
Abstract
Inadvertent perioperative hypothermia (IPH) is a common problem associated with perioperative patients which can have significant consequences for them during surgery and in the immediate postoperative period. Recognising and managing IPH remains an important aspect of perioperative nursing and is a significant factor in maintaining patient safety, achieving positive surgical outcomes and patient satisfaction.
A nurse-led clinical audit was undertaken in the operating theatre department of a major teaching hospital in Ireland to establish the incidence and management of IPH in the department. One hundred (n = 100) patients were included in the audit, both children and adults. Results of the audit were used to inform quality improvement initiatives, with the purpose of improving patient care standards in the operating theatre department in that hospital.
Keywords
Introduction
Inadvertent perioperative hypothermia (IPH) is a common problem associated with surgical patients which can have significant consequences during surgery and in the immediate postoperative period. It is defined as a core body temperature less than 36°C (Hart et al 2011, AORN 2016). IPH has been a cause of increased postoperative length of hospital stay by as much as 40%, and increases the risk of surgical site infections by 64% (Lynch et al 2010). Therefore the significance of recognising and managing IPH should not be underestimated. Indeed, promoting normothermia during the perioperative period (core body temperature 36–37.5°C) needs to remain an important aspect of perioperative nursing. This is a key factor in maintaining patient safety, achieving positive surgical outcomes and patient satisfaction.
A nurse-led clinical audit was undertaken in a major teaching hospital in Ireland, from November 2016 to February 2017. The purpose of this audit was to establish the incidence of IPH in the department and to examine how staff managed patient care to prevent IPH from occurring. The audit aimed to raise awareness amongst perioperative healthcare staff of the importance of and recognition of IPH. It endeavoured to illustrate the impact that IPH can have on surgical patients and to identify ways to improve patient outcomes.
Literature review
Classification and effects of IPH
Paulikas (2008) classifies hypothermia into three stages: mild, moderate and severe. Mild hypothermia is a core temperature ranging from 34–35°C, moderate hypothermia ranges in core temperature between 30–34°C and severe hypothermia occurs when core body temperature falls lower than 30°C. Complications that can arise as a result of IPH include coagulopathy, surgical wound infection (Choi 2007), increased allogeneic transfusions, delayed wound healing and morbid myocardial outcomes secondary to sympathetic nervous system activation (Welch 2002, Burger & Fitzpatrick 2009, Wagner 2010). Furthermore IPH can delay the length of the post anaesthetic recovery period and prolong hospitalisation (Weirich 2008, AORN 2016).
Patient shivering and discomfort occurs when the body attempts to regulate its own body temperature through a negative feedback system in the central nervous system, primarily in the hypothalamus. The hypothalamus acts as a thermostat, initiating heat-decreasing vasodilation or heat-increasing vasoconstriction as required in response to a change in body temperature (Sessler 2008).
Causative factors
Anaesthesia and the perioperative environment are two main contributing factors in IPH (Kurz 2001 cited in Knaepel 2012). General anaesthesia inhibits the thermoregulatory system and prohibits cellular metabolism, resulting in the body being unable to produce heat. The cool theatre suite environment contributes to the speed at which body heat is lost through convection and radiation from the skin and by evaporation from the surgical site (Kurz 2001 cited in Knaepel 2012). Additional elements which can decrease body temperature during surgery include the administration of unwarmed intravenous fluids (Paulikas 2008), a decreased basal metabolic rate, medication-induced vasodilation (Lynch et al 2010) and loss of heat from the lungs when unwarmed inhaled gases are mixed with warm air in the lungs (Good et al 2006, Singh 2014).
It is recommended that body temperature is monitored in patients undergoing general anaesthesia exceeding 30 minutes in duration and in every patient whose surgery will last more than one hour (NICE 2008, Sessler 2008). In the immediate preoperative period, patients can experience prolonged waiting in light surgical gowns and an extended period of fasting. This, in addition to the administration of premedication, may contribute to a reduction in core body temperature (Munday et al 2013).
Preventative measures
Consistent temperature measurement is crucial throughout the perioperative pathway in order to identify patients at risk of developing hypothermia and to identify those potentially at risk of further deterioration of temperature. Core body temperature can be measured in the pulmonary artery, the nasopharynx, distal oesophagus and the tympanic membrane (Lynch et al 2010) using monitoring techniques for axillary, oral, rectal, bladder and tympanic membrane and temporal methods. This remains an intrinsic responsibility of the perioperative nurse in delivery of care to his/her patients, in partnership with the anaesthetic and surgical teams.
Pre-warming patients on the ward is advocated by the National Institute for Health and Care Excellence (NICE 2008) for patients who are at risk of developing hypothermia prior to surgery. This can assist in maintaining normothermia throughout the perioperative care pathway. Pre-warming is associated with the rapid transfer of large amounts of heat to the patient before induction of anaesthesia. It causes vasodilation and increases the temperature of patient’s peripheral compartments. Pre-warming can continue to be performed both in the preoperative waiting area of the department and in the operating room (Kiekkas & Karga 2005, de Brito Proveda et al 2012) through the provision of warm blankets, forced warm air entry devices, thermal hats and leggings and a warm ambient room temperature. It is important to record all patients’ temperatures on arrival to the operating theatre department and to ensure their core body temperature is at and maintained at a minimum of 36°C.
Perioperative nurses must strive to ensure normothermia for all patients; they have a central role to play in preventing IPH. In that context they need to be aware of the implications that hypothermia can have on a patient undergoing surgery, the benefits of normothermia and the role that warming can have in improving overall patient outcomes. Prevention of IPH can bring about a reduction of the complications associated with this condition for the patient (Weirich 2008).
Clinical audit
A nurse-led clinical audit was undertaken in the hospital’s operating theatre department from November 2016 to February 2017. The purpose of this audit was to establish the incidence of IPH in the department, and to determine how staff managed patient care to prevent its occurrence. In this audit, a core body temperature of less than 36°C was signified as an indicator for IPH (Hart et al 2011). The audit aimed to raise awareness amongst perioperative healthcare staff on the importance and recognition of IPH. It set out to highlight to staff the impact IPH has on surgical patients and to identify their role in improving patient outcomes.
Key standards referred to and guiding the criteria on which the clinical audit tool was based included the following:
The local policy on the prevention and management of IPH in the hospital group (Cork University Hospital Group 2017) AORN recommended practices for the prevention of unplanned perioperative hypothermia (AORN 2016) NICE clinical guideline: The management of inadvertent perioperative hypothermia in adults (NICE 2008).
This nurse led audit, which occurred in consultation with the departments of anaesthesia and surgery, sought to determine at what specific part of the perioperative pathway the issue of IPH commenced, what interventions were put in place and by whom, and the effectiveness of these interventions.
The audit tool
The audit tool (Appendix 1) was developed by the audit leads (clinical nurse manager in the emergency theatre suite, anaesthetic nursing manager, acting clinical facilitator), with input from two consultant anaesthetists and one general surgical consultant. The questions were developed on evidence based criteria sourced from both local policy and NICE guidelines (2008). The audit tool was tested in a pilot phase and adjusted to include all patients (children omitted from pilot), length and type of surgery and whether elective or emergency surgery, the type of anaesthesia delivered and risk factors for IPH.
This prospective audit selected 100 patients (n = 100), both adults and children and was conducted over a four month period from November 2016 to February 2017. Verbal consent from patients was obtained prior to taking and recording temperature. Five theatre suites in the department were included in the audit catering for the following surgical specialities: breast, urology, vascular, cardiac and emergency surgery. All patients included in the audit had their temperature and the interventions implemented in the recovery room recorded.
Each patient’s temperature was recorded at five different intervals during the perioperative pathway (on arrival to theatre reception, on arrival to theatre suite, leaving theatre suite, on arrival to recovery room, leaving recovery room). Core temperature was recorded using tympanic membrane thermometers.
The warming interventions implemented in each area were recorded including use of the following interventions: warm blankets, forced warm air entry blankets, thermal hat and leggings and warm intravenous fluids.
Patient details, the surgery performed and the patient’s risk factors were recorded. These risk factors included: patient exposure, type of anaesthesia (+/− combined), fasting time (reduced metabolism), patient’s age, health status (ASA Grade 2 or over), cardiovascular disease, BMI, major surgery (>2 hours, abdominal surgery) and use of premedication (AORN 2014).
Results
One hundred (n = 100) patients were included in the audit: 13 children (<16 years) included 10 males and 3 females. 87 adults (>16 years) included 33 males and 54 females. The average age of patient was 47.3 years, with a range of 1 year 2 months to 87 years. Twenty four percent had elective surgery and 72% emergency surgery. Forty six percent of participants were inpatients, 41% were admitted via Day Of Surgery Admission Unit (DOSA), with the remaining 12% of patients whose admission source not recorded.
Temperature on arrival
The average waiting time in theatre reception was 34 minutes. Patient’s temperatures arriving into the theatre suite were recorded and the results show an average of 36.1°C with 10 patients recording a temperature >36° (range 35.6–35.9°) as shown in Figure 1.
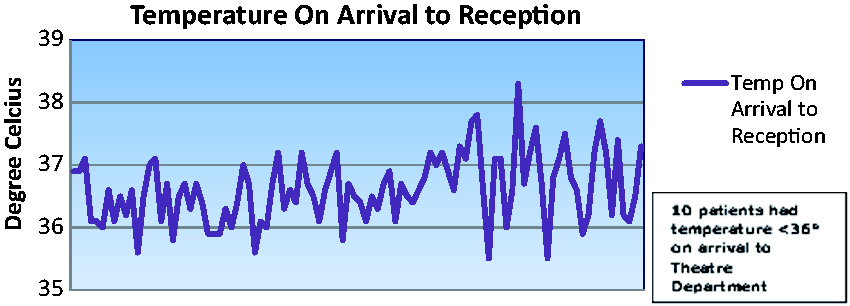
Patient temperatures recorded on arrival to operating theatre reception with 10 patients presenting with temperature >36
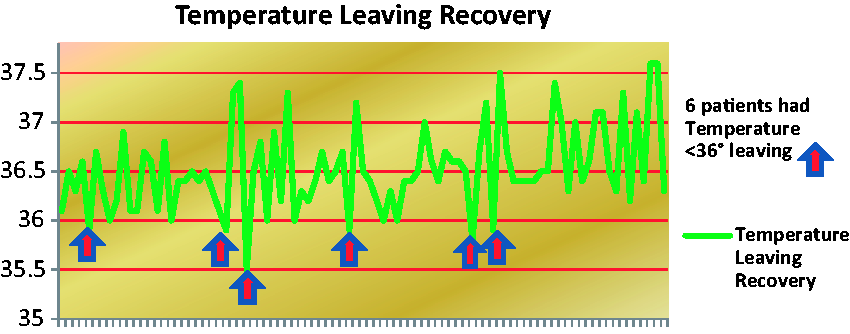
Patient temperatures recorded leaving operating theatre recovery room whereby 6 patients were discharged with temperatures ranging from 35.5-35.9
Temperatures recorded following the procedure
Patients had their temperatures recorded when leaving theatre suite, arriving in recovery and on leaving recovery. What is of note is that 19 patients had a temperature <36°C on leaving theatre suite, with 6 patients with a temperature recording at <36°C on leaving the department. Of these 6 patients, four patients had a temperature of 35.9°C, one 35.8°C and one 35.5°C (Figure 2). For these patients discharge was permitted as per local discharge from recovery guidelines with ongoing active reheating in place on return to the ward.
Warming interventions and their combination of use during surgery are outlined in Figure 3. The forced warm air entry Bair Hugger™ was the most popular choice.
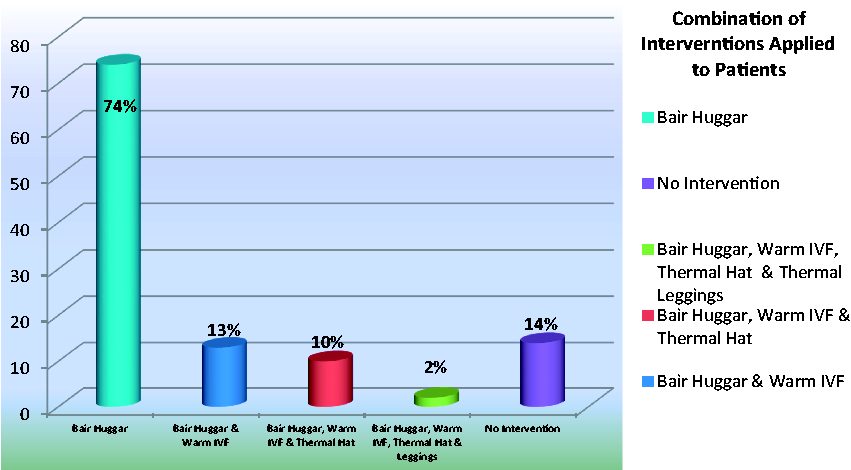
Warming Interventions and a combination of their use during surgical procedures
Risk factors
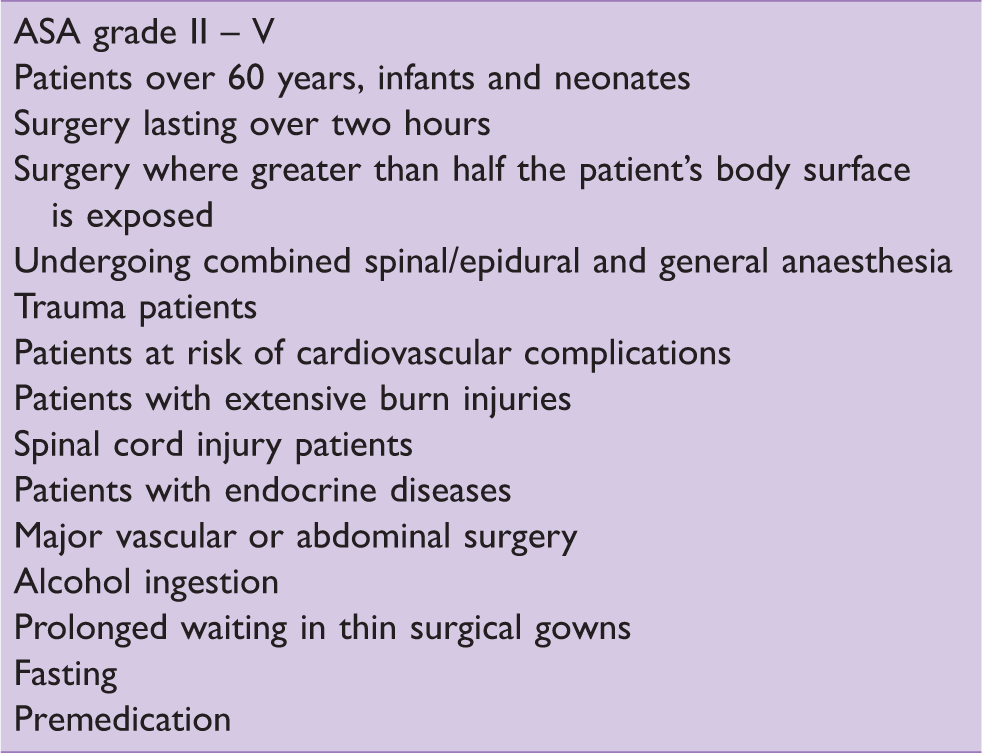
Eight percent of patients did not have any ASA risk factors recorded. Of the 92% of patients who did, 21% of these had fasting as the sole risk factor, 16% had 2 risk factors with a remaining 55% having 2 or more risk factors recorded. The risk factors are outlined in Table 1.
Risk factors for inadvertent hypothermia (Sources: NICE 2008, Lynch et al 2010, Munday et al 2013, AORN 2014)
Considering the 43 patients who had three or more risk factors, 81% (n = 35) of these had only one intervention used during surgery: the Bair Hugger™. Forty three percent (n = 20) had two interventions and 23% (n = 10) had three interventions. From temperatures recorded on leaving the theatre suite in this higher risk patient cohort, the results identified that eight patients (18%) had temperatures less than 36°C. Of these patients, one did not have any interventions applied (35.6°C), with one having no recorded intervention (35.6°C). This outlines that use of the Bair Hugger™ is most frequent with this high risk group.
Figure 4 goes further to outline the patient risk category group having either one, two, three or more risk factors for inadvertent hypothermia, the number of interventions used in this patient group and the temperatures recorded above and below normothermia.
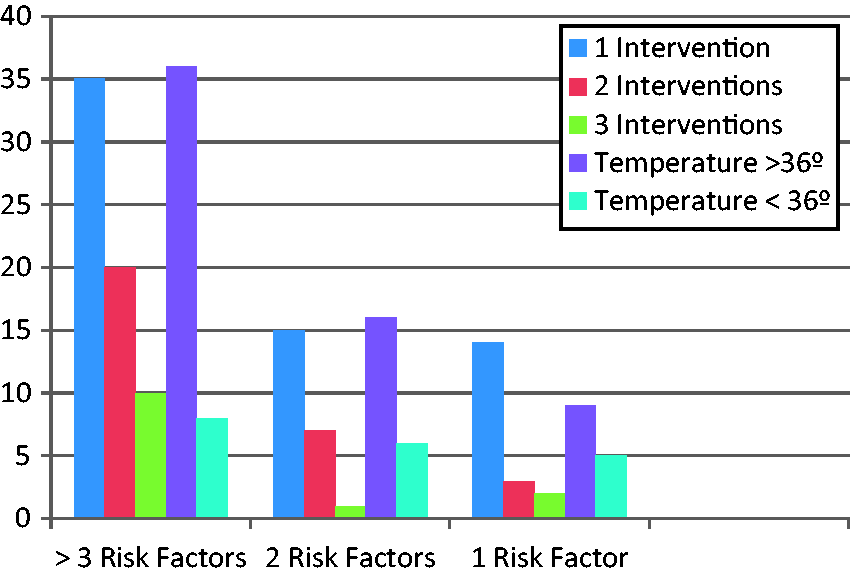
goes further to outline the patient risk category group having either one, two, three or more risk factors for inadvertent hypothermia, the number of interventions used in this patient group and the temperatures recorded above and below normothermia.
Implementation of results
The results of the audit were examined and used to inform quality improvement initiatives, with the purpose of improving patient care standards in the operating theatre department in this hospital. These initiatives included the provision of education for staff in the department, revision of local policy and provision of adequate resources for recording temperature and active reheating equipment throughout the department.
Presentation of the results of this audit has resulted in an increase in staff awareness of the incidence of IPH and an improved awareness of the patient care interventions required to prevent it. There is anecdotal evidence through verbal feedback from staff that individual consideration is now given to each patient by incorporating warming measures as early as possible in their perioperative pathway, from arrival in the reception area right throughout their period in the department. Additional thermometers have been made readily available throughout the department to assess and monitor patient temperature during their perioperative journey. Furthermore, the hospital policy on prevention and management of IPH has been reviewed and updated accordingly.
Conclusion
Clinical guidelines for the prevention and management of IPH should be readily available and accessible for staff in the clinical area. An understanding and knowledge of the causes, contributory factors and methods of preventing and treating IPH is a necessity for all perioperative healthcare staff. Vigilant patient care, together with awareness of the hazards of hypothermia, and the correct use of warming equipment and monitoring techniques will help to reduce and prevent the incidence of this condition. In addition, providing regular education sessions for staff (nurses, doctors, porters and healthcare assistants) across the operating theatre department on the management of IPH is a key factor in achieving successful outcomes in this regard. Extending this education to staff at ward level and in the day of surgery admission units is also warranted.
Nurses in the perioperative setting have a central role to play in preventing inadvertent perioperative hypothermia. They can lead the perioperative team in promoting patient safety by implementing warming measures for the patient throughout their perioperative pathway. Safe and effective patient care is of paramount importance. Patients have a right to expect the highest standard of care possible and nurses have a professional responsibility to ensure that they receive it.
No competing interests declared