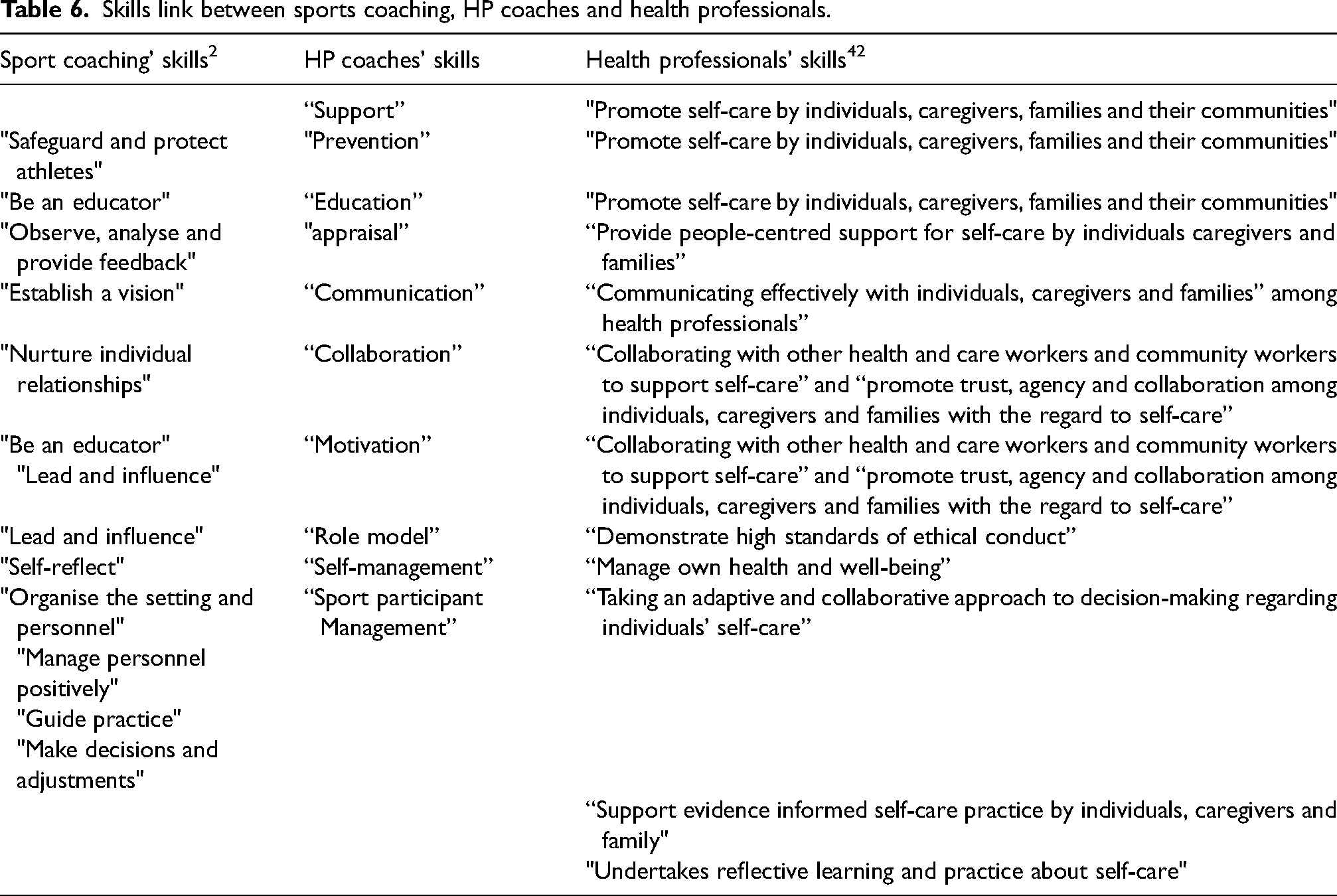
Beyond the comparison with the sport coaching framework, our skills findings also suggest a correspondence between the skills identified in this review and those identified among health professionals, described in the Self-Care Competency Framework published in 2024. 42 Although some competencies in the health professional framework (e.g., “Support evidence-informed self-care practice by individuals, caregivers, and families” and “Undertake reflective learning and practice about self-care”) 42 are not shared between coaches and health professionals, this is because coaches do not provide care and do not hold data related to the health status of their athletic participants. These competencies are therefore outside their scope of competence. In health professionals field, through the aspects of supports the individual to adapt options for self-care, demonstrating the awareness of the risks and health literacy development identify in “Promote self-care by individuals, caregivers, families and their communities” 42 can be related to support health, prevention and education skills of coaches in HP; Identifies vulnerabilities of individuals present on health professionals skill “provide people-centered support for self-care by individuals caregivers and families” 42 can be related at appraisal skill; “taking an adaptive and collaborative approach to decision-making regarding individuals’ self-care” 42 as the Sport participant' Management skill; “Communicating effectively with individuals, caregivers and families” 42 among health professionals could referred at the communication skills; “Collaborating with other health and care workers and community workers to support self-care” 42 and “promote trust, agency and collaboration among individuals, caregivers and families with the regard to self-care” 42 which came come close to collaboration and motivation skills thanks to the involvement of entourage; “Demonstrate high standards of ethical conduct” 42 which can referred to role model skill through the duty to maintain one's conduct; “Manage own health and well-being” 42 which can be related to self-management through the involvement of their own self-care practice. As much correspondence between the HP skills of coaches and those of health professionals suggests that HP aspects can be more integrated into the framework of sports coaching, and this explicitly, without requiring the development of new skills on the part of coaches. Thus, such integration suggests an orientation of coaching that would no longer be only linked to leisure or performance but also to health aspects within the practice itself.16,17 Moreover, these correspondences between the skills of the three environments that are sports coaching, HP and health professionals allows to highlight the fact that coaches have the capacity to apply the knowledge that could be transmitted to them beyond the coaching aspects. A strong political challenge then arises regarding the development of tools or guides linked to knowledge in the field of HP among coaches to enable application within SC.
Therefore, the present mapping of the coaches HP skills highlights the match with both coaching and health professional skills frameworks, putting forward the key role that coaches play in sports participants development beyond the performance and play aspects. 64
However, all skills are not used in the same way. The most used coaches’ HP skills (i.e., Motivation, sport participants’ management, self ‘management, support and communication) are also those that coach desire to acquire (cf. Figure 2). Notably, and linked to the importance of differentiating health professionals and coaches, skills such as prevention or appraisal are among the most needed and are the less predominant in coaches’ practices.
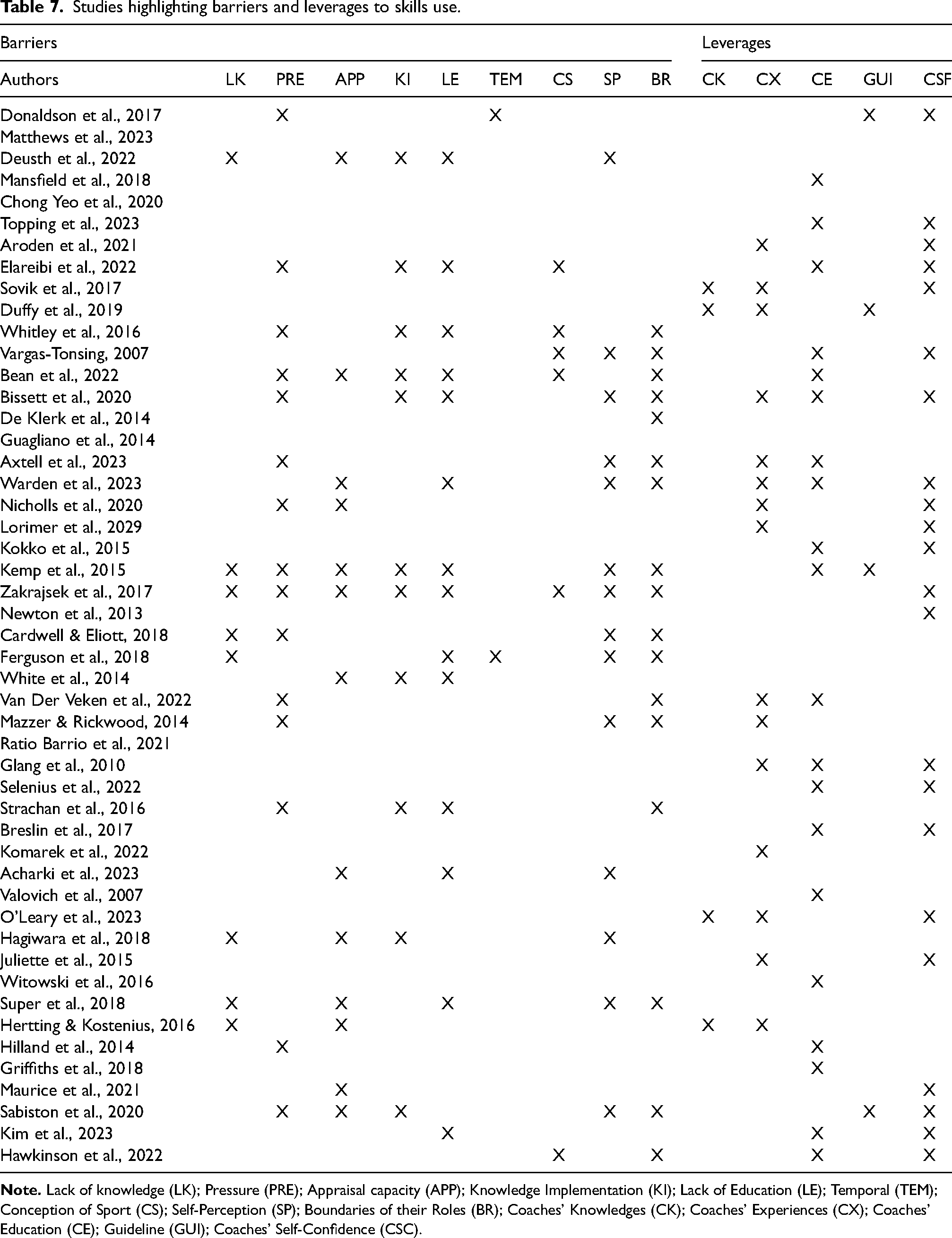
Barriers to coaches’ HP skills use are lying first in the definition of their role, where coaches feel lacking of confidence, legitimacy and knowledge to exert the role of health promoter (see Table 7). Similar results in terms of barriers have been found among school teachers, where their perceptions of HP being part of the program, the school environment, including relationships with parents, and with managers, have been found as key for HP programmes implementation. 71 Such results are also in line with previous studies on health promoting SC, 69 where the ability to embed health in daily activities is key for settings-based approach implementation. 72
Studies highlighting barriers and leverages to skills use.
Some of the barriers were also common with health professionals’ representation, especially on the lack of knowledge, lack of implementation skills 73 and the need for education. 54
Moreover, modifying coaches’ commitment towards HP is also based on the environment, and on the mandate from sports federations or governmental authorities to support SC HP.74–76
In the context of the coaching, the literature shows that coaches are often volunteers having a full-time job before dedicating time to coaching, leaving little opportunity of development through training or formal education. 65 This corroborates the limitations linked to the lack of training, knowledge and application of knowledge raised in this review. 77 Previous study on the implementation of a HP program, the FIFA11+, barriers were principally lack of knowledge, lack of player engagement, lack of link to football related goals, lack of facilities and resources and lack of time at training. 49 These barriers are also very similar to those identified in the present literature review, highlighting the importance of the sports environment in terms of support, but also targeting barriers internal to coaches (i.e., lack of time).
In regard to the barriers, the most cited were internal to coaches, such as self-confidence, knowledge or experience, which relates to coaches’ ability to question themselves and reflect on their practices. Previous studies on motivational climate have shown that coaches’ well- or ill-being was a predictor of coaches’ motivational climate, where job security, opportunities for professional development and work-life conflict predicted coaches’ well- or ill-being. In another study, administrative support, sports participants’ motivation, colleagues support and time constraints predicted coaches’ motivational climate. These studies have shown that coaches psychological state, as well as perception of support by its sports environment play key role in his behaviors. Interesting results are on the use of guidelines,78,79 which seems to be supportive in HP implementation, calling for more explicit and clear guidance on HP in organized sport. 80
Coaches’ commitment to psychological health principally through their skills, particularly regarding the ability to cope with daily challenges, manage stress and maintain self-satisfaction and personal fulfillment can be explained by the importance of psychological health in sports performance. 81
In general, results show that the social determinants of health is the most represented in the literature regarding coaches’ HP skills. Interestingly, leverages most represented determinants was economic, in terms of providing resources and financial contribution for environmental change or education. The social determinants of health is also the one that is the most implemented at SC levels in different European countries, which shows the alignment between coaches and SC practices.21,82,83
Practical implications
The study's results have multi-level implications within settings-based approach. 72 For public policies, findings suggest enhancing support for training, either by expanding HP training offer to sports coaches or by developing guidelines targeting essential skills. At sports federation level, reflections on the evaluation and initial training on coaches’ HP skills are key assets to support long-lasting and healthy sport practice. For coaches themselves, a reflection on their role in regard to HP and their ability to self-evaluate themselves would be key to foster HP. Finally, for sport participants, the analysis of coaches’ HP skills highlights the orientation of health actions implemented and received by sport participants on different types of health (i.e., physical, social or psychological)
Strengths and limitations
The literature review followed a systematic approach, searching several databases to gather all relevant studies. Although the term skill was primarily used in this study, it was not specifically defined in the literature. The category of skills was developed based on the discourse of established coaches and managers as reported in study results and not in interviews. Moreover, analyzed studies did not reported evidence of the effectiveness or even impact of the use of these skills. One of the limitations considered in this review is the lack of information on how coaches implement skills within practices and how these skills impact (i.e., directly or undirectly) health behaviors of sports participants. However, this will be the subject of future studies.
Conclusions
This research made it possible to identify ten coaches HP skills which have also been identified in framework on health professionals’ skills 82 and sport coaching skills, 81 but also include further skills due to the particularity of the sports coaches’ role. The strong presence of the social determinants in all factors makes it possible to imagine the interest in investigating and developing other health determinants and comparing their implications in the evolution of skills, strategies and barriers in terms of HP practices in SC. These results suggest on the one hand to take into account the two sectors of activity when developing tools or interventions for coaches implementing HP, and on the other hand it underlines the need to put implement concrete strategies based on the development of specific skills when developing tools that directly depend on the HP needs of coaches or sport participants. However, this also implies the need to analyze coaches’ perceptions of their role and their influence on practitioners’ health.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not necessary for this article because this review did not require human or animal participation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Doctoral School Biologie Santé Environnement and Région Grand-Est, Partnership between Santé publique France and Université Côte d'Azur and Université de Lorraine.