
Abstract
Acute lower back injuries represent a significant concern in soccer players, often resulting in substantial morbidity and prolonged recovery periods. Despite various injury prevention programs, effective mitigation of acute lower back injuries remains challenging. The FIFA 11+ Injury Prevention Program is widely recognized for reducing general musculoskeletal injuries, yet its specific efficacy in lowering acute lower back injuries among soccer players has not been thoroughly evaluated. This systematic review and meta-analysis determined the effectiveness of the FIFA 11 + program in reducing acute lower back injuries among soccer players. A comprehensive literature search was conducted in PubMed, Cochrane Library, Web of Science, and PEDro from January 2010 to June 2025. Randomized controlled trials implementing the FIFA 11 + program and reporting acute lower back injury outcomes were selected. Search terms included ‘neuromuscular training,’ ‘injury prevention programs,’ ‘FIFA 11+,’ ‘soccer,’ and ‘back injury.’ Our meta-analysis of five studies with 566,781 exposure hours and 61 total acute lower back injuries revealed significant reduction in injury incidence with the FIFA 11 + program (IRR = 0.37, 95% CI: 0.21–0.66; p < 0.001), representing a 63% reduction in injury risk. The absolute incidence changed from 1.09 to 0.39 injuries per 1000 h, with an absolute risk difference of 0.70 injuries/1000 h and a number needed to treat (NNT) of 1429 h. The I2 = 0% indicated high consistency across studies. This review provides evidence supporting the FIFA 11 + program's efficacy in significantly reducing acute lower back injuries among soccer players. These findings underscore the program's value as a critical component of injury prevention strategies in soccer.
Introduction
Football, known as soccer in some regions, is the most popular sport globally, with over 265 million registered players and billions of fans worldwide. 1 The sport generates significant economic value, with annual revenues exceeding $50 billion globally and providing employment for millions across a range of sectors. Its cultural and economic impact makes football a vital area of study in sports medicine. 1 This sport can be practised at various levels, including recreational and professional. 2 However, soccer players are commonly exposed to aggressive contact situations and experience significant stresses on different body parts, particularly during high-intensity movements such as sprinting, tackling, and jumping. 3 These factors could lead to a wide variety of musculoskeletal injuries and complaints, including those affecting the lower back.4–8
Such injuries can result from either direct traumas that interfere with sports activity completion or from insidious onset due to repeated minor traumas. 9 Prolonged and costly rehabilitation of this type of injury affects the status of the player and the club in which they play.10,11
Acute lower back injury is a prevalent and debilitating condition in both general and athletic populations, but prevalence data vary across studies. For this review, we define acute lower back injury as any acute musculoskeletal injury occurring in the lumbo-pelvic region that necessitated medical evaluation and resulted in time-loss from sport participation. This definition encompasses common low back injuries such as acute muscular strains, ligamentous sprains, and acute non-specific lower back pain (LBP) episodes, while excluding major structural pathologies (e.g., vertebral fractures or intervertebral disc herniations).12,13 Surveillance data indicates that LBP is a prevalent issue in football, with studies reporting that around 10 to 15% of players experience LBP annually.14,15 Youth and amateur players are disproportionately affected,13,16 likely due to limited access to structured training and conditioning programs. In professional football, the career prevalence of LBP ranges between 32 and 50%,15,17 which is concerning because it can significantly impact performance and career longevity. For example, a systematic review reported that musculoskeletal injuries, including LBP, account for a substantial proportion of time-loss injuries in football players. 18 These findings underscore the need for targeted prevention strategies like the Federation Internationale de Football Association (FIFA) 11 + program, especially given the higher prevalence rates observed among youth and amateur players. Despite its prevalence, LBP in football as in many other team and individual sports remains under-researched compared to other injury types, such as knee or hamstring injuries.12–14,19 Notwithstanding the athletes’ strength and flexibility, they might experience LBP due to repetitive flexion, extension, twisting and axial loading movements, which are inherent to many sports, including soccer. The causation of LBP is complex, influenced by a dynamic interaction of intrinsic factors, such as biomechanics, muscle strength, and prior injury history, alongside extrinsic factors, including playing surface, training load, and equipment. Understanding these variables is essential for developing effective prevention strategies.20,21 Moreover, the current non-surgical treatments for acute and chronic LBP have shown limited effectiveness, with evidence indicating that 9 out of 10 therapeutic procedures are ineffective. 22
Growing evidence supports the effectiveness of injury prevention programs such as the FIFA 11 + program in reducing injury rates, particularly among youth and amateur players. Studies conducted in Europe and North America have shown significant reductions (by 39 to 50%) in injury rates in recreational/sub-elite soccer players (mean age 10 to 20 years) who consistently implement the FIFA 11 + program as part of their training. However, there is currently no evidence for its effectiveness in elite professional players. Geographic variability also plays a role, with greater success observed in regions where structured training environments and medical support are more readily available. These findings highlight the importance of tailoring injury prevention programs to the specific needs and contexts of the players being targeted.23,24 To date, numerous studies have been conducted to assess soccer-specific injury prevention programs.25–27 In 2006, several institutions cooperated to develop a special injury prevention program called FIFA 11 + . 28 This program consists of three stages and comprises 15 exercises following a prescribed sequence, targeting muscle strength, kinesthetic awareness, and neuromuscular control during static and dynamic movements to reduce the risk of injury. 29 The program involves warm-ups at least twice a week, and to achieve effective results, a period of at least 10 to 12 weeks is needed. Additionally, research has indicated that the effectiveness of the program is increased using a qualified trainer and medical monitoring.30,31
The FIFA 11 + injury prevention program has been examined in multiple recent studies. Favorable results have been reported regarding the reduction in the overall incidence of injury among children31,32 and adult2,33 soccer players. Other improvements have been reported in the total number of missed days. 2
Given the recent development of the FIFA 11 + injury prevention program, and the promising effects reported in the literature, it is essential to summarize its effectiveness. Several previous reviews have been conducted to explore how the FIFA 11 + injury prevention program can prevent injuries in soccer players, including that conducted by Barengo et al. (2014) and Thorborg et al. (2017),28,34 incorporating a wide variety of study designs such as observational cohort studies and case controls in addition to clinical trials. Furthermore, another review conducted by Al Attar et al. in 2015 35 assessed nine randomized controlled trials (RCTs), but it focused on lower extremity injuries only. To the authors’ knowledge, no previous reviews have been conducted to assess the effectiveness of the FIFA 11 + programs in preventing acute lower back injuries in soccer players, appreciating the fact that FIFA 11 + program was not primarily designed to prevent low back injuries and complaints. This systematic review and meta-analysis, therefore, aim to address this gap by evaluating the available evidence on the effectiveness of the FIFA 11 + program in reducing acute lower back injuries in soccer players.
Method
Design
The study protocol was registered in advance with the International Prospective Registry of Systematic Reviews, PROSPERO (CRD42023382959). This systematic review with meta-analysis adheres to the reporting guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines. 36
Criteria for inclusion of studies
Inclusion criteria for this systematic review and meta-analysis were as follows: (1) RCTs investigating the effectiveness of FIFA 11 + injury prevention programs compared to the same program, another program, or regular warm-up, specifically focusing on soccer players and referees and reporting acute lower back injuries; (2) reporting at least two of the following: number of back injuries, back injury rate, and exposure hours; and (3) only studies published in English between 2010 and 2025 were included. No restrictions were applied based on age, gender, or playing level. These criteria were chosen to ensure a comprehensive evaluation of the impact of the FIFA 11 + program on acute lower back injuries among soccer players.
Outcome measures
The primary outcome measures were rates of acute lower back injury in the control group versus the intervention group. Lower back injury was defined as acute lumbo-pelvic tissue damage or other disruption of normal physical function due to participation in sports, resulting from rapid or repetitive transfer of kinetic energy, in alignment with Waldén et al. (2023). 37 This definition reflects commonly accepted criteria in the field. To ensure consistency across studies, injuries were categorized as those affecting the lumbo-pelvic region, including vertebrae, muscles, ligaments, and tendons, while excluding injuries to the thoracic and cervical spine. Chronic or gradual-onset LBP, as well as major structural pathologies (e.g., disc herniations), were excluded from this review due to their relatively low incidence among soccer players and the limited preventive capacity of neuromuscular warm-up programs such as the FIFA 11 + program to prevent such pathologies. The classification used by Silvers-Granelli et al. (2015) aligns with this definition, as their reference to “spine injuries” pertains specifically to the lumbar region. 2
Search methods for the identification of studies
Two independent investigators conducted searches for relevant studies in the Cochrane Library, PubMed, Web of Science, and Physiotherapy Evidence Database (PEDro) between January 2010 and June 2025. Keywords included various terms related to FIFA 11+, warm-up programs, neuromuscular training, soccer players, and athletic injuries. Search strategies included both keywords and Medical Subject Headings (MeSH) terms, such as ‘Back Injuries,’ Athletic Injuries,’ and ‘Soccer,’ tailored to each database's specific guidelines to ensure comprehensive retrieval of relevant studies and only studies published in English were considered
Data extraction and synthesis
Articles were initially screened for relevance based on title and abstract using the Rayyan Intelligent Systematic Review platform (https://rayyan.ai). The full text of relevant studies was downloaded and thoroughly evaluated against the inclusion and exclusion criteria. Two independent reviewers conducted this evaluation following pre-defined criteria, and conflicts were resolved through discussion. Agreement between reviewers was calculated as Cohen's kappa. Data from included studies were extracted and organized in a predesigned Excel spreadsheet, covering authors, publication year, population characteristics, study duration, interventions, intervention compliance, sports/level, and exposure hours. Missing data were obtained by contacting corresponding authors.
Administration
EndNote version X8 and Rayyan were used for storage, collation, and screening of studies. Primary outcome results from individual studies were extracted and collated in Excel before being transferred to Review Manager (RevMan), version 5 (Cochrane Collaboration, London, United Kingdom).
Meta-Analysis
To calculate the injury incidence rate, the number of incident injuries was divided by the total time at risk and multiplied by 1,000, as described by Waldén et al. (2023). 37 The Injury Risk Ratio (IRR) was calculated as the injury incidence rate in the intervention group divided by the injury rate in the control group, with an IRR < 1 indicating a positive intervention effect. The inverse variance random-effects model was employed to account for diverse populations and exercise doses. Heterogeneity was assessed using statistical models, including the I2 statistic, and RevMan V5 software was used for analysis. The overall effect of the FIFA 11 + and the FIFA 11 + kids was assessed, followed by subgroup analysis for the FIFA 11 + and the FIFA 11 + kids, separately.
If 10 or more studies were available, it was intended to create a funnel plot to assess the risk of potential publication bias. Egger's test and Begg's test would then be performed to assess the funnel plot asymmetry. The Duval and Tweedie's Trim and Fill method would be applied to determine whether the overall IRR estimate required any adjustments for the publication bias based on the filled studies.
Assessment of risk of bias in included studies
The methodological quality of included trials was assessed using the PEDro scale, which Moseley and Pinheiro (2022) 38 have shown has robust clinimetric properties for appraising the risk of bias and completeness of reporting of RCTs. The scale consists of eleven individual criteria. As it is valid to also treat the scale as unidimensional, 39 we also report the total score, which excludes the criterion related to external validity so total scores can range from 0 to 10, with classifications of ‘excellent’ (score 9 to 10), ‘good’ (6 to 8), ‘fair’ (4 to 5) and ‘poor’ (0 to 3).
Results
Flow of studies through the review
The initial database search identified a total of 444 studies. After the removal of 162 duplicate records, 282 studies remained for title and abstract screening. Following this screening process, 162 studies were excluded for not meeting the predefined inclusion criteria. A total of 120 studies were subsequently evaluated for full-text eligibility. Of these, 112 studies were excluded after full-text assessment for reasons such as not meeting the inclusion criteria. This resulted in the retrieval of eight full-text articles for detailed review. Among these, three articles were excluded for not being RCTs. Ultimately, five studies met all inclusion criteria and were included in the systematic review and meta-analysis.2,32,33,40,41 Cohen's kappa was 0.87 for title/abstract screening and 0.92 for full-text review. The selection process is detailed in Figure 1.
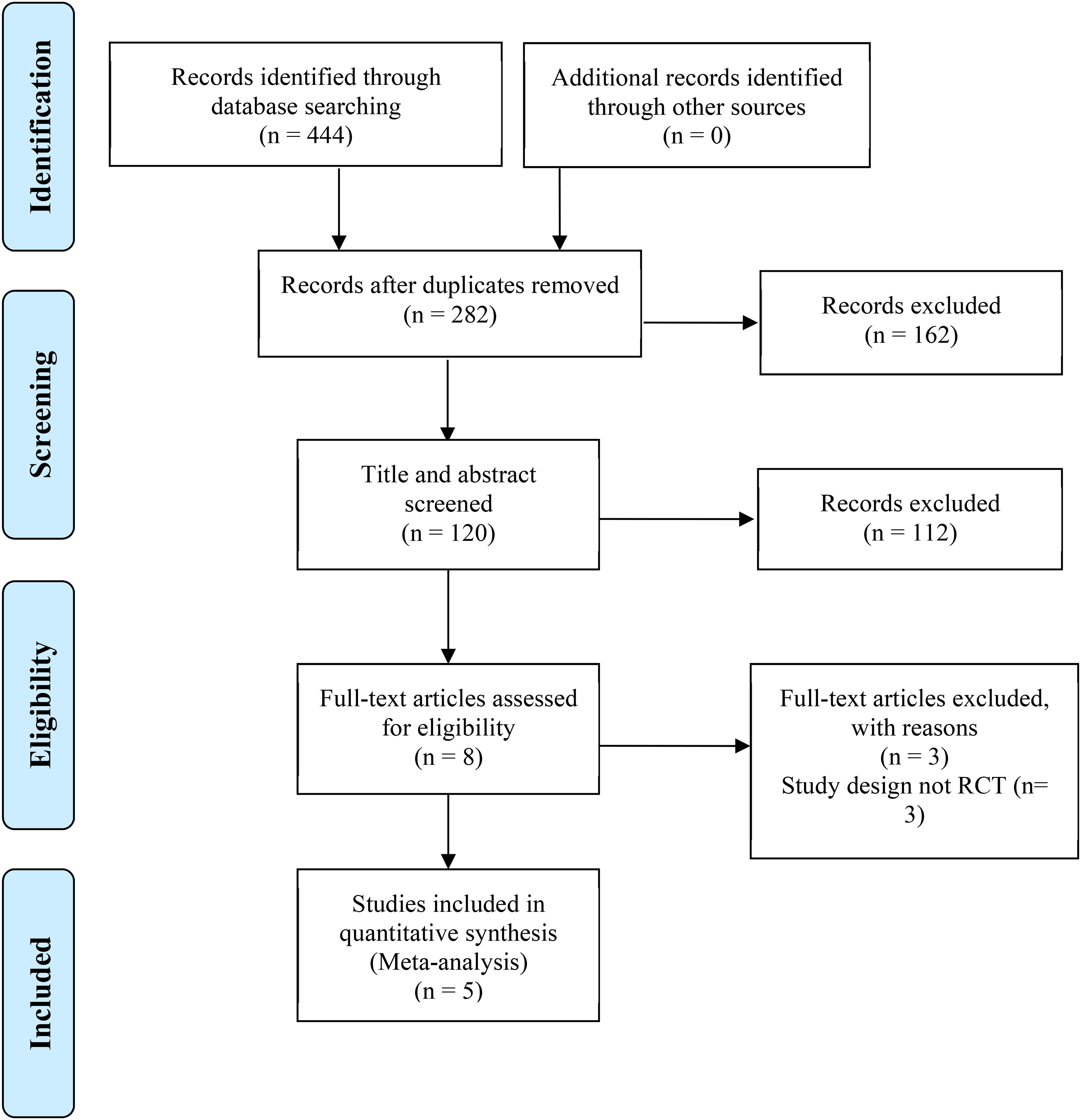
PRISMA flow diagram.
Characteristics of included studies
Three studies involved amateur soccer players and referees,2,33,41 while the remaining two trials were conducted with children.31,40 The trials encompassed a total of 566,781 exposure hours (279,698 h for the experimental group and 278,083 for the control group). All five trials were cluster RCTs, with one conducted in the United States, 2 one in Australia, 33 two in Saudi Arabia,40,41 and a multicentre study in four countries (Switzerland, Germany, the Czech Republic, and the Netherlands). 32 Four trials involved male players and referees,2,33,40,41 and one included both genders. 30 The age range varied across trials, with one trial including collegiate soccer players aged 18 to 25 years, 2 one involving amateur soccer referees aged 25 to 37 years, 33 one involving amateur soccer players aged 14 to 35 years, 33 and two trials with child soccer players aged 7 to 13 year.32,40
Two trials employed the FIFA 11 + injury prevention program as a warm-up for the intervention groups,2,41 whilst one used the program both pre-and post-training. 33 The FIFA 11 + injury prevention program for kids was used in two trials,32,40 incorporating five different levels of single-leg stance exercise. The length of the injury prevention program ranged from 6 to 12 months. Control programs varied across trials, with three using standard warm-up,32,40,41 one using the FIFA 11 + injury prevention program as pre-training only, 33 and one employing an aerobic warm-up in the control group. 2 Table 1 provides a summary of the characteristics of the five trials, while Table 2 details the rates of acute lower back injuries and exposure hours in the intervention and control groups. Included studies collected exposure data using a combination of self-reports by athletes, logs maintained by coaches, and match statistics recorded by observers.
Characteristics of the included trials (n = 5).
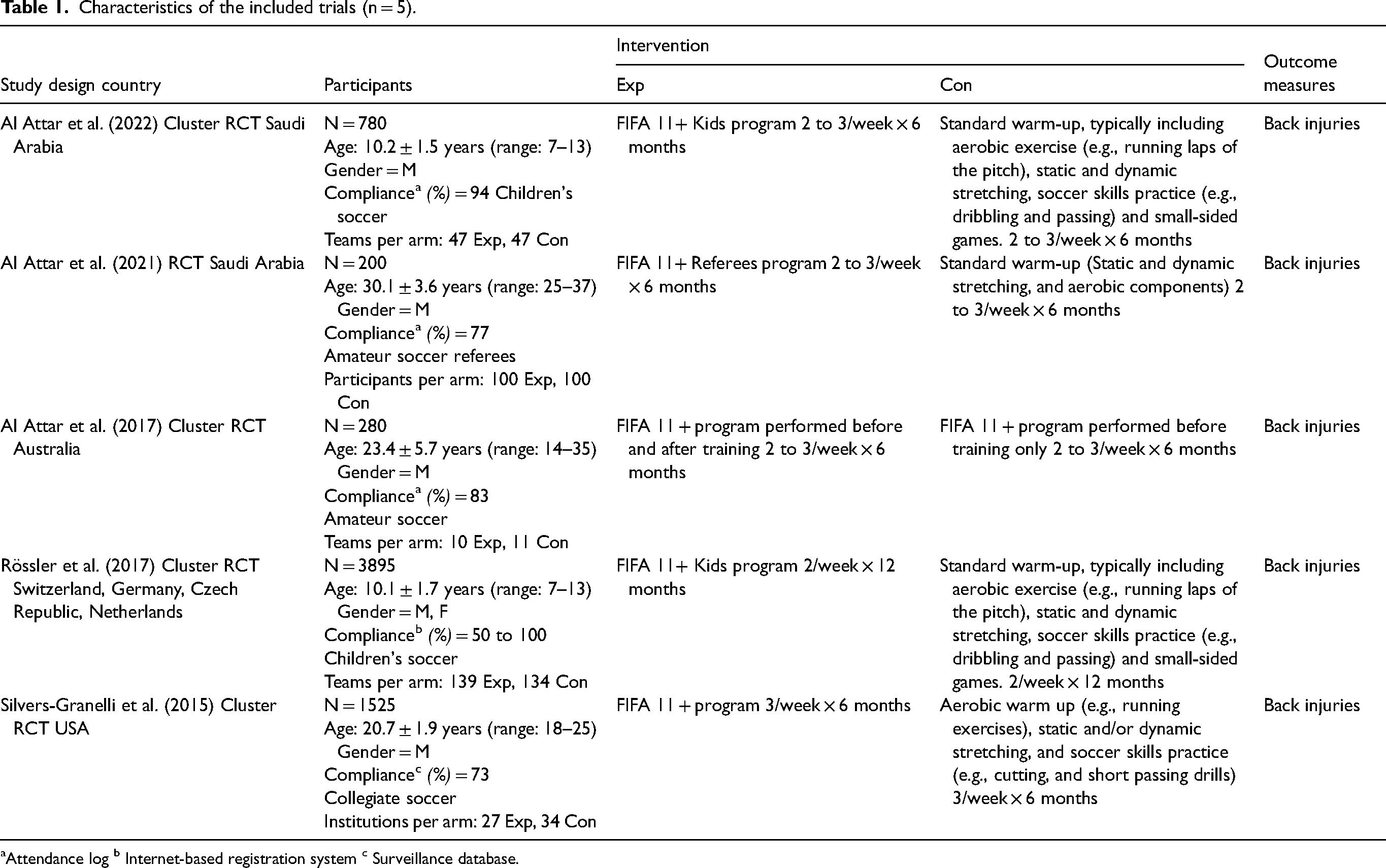
Attendance log b Internet-based registration system c Surveillance database.
Injury rates per 1000 h of exposure in the intervention and control groups of the included studies.
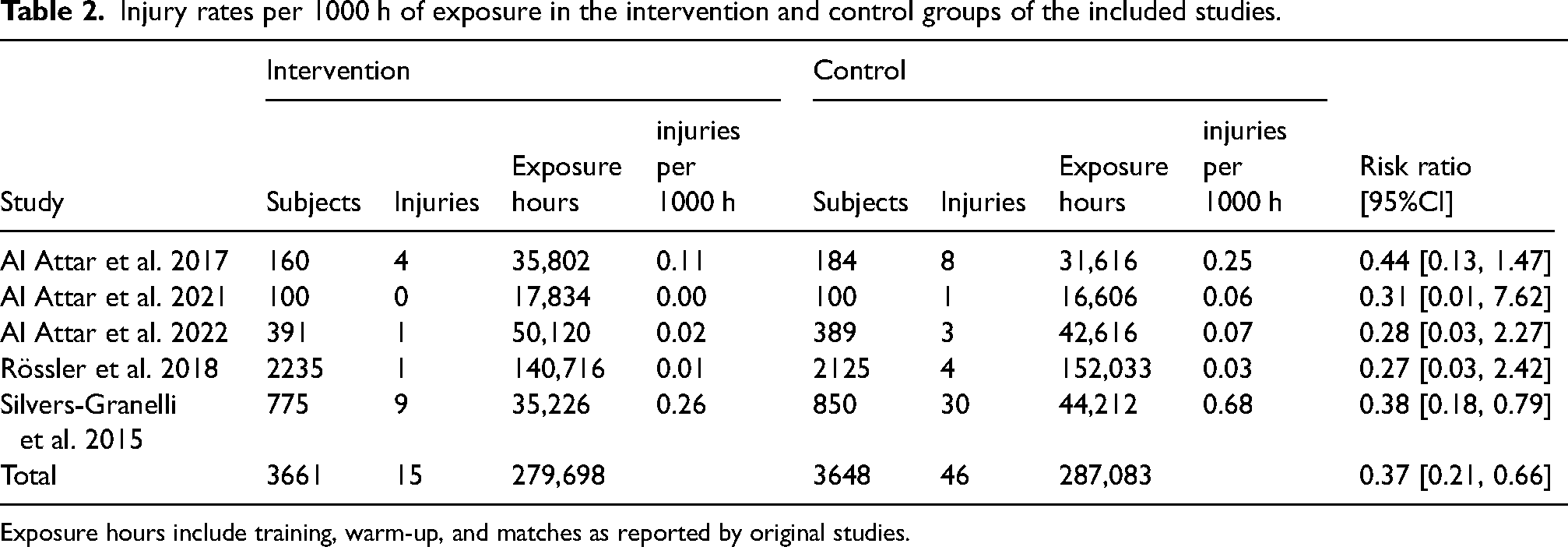
Exposure hours include training, warm-up, and matches as reported by original studies.
Risk of bias and methodological quality assessment
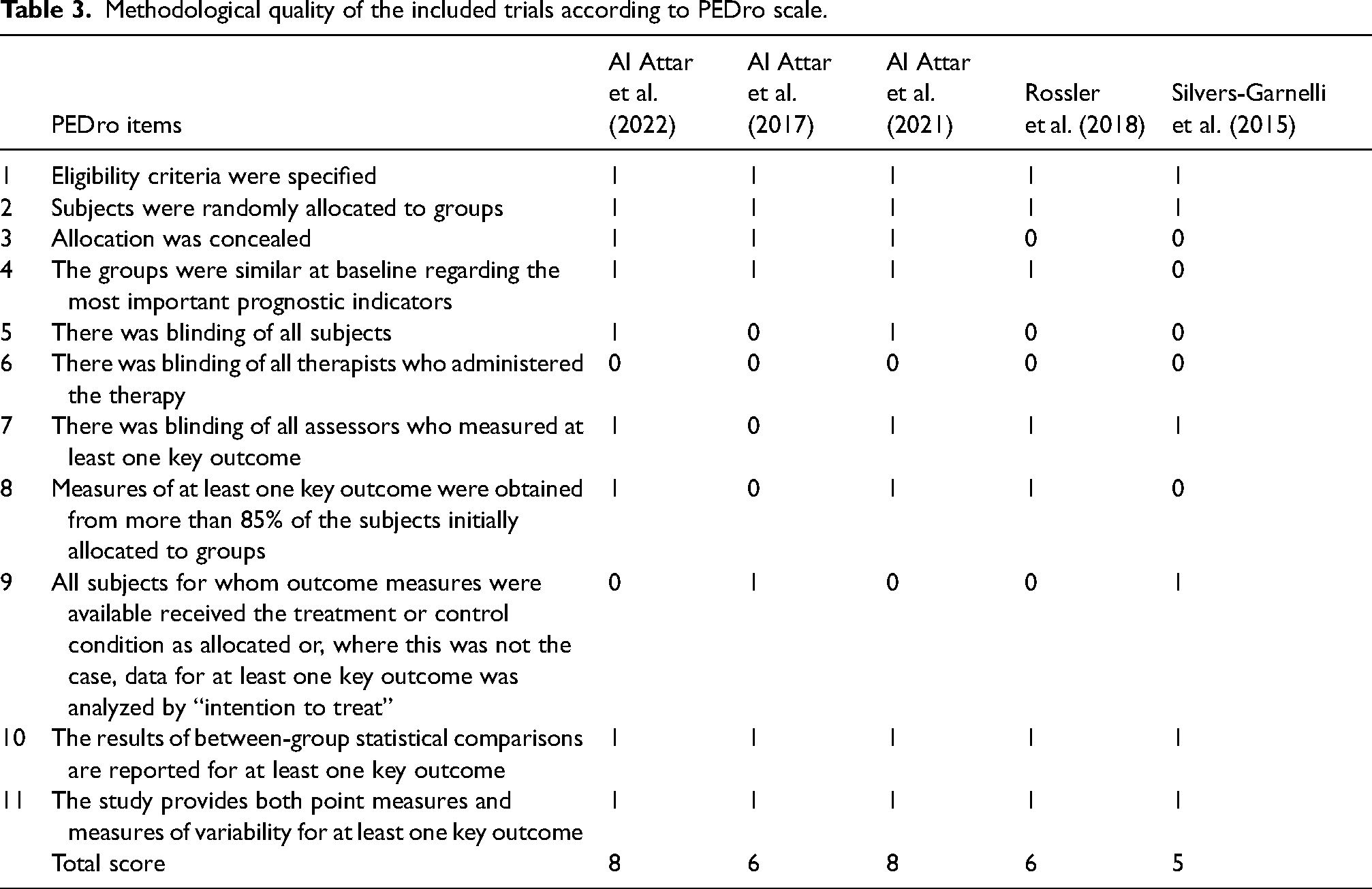
According to the PEDro scale, four studies were rated as good quality,32,33,40,41 and one study was rated as fair. 2 The overall methodological quality of the trials ranged from 5 to 8 out of 10, with a mean score of 6.6, indicating good quality. Table 3 presents the individual criteria ratings and the total scores of the reviewed articles according to the PEDro scale. In line with PEDro guidelines, items that were not met or not clearly reported were assigned a score of 0. Specifically, allocation concealment was unclear in two studies,2,32 and blinding of participants was not reported or not implemented in three studies.2,32,33 Assessor blinding was not reported in one study, 33 and intention-to-treat analysis was not performed or clearly described in three studies.2,32,40 These limitations reflect common reporting challenges in sports injury prevention trials and have been explicitly documented to enhance the transparency and interpretability of study quality assessments.
Methodological quality of the included trials according to PEDro scale.
Pooled injury estimates
The pooled results, encompassing 7309 players and 566,781 exposure hours, revealed 61 acute lower back injuries (see Table 2). The pooled incidence rate (IR) was 0.39 injuries per 1000 h of exposure for the intervention groups and 1.09 injuries per 1000 h of exposure for the control groups.
Meta-analysis results
Reduction of injuries based on total exposure hours
The pooled results indicated a 63% reduction in acute lower back injury per 1000 h of exposure compared with the control group, with an IRR of 0.37 [95% confidence interval (CI) 0.21 to 0.66]. Inconsistency statistics showed homogeneity among studies (I2 = 0%) (Figure 2). The absolute incidence changed from 1.09 to 0.39 injuries per 1000 h, with an absolute risk difference of 0.70 injuries/1000 h and a number needed to treat (NNT) of 1429 h. This means that approximately 20 players would need to perform the FIFA 11 + program consistently for one year (at standard weekly exposure levels) to prevent one acute lower back injury. While the NNT appears high, the preventive impact at the population level can be substantial.
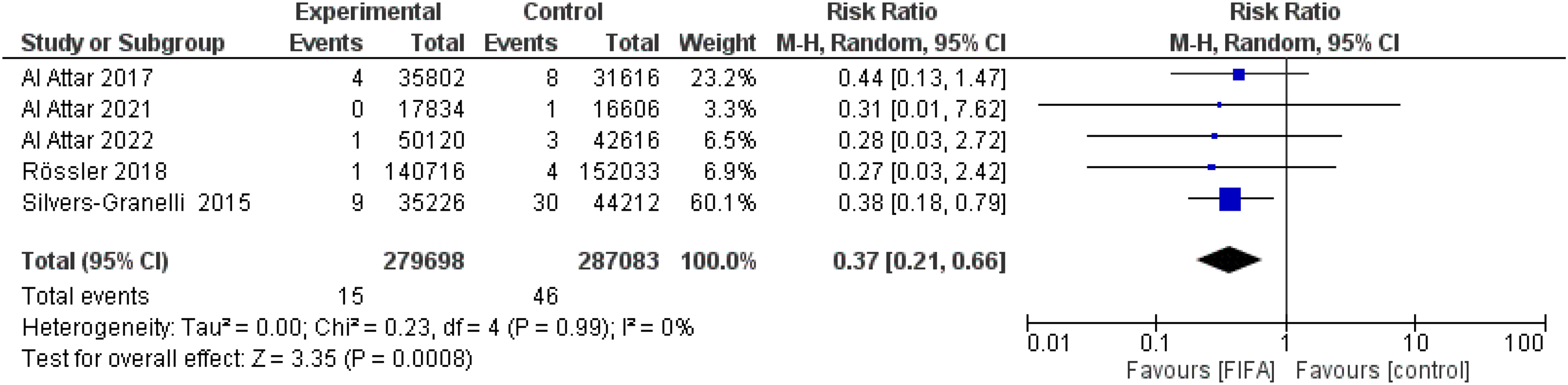
Forest plot of trials comparing the effects of all FIFA 11 + vs regular warm-up on overall incidence of acute lower back injuries in soccer players. A random-effects model was used. The pooled Injury Risk Ratio (IRR) was 0.37 (95% CI: 0.21–0.66). Heterogeneity: Tau2 = 0.00; I2 = 0% (95% CI: 0–45%); Q(4) = 3.2; p = 0.52. Study-specific weights (%) and confidence intervals are displayed in the plot.
Subgroup analysis of the FIFA 11+ and FIFA 11+ kids injury prevention programs
The pooled results of the FIFA 11 + injury prevention program alone (n = 3) revealed a 61% reduction in overall acute lower back injury per 1000 h of exposure in the intervention group, compared with the control group, with an IRR of 0.39 (95% CI 0.21 to 0.73, p = 0.03) (Figure 3). The results of the FIFA 11+ Kids injury prevention program alone (n = 2) indicated a 72% reduction in overall acute lower back injury per 1000 h of exposure in the intervention group, compared with the control group, with an IRR of 0.28 but this was statistically non-significant (95% CI 0.06 to 1.33, p = 0.11). Inconsistency statistics indicated homogeneity between studies (I2 = 0%) (Figure 4).
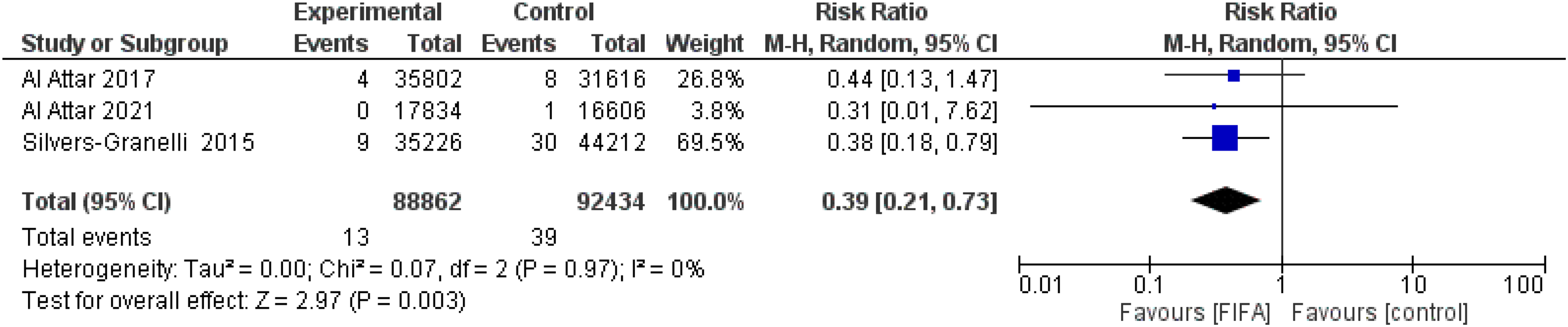
Forest plot of trials comparing the effects of FIFA 11 + alone vs regular warm-up on overall incidence of acute lower back injuries in adult soccer players. The pooled IRR for the FIFA 11 + adult subgroup was 0.39 (95% CI: 0.21–0.73), indicating a 61% reduction in injury risk. Heterogeneity: Tau2 = 0.00; I2 = 0%. Random-effects model was applied.

Forest plot of trials comparing the effects of FIFA 11+ Kids alone vs regular warm-up on overall incidence of acute lower back injuries in child soccer players. The pooled IRR for the FIFA 11+ Kids subgroup was 0.28 (95% CI: 0.06–1.33), reflecting a 72% relative reduction, though not statistically significant (p = 0.11). Heterogeneity: Tau2 = 0.00; I2 = 0%. Random-effects model was used.
Sensitivity analyses
A leave-one-out sensitivity analysis was conducted to examine the influence of individual studies on the overall effect size. Excluding Silvers-Granelli et al. (2015) 2 reduced the pooled IRR from 0.37 to 0.45 (95% CI: 0.22–0.92). When each of the other studies was individually removed, the pooled IRR estimates ranged from 0.33 to 0.42, with all confidence intervals remaining statistically significant. These results suggest that no single study disproportionately influenced the overall findings, indicating the robustness of the meta-analysis.
Publication bias
Although our protocol specified that publication bias analyses would be conducted only if ten or more studies were available, Egger's regression test was performed to explore potential small-study effects. The test yielded p = 0.62, suggesting no evidence of publication bias. However, this result should be interpreted with caution given the small number of included studies (n = 5), which limits the power and validity of such tests.
Discussion
Principal findings
The current study represents the first comprehensive systematic review and meta-analysis of RCTs evaluating the efficacy of the FIFA 11 + injury prevention program in mitigating acute lower back injuries among soccer players. Our investigation yielded preliminary evidence that the implementation of the FIFA 11 + program may contribute to reducing lower back injuries among soccer players. The meta-analysis revealed a substantial 63% decrease in the incidence of lower back injuries per 1000 h of exposure (IRR = 0.37), though further high-quality research is needed to confirm these findings. Despite the statistically significant relative reduction, the absolute reduction in injury rates from 1.09 to 0.39 injuries per 1000 h is clinically modest. Practitioners and coaches should interpret these findings with caution, recognizing that the absolute risk reduction translates to less than one injury prevented per 1000 h of exposure. This translates to an NNT of 1429 h of exposure, meaning that one injury would be prevented for approximately every 20 players completing the FIFA 11 + program for one full season, assuming ∼70 h per player. Nevertheless, in high-volume settings, even modest absolute reductions may yield meaningful population-level benefits, especially in youth and amateur sports. Furthermore, the FIFA 11 + program has also been shown to reduce other types of sports injuries, particularly of the lower extremity. Therefore, its demonstrated effectiveness in reducing lower back injuries should be considered in addition to its other benefits, which strengthens the argument for its broader and more consistent implementation. It is also important to consider total exposure; soccer is the most popular sport worldwide. Based on national data, approximately one million adults in Australia play soccer regularly. Assuming an average of 75 min per player per week, this equates to roughly 1.25 million exposure hours weekly. Applying the observed absolute risk reduction of 0.70 injuries per 1000 h, nationwide implementation of the FIFA 11 + could prevent an estimated 875 acute lower back injuries per week, assuming full compliance and consistent exposure. This estimate is illustrative and should be interpreted with caution, acknowledging potential variation in compliance, training quality, and player adherence. 42
Our findings align with the outcomes of a previous systematic review by Barengo et al. (2014), which demonstrated the effectiveness of the FIFA 11 + program in reducing overall injury risks, including those related to the lower back, while also enhancing neuromuscular performance in soccer players. 28 Similarly, encouraging results were reported in another systematic review and meta-analysis focusing on the FIFA 11+ Kids injury prevention program, highlighting a significant decrease in injury risk among child soccer players. 43 The success of the FIFA 11 + programs in lowering the risk of lower back injuries may be attributed to their emphasis on improving balance, coordination, and strengthening both the upper and lower extremities, as well as the core and back muscles.
Injury causation in sports is inherently multifactorial, encompassing a dynamic interaction of intrinsic factors, such as biomechanics, flexibility, and prior injury history, along with extrinsic factors, including training load, playing surface, and environmental conditions. The FIFA 11 + program addresses specific risk factors, such as neuromuscular control and strength deficits, and should be considered a component of a comprehensive primary injury prevention strategy rather than a standalone intervention. This holistic approach aligns with the evolving understanding of injury mechanisms in both clinical practice and research.
This review focuses on gradual onset or repetitive strain injuries affecting the lumbo-pelvic region, which are associated with cumulative mechanical loading over time. Acute traumatic contact injuries, such as those caused by direct impacts or falls, are outside the scope of this review as they are less likely to be mitigated by neuromuscular training programs like the FIFA 11 + . This distinction ensures that the findings and recommendations of this study are appropriately targeted.
Injury prevention programs that include balance, coordination, and core stability exercises have demonstrated effectiveness in reducing injury rates across various populations and injury types. For example, systematic reviews and meta-analyses have shown that programs with balance training significantly reduce knee and ankle injuries in athletes, particularly when compliance and follow-up are emphasized. Similarly, RCTs have highlighted improvements in dynamic balance when combining plyometric and balance exercises, reinforcing their role in enhancing functional stability.44–50
As noted in the Results, there was some variability in the methods used to collect exposure data. This introduces potential inconsistencies in the reliability of exposure data. While athlete self-reports may be subject to recall bias, coach and observer logs provide more objective measures, albeit limited by inter-rater reliability.
Directions for future research
The current study, consistent with prior research, underscores the critical importance of integrating FIFA 11 + injury prevention programs into the warm-up routines of soccer players. We advocate proactive efforts from FIFA to encourage the widespread adoption of the FIFA 11 + injury prevention program, particularly among youth players. By doing so, teams can benefit from a full season of service with minimal injury risk to their players. Reduced injury incidents not only translate to less time lost in rehabilitation but also contribute to a decreased economic burden.28,51
The results indicate a potential beneficial effect of the FIFA 11 + program in preventing/reducing (acute) lower back injury, but these findings should be interpreted with caution due to the limited number of included studies and variability in study designs. Future research endeavors should delve into the dose-response relationship, exercise intensity, and the nuances of implementation and compliance with FIFA 11 + programs. A more comprehensive understanding of these parameters is paramount for the effective adoption and implementation of the FIFA 11 + program across various levels of soccer. Additional core and back-specific exercises could be investigated to explore whether they further optimize the preventive effect.
Expanding the focus of future research is crucial. Although our study primarily included children and pre-adolescent players, there is an urgent need to explore the effects of the FIFA 11 + injury prevention program on mature soccer players. As the program gains prominence, separate studies addressing both female and male players would contribute significantly to the body of knowledge in soccer injury prevention.
Future studies should aim to improve the classification of back injuries by consistently distinguishing between acute and gradual onset injuries. Such differentiation will allow for more precise evaluations of prevention programs and their specific efficacy in mitigating certain types of injuries. Analyzing the aetiological factors for the occurrence of lower back injury in soccer players might influence enhancement of the prevention program by specific exercises to mitigate the aetiological factors.
Strengths and Limitations: One notable strength of the current study lies in the meticulous approach taken to minimize heterogeneity between included studies, with the PEDro scale serving as a robust tool for assessing study quality. Widely recognized for its validity and reliability, the PEDro scale has been consistently applied in previous reviews. 52 We acknowledge the preference of Armijo-Olivo et al. (2015) 53 for reporting individual criteria rather than a summary score. Not all authors subscribe to that view, because a Rasch analysis has confirmed that it is valid to calculate the total PEDro score and to treat the total PEDro score as an interval level measurement. 52 To satisfy both views of this issue, in Table 3 we presented both individual criteria ratings and total quality scores. Those who prefer the individual criteria can ignore the total score. The PEDro scale has substantially better clinimetric properties than the Cochrane Risk of Bias 2 tool. 38
However, several limitations warrant consideration. The challenge of blinding both participants and trainers, while inherent in sports injury prevention trials, remains a potential source of bias that could impact the overall quality of the included trials. 54 The inclusion of a relatively small number of trials with only 61 injuries poses a limitation to the robustness of our conclusions. Nevertheless, the incorporation of cluster RCTs with substantial participant numbers and exposure hours strengthens the reliability of our results.
Additionally, the inclusion of trials with participants from diverse countries enhances the generalizability of our results, making them pertinent to soccer players globally. However, included studies were conducted in high-income countries, which may limit the generalizability of the findings to low-resource settings. Differences in access to medical support, coach education, and implementation infrastructure may influence both adherence and the overall effectiveness of the FIFA 11 + program in such contexts. Although we only include trials published in English, analysis of PEDro shows that < 2% of trials of physical interventions in the sports field are published in languages other than English and none of these examined FIFA 11+, so any language bias can be expected to be negligible. Another key strength of the current study lies in its comprehensive and systematic approach to synthesizing evidence on the effectiveness of the FIFA 11 + program in reducing lower back injuries.
In terms of population focus, our study predominantly featured children and pre-adolescent players, leaving a significant gap in understanding the effects of the FIFA 11 + injury prevention program on mature soccer players. Future research endeavors should broaden their scope to include adult players, with dedicated studies addressing both female and male participants and occurrence of acute and chronic lower back injury. This expansion would contribute vital insights to tailoring injury prevention strategies across diverse demographics within the soccer community. The findings of this review primarily reflect amateur and youth players, predominantly male, as these groups were the focus of the majority of the included studies. Future research should explore the effectiveness of injury prevention programs like the FIFA 11 + among professional players and female athletes, who remain underrepresented in the current literature. The subgroup analysis for the FIFA 11+ Kids program revealed a non-significant 72% reduction in lower back injuries (p = 0.11). This result should be interpreted with caution due to the limited number of studies and participants in this subgroup, as well as the generally lower incidence of injuries in children compared to older players. Further research with larger samples is needed to establish clearer evidence regarding the effectiveness of the FIFA 11+ Kids program in preventing lower back injuries.
Incidence was selected as the primary outcome measure in the current study because it was consistently reported across the included studies, allowing for standardized comparisons. However, we recognize that incidence alone may not reflect the full impact of acute lower back injury. Future research should incorporate measures of burden, including time-loss injuries and performance impairments, to provide a more holistic understanding of the impact of lower back injury on athletes. While incidence rates provide useful information about the frequency of lower back injury, they do not account for its functional burden. Incorporating measures of time loss and performance impacts in future studies would enhance the practical applicability of the findings.
The current study emphasizes the need for precise and consistent definitions of injury regions in sports research. Ambiguities in terminology, such as the use of ‘spine’ to encompass multiple regions, can lead to misinterpretations and highlight the importance of careful review and standardization.
The variability in exposure data collection methods across studies poses challenges to the consistency and reliability of the findings. While self-reported data may lack precision, coach-reported and observational data offer more structured reporting but can introduce observer bias. These methodological differences should be considered when interpreting the results, and future studies should aim for standardized data collection systems to enhance reliability.
Our findings indicate a reduction in acute lower back injuries in the intervention group (6 injuries) compared to the control group (16 injuries). However, it is important to note that a substantial portion of the data comes from the RCT study by Silvers-Granelli et al. (2015). 2 Excluding this study would reduce the sample size to a level insufficient for drawing robust conclusions. While the observed trend suggests a positive effect of the FIFA 11 + program, this does not imply conclusive evidence, as the small number of injuries and potential confounding factors limit the generalizability of these findings. While the FIFA 11 + program shows potential in reducing lower back injuries, it is crucial to interpret these results cautiously. Furthermore, correlation does not equate to causation, and other factors, such as player fitness levels, variability in coaching practices, adherence to the intervention, and external conditions, may have contributed to the observed outcomes. Assuming that the intervention and control groups were identically matched and that no external factors impacted the results, the observed differences would suggest the program's effectiveness. Nevertheless, these assumptions need to be rigorously tested through larger, high-quality RCTs to establish causation more definitively.
Conclusion
This systematic review and meta-analysis suggest that the FIFA 11 + warm-up program may reduce the relative risk of acute lower-back injuries in soccer players (IRR = 0.37; 95% CI 0.21–0.66), though the absolute reduction from 1.09 to 0.39 injuries per 1000 h is clinically modest. Further large-scale, rigorously reported RCTs—particularly in adult and female cohorts—are warranted to confirm these findings and to optimize program components for comprehensive low-back injury prevention. The robust evidence presented underscores the program's valuable contribution to enhancing player well-being and highlights its potential as a cornerstone in comprehensive injury prevention strategies within the realm of soccer. While our meta-analysis indicates a notable relative reduction in acute lower back injuries with the FIFA 11 + program, the clinical significance of this finding is limited given the low baseline incidence rate. Future research aside from analyzing aetiological factors for the occurrence of lower back injuries should emphasize both absolute and relative injury rate reductions to provide clearer guidance for clinicians and coaches. Compared to previous studies on FIFA 11+, which reported reductions in lower limb injury rates ranging from approximately 0.5 to 1.5 injuries per 1000 h, our observed reduction in acute lower back injuries (approximately 0.7 injuries per 1000 h) falls within a similar range. This supports the consistency of FIFA 11 + in reducing injury incidence across different anatomical regions, although clinicians should recognize the varying baseline risks and clinical implications for each injury type. As we move forward, embracing and advocating for the widespread adoption of the FIFA 11 + program emerges not only as a prudent choice for safeguarding player health but also as a strategic measure for fostering the longevity and sustainability of soccer participation globally.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.