
Abstract
Context
Non-technical skills are the cognitive and affective behaviours that underpin clinical practice in surgery. The purpose of this study was to explore the factors that affect how scrub practitioners use non-technical skills during surgery and their behavioural responses to those factors.
Methods
Eight scrub practitioners participated in a qualitative semi-structured interview study.
Results
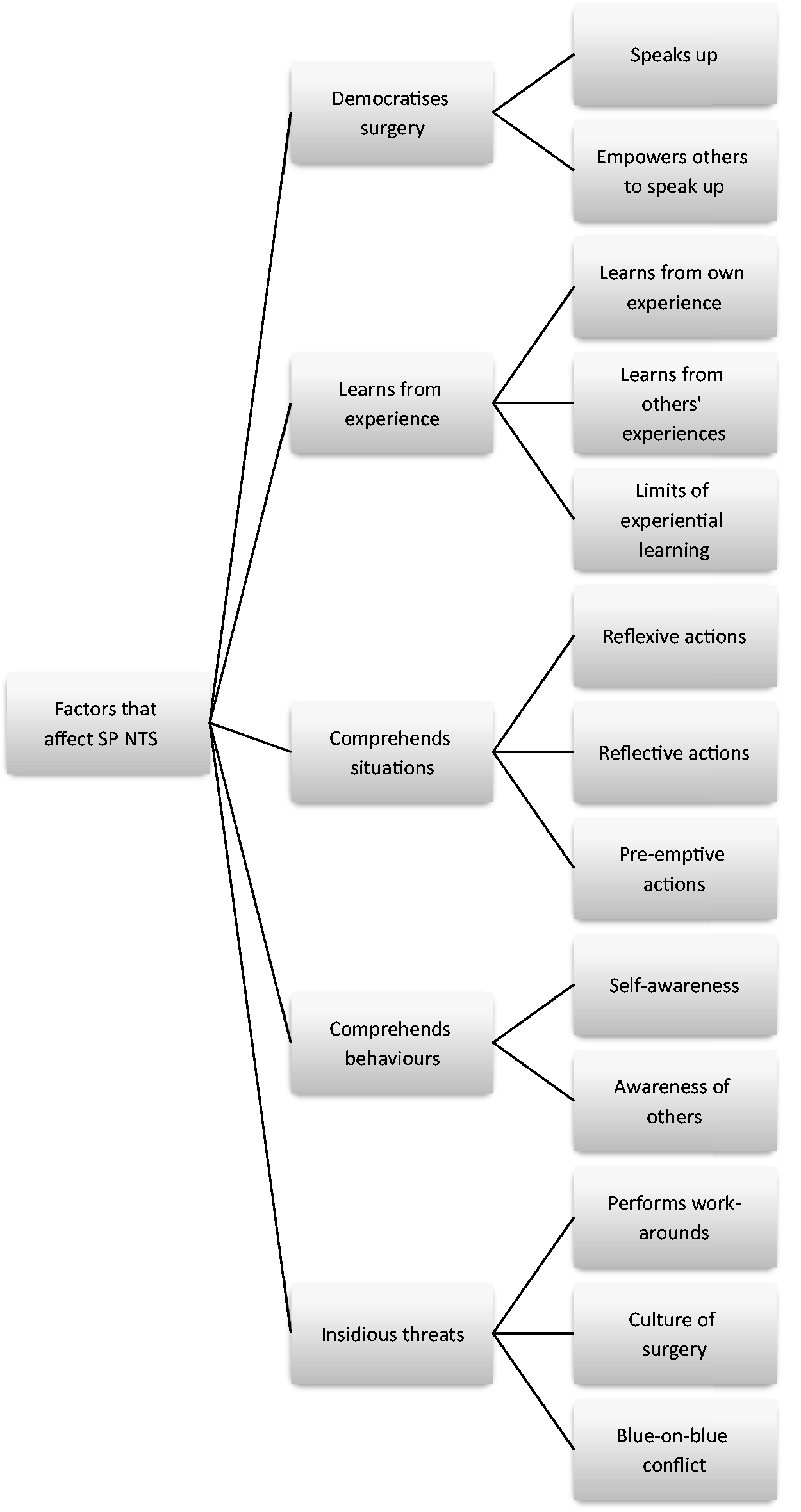
Five major categories were found to affect scrub practitioner non-technical skills. These categories were democratises surgery, learns from experiences, comprehends situations, comprehends behaviours and insidious threats.
Key findings and implications:
A scrub practitioner’s ability to use non-technical skills results from the interdependent relationship of intrinsic and extrinsic motivators that affect their own behaviours, and those of their colleagues, during surgery.
Introduction
Non-technical skills (NTS) is a generic term for affective and cognitive behaviours that include leadership, teamwork, situational awareness and decision making (Flin et al 2008). Each professional grouping participating in surgery uses different NTS behaviours (Rutherford et al 2015). Scrub practitioners (SPs) are generally acknowledged to use the cognitive NTS of situational awareness and the affective skills of teamwork and communication (University of Aberdeen 2010) and to a lesser extent, decision making and leadership skills (Kang et al 2014). An external review that investigated the root causes of unintentionally retained surgical items in one NHS Trust highlighted the contributory role of the SP in the development of serious untoward incidents (Toft 2014). Their root causes were not isolated events, but resulted from a series of complex interdependent latent conditions and errors. These included the formation of cognitive biases by surgeons and SPs that reduced situational awareness, complex interprofessional relationships that detracted from communication processes and established clinical practices that failed to mitigate errors made by fallible practitioners. This study aimed to explore the factors present within the surgical team and theatre environment that affect SP NTS and analyse how SPs respond to those factors.
Methods
Qualitative interviews were conducted to explore the factors that affect the use of NTS by SPs. Methods associated with Grounded Theory were chosen to collect and analyse interview data (Charmaz 2014). The study purposively sampled SPs recruited from an English NHS Foundation Trust. Posters promoting the study were placed in communal areas of the Trust’s Operating Department and SPs were asked to contact the researcher if they wished to participate. Inclusion criterion for the study was any Operating Department Practitioner or Registered Nurse employed as an SP. Eight participants were interviewed (six female, two male). The average time spent employed as an SP was 16 years (range 0.5–35 years).
Semi-structured interviews explored the actions of the participants and their colleagues during one or two inconsequential events that had occurred during surgery. Interviews averaged 29 min (range 9–51 min) in duration. A topic guide was developed using the Scrub Practitioner List of Intraoperative Non-Technical Skills assessment framework (University of Aberdeen 2010). The interview schedule was piloted and amended following feedback. The topic guide was further amended after the fourth interview and questions revised in response to data arising from the emergent themes from preliminary interviews.
The researcher manually transcribed the recordings. Data coding commenced after the first interview to identify emergent themes and facilitate analysis of their association with themes that emerged in subsequent interviews. Analysis was undertaken by using constant comparative methods to identify similarities and differences in the data (Charmaz 2014). Validation of the emergent themes was undertaken with seven of the eight participants to prevent misrepresentation of the participants’ perspectives.
Ethics
The study was approved by the NHS Trust’s Research and Development Department and the School of Health Research Ethics Committee at the University of Central Lancashire. Written informed consent was obtained from all participants. Participants were able to withdraw from the research and have their data deleted for a period of up to three weeks after their interview. Data identifying an individual, location or organisation were removed during interview transcription.
Findings
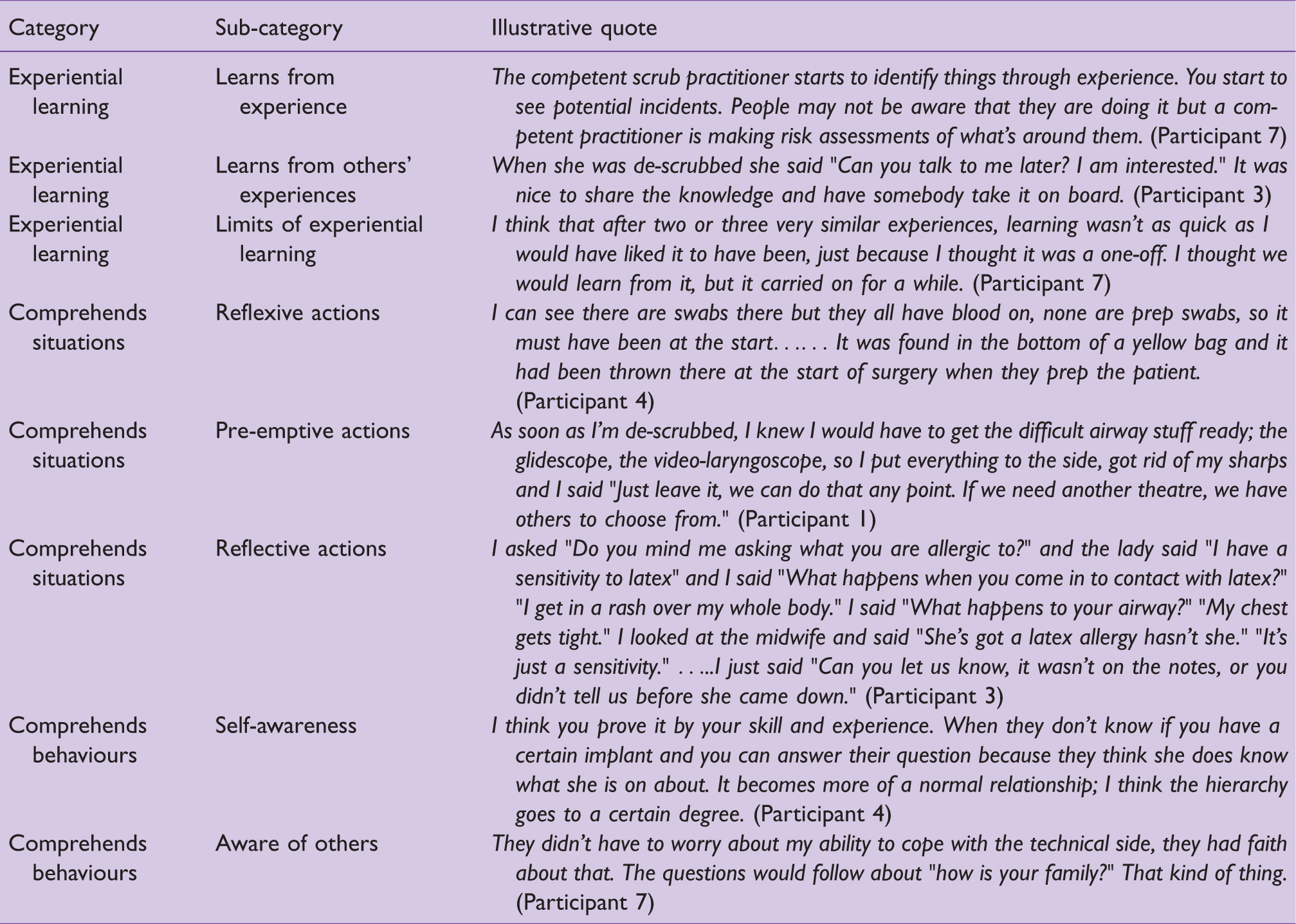
Practitioners described situations during surgery that promoted or had the potential to detract from their NTS behaviours. Five major categories emerged from data analysis; democratises surgery, learns from experiences, comprehends situations, comprehends behaviours and insidious threats (see Figure 1). Each major category comprised of two or three categories. This paper reports the findings of the democratising surgery and insidious threats categories only. Verbatim quotes from the three remaining categories are reported in Table 1.
Major themes and sub-themes emerging from findings
Illustrative quotes from participants
Democratising surgery
A key factor that facilitated the use of NTS was the ability of practitioners to communicate a concern to a colleague. Two categories emerged; speaks up and being empowered to speak up. Speaks up has two distinct sub-categories; unambiguous communication and suggestions that contain a prelude. Both forms of communication originated from participants realising that a chosen course of action was inappropriate. Most participants used unambiguous communication when a matter of urgency required an immediate response from another individual, typically when informing a surgeon that a countable item was missing.
The perception of accountability was found to affect communication strategies. Most participants suggested unambiguous communications were necessary because item accountability was perceived as their responsibility. Communicating a missing item was delivered unambiguously because the situation was perceived as unambiguous. Some participants overcame personal characteristics that might have detracted from obtaining a response. One participant commented that their innate characteristic of quietness minimised distractions. However, the individual demonstrated their ability to modify those characteristics by altering their vocal tone whilst describing a situation when ambiguity was experienced. Participant Interviewer – P I
The response demonstrates that innate characteristics were purposefully over-ridden to obtain an immediate response from the surgeon. The surgeon’s response to unambiguous communication demonstrated that speaking up allowed the practitioner to convey their concern. Consequently, the surgery was interrupted until the missing item was accounted for.
Statements or questions were guised as suggestions when a practitioner recognised that another individual’s intended actions were inappropriate, and that an alternative action was desirable. One participant suggested that development of this soft skill was essential in the operating theatre.
The complexities of interprofessional working can be seen as a threat to patient safety. Participants may have difficulty communicating their comprehension of a situation to their colleagues due to established hierarchal structures. To overcome this, some participants used a prelude as a buffer to prevent the recipient of the message from perceiving that their actions were being challenged. This participant described a suggestion made to a consultant surgeon regarding the use of an alternative dressing whilst supervising a novice SP.
The practitioner recognised the consultant’s status by conceding that the decision is ultimately the consultant’s. However, the strategic use of the prelude ‘Can I just give you some advice?’ resulted in the surgeon demonstrating surprise that an alternative plan had been suggested. By empowering the participant to speak up, the surgeon demonstrated that the advice of others informed his clinical decision making process. However, empowering the participant had greater symbolism. The surgeon’s response demonstrated to the novice SP that speaking up is normative behaviour within perioperative culture. The act of dissemination of culturally normative behaviours may encourage the novice to also speak up to voice their concerns on future occasions.
Most of the participants described scenarios that resulted in multi-tasking whilst scrubbed. Multi-tasking during surgery was facilitated by circulating practitioners. However, the boundary formed by the surgical field also represents a professional boundary, particularly when the circulating practitioner is of a lower banding grade. Some of the participants recognised personal limitations and valued the input of their colleagues to raise safety concerns.
Although participants perceived that the surgeon transferred item accountability to the SP, some participants described sharing that responsibility with the circulating practitioner. This participant demonstrated that by sharing responsibility, the circulator is empowered to speak up. The circulator’s challenge transcends a professional boundary that might be interpreted as questioning the participant’s competence. However, by empowering an individual to speak up, the professional boundary is diminished and collective responsibility is established that may highlight safety concerns that are unrecognised by the SP.
Insidious threats
The major category of insidious threats developed in recognition that the factors that contributed to latent threats in this study were interwoven with the existing fabric of perioperative culture. Some practitioners described clinical scenarios where colleagues violated systems that were developed to improve safety by devising work-arounds that adapted to the circumstances of surgery. The Surgical Time Out and Sign Out is a standard operating procedure briefing process that intends to transform surgical culture by promoting team working (WHO 2009). This study found that some staff demonstrate apathy towards its use by performing work-arounds that resulted in short-cuts.
Compliance by individual team members with the briefing process is dependent on the surgical phase. The Time Out occurs prior to surgery and appears to function as a barrier to commencing surgery. Shared situational awareness develops because the surgical team has to discuss the specifics of the case before surgery is allowed to begin. The Sign Out occurs towards the end of surgery and does not provide a barrier towards completing surgery; the barriers are the tasks that each practitioner is responsible for and greater effort is expended to complete these. The surgical team disbands into their sub-teams and the resulting uncoupling reduces shared situational awareness.
The behaviours of individuals during different surgical phases suggested that some theatre teams are comprised of sub-teams that function independently and only unite for a limited period to achieve a common goal. One participant described a situation when a recovery practitioner was unavailable to recover a patient undergoing surgery. Management of the situation required a collaborative decision. However, the team disbanded before the surgery’s completion.
All of the participants stated that management of similar situations defaulted to the SP. Surgical team membership is transient at the end of procedures because each individual chooses to prioritise their own responsibilities over collaboration. SPs are unable to exercise this choice because they hold membership of the surgical team for the entire duration of the surgical procedure. Consequently, the SP is conflicted between prioritising their responsibilities and managing the wider environment. Individuals are afforded differing degrees of autonomy within their clinical practice and this appears to be dependent on their role during surgery. Superficially, SPs may be perceived as having limited autonomy because they are regarded as being responsive to the needs of surgeons. By failing to collaborate, their colleagues passively delegate additional roles to the SP that conflict with tasks that must be prioritised at a particular stage of surgery.
The scenario above triangulates with the behaviours of only some clinicians during surgery. The findings demonstrated examples when participants were able to cross traditional professional boundaries and clinicians responded to concerns raised. Some participants suggested that the attitude of the recipient of the message, and not their professional status, was the barrier to their use of NTS. Two participants gave examples of episodes where ‘blue-on-blue’ conflict had the potential to emerge between practitioners from the same, or similar, professional background.
In the context of this research, the term ‘blue-on-blue’ refers simultaneously to the traditional colour of the uniform worn by the theatre team, ‘theatre blues’ and to the military term for ‘friendly fire.’ The presence of collegial relationships promotes effective interpersonal and interprofessional behaviours. However, in the presence of blue-on-blue conflict, a practitioner’s ability to offer alternative suggestions is compromised by individuals who are unwilling to compromise their viewpoint. Acting with impunity reduces collaboration and reduces the effectiveness of individuals and the systems they function within to minimise errors.
Discussion
SPs use distinctly different communication behaviours whilst voicing concerns during surgery. The presence of a democratic system during surgery was essential to achieve this condition: speaking up and empowering others to speak up enabled this. The category of insidious threats described a series of conditions that detracted from the ability to speak up and impeded surgical democracy.
Individuals who possess hegemonic control over others are able to exercise that control to influence the behaviour of others (Crotty 1998). The surgeon’s hegemonic status provides that individual with the power to dismiss the SP’s concerns and continue with the progress of the surgical procedure (Gardezi et al 2009). SPs being able, or enabled, to speak up achieves the condition of democracy in surgery by redistributing power from the surgeon to other theatre practitioners and reduces established hierarchies (Finn 2008). This study’s findings suggest that SPs are aware of their ability to influence decisions made by surgeons, and use preludes in their communications to attempt to influence a surgeon’s decision making. This behaviour was reciprocated by surgeons when they became aware of the potential contribution of the individual raising the concern, and empowered that individual to speak up.
The findings suggest that these egalitarian conditions may be frequently absent during surgery. Some participants suggested that some surgeons leave the operating room before the Surgical Sign Out or fail to acknowledge an SP communicating that all countable items are present at the end of surgery. This communication has the potential to alter the established power differentials that exist during surgery. At a fundamental level, the communication that the count is correct is the SP permitting the surgeon to complete surgery; the absence of a countable item should result in the withdrawal of permission to complete the surgery until all equipment has been accounted for. Failure to acknowledge the communication may be a manifestation of passive resistance towards the power that the SP might exercise.
At the extreme range of behaviours, participants described blue-on-blue conflict. The protagonist’s behaviours introduce interpersonal tensions that were intended to actively undermine the recipient’s self-efficacy. The Theory of Planned Behaviour states that an individual will choose to engage with a behaviour based on the ease or difficulty of performing that behaviour on previous occasions (Ajzen 1991). This theory explains the presence of blue-on-blue conflict within the perioperative team. An individual who subjectively perceives they possess hegemonic power over another colleague may repress the behaviours of that colleague by introducing the potential for conflict. Individuals experiencing this condition during surgery may subjugate during the current surgical procedure, and on future occasions, because conforming to these subjective norms is less difficult than challenging the condition imposed up on a practitioner by another practitioner of dominant status.
Limitations of this study
Overall, the findings have limited generalisability and transferability to SPs in other clinical settings. The study was small scale and failed to attain theoretical data saturation. Although the clinical setting is typical of most NHS Foundation Trusts, some complex specialities had been recently re-deployed to specialist centres. SPs employed in more complex clinical specialities may have different perspectives of their experiences of using NTS (Kang et al 2015).
Conclusion
This study found that effective NTS behaviours were promoted by factors that were both intrinsic and extrinsic to the participants. Intrinsic factors manifested as each participant’s personal characteristics. These characteristics resulted in behaviours that allowed the participant to function effectively on an interpersonal and interprofessional level. The participant’s comprehension of the clinical situation facilitated their ability to discriminate between available options and apply the appropriate behaviour to the clinical situation. The extrinsic factors were generated by colleagues who possessed a similar comprehension of the situation and reciprocated the participants’ positive behaviours with similar positive behaviours. NTS behaviours were found to have been moderated by some of the participants’ colleagues being unable to discriminate between effective and ineffective behaviours. This resulted in individuals, irrespective of their hierarchal status, acting with impunity and violating systems that were intended to act as barriers against incidents occurring. SPs must be able to explicitly recognise how those factors promote or detract from their use of NTS, and be empowered by their colleagues to develop strategies that promote their use of effective NTS behaviours.
No competing interests declared