
Abstract
The aim of the study is to utilize the Rosenbaum Concussion Knowledge and Attitudes Survey (RoCKAS) with adults in the middle east and north Africa (MENA) to examine the knowledge and attitudes of adult athletes and coaches participating in any sports using exploratory cross-sectional study design. Independent sample t-testes, analysis of variance (ANOVA) and multiple regression analysis were utilized. The responses were collected from 253 participants (Athletes = 200; Coaches = 53). Among athletes, CKI was significantly different between genders (p = 0.002), athletic level (p = 0.023), and sport type (p = 0.007). For athletes, age groups significantly differed in CAI scores (p = 0.031) and athletic level (p = 0.01). For coaches, both CKI and CAI were significantly different between age groups (p = 0.025 & p = 0.04). Having a diploma or bachelor's degree was a significant predictor of decreased CKI (B = -5.27, p = 0.005 & B = -3.19, p = 0.003, respectively). In coaches, having 6–10 years of experience (B = 6.48, p = 0.036) or >15 years of experience (B = 10.73, p = 0.008) were significant predictors of increased CKI scores. In conclusion, athletes and coaches in MENA appear to have the basic foundational knowledge of SRC and some degree of safe attitude toward SRC. In coaches, years of experience were predictor of sport-related concussion (SRC) knowledge and attitude. Tailored awareness is needed for athletes and coaches across different sports in MENA to improve their recognition and management of SRC.
Introduction
Concussion is a traumatic brain injury that occurs as a result of a direct or indirect high impact collision to head, neck or body, resulting in an impulsive force.1,2 Concussion injuries, which often occur during sports competitions or practice, have been termed Sport Related Concussion (SRC). 3 SRC has been designated a public health issue, affecting around 3 million athletes annually in The United States Of America (USA).4,5 SRC injuries can be extremely debilitating symptoms for athletes, both in the immediate (i.e., after the injury occurred) and later stages after the injury.1,6 SRC has been suggested to contribute to neurological degeneration causing cognitive, motor, and psychological impairments. 7 SRC is considered a functional derangement despite structural changes including reduced blood flow to certain areas of the brain after the injury, due to the functional sequelae that accompany the injury. 8 Rapid return to play after SRC was found to cause irreparable brain damage, evident by persistent neurological symptoms, was found in athletes who returned to play 24 h after an SRC injury if it was not managed properly. 7
According to the International Conference of Sport Concussion, several endeavors have been made to develop tools utilized in the detection of SRC.2,6 Among these is the Concussion Recognition Tool-6 (CRT6), which targets non-medical practitioners to recognize incidents of concussion in children and young adults. A similar tool is the Sport Concussion Assessment Tool-6 (SCAT6), which was developed to be used by medical practitioners and is wildly used in clinical settings. Both the CRT6 and the SCAT6 were designed to be used in the immediate phase (up to 72 h) after any suspected SRC, while the Sport Concussion Office Assessment Tool-6 (SCOAT6), was intended to be used in the later stages (after the 72-h window) following the SRC injury. 6 Nevertheless, in order to utilize these tools, basic knowledge of SRC's signs/symptoms and safe attitudes toward SRC should be adopted by athletes and coaches.
The reporting practices for concussions have been a focus in the literature in reference to both athletes and coaches given their impact early detection and management of SRC in athlete. 9 Pressure to return to play after a suspected SRC was measured among college athletes in the USA using an question enquiring about their reporting intentions with a 7-points Likert scale and 26.5% reported that they experienced at least one source of pressure to continue playing (i.e., coaches, teammates, parents and fans), with coaches being the most frequent source of this pressure. 9 Interestingly other studies, in the USA, exploring sex differences on SRC reporting behaviors have found that female athletes were more inclined to report SRC injuries and symptoms compared to male athletes.10,11
One factor that may impact the reporting practices when it comes to SRC injuries and referrals for further diagnostic testing is the baseline knowledge of the signs and symptoms of concussion. A widely used tool in assessing knowledge and attitude toward SRC is the Rosenbaum Concussion Knowledge and Attitudes Survey (RoCKAS). 12 In a study exploring premature pressure to return to play, athlete knowledge levels of SRC did not influence the reporting of a concussion injury, showing that the knowledge alone did not allow for safer practices among athletes. 9 In contrast, other studies have found that rugby players were found to think that head impact and loss of consciousness were requisites for the classification of an injury as a concussion.13,14 The same athletes were also not aware of the long-term effects of concussions and reported leaning toward continuing a game even if suspected of concussion. This showed that there is a lack of knowledge among athletes of a contact sport which was associated with harmful practices.
To date, only one study has explored the knowledge and attitudes towards concussion in athletes in the middle east and north Africa region (MENA), however, this was conducted with adolescent athletes (n = 234). 15 Although this work explored adolescent athletes (i.e., < 18 years), it provided a valid and reliable culturally adapted and translated Arabic version of the RoCKAS-ST which serves to accommodate the population of MENA region. MENA is recognized as a common region,16–18 which include Algeria, Bahrain, Djibouti, Egypt, Iraq, Jordan, Kuwait, Lebanon, Libya, Malta, Morocco, Oman, Palestine, Qatar, Saudi Arabia, Syria, Tunisia, United Arab Emirates, and Yemen. These counties share several cultural, educational, healthcare, and sports-related characteristics that may contribute to similar perspectives and practices regarding concussion recognition and management. 19 Therefore, primary aim of the current study is to utilize this tool with adults in MENA countries to examine the knowledge and attitudes of adult athletes and coaches aged 18–65 years participating in any sports. The secondary aim for the study is to identify, if any, the variables that would predict the athletes and coaches’ knowledge and attitudes toward concussion.
Methods
Study design
This was an exploratory cross-sectional study that investigated SRC knowledge and attitudes of athletes and coaches from various sports across the MENA region. The inclusion criteria for this study were 1) athletes and coaches needed to have participated in at least one tournament as an adult, 2) participants were between the ages of 18–65 years. The exclusion criteria for this study was individuals with mental and physical disabilities. This project was approved by the research ethical committee at Kuwait University (VDR / EC – 05), in accordance to the Declaration of Helsinki.
Procedure
An online form (Google Forms™) was used to collect participant responses, which included the consent form that was signed electronically. The recruitment utilized purposive sampling where sporting institutions around the MENA region were contacted, and the questionnaire link was sent to them. Social media was also utilized where a post was circulated with the inclusion and exclusion criteria and the link to the questionnaire. Snowball sampling was also employed in terms of encouragement of participants to inform their colleagues about the study.
Instruments
The online form comprised a demographics section that included age [18–25 years, 26–35 years, 36–45 years, or >45 years], gender, educational level, sport type [individual vs. team sports], athletic level [amateur vs. semi-professional vs. professional], number of years of experience, nationality, and previous diagnosis of SRC [for the athlete him/herself or the coach]. These criteria were used to extract enough information describing athletic profile of the athletes and coaches. These terms were operationally defined as the following and were provided in the online form to ease the selection process for participants:
Team sports: were any sport where an interaction between players was vital for the success of the team, during a particular competition.
20
Individual sports: were sports where players were solely responsible for success, during a particular competition.
20
Professional athletes: were any athlete that has a written contract with a certain institution, and it entails receiving a regular salary for their full-time participation in a certain sport.
21
Semi-professional athletes: were an athlete that has a written contract with a certain institution, and it entails receiving a regular monetary incentive for their part-time participation in a certain sport.
21
Amateur athletes: were an athlete that is not associated with any institution and does not receive an incentive for their participation in any sport or athletic endeavor.
21
The participants were presented with the RoCKAS-ST questionnaire, which consists of five sections. Section 1 includes 18 questions regarding SRC knowledge with true and false options. Section 2 includes 3 scenario-based questions in the same format, whereas sections 3 and 4 explored attitudes towards SRC using a 5-point Likert scale with 8 scenario-based questions (i.e., agree/ strongly agree, neutral, and disagree/ strongly disagree). The final section includes 16 items of a symptom recognition checklist, with 8 correct symptoms (i.e., feeling in a “fog”, headache, feeling slowed down, sensitivity to light, difficulty remembering, difficulty concentrating, dizziness, drowsiness), and 8 distractor symptoms (i.e., hives, weight gain, difficulty speaking, arthritis, reduced breathing rate, excessive studying, panic attacks, hair loss). Scoring of the questionnaire was completed using the scoring key presented by Rosenbaum and Arnett (2009). 22 There were 3 validity questions (Section1, questions 4, 10 &15). If more than one question was answered incorrectly, the response was considered invalid and was included in the final analysis. The online form was available in both Arabic and English. The Concussion Knowledge Index (CKI) has a maximum score of 26, with higher scores indicating increased knowledge. For the Concussion Attitude Index (CAI), calculations were made using from sections 3 and 4, with a raw score ranging between 15–75. The calculation were done based on the scoring key provided by Rosenbaum and Arnett (2009). 22 Depending on the scenario, selections demonstrating a safe attitude would be provided a score of 1 with a maximum score is 15.15,22
Data analysis
Data analyses were conducted using IBM® SPSS Statistics for Windows, Version 27.0 (IBM Corp., Armonk, NY, USA). All continuous variables were evaluated by the Shapiro–Wilk and Kolmogorov–Smirnov tests to assess for normality of distribution. Descriptive analyses were conducted to calculate the frequencies and proportions of the categorical variables (i.e., biological sex, age, education level, sport types, years of experience, previous diagnosis of SRC, and athletic level) and were expressed as count (n) and percentage (%). Means and standard deviations (mean ± SD) were calculated for continuous variables (i.e., CKI score, CAI score). An a priori power analysis for multiple linear regression indicated that a minimum sample of approximately 170 participants was required to detect a medium effect size (f2 = 0.15) with 22 predictors, an alpha level of 0.05, and a statistical power of 0.80.
An independent samples t-test was used to determine whether any differences existed in the total mean scores of CKI and CAI between athletes and coaches. Assumptions for the independent samples t-test were evaluated, including the homogeneity of variances using Levene's Test. In addition, a one-way Analysis of Variance (ANOVA) compared mean scores of CKI and CAI across categorical sample characteristics with >2 levels (i.e., age, education level, years of experience, and athletic level), and independent samples t-test for binary sample characteristics (i.e., biological sex, sport types, and previous diagnosis of SRC), stratified by target population (athlete and coach). Effect size was calculated using Cohen's d and Eta squared (η2). The effect sizes were interpreted as d ≈ 0.20 as small, d ≈ 0.50 as moderate, and d ≥ 0.80 as large for Cohen's d; whereas the interpretation was η2 ≈ 0.01 as small, η2 ≈ 0.06 as medium, and η2 ≥ 0.01 as large for Eta squared. 23
Multiple regressions analyses were performed to explore the impact of any associated predictors on CKI and CAI scores among athletes and coaches. The primary outcome was defined as a continuous variable (CKI and CAI scores). Predictors variables were defined as a categorical variable included biological sex, age group, education level, sport type, years of experience, history of sports-related concussion (SRC), and athletic level. Reference categories were defined for all categorical variables. Separate regression models were built for each outcome variable within each subgroup (athletes and coaches). All assumptions of linear regressions were evaluated prior to analysis. The models were evaluated for linearity between predictors and outcomes using visualization of the standardized residuals against their normal scores by graphing Q-Q plots. In addition, independence of errors was evaluated using the Durbin–Watson test statistic. Furthermore, the variance of the residuals (homoscedasticity) was assessed by plots of standardized residuals versus predicted values. Moreover, multicollinearity was tested prior to model building using the Variance Inflation Factor (VIF) index, and values greater than 5 indicated multicollinearity. 24 Results were presented as unstandardized coefficients (B), standard errors (SE), t-values, and p-values.
Results
Demographics
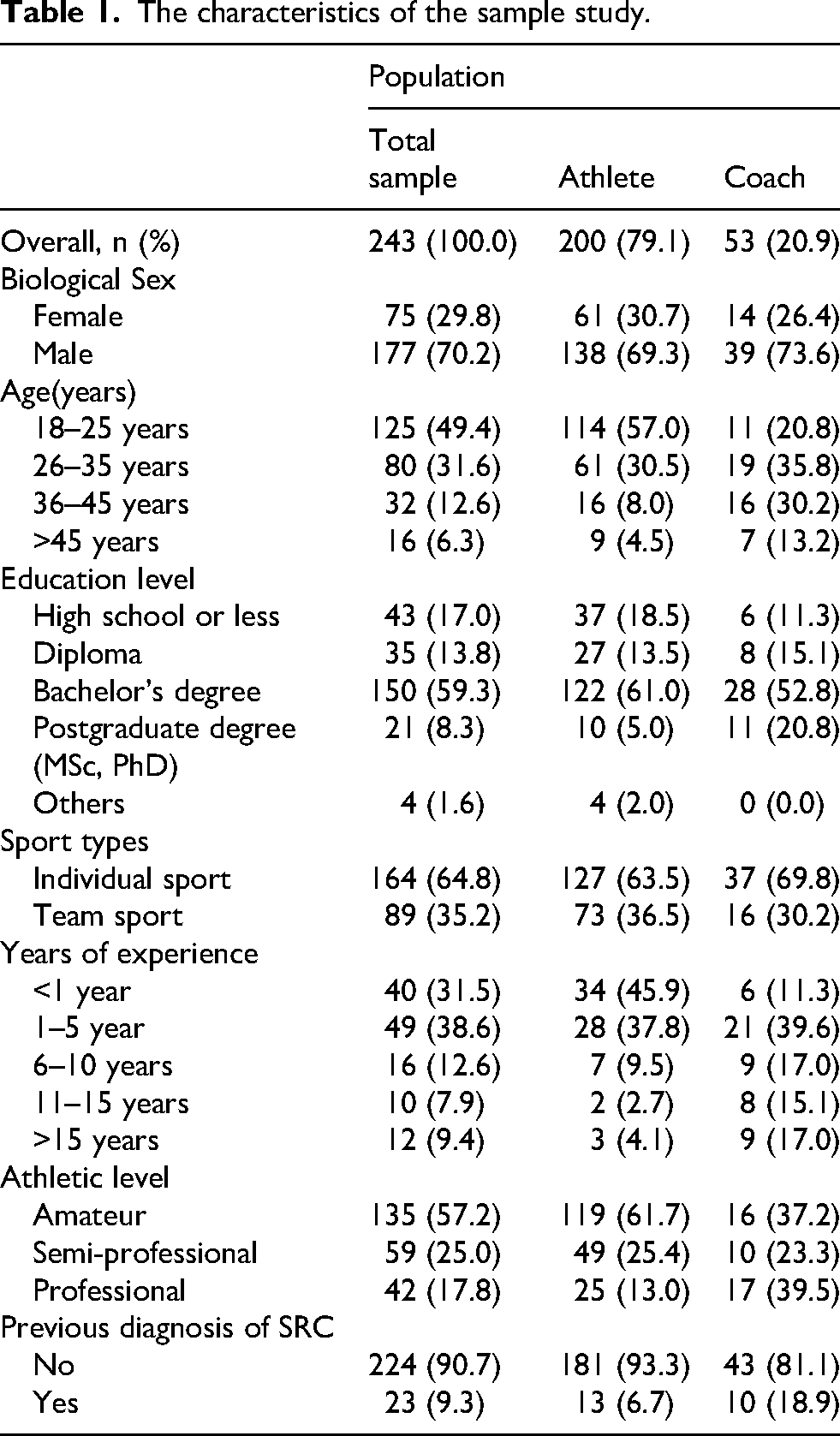
Two hundred fifty-three athletes (n = 200 [79.05%]) and coaches (n = 53) participated in this study. Most participants were males (n = 177 [70.2%]), which was consistent across both groups (male athletes = 138 [69.3%]; male coaches = 39 [73.6%]). Almost half of the participants (n = 125 [49.4%]) were between 18–25 years old (athletes=114 [57.0%]; coaches=11 [20.8%]), with those others being older. A bachelor's degree was the educational level for more than half of the participants (n = 150 [59.3%]; athletes = 122 [61.0%]; coaches=28, [52.80%]). Individual sports were the dominant type practiced (n = 164 [64.80%]; athletes = 127 [63.50%]; coaches = 37 [69.80%]). The majority had less than one year of experience (n = 34, 45.9%). As a group, most athletes reported being an amateur level (n = 119, 61.70%). On the other hand, more than one-third of the coaches reported coaching as professionals (n = 17, 39.50%). The majority of athletes reported having not sustained an SRC (n = 181, 93.30%), nor had coaches coached an athlete who had sustained a SRC (n = 43, 81.10%) (Table 1). Although 83% (n = 210) of the participants were from Kuwait, several nationalities participated in this study from around the MENA region [Saudi Arabia n = 9 (3.6%); Egypt n = 8 (3.16%); Jordan n = 5 (2%); Syria n = 4 (1.6%); Qatar & Tunisia each n = 3 (1.2%); Bahrain & Iraq each n = 2 (0.8%); Oman & United Arab Emirates each n = 1 (0.4%); Others n = 5 (2%)]. Descriptive detailed response of each question of the RoCKAS-ST question is provided in Supplementary Tables 1–4.
The characteristics of the sample study.
Concussion knowledge index (CKI)
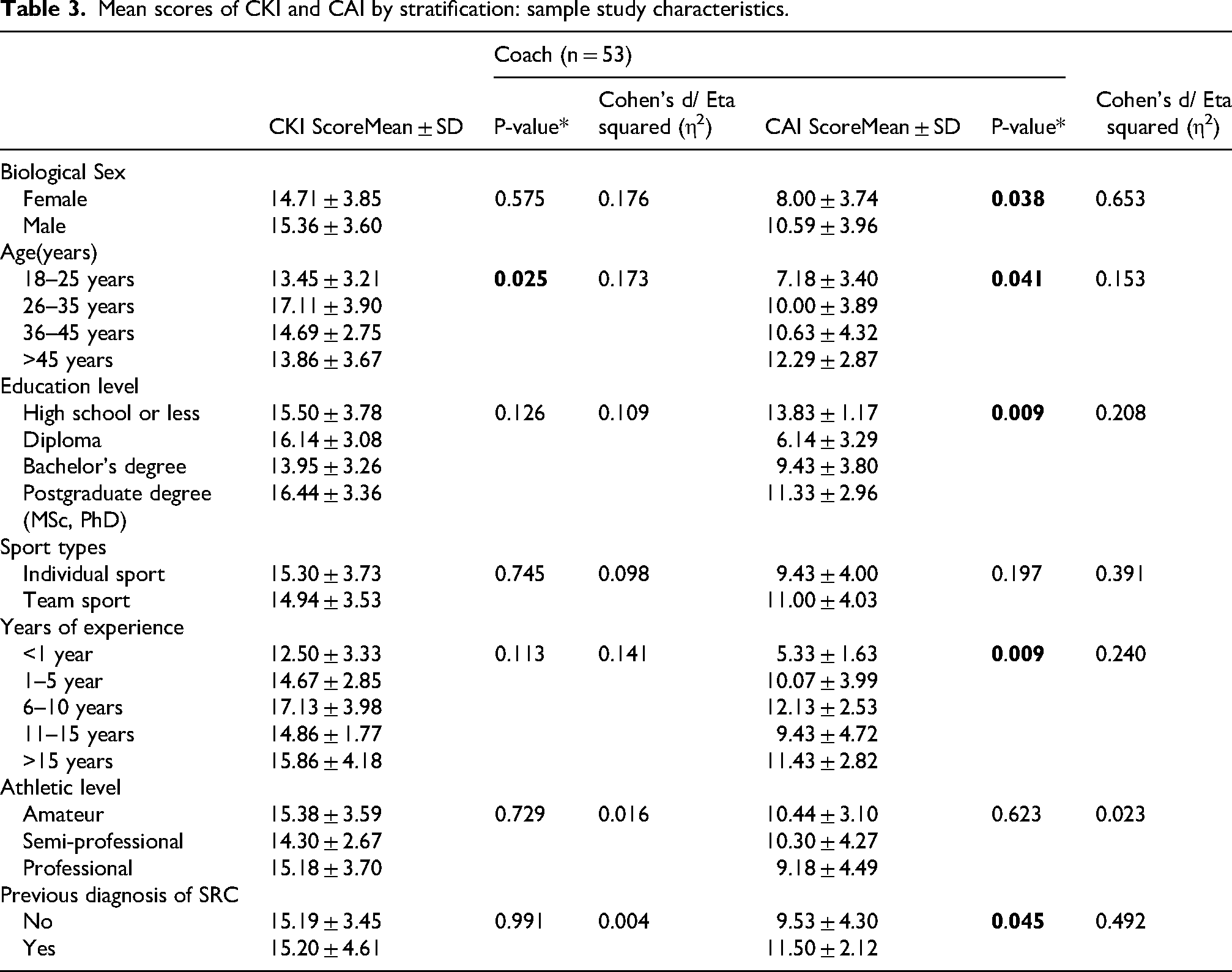
Female athletes had a significant greater concussion knowledge than their male counterparts, as defined by the CKI (female = 15.74 ± 3.29 vs. male = 14.14 ± 3.34, p = 0.002). Likewise, athletes participating in individual sports scored significantly higher CKI compared to athletes participating in team sports (individual sports=15.09 ± 3.39 vs. team sports=13.74 ± 3.33, p = 0.007). Athletes practicing at an amateur level scored significantly the highest across all levels on the CKI (14.11 ± 3.01, p = 0.023) (Table 2). For coaches, CKI was significantly different between age groups (p = 0.025). Post hoc analysis revealed that 26–35 age group scored statistically higher than 18–25 age group (17.11 ± 3.90 vs. 13.45 ± 3.21, p = 0.034). Effect sizes of CKI scores were reported for both athletes and coaches (Tables 2 and 3). There was no significant difference in terms of CKI scores between athletes and coaches (14.60 ± 3.40 vs. 15.19 ± 3.64, p = 0.269).
Mean scores of CKI and CAI by stratification: sample study characteristics.
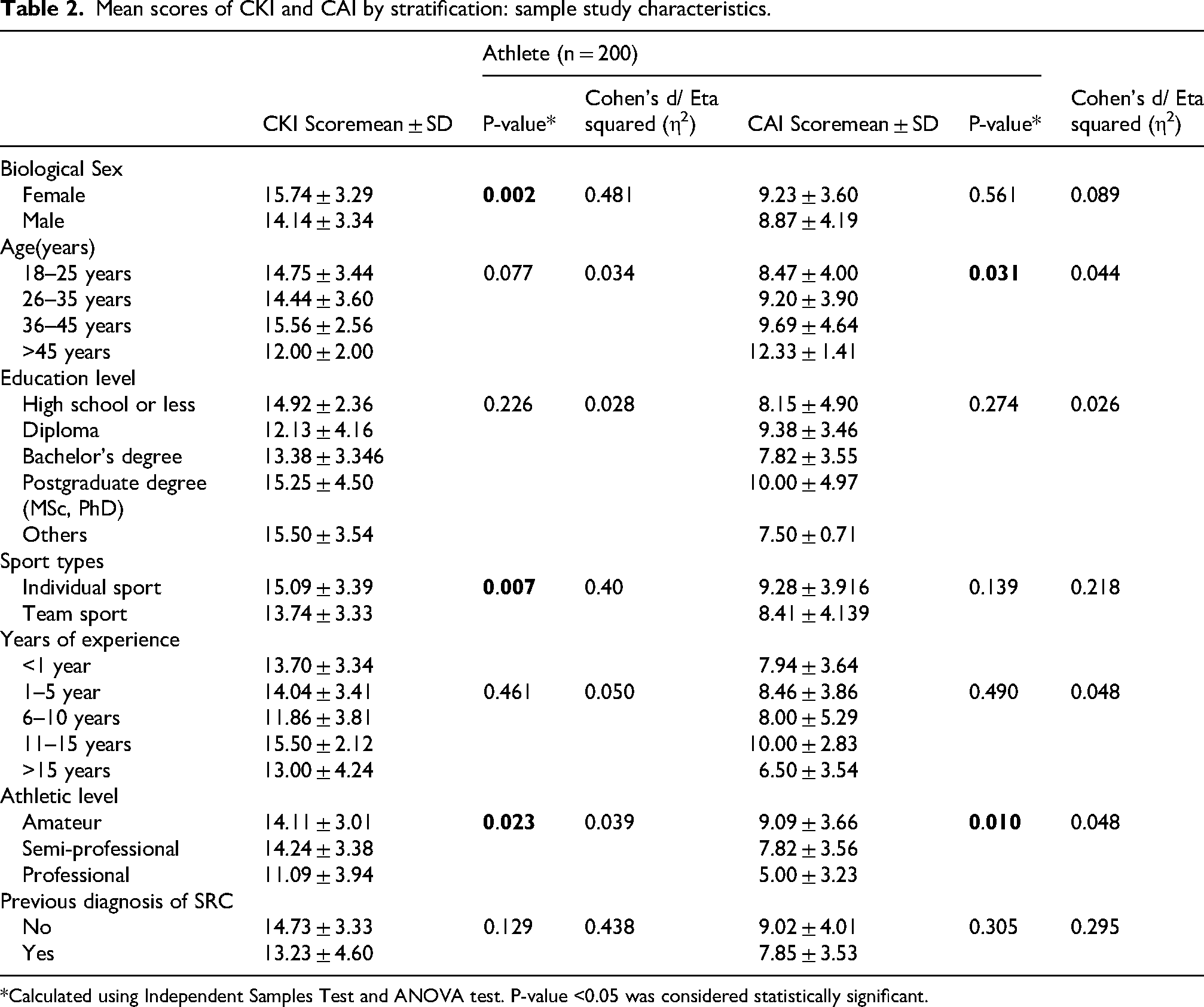
*Calculated using Independent Samples Test and ANOVA test. P-value <0.05 was considered statistically significant.
Mean scores of CKI and CAI by stratification: sample study characteristics.
Concussion attitude index (CAI)
Athletes practicing at a professional level scored significantly lower across all levels on the CAI (5.00 ± 3.53, p = 0.010; vs. amateur, p = 0.008 & vs. semi-professional, p = 0.026). Additionally, athletes significantly differed on age groups in CAI (p = 0.031), with athletes aged more than 45 years scoring significantly higher than 18–25 age groups (12.33 ± 1.41 vs. 8.47 ± 4.00, p = 0.027) (Table 2). For coaches, CAI was also significantly different between age groups (p = 0.041), where coaches aged more than 45 years scored significantly higher score compared to 18–25 years age group (12.29 ± 2.87 vs. 7.18 ± 3.40, p = 0.039) and between genders (males scoring highest, 10.59 ± 3.96, p = 0.038). Educational levels were also significantly different on CAI scores (p = 0.009). Coaches with a high school degree or less (13.83 ± 1.17) had the highest CAI scores compared to Diploma holders (6.14 ± 3.29, p = 0.010) and Bachelor's degree holders (9.43 ± 3.80, p = 0.044). CAI significantly differed between coaches with different years of experience (p = 0.009). Coaches with <1 year of experience (5.33 ± 1.63) had significantly lower score compared to coaches with 6–10 years of experience (12.13 ± 2.53, p = 0.010) and >15 years of experience (11.43 ± 2.82, p = 0.011). Finally, coaches of athletes that reported a previous concussion diagnosis scored significantly highest on the CAI compared to the coaches that did not (11.50 ± 2.12, p = 0.045) (Table 3). Effect sizes of CAI scores were reported for both athletes and coaches (Tables 2 and 3). No significant difference was found between CAI scores of athletes and coaches (8.97 ± 4.01 vs. 9.91 ± 4.04, p = 0.131) (Figure 1).
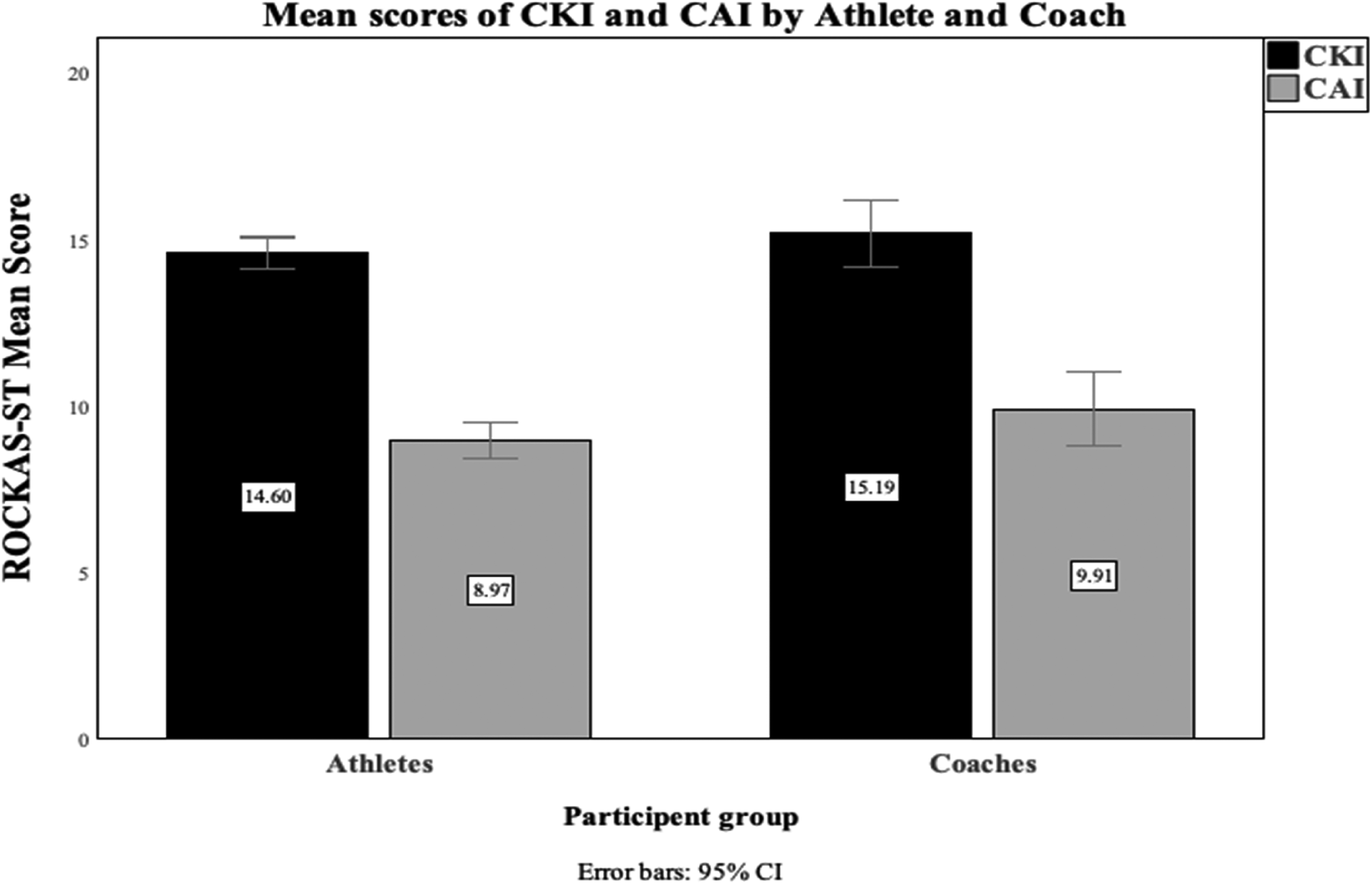
Mean scores of CKI and CAI by athlete and coach.
Linear regression models
Multiple linear regression models revealed that in athletes, having a diploma and bachelor's degree was a significant factor of lower CKI scores (B = –5.27, p = 0.005 & B = –3.19, p = 0.003, respectively). Being aged between 36–45 years was a significant factor of increased CAI scores (B = 5.37, p = 0.024), while being a professional athlete was a significant factor of decreased CAI scores (B = –4.25, p = 0.005) (Table 4).
Predictor associated with CKI and CAI scores.
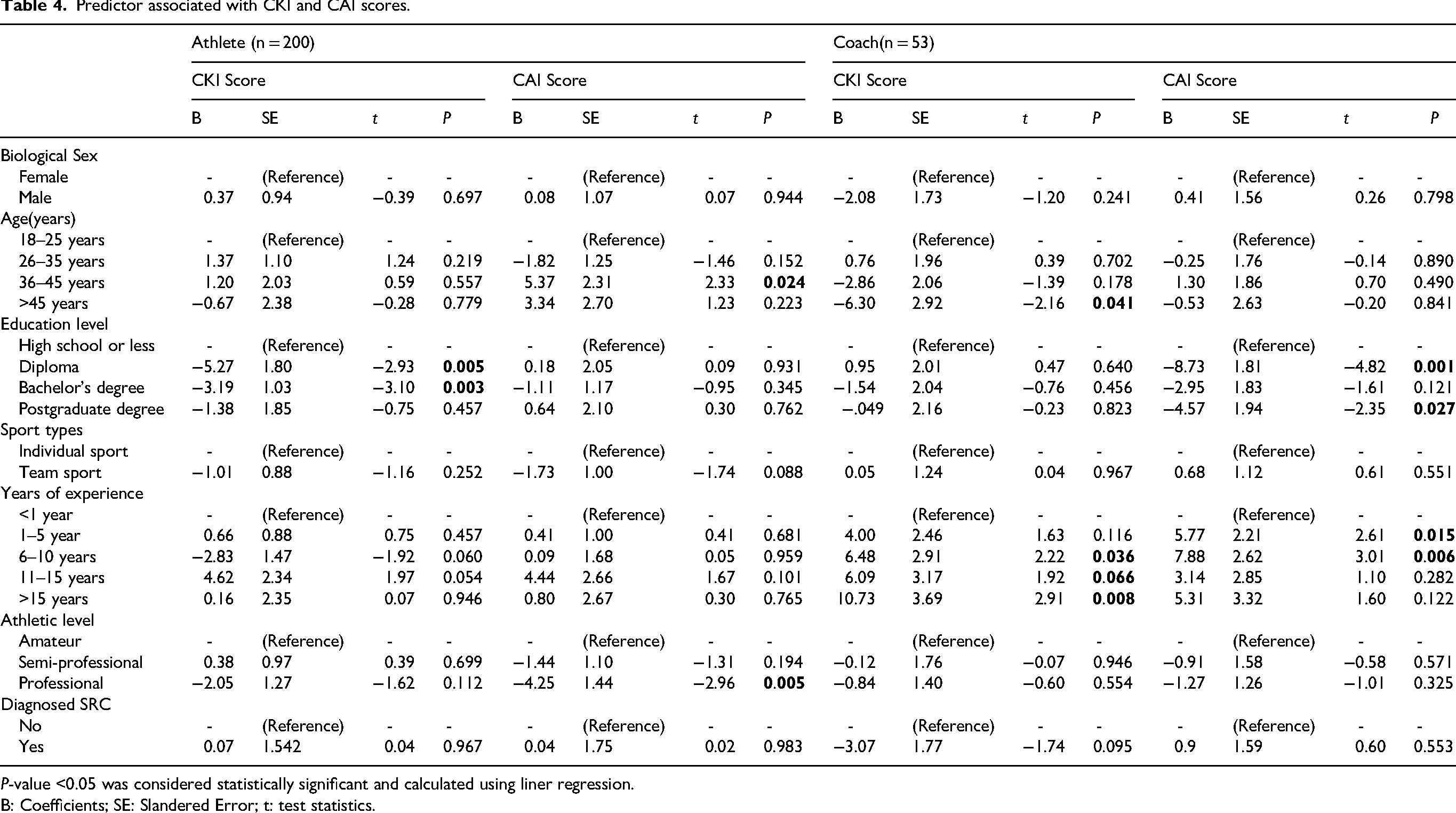
P-value <0.05 was considered statistically significant and calculated using liner regression.
B: Coefficients; SE: Slandered Error; t: test statistics.
In coaches, being aged more than 45 years was a significant factor of decreased CKI scores (B = – 6.30, p = 0.041). Having 6–10 years of experience (B = 6.48, p = 0.036) and >15 years of experience (B = 10.73, p = 0.008) were both significant factors of increased CKI scores. Likewise, having either 1–5 or 6 −10 years of experience were significant factors of increased CAI scores (B = 5.77, p = 0.015 & B = 7.88, p = 0.006, respectively). Finally, having a diploma and postgraduate degree were significant factors of decreased CAI scores (B = –8.73, p = 0.001 & B = –4.57, p = 0.027, respectively) (Table 4).
Discussion
This study examined the knowledge and attitudes of adult athletes and coaches aged 18–65 in the MENA region. Our results indicate that several factors influenced the coaches’ knowledge of SRC (i.e., age) and attitude toward (i.e., gender, age, educational level, years of experience, and training an athlete with previous SRC injury). On the contrary, athletes’ knowledge of SRC, on the other hand, was influenced by gender, sport type (i.e., individual vs. team sports), and athletic level. Similarly, their attitude toward SRC was influenced by age and athletic level. A significant factor of age was found to contribute to their results within the coach group, with ages between 26–35 years having the highest knowledge and ages >45 years having lower knowledge of SRC. This age-related difference may be due to openness of younger coaches in seeking this knowledge and learning about new issues. Having this type of knowledge is important because athletes have reported that 70% of their knowledge about SRC comes from their coaches. 25 It was also reported that coaches exert the highest pressure on athletes to return to play. 9 Coaches have previously been found to be only 38.9% of the time correct in identifying concussion and its symptoms in their athletes. 26
Interestingly, Salmon et al. 27 report significantly safer attitude scores for coaches aged >45 years, which may reflect openness towards SRC reporting but not the proper knowledge for implementation. In other words, lack of knowledge about SRC may hinder safe reporting practices regardless of positive attitudes. This was consistent with the results of Manseer et al. 12 where coaches older than 50 years had safer attitudes toward SRC compared with younger age groups. 12 Interestingly, the age finding may correspond to an increase in years of experience, where Manseer and colleagues also reported that coaches with 6–10 years of experience had significantly safer attitudes toward SRC. This could be caused by the fact that prior experience and first-hand exposure to SRC made these types of injuries more salient. These results are in line the findings in this study, where multiple regressions demonstrated that having 6–10 years of experience were predictors of better attitudes toward SRC. This is aligned with published literature where coaches with >5 years of experience scored significantly higher on CAI compared to coaches with <2 years of experience. 27 Moreover, coaches that trained athletes with previous SRC injury had significantly safer attitudes toward SRC than ones that did not. Similarly, athlete ages 36–45 years and > 45 years were significant predictors of safer attitudes toward SRC, which was comparable with the literature when examining professional and amateur cyclists. 28
Coaches with a high school degree or less had significantly safer attitudes toward SRC in our study. This could mean that exposure to formal academic education does not guarantee better attitudes toward devastating injuries like SRC, but instead years of experience and being exposed to SRC. This finding is not in line with other explorations of formal education in coaches, as educational level has been found to not affect the attitude of coaches.12,27 A similar finding was found in athletes in our study, where holding a diploma or bachelor's degrees were significant predictors of a decreased knowledge of SRC.
Semiprofessional athletes demonstrated significantly greater knowledge of SRC, while amateurs showed better attitudes. Echoing these results, being a professional athlete was a predictor of worse attitudes toward SRC. Higher risks are associated with being a professional which would explain these results; sustaining a SRC could affect the athlete's performance and could have monetary consequences during contract renewal and negotiations. This is in accordance to the literature where second category cyclists had worse attitudes toward SRC compared to recreational cyclists. 28 Athletes in individual sports and female athletes had significantly better knowledge of SRC, which is consistent with the literature.10,11,28,29
Notably, there was no significant differences between athletes and coaches in terms of either knowledge or attitudes toward SRC. This result may partially be attributed to a discrepancy in the sample size between the two groups (athletes n = 200 vs. coaches n = 53) or to similar knowledge and attitudes across both groups. Our findings contrast with those reported by Salmon and colleagues 27 where rugby coaches and players demonstrated significant differences, with coaches scoring higher on both indices of the ROCKAS-ST. 27 Our sample had much lower CKI score compared to this population in both coaches and athletes. 27 Similarly, Oluwaseyi and team showed that Nigerian players had higher CKI score than our sample. 30 Regarding CAI, they used the raw score of the index (range = 15–75), which when calculated for our sample and compared to their results, it was showed similar trend to CKI (Coaches: current study =51.65 ± 6.67 vs. Salmon et al.= 65.30 ± 5.40; Athletes: current study =50.36 ± 5.80 vs. Salmon et al.= 59.30 ± 6.80). 27
Although the majority of participants were from the State of Kuwait, there was several nationalities that also participated from the MENA region and others. Therefore, these preliminary results demonstrate that awareness is much needed among athletes and coaches in the MENA region. Awareness can be achieved through targeted campaigns that aim to improve the knowledge and attitudes of both groups toward SRC. Given that 64.3% of athletes reportedly use social media as their source of knowledge about SRC, 25 this information could be delivered through educational seminars and videos along with the use of social media, which is of increasing popularity for knowledge dissemination and public awareness among the younger generation. Sporting institutions and organization should also be keen on educating their staff, coaches, and athletes on SRC.
Like any scientific endeavor, some limitations existed in this study and should be acknowledged. Future studies should aim to include larger number of participants particularly the sample size of our coaches group. There was a lack of representation from different countries in the MENA region (i.e., other than Kuwait), which should be considered in future studies. The use of a questionnaire with fixed questions, which would limit the amount of information extracted from the participants. Future studies should explore qualitative approaches that would expand our insight into knowledge and attitude toward SRC. Longitudinal studies would also allow for a better understand of the perspectives of athletes and coaches on SRC. Another limitation was the discrepancy between genders, given that more male athletes participated in the current study. In addition, there was a lack of information obtained regarding the age group that participating coaches were training, which prevented further analyses to compare coaches of younger athletes versus those of older athletes.
Conclusion
Coaches’ knowledge of SRC was influenced by age whereas their attitude was influenced by gender, age, educational level, years of experience, and training an athlete with previous SRC injury. Athlete knowledge of SRC, on the other hand, was influenced by gender, sport type (i.e., individual vs. team sports), and athletic level. Similarly, their attitude toward SRC was influenced by age and athletic level. This study highlights the need to implement campaigns and educational programs to enhance both the knowledge and attitudes toward SRC in athletes and coaches in the MENA region.
Supplemental Material
sj-docx-1-spo-10.1177_17479541261462097 - Supplemental material for Knowledge and attitudes toward sport-related concussion among coaches and athletes in Middle East and North Africa region: Preliminary results
Supplemental material, sj-docx-1-spo-10.1177_17479541261462097 for Knowledge and attitudes toward sport-related concussion among coaches and athletes in Middle East and North Africa region: Preliminary results by Anwar B Almutairi, Abdullah Y Alabdelwahab, Maraheb Alkhalidi and Peter Theobald in International Journal of Sports Science & Coaching
Footnotes
Ethical considerations (including approval number)
Ethical approval for the current study was obtained from the ethical committee at Kuwait University (VDR / EC – 05). The study adhered to the Declaration of Helsinki.
Consent to participate
Signed written informed consent forms were obtained from all participants.
Consent for publication
Not Applicable
Author contributions
A.B.A interpreted the data, prepared ![]() and drafted the manuscript. MA analyzed the data and prepared the tables and substantively revised the final manuscript. A.A. interpreted the data and substantively revised the final manuscript. A.B.A., A.A., MA & P.T. have design of the work and acquired the data. All authors approved the submitted version of the manuscript.
and drafted the manuscript. MA analyzed the data and prepared the tables and substantively revised the final manuscript. A.A. interpreted the data and substantively revised the final manuscript. A.B.A., A.A., MA & P.T. have design of the work and acquired the data. All authors approved the submitted version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data that support the findings of this study are available from the corresponding author upon request (almutairi.anwar@ku.edu.kw).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.