
Abstract
Men in the criminal justice system experience significant health inequalities compared to the general population. Yet, research and policy attention have largely focused on the health needs of individuals in prison, overlooking those under community supervision. This study addresses this gap by exploring the physical health needs of men on probation and identifying ways to improve healthcare provision from their perspective. Using a mixed-methods approach, we surveyed and interviewed 33 men on probation in South Wales, UK, to explore their self-reported physical health conditions, barriers to accessing services, and ways in which provision could be improved. From a desistance and an inclusion health perspective, the voices of men on probation are key in shaping healthcare interventions. This study contributes to both academic and practice knowledge by providing empirical insights to inform “user-led” service design, offering recommendations for policymakers and practitioners seeking to reduce health inequalities, support desistance, and improve access to primary healthcare for justice-involved populations.
Introduction
Men involved in the criminal justice system (CJS) face disproportionate health challenges, experiencing significantly poorer physical health outcomes and higher mortality rates than the general population (Aldridge et al., 2018; Skinner and Farrington, 2023). Research has consistently highlighted that this population is burdened with chronic health conditions, mental health issues, substance misuse, and communicable diseases, often compounded by socioeconomic adversity, homelessness, and stigma (Martin et al., 2020; Plugge et al., 2014; Rabaiotti, 2024; Skinner and Farrington, 2023; Spaulding et al., 2011). In England and Wales, the health needs of people in the CJS have increasingly become a policy concern for His Majesty’s Prison and Probation Service (HMPPS), the Ministry of Justice (MoJ), the National Health Service (NHS), for both the UK and the devolved Welsh governments. Historically, most attention has been paid to prison health, with access to health provision remaining poor (Bowstead and Meek, 2024). However, more recent strategies have started to recognise the health challenges faced by those under probation supervision.
The HMPPS Reducing Reoffending Strategy for Wales (2022) outlines “seven pathways” to reducing reoffending, including accommodation, employment, finance, family, attitudes, and substance misuse. The strategic plan refers to drug treatment and mental health efforts, but there is a lack of emphasis on the need to strengthen broader health services for people under community supervision. Compared with NHS Wales, NHS England has historically been more progressive in its plans to improve the health of people in the CJS. For example, the NHS Long Term Plan (NHS England, 2019) included several explicit commitments to improve health services for people in contact with the CJS, including increasing investment in probation-specific mental health services and improving access to substance misuse treatment, including through joint working with probation services. Importantly, this is followed through into the NHS England (2021) Health and Justice Inclusive Workforce programme and Inclusion Health Framework, which further prioritises building a skilled workforce to deliver these commitments, recognising the importance of trauma-informed and inclusion health approaches (NHS England, 2023). Despite these positive commitments, the major health inequalities of people in the CJS still persist (Brooker, 2024; Rabaiotti, 2024; Sirdifield et al., 2019a, 2024; Williams et al., 2024). Furthermore, the updated Long-Term Plan has no specific health and justice reference other than priorities to reduce inequalities (Department of Health and Social Care (DOHSC), 2025). A report directly addressing the health of people on probation by the Chief Medical Officer for England may go some way to address this stark omission; however, concerns exist as to the future of sustained, collaborative, and appropriately funded inclusion health models (Jeffery, 2025; Whitty, 2025).
Within Wales, where the study outlined in this paper took place, the Welsh Government has devolved responsibility for the delivery of healthcare, with Public Health Wales (PHW, 2023) centring its strategy around fair and equal access and has recently developed a more concerted approach to inclusion health (PHW, 2025; Rabaiotti, 2024). Despite this, health and justice outcomes are even worse than in England due to the “jagged edge” of devolution (Jones and Jones, 2022). The “jagged edge” refers to the uneven and fragmented division of powers between Wales and England, whereby health, as well as housing, social services, and other local government responsibilities, are devolved to Welsh Government, but criminal justice is not and remains reserved to Westminster, creating gaps in policy alignment, accountability, and service delivery (Jones and Jones, 2022; Rabaiotti, 2024, 2025). Furthermore, in comparison to prison populations, little attention has been paid to the physical health needs of men on probation (MOP), and there is an evidence gap in examining health interventions and reduced reoffending (Cordle and Gale, 2025). While inclusion health principles, defined as interdisciplinary, person-centred approaches designed to reduce health inequalities among the most marginalised populations (Luchenski et al., 2018), have been increasingly championed in national policy, there is still limited practical discussion or evaluation of how these approaches can be systematically embedded within probation services (Rabaiotti, 2024). Much of the current policy emphasis remains focused on prison healthcare or the transitions from prison to community, leaving gaps in how to sustain accessible, equitable healthcare for those under community supervision alone.
In addition, these multiple national policies and strategies aimed at improving the health outcomes are missing the voices and lived experiences of MOP. While inclusion health principles advocate for co-production and the involvement of people with lived experience (Luchenski et al., 2018), most existing strategies have focused on system-level reforms without directly engaging with MOP in identifying barriers or designing solutions. Without actively including men on probation in policy development, service design, and evaluation, there is a risk that national efforts will continue to overlook the specific, ground-level realities, needs, and ideas that could most effectively drive improvements in healthcare access and equity for this population.
Study aims
As such, our study aimed to fill key gaps in knowledge to help inform solutions to address the physical health needs of MOP. Specifically, we sought to:
This study makes a key and timely contribution to the national and international conversation on inclusion health and, more broadly, desistance by foregrounding the physical health needs of one of the most marginalised and underserved populations in England and Wales: men under probation supervision. Desistance scholarship consistently emphasises the importance of addressing structural inequalities, supporting agency, and enabling access to social and personal resources, including health, as central to sustaining long-term change (Maruna, 2001; McNeill, 2012). In this context, unmet physical health needs and barriers to care can be understood as undermining the conditions necessary for desistance, while improved access to responsive, person-centred healthcare may act as a key enabler of it (Link et al., 2019). Whereas the overwhelming majority of criminal justice health research has focused on people in prison (Aldridge et al., 2018; Plugge et al., 2014; Skinner and Farrington, 2023), the experiences of men on probation (who represent the largest proportion of the supervised population in England & Wales) have received comparatively little scholarly or policy attention.
High-quality healthcare provision for this group requires meaningful engagement with lived experience, yet this has been lacking in existing evidence bases (Sirdifield et al., 2024). By systematically capturing the voices of men on probation, this study addresses a critical gap and provides the first detailed account of their physical health needs, the structural and service-level barriers they face, and their directly articulated recommendations for improvement and reform. Aligned with the Inclusion Health framework (Luchenski et al., 2018), which advocates for holistic, person-centred approaches to reducing health inequalities among marginalised groups, the study advances understanding of health inequalities and identifies practical, community-informed solutions to improve healthcare access from the perspectives of MOPs. Its significance lies in generating high-value, practice-ready evidence capable of informing more inclusive, responsive, and equitable health policies and services that can also support desistance. By centring lived experience, the study provides insights with clear potential to influence future research, commissioning, and practice across health, probation, and public health systems.
Literature review: Physical health needs and challenges of men in the criminal justice system in England and Wales
It is well established that men in the CJS experience disproportionately poor health outcomes across multiple domains (Aldridge et al., 2018; Plugge et al., 2014; Rabaiotti, 2024; Skinner and Farrington, 2023; Spaulding et al., 2011). Aldridge et al.’s (2018) study highlighted that CJS-involved populations, including prisoners and probationers, face higher morbidity and mortality rates due to a combination of pre-existing disadvantage, poor access to healthcare, and elevated exposure to health risks such as violence, substance misuse, and communicable diseases. Specifically, men in the CJS are more likely to suffer from cardiovascular disease, respiratory illness, diabetes, musculoskeletal disorders, and infectious diseases such as hepatitis and HIV (Plugge et al., 2014; Spaulding et al., 2011).
These physical health challenges do not occur in isolation but are closely intertwined with mental health disorders, including depression, anxiety, and post-traumatic stress disorder (PTSD), as well as substance use problems (Crowley et al., 2019; Skinner and Farrington, 2023). This clustering of multiple health problems creates what has been called a “syndemic” situation, where co-occurring conditions interact to worsen overall health outcomes (Link et al., 2019). Furthermore, physical health challenges contribute not only to reduced quality of life but also to increased risks of reoffending, complicating efforts at desistance (Jackson and Vaughn, 2018; Link et al., 2019; Sirdifield et al., 2024).
The dominance of prison-focused research
While these health inequalities have been increasingly recognised in public health research, most studies have focused almost exclusively on prison populations (Herbert et al., 2012; Massoglia and Pridemore, 2015; Royal College of Physicians, 2018). Research on incarcerated men (IM) highlights poor access to health services, inadequate screening and preventive care, limited opportunities for exercise, and substandard diets (Health and Social Care Committee, 2018; Lester et al., 2003). Upon release, many men carry these unresolved health problems into the community, where they often struggle to access appropriate care, leading to further deterioration and avoidable deaths (Binswanger et al., 2011; Dirkzwager et al., 2021).
Yet, the population under probation supervision is much larger than the prison population. As of September 2025, more than 246,500 individuals were on probation in England and Wales – almost three times the size of the prison population (HMPPS/MoJ, 2026). Despite this, the health needs of MOP have received little systematic attention. The research that has focused on probation populations in Wales found that people on probation exhibit poorer self-reported health, higher rates of unhealthy behaviours, and greater use of reactive (rather than preventive) health services (e.g. the use of emergency services) compared to the general population (Williams et al., 2024). However, there remains a stark gap in knowledge and targeted health service provision for this group (Rabaiotti, 2024).
Barriers to healthcare access for men on probation
Numerous barriers hinder MOP from accessing healthcare. At the individual level, stigma, fear, and mistrust act as powerful deterrents, particularly among those who have experienced discrimination or judgement from healthcare professionals (Edgar and Tsintsadze, 2017; Martin et al., 2020). For ethnically diverse probationers, racism within both the healthcare and justice systems compounds these barriers, reducing trust and engagement (Lammy, 2017; Marmot et al., 2024). Structural barriers are equally significant. Many MOP live in poverty, lack stable housing, or face food insecurity, which undermines their ability to prioritise health or maintain engagement with healthcare providers (Fitzpatrick and Willis, 2021; Marmot et al., 2010). Brooker et al. (2009) and Sirdifield et al. (2019a) note that some MOPs are often not registered with a GP, limiting access to primary care services. Even when registered, rigid appointment systems, transportation difficulties, and the competing demands of probation supervision can make attending healthcare appointments difficult (Jackson and Hoole, 2008; Lang et al., 2014). As a result, MOP often turn to crisis services, such as emergency departments, instead of engaging in routine or preventive care (Williams et al., 2024).
Unhealthy lifestyles and social determinants of health
Compounding these challenges are the unhealthy lifestyles often associated with justice-involved men, including higher rates of smoking, substance use, poor diet, and limited physical activity (Brooker et al., 2009; Williams et al., 2024). For example, in Williams et al. (2024) study, 26% of MOP report eating fruit and vegetables less than once a week, and 25% exercise less than once a week. These behaviours are not simply a matter of individual choice but are shaped by the social determinants of health, including poverty, unstable housing, unemployment, and social isolation (Link et al., 2019; Marmot et al., 2010; Morgan et al., 2025a). General strain theory offers a useful framework for understanding how health-related strain interacts with socioeconomic adversity to increase the likelihood of maladaptive behaviours, including substance misuse and criminal activity (Stogner and Gibson, 2010). Poor physical health can thus be both a consequence and a driver of offending behaviour, highlighting the importance of addressing health needs as part of broader rehabilitation efforts (Jackson and Vaughn, 2018; Sirdifield et al., 2024).
Inclusion health and its promise
Inclusion health provides a framework for addressing the complex, intersecting needs of marginalised populations, including people in contact with the CJS (Luchenski et al., 2018; NHS England, 2023). At its core, inclusion health challenges traditional, siloed healthcare delivery models, advocating instead for holistic, person-centred, trauma-informed, and multi-agency interventions that simultaneously address clinical, psychological, and social needs (Luchenski et al., 2018). Key components include improving collaboration between health and justice agencies, ensuring continuity of care during transitions between prison and community, offering outreach and engagement services, and advocating for structural changes to reduce health inequalities (Rabaiotti, 2024). Research shows that inclusion health approaches can reduce health inequalities, improve service engagement, and achieve better health outcomes by responding to the realities of marginalised populations’ lives, including the barriers they face accessing mainstream healthcare (Aldridge et al., 2018; Luchenski et al., 2018).
Indeed, several small-scale initiatives illustrate the potential of inclusion health approaches. For example, health trainers (people with lived experience) have been deployed to support probationers with health behaviour change, including smoking cessation, improved diet, and increased physical activity (Bailey and Kerlin, 2015; Dooris et al., 2013). Similarly, health navigators (usually peer support or advocates) help probationers access primary care and other health services, simplifying care pathways and improving continuity (O’Connell et al., 2020; Whitty, 2025). Healthy living hubs co-located within probation offices have also been piloted, improving access to health services and offering integrated, multi-agency support (Brooker, 2024; Jackson and Hoole, 2008). However, schemes can be less effective in probation settings than prison or mental health settings due to lower attendance rates and a lack of organisational support (Bailey and Kerlin, 2015). Moreover, these initiatives remain localised, underfunded, and inconsistently commissioned across England and Wales (Sirdifield et al., 2019b).
Furthermore, there has been limited discussion about how inclusion health principles can be applied specifically to the probation context or how they align with or inform desistance perspectives to further contributions to interdisciplinary theories (McNeill, 2012). While the inclusion health field has expanded in relation to homelessness, prison healthcare, and substance misuse services, there remains little dedicated work on the challenges and opportunities of using inclusion health frameworks to meet the needs of MOP (Brooker, 2024; Rabaiotti, 2024). This is a significant gap, as MOPs represent a group with often intense, intersecting vulnerabilities, including poor physical and mental health, histories of trauma and abuse, disrupted social networks, and high levels of poverty that require joined-up, inclusion-oriented responses (Weaver, 2022; Williams et al., 2024).
The importance of centring men’s voices
Despite the promising potential of inclusion health, research remains limited, particularly regarding the perspectives of MOPs themselves. Most studies have focused on epidemiological data, professional perspectives, or prison-based interventions, leaving a critical gap in understanding the lived experiences of MOPs (Brooker et al., 2023; Rabaiotti, 2024; Sirdifield et al., 2024). Without centring the voices of those most affected, service development risks being top-down and disconnected from the real-world challenges faced by probationers. As such, our study seeks to address this gap by exploring the physical health needs of MOP in South Wales, identifying barriers to healthcare access, and gathering the men’s own ideas for improving services. By involving MOP directly in the design and delivery of health initiatives, services can become more attuned to their needs, more accessible, and ultimately higher quality (Sirdifield et al., 2024).
Methodology
This exploratory study was conducted between March 2024 and September 2024 in a Probation Delivery Unit (PDU) in South Wales, UK, and focused on the physical health needs and healthcare access challenges of MOP. A mixed-methods design was used, combining structured surveys with semi-structured interviews, to gather both quantitative and qualitative data. This approach provided both breadth and depth, helping us understand the physical health needs of the sample and gain richer insights into individuals’ experiences and ideas of how healthcare provisions can be improved.
Inclusion and exclusion criteria
The study focused specifically on adult men aged 18 and over who were currently under probation supervision. This inclusion criterion was chosen because the research aimed to explore the needs and experiences of MOPs, who represent the majority of the probation caseload and who have been underexplored in health research compared to male prisoners (Brooker et al., 2023; Williams et al., 2024). Women were excluded from the study because research indicates that women in the CJS often present with distinct and complex needs compared to men, including higher rates of trauma, domestic violence, caregiving responsibilities, and mental health challenges (Corston, 2007; HMIP, 2024). There is growing recognition that male-centred models of healthcare or service delivery are inadequate for meeting the specific needs of women (HMIP, 2024). To avoid conflating or overlooking gender-specific issues, we focused this study exclusively on men and recommend that future research explore women’s experiences to inform gender-responsive healthcare.
Sample and recruitment
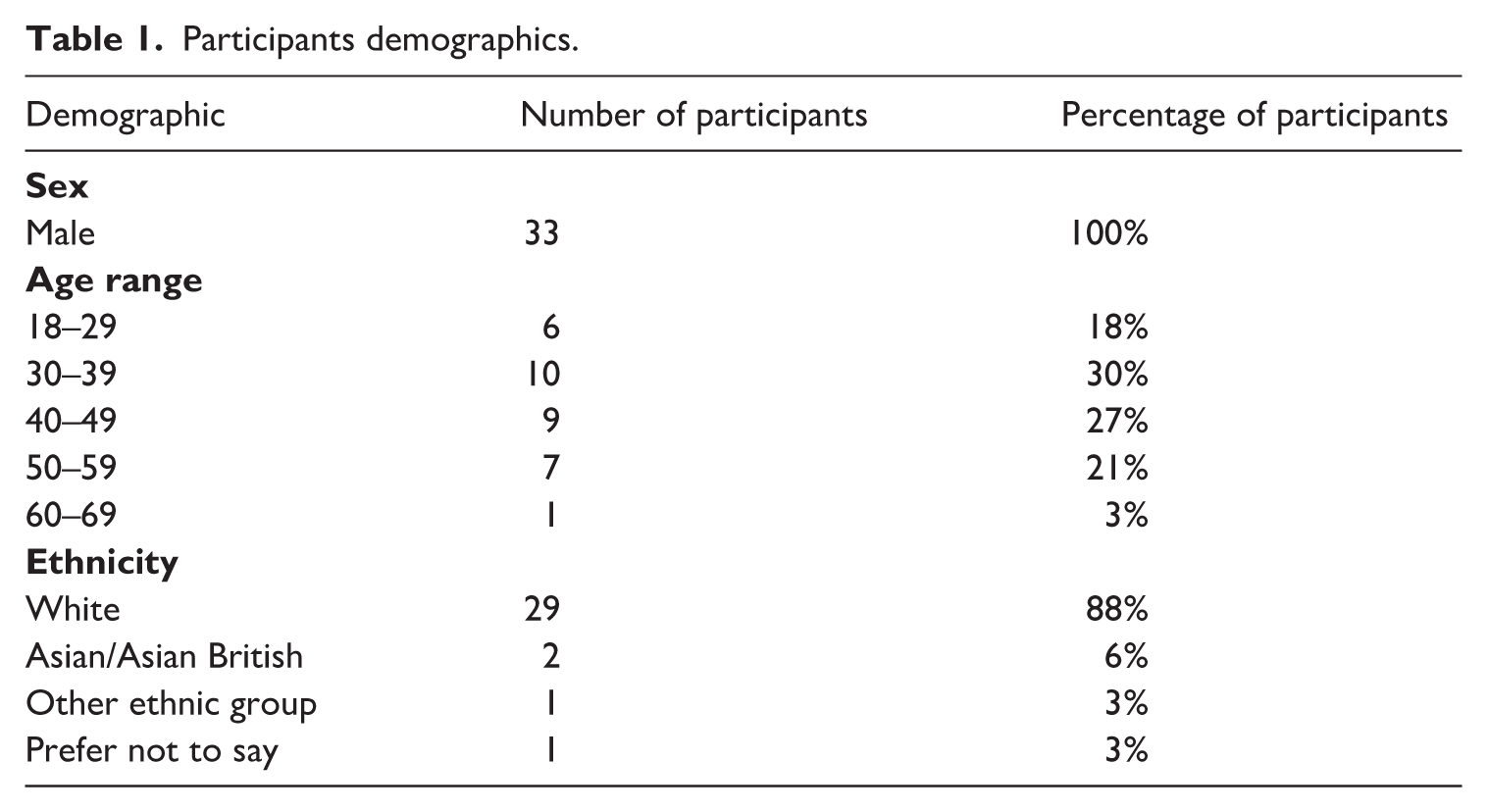
Participants were recruited using a convenience sampling approach, which was considered the most practical and appropriate method for this exploratory study, enabling the research team to base themselves within the PDU and access individuals currently engaged with probation services (Emmel, 2013). Recruitment took place in multiple ways. Flyers advertising the study were distributed within the PDU, and researchers were also present in the open-plan reception area, where individuals attending for probation appointments could approach the team or be informally spoken to about the study. Potential participants were typically approached on arrival or while waiting for their appointment and asked whether they would be interested in taking part. Where individuals expressed interest, arrangements were made to speak either before or after their appointment or at another time convenient to them. Initial conversations took place in the reception area, with interviews conducted in a private interview room to ensure confidentiality. Throughout recruitment, the research team was mindful of the power imbalances between researchers/participants and particularly the inherent power imbalances in probation settings (Morgan et al., 2025b; Smith et al., 2009). To minimise this, individuals were offered drinks and snacks on arrival, which were not contingent on participation, and it was made explicit that involvement was entirely voluntary and would have no impact on their supervision. A total of 33 men participated in the study. While this approach facilitated access to a typically hard-to-reach population, it is important to acknowledge that convenience sampling limits the generalisability of the findings, as the sample may not be representative of all men on probation.
Over half of the participants (55%, n = 18) were being supervised post-release from prison (on licence), while 30% (n = 10) were subject to a community order, and 15% (n = 5) preferred not to disclose their supervision type. Three-quarters (76%, n = 25) had been in prison within the past 12 months, while 21% (n = 7) had not. 45% (n = 15) of the men had been in prison three or more times, 27% (n = 9) had been in prison twice, 15% (n = 5) had been to prison once, and 12% (n = 4) had never been in prison. In comparison to the local probation population (see Williams et al., 2024), our sample was proportionally similar in terms of ethnicity and age (though with slightly more older participants) but included a greater proportion of men under post-release supervision. Table 1 provides an overview of the demographics of our participants.
Participants demographics.
Data collection
We developed a structured survey combining closed and open-ended questions to collect data on participants’ self-reported physical health, healthcare access, barriers, and service use. Quantitative questions used Likert-type scales (e.g. ranging from “strongly agree” to “strongly disagree”) and yes/no formats to assess participants’ perceptions, healthcare experiences, and health conditions. For example, participants were asked whether they were registered with a GP, whether they had seen a GP in the past 12 months, whether they had experienced challenges booking or attending appointments, and if they felt their health needs were being met. Open-ended questions invited participants to describe the barriers they faced in more detail and to share their ideas about how services could be improved. These qualitative responses provided rich contextual insights that complemented the quantitative data, capturing nuances in experience that might otherwise have been missed.
The survey was designed to be completed by participants on an iPad or on paper. Several of our participants needed assistance in completing the survey due to limited (digital) literacy levels. Literacy levels tend to be lower among people in the CLS than among the general population. As such, we had to read the questions aloud and enter responses for some participants. For some participants, the survey also doubled up as an interview, as many participants wanted to explain or justify their responses, providing significant information about their health and ideas to improve healthcare provisions.
Therefore, in addition to surveys, we conducted semi-structured interviews with 18 participants to explore their experiences in greater depth. The interviews focused on key themes identified in the survey responses, such as challenges accessing healthcare, continuity of care following release from prison, stigma or discrimination, and ideas for service improvements. Interviews were conducted in private rooms at the probation centre, providing a confidential and comfortable environment for participants to speak openly. Each interview lasted between 30 and 60 minutes and was audio-recorded with participants’ consent. An interview guide was designed to ensure that core topics were covered while allowing flexibility for participants to raise issues they felt were important.
Data analysis
Quantitative survey data were analysed using descriptive statistics, including frequencies and percentages, to summarise participants’ demographics, health conditions, healthcare access patterns, and reported barriers. Given the modest sample size, we did not conduct inferential statistical tests but instead focused on identifying broad trends and patterns relevant to the study’s aims (Bryman, 2016).
Qualitative data, including open-ended survey responses and interview transcripts, were analysed thematically, following Braun and Clarke’s (2012) six-step process. This involved familiarisation with the data, generating initial codes, searching for themes, reviewing themes, defining and naming themes, and producing a final thematic analysis report. The analysis combined deductive and inductive thematic approaches. Initial coding focused on identifying themes aligned with the research questions (e.g. perceived barriers, service improvement). A second, more inductive phase looked for additional patterns or outliers – unexpected findings or distinctive insights that offered new contributions to the literature on health access and inequality among probation populations (see Braun and Clarke, 2012). Both authors were actively involved in the analytic process. One author is a former probation officer whose doctoral research focuses on probation values, while the other has over a decade of experience researching desistance in the criminal justice system and the implementation of evidence-based practices. These complementary perspectives informed the analysis, supporting both applied insight and critical interpretation of the data.
Ethics
Ethical approval for the study was obtained from Swansea University’s Faculty of Humanities and Social Sciences Ethics and Research Committee and HMPPS National Research Committee. All participants were provided with detailed information sheets explaining the study’s purpose, what participation involved, and their rights, including the right to withdraw at any time without consequence. Written informed consent was obtained from all participants before data collection. All data were anonymised, and participants were assigned pseudonyms. No identifiable information was included in transcripts, analysis, or reporting.
Results
Two key themes were created from our analysis of the data: healthcare barriers and healthcare opportunities, which were made up of several sub-themes. The findings revealed numerous barriers to healthcare access and ways to improve healthcare provisions from the MOPs’ lived experience. The quotes from the men are presented verbatim, and pseudonyms have been used to ensure confidentiality and anonymity. Within the sample, 54% (n = 15) reported having “musculoskeletal and pain issues,” 36% (n = 10) having substance-misuse-related conditions, 29% (n = 8) having a heart/cardiopulmonary condition, and 21% (n = 6) having dental issues.
Theme 1: Healthcare barriers
Healthcare barriers emerged as a key theme, with men on probation describing multiple challenges to accessing care, including a lack of continuity between prison and community services, difficulties building trust and rapport with healthcare professionals, inflexible GP appointment systems, and the compounded effects of digital exclusion on healthcare access. These findings align with wider research highlighting how structural, relational, and technological barriers disproportionately impact marginalised justice-involved populations, exacerbating existing health inequalities (Binswanger et al., 2011; Hider et al., 2023; Luchenski et al., 2018; Weaver, 2022; Williams et al., 2022).
Lack of continuity of care between prison and community
Participants raised a lack of continuity of care as a key issue, with participants describing fragmented or poorly coordinated healthcare during the transition from prison to the community. One participant reflected, Prisons take you off meds that you find helpful and beneficial and when you get out your own doctor is reluctant to put you back on those meds.
Disruptions to care during the transition out of prison are well-documented in the literature, with studies showing that people leaving custody often face gaps in medication, delays in accessing primary care, and poor inter-agency communication (Binswanger et al., 2011; Flanagan, 2004). Improving continuity of care requires better data sharing, joint-up working between prison and community health services, and proactive re-entry planning (Carswell et al., 2017; Rabaiotti, 2024).
Building trust and rapport with health professionals
Many participants described negative experiences with healthcare professionals, particularly feelings of not being listened to or treated with respect. As Alun noted, If I tell them I’ve got a problem, they’ve already assessed you and say “it must be that.” . . . they think they can read you off charts. It just depends what side of the bed they got out of in the morning. They’re only human. They gotta be professional about it, but sometimes they’re not really listening. It’s hard to get your point across.
Rhys described a crisis moment: So when I phoned the GP up and I was suicidal and they turned around and said, “well, there’s not much we can do. If you want help call 999 if you feel suicidal.” And that was pretty much it. So being in that position, you feel sort of very much on your own and well, you know, can I turn to them? And if I’ve got an issue then probably not, you know.
Positive experiences were also highlighted, where respect and choice were emphasised: [My GP] is understanding and he’s good to talk to. And they give me a choice.
Improving the quality of healthcare interactions, particularly through trauma-informed, non-judgmental approaches, is crucial for increasing engagement and trust among justice-involved populations (Williams et al., 2022).
Inflexible GP appointments
Participants highlighted significant barriers to accessing GP appointments, largely due to inflexible, digitally driven booking systems. Men expressed frustration at being required to call early in the morning, endure long waits, or navigate online systems they found inaccessible. Alun described, It’s hit and miss . . . If you don’t phone early then they won’t pick up or you’ll be on it for 20 minutes before the phone gets answered. If you call late, it’s just engaged all the time. I would normally just walk in and make an appointment, but the last five to ten years, it’s all gone to telephone now.
Fred added, Before, right, you used to walk in any time before 11am, but they stopped now because COVID came about. Now you gotta phone them up by 8am in the morning and then you say “can I have a call back off a doctor?”, and they might not ring you back until the next day.
These rigid systems disadvantage MOP, who may struggle with chaotic lifestyles, probation appointments, or limited phone/Internet access (Brooker et al., 2009; Morgan et al., 2025c). Extending appointment hours or offering more flexible drop-in options could help address these barriers and reduce unnecessary use of emergency services.
Digital exclusion and healthcare access
Linked to the above, challenges in accessing and using digital technology acted as a barrier for the men. The shift towards digital healthcare systems, accelerated by the COVID-19 pandemic, emerged as a significant barrier for many men, particularly those released from long prison sentences. Kyffin shared, Everything has changed. One. It has got more digital. Two. They’re not taking appointments over the phone anymore . . . I’m useless with tech.
Alun stated, I knew it [his transition from prison into the community] was gonna be hard. I’m not one with computers and IT and all that. I hate having a swipe phone. I don’t even own a phone now. I’ve gotta get one because everyone needs me to get a phone, but I can’t stand phones.
Digital exclusion is often driven by poverty, low literacy, and lack of digital skills (Hider et al., 2023; Holmes and Burgess, 2022; Morgan et al., 2025c). Addressing digital barriers through training, device access, or maintaining non-digital service routes is critical to ensuring equitable healthcare access (Morgan et al., 2025c).
Theme 2: Healthcare opportunities
In response to the healthcare challenges the men faced, they offered experience-based suggestions for how healthcare provision could be improved to better meet their needs. These included the development of community-based drop-in centres that address multiple needs beyond health, such as housing, benefits, and food; the introduction of specialist support workers or health advocates to help navigate complex systems; peer support and outreach, recognising the unique value of lived experience in building trust and engagement. These proposals not only align with inclusion health principles, which advocate for holistic, person-centred, and community-informed models of care (Luchenski et al., 2018); but principles of desistance, which include opportunities to develop social capital through building relationships (McNeill et al., 2012).
Drop-in centres addressing multiple needs
A key sub-theme was the men’s call for community drop-in centres where the men could access not just health services, but broader social support, including housing advice, benefits help, and opportunities for social interaction. This reflects a recognition among participants that their physical health is inextricably linked to social determinants like housing, employment, and social isolation (Luchenski et al., 2018; Marmot et al., 2010). Ceri described the benefit of such services. He was particularly concerned with the state in which many left prison with little emotional, physical, psychological and financial support: People need to know how to apply for certain applications cause in jail, I don’t know how many people couldn’t read or write or couldn’t even count or do simple maths. So any help with applications, getting appointments and all that. To explain to them verbally, so that they can understand, because when you put it in writing or in numbers, you know, they’re going to struggle with that. So anything where . . . you could usher them along. Yeah, that would be a God send.
Alun echoed the need for accessible, multi-service hubs: I can’t think of any place in [location] [such as a drop-in centre] like this. You know, I was homeless years ago. I’ve been in [location] all my life. There was always places to eat and all that, but help trying to secure accommodation, a dentist, to get an NHS appointment or just to follow up on checks and things like that . . . it’s not there.
Beyond practical services, and in line with desistance research on social capital (Farrall, 2004; McNeill et al., 2012), Lloyd emphasised the importance of social connection and well-being: Well, you could just pop in [to the drop-in centre] if you wanted a game of pool or table tennis, you could just go there to chill out for an hour. So if you were stressed out and needed help, just go there for a chat.
These reflections also align with the inclusion health framework, which promotes integrated, holistic services addressing health and social needs together, particularly for marginalised groups like MOP (Luchenski et al., 2018). Opinions were divided on whether health services should be co-located within probation offices. Some men valued the convenience, seeing it as just another access point. As Rhys stated, Yeah, I mean at the end of the day it’s something, it’s an avenue, it’s something available, isn’t it, whether that’s here, whether that’s there, it doesn’t really matter, it just somewhere where it is available.
Others, however, were wary of combining probation with healthcare. Alun noted, In this setting [the probation office], people just want to pop in here, get in here, give your name and get out.
These mixed views echo research suggesting that while co-location can improve service integration (Jackson and Hoole, 2008), it must be carefully implemented to avoid reinforcing stigma or undermining trust (Brooker, 2024). The reluctance among some MOPs to engage with healthcare can be understood within the broader context of probation’s shift towards supervision, risk management, and control, where compliance-focused practices and managerial pressures may undermine trust and deprioritise health needs (Tidmarsh, 2024).
Specialist support workers and health advocates
Several participants emphasised the value of having health advocates or support workers who could help navigate complex healthcare systems, particularly for those with mental health challenges or histories of addiction. Nic explained, They need someone on the outside or a charity who is there 24/7. Because a lot of them, and I speak on behalf of addicts, they need help. In my early days when I suffered with depression, it’s worse in the nighttime. The only people available is the Samaritans which I’ve used.
While Ceri recognised the difficulty of providing one-to-one keyworkers due to cost implications, he saw potential in group-based models within a supportive environment: Even if it’s group based, you know, going into somewhere. I understand, you know, you can’t have a key worker for every individual who comes out of prison but they can organise it in such a respect that there could be group sessions, you know, or mandatory group sessions for people who need the support.
Research emphasises that probationer and worker relationships are central to desistance-based practice (McNeill et al., 2012). Furthermore, health trainer and navigation models, increasingly used in inclusion health and probation settings, have been shown to improve access, build trust, and reduce health inequalities among vulnerable populations (Dooris et al., 2013; O’Connell et al., 2020; Whitty, 2025).
Peer support and outreach
Participants also called for more peer support and outreach, particularly from people who had lived experience of probation, addiction, or prison. Meic explained, I’d say more outreach, you know, if people want to change, like I don’t think people get shown . . . they don’t get to listen to somebody that’s been there and done it. So then, you know, maybe if I was in a group and I brought something up, maybe that person would take what I say as an idea.
He continued, They need someone to reach out to them and, you know, tell them that they are worth something. There’s more to life than what they’re going through. If you said to someone “have a good day, stay off the drugs.” If they get told that, maybe it will prevent them from doing something in the future, you know.
Meic’s reflections echo desistance principles of hope and support for change (McNeill et al., 2012). While, peer-led interventions are increasingly recognised as effective in promoting engagement, building self-efficacy, and providing credible role models in inclusion health work (Walton et al., 2024; Whitty, 2025).
Discussion
This study explored how health inequalities and access to primary healthcare can be improved for MOP. Using a mixed methodology, we centred the men’s perspectives, capturing their insights into the barriers they face and their recommendations for improving services. The findings provide rich, qualitative evidence that can inform the design of more inclusive and responsive healthcare services for this often-overlooked population. Our findings highlight the need for integrated health and probation services that improve treatment pathways and ensure continuity of care (Brooker et al., 2023). Policymakers should explore models such as GP-probation co-location, mobile health services, and flexible appointment systems to accommodate the complex lives of probationers. Health services must also address broader social determinants of health, including housing stability, employment opportunities, and food security, recognising that these are inextricably linked to health outcomes (Link et al., 2019; Marmot et al., 2010) (as well as justice outcomes). To close the health disparity gap, future (inter)national strategies must ensure that inclusion health principles are not limited to the prison setting but are fully extended to probation populations. This will require dedicated policy attention, sustained funding, cross-agency leadership, and meaningful involvement of people on probation themselves in designing, implementing, and evaluating health services (Jeffery, 2025). Without such efforts, the risk remains that probation populations will continue to fall through the cracks of fragmented health and justice systems.
Our study has demonstrated the value of involving MOP directly in identifying barriers and co-creating solutions. For example, the men’s reflections on the need for multipurpose drop-in centres, flexible appointment systems, and peer-led outreach were grounded in their real-world experiences of exclusion, stigma, and service fragmentation. Their insights challenge top-down assumptions about what “ought” to work, offering instead practical, low-barrier interventions designed around their actual needs. Moreover, their suggestions are aligned with evidence-based principles which support the desistance process (McNeill et al., 2012). Centring lived experience is increasingly recognised as an essential part of inclusion, health and desistance-focused work (Morgan et al., 2025b; Sirdifield et al., 2024; Weaver, 2022).
While we did not use a co-production approach due to time limitations on our research, future research should utilise this approach to centre the voices of MOPs. Co-production approaches, which position “service users” as equal partners in service design and delivery, can help ensure that interventions are accessible, acceptable, and effective (Morgan et al., 2025b). They can also foster a sense of agency, ownership, and trust among participants – factors known to support engagement and positive health outcomes (Weaver, 2022). By foregrounding MOP’s voices, this study contributes to a growing body of evidence advocating for user-led innovation in health and justice settings. Future efforts to improve healthcare for probation populations should continue to prioritise co-production and expert-by-experience involvement, recognising that the people closest to the problem are often those best placed to help design the solution, coinciding with inclusion health principles.
The challenges of addressing MOP’s needs: Policy and practice recommendations
While the ideas from men on probation (MOP) in our study (multipurpose drop-in centres, flexible appointments, peer support, improved continuity of care, digital inclusion efforts, and trauma-informed healthcare) are both thoughtful and grounded in lived experience, realising these changes presents significant challenges. These challenges arise not only from service design and delivery complexities but also from wider structural issues in society, structural inequality within the NHS, differing political priorities, and the broader difficulty of meaningfully engaging marginalised groups, which may apply to other jurisdictions globally.
One of the most significant barriers to implementing the changes proposed by the men relates to the ongoing pressures on the NHS. The NHS has faced rising demand alongside real-term funding constraints for over a decade, exacerbated by the impacts of COVID-19, workforce shortages, and escalating waiting times (Arnold and Jefferies, 2025; Charlesworth and Johnson, 2018; Khan, 2024). GPs, in particular, report unsustainable workloads, with appointment slots increasingly rationed, rising patient lists, and declining continuity of care (Khan, 2024). The suggestion of flexible appointments and out-of-hours services for MOP, while valuable, may be difficult to deliver in practice without additional investment or structural reform. Current GP contracts and workforce models often do not support the kinds of tailored, proactive outreach or drop-in systems that the men envision. Moreover, mental health services, which were frequently mentioned in the study as important, are particularly under-resourced, with chronic underfunding relative to need and growing unmet demand (Mental Health Foundation, 2022). Developing multipurpose drop-in centres or co-locating services within probation offices also raises significant logistical and resource questions, particularly within a contemporary probation context increasingly shaped by risk management and control-oriented practices, which may constrain the delivery of holistic, health-focused support. While inclusion health hubs have been piloted in some contexts (Luchenski et al., 2018), scaling such models would require cross-sector funding agreements, inter-agency collaboration, and political backing. Without dedicated funding streams for health initiatives, there is a risk that new initiatives will struggle to gain traction or become vulnerable to short-term commissioning cycles, a key consideration for inclusion health initiatives globally.
Even where effective models exist, implementing them at scale depends on political will. There is limited political focus on the health of justice-involved populations in England and particularly in Wales, despite long-standing evidence of health inequalities and avoidable deaths (Aldridge et al., 2018; Royal College of Physicians, 2018). Public and political discourses around probationers often prioritise criminality, risk management, and public safety, rather than health, rehabilitation, or inclusion (Sparks, 2013). For other jurisdictions, too, the political context matters because policymakers’ attention and funding decisions can be shaped by public and media narratives. Advocating for better health provision for MOP requires reframing justice-involved populations not simply as “offenders” but as citizens with rights, needs, and potential (Edgar and Tsintsadze, 2017; Weaver, 2022). Without such reframing, there is a risk that proposals for more inclusive health services and more desistance-focused services will be deprioritised or dismissed as politically unpalatable, particularly in a policy climate marked by austerity and criminal justice “toughness” (see Loader, 2010). Indeed, the latest NHS Long Term plan does not refer to health and justice despite CJS populations facing the worst health outcomes (Jeffery, 2025), and the latest Ministry of Justice probation policy appears focused on centralised technology, rather than locally commissioned collaborative delivery (Rabaiotti, 2025).
Furthermore, realising the suggestions from the men in our study also involves confronting deeper structural and cultural barriers – greater attention and accountability need to be placed on the structural inequality that draws people into the CJS. The inclusion health framework (Luchenski et al., 2018) emphasises that marginalisation is not simply the result of individual vulnerability but of structural exclusion embedded within social systems. Addressing health inequalities for MOP requires not just tweaking service models but tackling broader issues of poverty, discrimination, and criminalisation that shape health risks, access to healthcare, and impede desistance (Marmot et al., 2010). For example, improving continuity of care between prison and community requires more than just technical fixes like shared IT systems; it also requires overcoming siloed working cultures, professional hierarchies, and resource constraints (Binswanger et al., 2011; Carswell et al., 2017). Addressing digital exclusion is not just about providing training but about tackling the economic precarity and low literacy that underpin exclusion (Hider et al., 2023; Morgan et al., 2025c). Similarly, changing the way healthcare professionals engage with MOP involves not just individual training but wider cultural change within healthcare systems to recognise, value, and prioritise the needs of marginalised populations (Williams et al., 2022). Importantly, responding to the health needs of men cannot be done in a silo; it must consider the holistic needs of MOP and tackle wider and related issues such as poverty, mental health, food, housing, employment and financial insecurity, addictions, and social/digital isolation (Morgan et al., 2025a).
Limitations of the study
While this study offers important insights, several limitations should be acknowledged. First, the study included only male participants and did not explore the health needs of women on probation. This is a significant limitation, as there is a growing body of research showing that women in the CJS often present with distinct and complex needs compared to men (Corston, 2007; HMIP, 2024). For example, women in the CJS are more likely to have experienced gender-based violence, sexual abuse, and trauma, and they frequently have primary caregiving responsibilities that shape their health needs and service engagement (Corston, 2007). There is increasing recognition that applying male-centred models to women is inadequate and potentially harmful and that tailored, gender-responsive approaches are needed (Corston, 2007; HMIP, 2024). Future research should explicitly examine the specific health needs of women on probation and support the development of services that reflect their experiences and challenges (Williams, 2025).
Second, the study was limited to a single probation area, which may affect the generalisability of the findings. While the sample size provided valuable qualitative insights, it was relatively small and may not capture the full diversity of MOPs’ experiences, including those from minority ethnic or LGBTQ+ backgrounds, or those with neurodiverse conditions. Future research should explore how intersectional identities shape healthcare access and needs within probation populations.
Concluding thoughts
This study provides important insights into the physical health needs and healthcare access challenges of men on probation (MOP), a group often overlooked in health and justice research. The study identified high levels of chronic health conditions, frequent barriers to accessing primary care, and critical gaps in continuity of care following release from prison. Importantly, the study centred the voices of MOP, revealing their practical, experience-based suggestions for improving healthcare provision. While national strategies from HMPPS, MoJ, and the NHS increasingly acknowledge the importance of inclusion health, MOP’s voices remain largely absent from policy design and service development. Moving forward, it is essential that healthcare interventions and probation services meaningfully incorporate lived experience perspectives, ensuring that MOPs are co-producers of the solutions intended to support them. Only by embedding inclusion health principles and resourcing cross-sector collaboration can we begin to reduce the profound health inequalities facing this marginalised group and support desistance.
Footnotes
Acknowledgements
The authors would like to thank the following: the family and friends of the late Dr Bob Russell-Jones (who was honoured with an OBE for his medical work with men in HMP Swansea), whose legacy fund via the St David’s Medical Foundation made this project possible; Anneliese Hall for supporting data collection; and, importantly, the men who contributed their time and experiences.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received £16,000 in funding from the St. David’s Medical Foundation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.