
Abstract
Despite the widespread use of both High-Intensity Interval Training (HIIT) and Moderate-Intensity Continuous Training (MICT) among endurance runners, most systematic reviews over the past decade have examined heterogeneous populations, limiting the applicability of their findings to this athletic group. This systematic review specifically focuses on endurance runners and aims to synthesize current evidence on the comparative effects of HIIT and MICT across multiple adaptation domains. A total of 11 studies were analyzed, covering five key domains: physiological (e.g., oxygen uptake, heart rate variability), biochemical (e.g., lipid profiles, glucose metabolism), physical (e.g., endurance performance, pacing), biomechanical (e.g., stride length, ground contact time), and perceptual (e.g., rating of perceived exertion) adaptations. Both HIIT and MICT contribute to cardiovascular fitness, but HIIT has been associated with faster improvements in oxygen consumption, heart rate variability, and metabolic flexibility, alongside earlier gains in mitochondrial density and fat oxidation. MICT appears to promote more sustained enhancements in lipid profiles and glycemic control, supporting its role in long-term cardiovascular health. Biomechanical adaptations, such as improved running efficiency and reduced ground contact time, have been more frequently reported with HIIT, while both modalities contribute to reduced perceived exertion over time. These findings highlight the complementary benefits of HIIT and MICT for endurance runners and support their integration in periodized training programs to optimize performance adaptations.
Keywords
Introduction
Understanding how high-intensity interval training (HIIT) and moderate-intensity continuous training (MICT) differ in their effects on performance and physiology is crucial for designing effective endurance programs.1,2 While both are widely used in sport and exercise science, they elicit adaptations through markedly different training stimuli, leading to distinct time courses, magnitudes, and sustainability of improvements.3,4 This systematic review focuses specifically on the differences in chronic adaptations between HIIT and MICT in endurance-trained runners, a population for which direct multi-domain comparisons remain scarce.
HIIT, characterized by repeated bouts of near-maximal effort interspersed with recovery periods, elicits a potent metabolic and cardiovascular stimulus, whereas MICT involves prolonged continuous exercise at moderate intensity, promoting steady-state cardiovascular and metabolic adaptations.1,5 HIIT is associated with rapid improvements in maximal oxygen uptake (
In contrast, MICT supports progressive increases in stroke volume, lipid metabolism, and blood glucose regulation, which are particularly relevant for long-term cardiovascular health and endurance sustainability.2,14 Physiologically, the higher intensity of HIIT produces greater lactate accumulation and faster improvements in lactate clearance and glycogen utilization,11,15–17 whereas MICT maintains a lower metabolic strain, facilitating recovery and higher training volumes.3,18 These distinct demands result in different time courses and magnitudes of adaptation across multiple domains.
While numerous systematic reviews and meta-analyses have compared HIIT and MICT in terms of
The present review addresses this gap by systematically comparing HIIT and MICT in endurance-trained runners across physical, physiological, biochemical, biomechanical, and perceptual domains. This approach aims to generate sport-specific, evidence-based recommendations for optimizing performance while managing fatigue and injury risk in this athletic population.
Materials and methods
Study design
This systematic review was conducted in accordance with the updated Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines, 24 which reflect advances in methodology for identifying, selecting, appraising, and synthesizing studies. The protocol was not registered in the International Prospective Register of Systematic Reviews (PROSPERO) because the review did not include outcomes directly related to human health.
Information sources
One researcher (FM) independently searched four electronic databases to avoid a biased literature sample: PubMed, Scopus, Web of Science and Google Scholar. The searched covered all data available literature as of June 2025, with the date of the last search being June 30, 2025. Search alerts were created to monitor any new search results after the date of the last search up to July 20, 2025. Any articles identified by this search that were deemed relevant (based on title and abstract) were sent to one researcher (MB) for full-text eligibility assessment. Another researcher (LF) double checked the included papers from this assessment and modified the eligibility criteria to limit the scope of the systematic review. Hand searching of reference lists and forward citation searching of included studies was also used to identify articles.
Eligibility criteria
To be included, studies had to be: (1) written in English; (2) published in peer-reviewed journals; (3) conducted on a sample of at least eight participants; (4) involving subjects trained in the endurance discipline of running; (5) directly comparing two training methodologies (HIIT and MICT); (6) lasting at least four weeks; and (7) prescribing a minimum of three training sessions per week.
For the purposes of this review, “endurance-trained runners” were defined as recreational, competitive, or master runners with a documented training history of at least one year of continuous endurance running, typically engaging in three or more running sessions per week. Where available, reported
For the purpose of this review, HIIT was defined as an intermittent training modality consisting of repeated high-intensity efforts performed at or above 85%
MICT was defined as continuous aerobic exercise performed at 55–80%
Conference abstracts and theses were excluded due to the limited methodological detail typically available, which prevents accurate risk of bias assessment and complete data extraction.
Search strategy
A PICO strategy was used to build the search criteria. The terms included combinations of “high-intensity interval training” OR “HIIT”, “moderate-intensity continuous training” OR “MICT”, “interval training”, “continuous training”, AND “runners” OR “athletes” OR “distance runners”. Boolean operators were applied to maximize coverage. The search strategy was adapted to each database using controlled vocabulary (e.g., MeSH in PubMed). Additionally, we manually reviewed the reference lists of all included studies and relevant systematic reviews. No filters or restrictions were applied.
Study selection
Duplicate references were removed first by systematic review software (Rayyan, Quatar Computing Research Institute, Doha, Qatar) 25 and then manual methods. Two authors (MB and FM) independently screened titles and abstracts to determine initial eligibility using systematic review software (Rayyan). Blinding of authors was used to reduce bias during this process. Finally, the authors reviewed the full text to determine eligibility for inclusion based in the eligibility criteria. Disagreements in eligibility decisions were resolved through discussion, or with a third reviewer (MB) when required.
Data extraction and analyses
Data extraction was completed independently by two authors (FM and LF) using standardized form that was pilot tested on ten randomly selected included studies and refined accordingly. The data were then merged by one author (FM) and any discrepancies in the extracted data were resolved through discussion, or with a further reviewer (MB) consulted if required. Extracted data from each full-text article included: 1) study identification; 2) sample size); 3) demographic information (including sex, age, and competitive level); 4) training intervention; 5) assessment; and 6) comparison between groups. If insufficient data were reported, the authors were contacted by e-mail. When data were not presented in tables or text and when authors did not provide the requested data, these were extracted from figures using an online WebPlotDigitizer 26 where possible.
Assessment of methodological quality
The first reviewer (FM) assessed the methodological quality of studies using the following criteria adapted from CONSORT 2010 25 : A) groups at baseline had to be similar; B) baseline demographic and descriptive characteristics were provided for each group; C) subjects’ inclusion and/or exclusion criteria were clearly mentioned; D) primary and secondary outcome measures were predefined (including how and when they were assessed): E) reliability of outcome measure was investigated; F) treatment protocol was sufficiently described (in order to be replicable); G) acceptable compliance of 75%; H) dropouts (maximum <30%) were reported; I) groups were randomized; and J) for each primary and secondary outcome, results of each group and estimated effect size were reported (preferably with precision, such as 95% confidence interval). If there were uncertainty about scoring items, the second reviewer (LF) independently assessed the specific study. If there still was uncertainty about scoring items, a third reviewer (MB) independently assessed the study under review. For each of the above-mentioned items, one point could be scored and the total score of the methodological quality could range between 0 and 10. If an item was not present or not reported, 0 point was scored. Studies scoring 9–10, 6–8, 4–5, and 0–3 were classified as excellent, good, fair, and poor, respectively. 25 Depending on the study design of the included studies, some items were not applicable. Therefore, these items were excluded from the calculation of the quality of assessment.
Results
Search strategy
The initial search identified 350 titles. After screening based on the inclusion/exclusion criteria, 8 articles were selected for the review. The main reasons for exclusion, such as population not being endurance-trained runners, lack of HIIT vs. MICT comparison, or focus on non-running sports, are detailed in the PRISMA flow diagram (Figure 1).
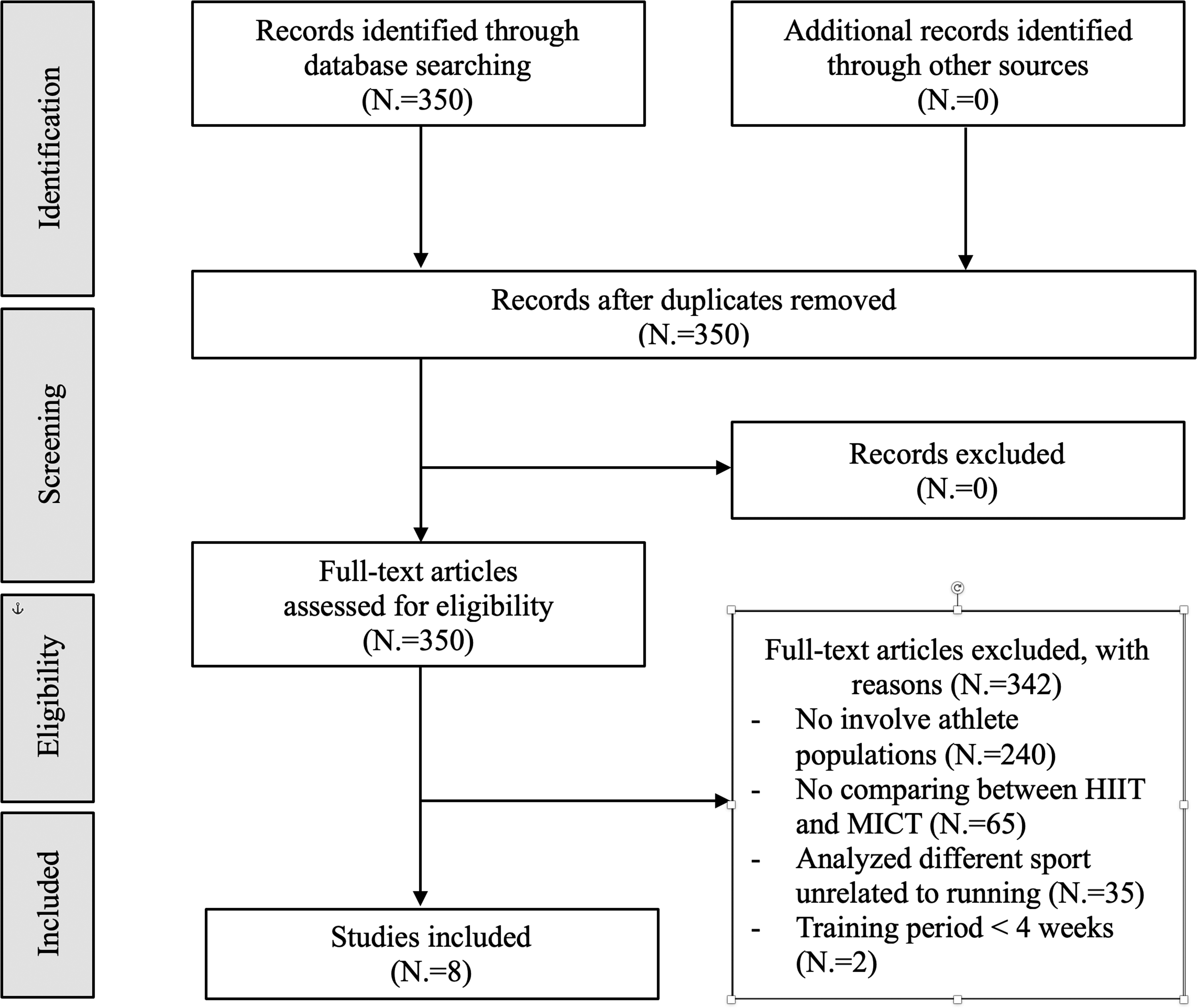
Flowchart of the selection process for inclusion in the systematic review.
Seven studies27–33 were conducted with parallel-group designs, while one 34 used crossover designs.
The average duration of the training protocols was 9.7 weeks, with a range from 6 to 16 weeks, while the total study durations (including testing phases, preparatory periods, or washout intervals in crossover designs) ranged from 6 to 24 weeks. The total number of participants in the included studies was 160; 3 studies involved men only (72 participants), 2 involved women only (40 participants), and 2 included both men and women (37 participants). One study did not report the gender distribution of the participants (11 participants).
The limited number of included studies reflects the strict eligibility criteria applied in this review, particularly the focus on endurance-trained runners and the requirement for direct HIIT vs MICT comparisons. This approach ensures homogeneity in the analysis but also restricts generalizability.
Reported quality
Study quality was assessed using a standardized scoring system based on key methodological criteria. Results of reported quality assessment are provided in table 1.
Risk of bias.
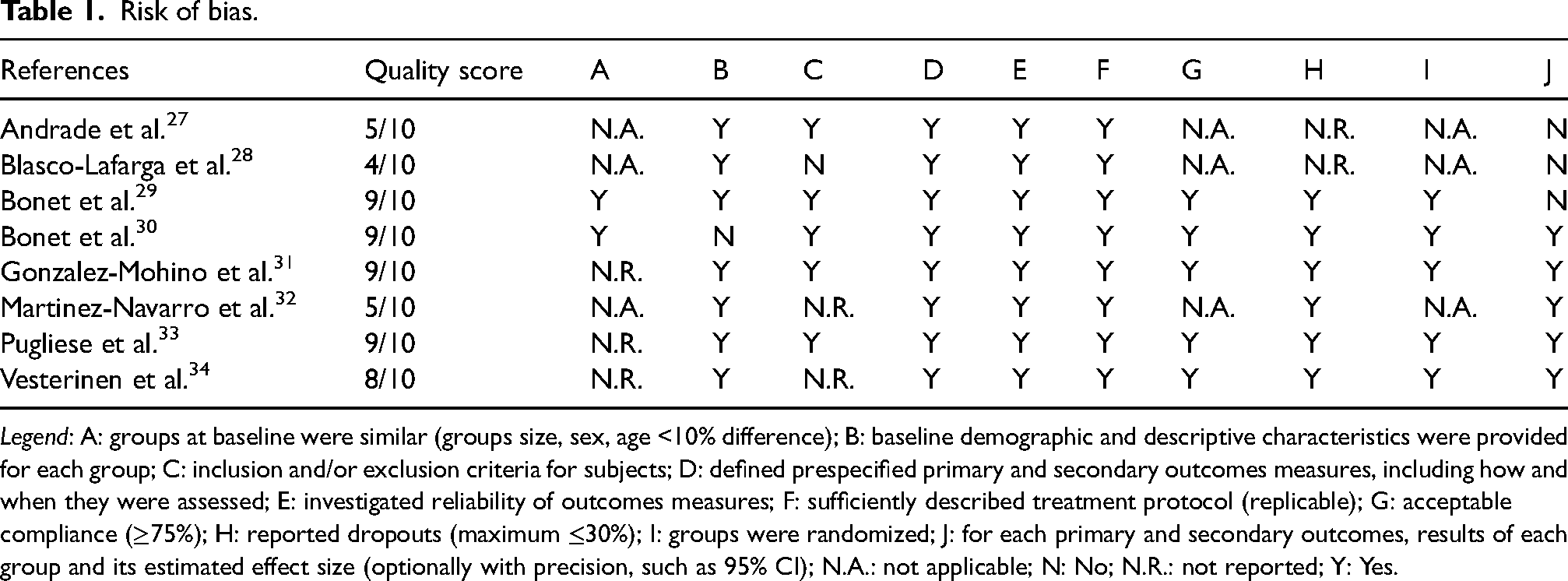
Legend: A: groups at baseline were similar (groups size, sex, age <10% difference); B: baseline demographic and descriptive characteristics were provided for each group; C: inclusion and/or exclusion criteria for subjects; D: defined prespecified primary and secondary outcomes measures, including how and when they were assessed; E: investigated reliability of outcomes measures; F: sufficiently described treatment protocol (replicable); G: acceptable compliance (≥75%); H: reported dropouts (maximum ≤30%); I: groups were randomized; J: for each primary and secondary outcomes, results of each group and its estimated effect size (optionally with precision, such as 95% CI); N.A.: not applicable; N: No; N.R.: not reported; Y: Yes.
The mean reported quality was 7.36, ranging from 4 to 9. Of the 8 included study, 4 were classified as excellent,29–31,33 1 was classified as good, 34 and 3 were classified as fair.27,28,32
Study outcomes
The included studies analyzed five categories of outcomes: i) physical, including performance-related measures such MAS, running economy, and time-trial performance; ii) physiological, assessing parameters like
Table 2 shows performance, physiological, biochemical, biomechanical, and perception outcomes of the examined studies.
Results on physical, physiological, biochemical, and perception of MCT and HIIT.
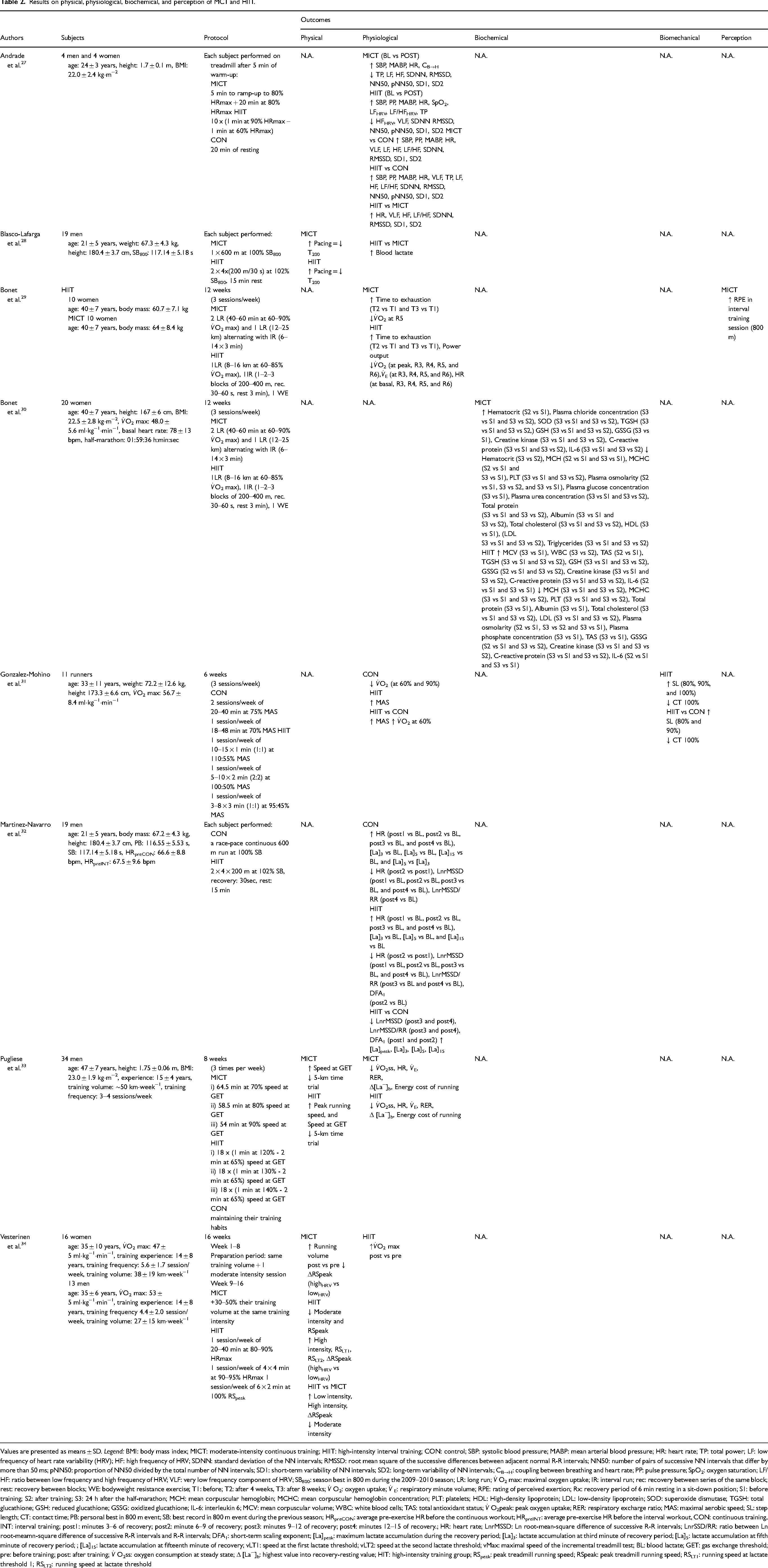
Values are presented as means ± SD. Legend: BMI: body mass index; MICT: moderate-intensity continuous training; HIIT: high-intensity interval training; CON: control; SBP: systolic blood pressure; MABP: mean arterial blood pressure; HR: heart rate; TP: total power; LF: low frequency of heart rate variability (HRV); HF: high frequency of HRV; SDNN: standard deviation of the NN intervals; RMSSD: root mean square of the successive differences between adjacent normal R-R intervals; NN50: number of pairs of successive NN intervals that differ by more than 50 ms; pNN50: proportion of NN50 divided by the total number of NN intervals; SD1: short-term variability of NN intervals; SD2: long-term variability of NN intervals; CB→H: coupling between breathing and heart rate; PP: pulse pressure; SpO2: oxygen saturation; LF/HF: ratio between low frequency and high frequency of HRV; VLF: very low frequency component of HRV; SB800: season best in 800 m during the 2009–2010 season; LR: long run;
Physical outcomes
Physical performance outcomes included running time-trial performance, peak running speed, and pacing strategies. Across studies, both HIIT and MICT improved endurance performance, but HIIT typically induced faster and larger gains.
In time-trial events, HIIT reduced completion times by approximately 5–8% over distances ranging from 200 m to 5 km, whereas MICT improvements were smaller (2–5%).28,33 Peak running speed increased by 5–7% with HIIT compared to ∼3% with MICT, and velocity at lactate threshold improved by 6–7% versus 2–3%, respectively. 34
Pacing efficiency also improved in both groups, but changes were more pronounced following HIIT, with greater reductions in variability and faster adjustments in short-distance events. 28
Overall, these findings indicate that while both training modalities enhance physical performance in endurance-trained runners, HIIT is more effective for improving high-intensity running capacity, submaximal velocity, and pacing control.
Physiological outcomes
Physiological outcomes included
Cardiovascular efficiency, as reflected by reductions in resting HR (−7 to −10 bpm) and respiratory minute volume (−15%) during standardized exercise, improved more with HIIT.29,33 HRV also showed favorable chronic adaptations, with increases in parasympathetic modulation and reduced sympathetic dominance after HIIT. 27
Blood lactate clearance improved more markedly with HIIT, with faster post-exercise reductions observed in standardized recovery tests compared to MICT.28,32 Time to exhaustion increased by around 10% with HIIT, whereas changes in MICT were minimal.
In summary, HIIT led to greater gains in aerobic capacity, submaximal efficiency, autonomic regulation, and lactate clearance than MICT, highlighting its effectiveness for enhancing endurance performance.
Biochemical outcomes
Biochemical adaptations, examined in one study, 29 showed that both HIIT and MICT improved lipid profile, antioxidant capacity, and metabolic regulation, with consistently greater changes following HIIT. Total cholesterol, LDL cholesterol, and triglycerides decreased by ∼15–20%, ∼18–20%, and ∼10–18% respectively after HIIT, compared to ∼10–12% reductions with MICT. Antioxidant markers, including total and reduced glutathione, increased by 15–18% with HIIT versus 10–12% with MICT, while superoxide dismutase activity rose by 17%, indicating enhanced oxidative defense. Metabolic parameters also improved more after HIIT, with reductions in plasma glucose (∼13%), albumin (∼8%), osmolarity (∼10%), and urea (∼12%), suggesting better glucose regulation, protein turnover, and hydration status. Overall, these results indicate a broader and more pronounced biochemical adaptation with HIIT compared to MICT.
Biomechanical outcomes
Biomechanical adaptations, reported in three studies,31,33,34 indicated that HIIT was generally more effective than MICT in improving running mechanics and economy. Stride length increased by ∼5–7% and contact time decreased by ∼6–8% across submaximal and maximal intensities following HIIT, compared to smaller changes of ∼3% and ∼4% respectively with MICT. 31 HIIT also improved running symmetry by ∼3%, reflecting enhanced neuromuscular coordination. Complementary findings showed greater improvements in running economy with HIIT, with reductions in energy cost of ∼6–7% versus ∼2–3% for MICT.33,34
Perception outcomes
Perceptual outcomes, assessed longitudinally in one included study, 29 indicated that HIIT was associated with consistently higher RPE values compared to MICT across the training period, reflecting its greater cumulative physiological and neuromuscular demands. Nevertheless, both groups demonstrated a progressive reduction in RPE from the initial to the final weeks of the intervention, suggesting improved tolerance and adaptation to the training load over time.
Discussion
This systematic review compared the chronic adaptations to HIIT MICT in endurance-trained runners across physical, physiological, biochemical, biomechanical and perceptual domains, with a focus on where and why these modalities differ. Physically, HIIT yielded larger short-term gains in time-trial performance, lactate-threshold velocity and peak running speed than MICT in our included trials, a pattern that aligns with meta-analytic evidence showing superior near-term improvements in performance-related markers and
Biochemically, in the only eligible study that tracked chronic blood markers, HIIT produced larger improvements in lipid profile (greater reductions in total and LDL cholesterol) and higher gains in antioxidant status than MICT over 8–12 weeks, mirroring prior mechanistic and training studies where high-intensity work accelerated mitochondrial enzyme up-regulation and metabolic flexibility.11,12,22,29 The likely drivers include stronger activation of AMPK/PGC-1α signaling, increased oxidative enzyme activity and enhanced lactate transport capacity (MCT1), which tend to be intensity-sensitive15,17; nevertheless, the same intensity that hastens adaptation may transiently elevate inflammatory mediators, underscoring the need for adequate recovery to avoid functional overreaching.36,39
Biomechanically, HIIT was associated with greater improvements in stride length and shorter ground-contact time than MICT, alongside larger reductions in running energy cost, suggesting faster gains in neuromuscular coordination and elastic energy utilization; repeated high-force, high-rate contractions at race-relevant speeds likely amplify motor-unit recruitment and stiffness optimization,31,33,34 whereas MICT offers smaller yet directionally similar changes via cumulative repetition at submaximal speeds. 36 Perceptually, HIIT elicited higher session RPE than MICT across the intervention period in the one study that tracked this outcome, although both showed declining RPE over time, an index of improving tolerance; this fits broader observations that MICT's lower perceived strain can facilitate high-volume phases and day-to-day compliance, 40 while HIIT's greater enjoyment in trained cohorts may sustain adherence when applied judiciously.10,41
Taken together, the comparative picture that emerges is that HIIT more effectively targets rapid enhancements in aerobic capacity, performance, metabolic regulation and running mechanics, whereas MICT more reliably underpins durable cardiovascular and autonomic adaptations at a lower perceptual cost. While HIIT tends to elicit faster and, in many cases, larger improvements in aerobic and metabolic parameters compared to MICT, its higher physiological and neuromuscular demands often necessitate longer recovery intervals between sessions.3,39 This can reduce the total weekly training volume, particularly during periods of high competition or concurrent training loads. In endurance-trained runners, balancing session intensity, recovery duration, and cumulative training volume is critical to sustaining gains and preventing maladaptation. Insufficient recovery following repeated HIIT sessions may lead to accumulated fatigue, compromised technique, or increased injury risk, potentially offsetting initial benefits. By contrast, MICT's lower recovery demands facilitate higher overall training frequency and volume, supporting long-term durability. A periodized approach that strategically integrates HIIT within a predominantly MICT-based program may therefore optimize both rapid performance gains and sustained physiological adaptations. Consequently, models that integrate the two (e.g., polarized periodization) are theoretically and empirically justified to balance speed of improvement with long-term robustness, aligning training intensity distribution with the athlete's goals, calendar and recovery capacity.3,36,42
Methodological considerations and limitations
The methodological quality of the included studies was generally rated as good to excellent according to adapted CONSORT criteria, with most trials reporting randomization procedures, baseline characteristics, and predefined outcomes. However, several factors limit the strength of the conclusions, particularly regarding the direct comparison between HIIT and MICT in endurance-trained runners. First, the small number of eligible studies (N = 8) reflects the specificity of the inclusion criteria ensuring population homogeneity but narrowing generalizability. Evidence from other populations, such as overweight adults, older adults, or sedentary individuals, confirms the efficacy of HIIT and MICT in improving cardiometabolic health,43–46 but the mechanisms and magnitude of adaptation may differ in highly trained endurance athletes.
Second, sampling methods were often based on convenience recruitment from recreational or club-level runners, with variability in training history, sex, and age potentially influencing responsiveness to HIIT and MICT. Third, the lack of standardized protocols (differences in frequency, session duration, target intensity (e.g., %
Most interventions lasted 3–12 weeks, which may capture the rapid phase of adaptation typically associated with HIIT but not the longer-term sustainability often attributed to MICT. In addition, adherence, enjoyment, and real-world feasibility (critical factors for interpreting “sustainable” adaptations) were rarely quantified. Finally, distinctions between acute and chronic responses were not always clear in the primary studies; in this review, acute effects (e.g., immediate RPE or lactate responses) were separated from chronic outcomes (e.g., changes in
These methodological constraints mean that conclusions about the relative speed and sustainability of adaptations to HIIT and MICT should be interpreted with caution. Nevertheless, despite the small number of studies and protocol variability, the present synthesis highlights consistent patterns suggesting that the two modalities produce complementary benefits. This supports the rationale for integrating HIIT and MICT within a periodized training framework, allowing athletes to leverage the rapid gains associated with HIIT while building the long-term cardiovascular stability fostered by MICT.
Conclusion
Both HIIT and MICT promote relevant adaptations in endurance-trained runners, but their profiles differ: HIIT primarily accelerates improvements in aerobic capacity, neuromuscular performance, and metabolic function, whereas MICT supports the gradual consolidation of cardiovascular adaptations with lower perceptual load. These complementary characteristics make their combined use within periodized training frameworks an effective strategy to optimize performance and long-term endurance development. The choice of emphasis should be tailored to the athlete's competitive calendar, training phase, and recovery profile.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Not applicable.
Author contributions
Conceptualization: LF and MB; Methodology: FM and MB; Writing—original draft preparation: FM and MP; Writing—review and editing: LF, EF, and MB. All authors have read and approved the final manuscript.