
Abstract
Aim
To assess the clinical parameters and compare the stress and pain response between fast-track recovery protocol and conventional treatment in patients undergoing major liver resection.
Methods
Eighty-eight patients suffering from malignant liver tumours were surgically treated from May 2012 to March 2015. After randomisation, they were prospectively divided into two groups: group fast-track patients (n = 46) and group conventional treatment patients (n = 42). Demographic and clinical data were collected and patients were assessed with pain scale (behavioural observation scale and visual analog scale), while depression levels were evaluated with Zung self-rating depression scale and three Numeric Analog Scale self-reported questions. Peripheral blood samples were collected at time points: T1 on the admission day, T2 on the day of surgery and T3 on the day of discharge examining serum levels of adrenocorticotropic hormone and cortisol.
Conclusion
Fast-track recovery protocols seem to be associated with improvement in several clinical parameters, without compromising, biologic or emotional stress in patients undergoing major liver resection.
Keywords
Introduction
The hypothalamic-pituitary-adrenal (HPA) axis is a neuro-endocrine system that regulates circulating levels of glucocorticoid hormones. These hormones are vital for normal homeostasis and play a pivotal role in the response to stress (Gibbison et al 2013). During the last 20 years, stress response to surgery and trauma through the hormones has been studied extensively. Plasma adrenocorticotropic hormone (ACTH) and cortisol concentrations increase in response to surgery and trauma. There is considerable inter-individual variation in the HPA response to surgical stress. In addition, the pulsatile secretory patterns of ACTH and cortisol contribute to the apparent variability in the measured responses to surgical stress (Salem et al 1994). Dimopoulou et al (2008) showed that after major surgery, the cortisol and ACTH levels are elevated, in early phase. Progressively, cortisol levels remain higher, but ACTH levels return to the preoperative levels (Dimopoulou et al 2008).
Pain is a common symptom after surgery, so pain’s management and treatment are major elements in all phases of postoperative hospitalisation. Undertreated postoperative pain directly influences postoperative care as well as the patient’s ability to endure treatment and to return to everyday life. Consequently, a reliable pain assessment is a major step for optimal postoperative pain management, while pain intensity is achieved using visual analogue scales and numerical rating scales (Kim et al 2012).
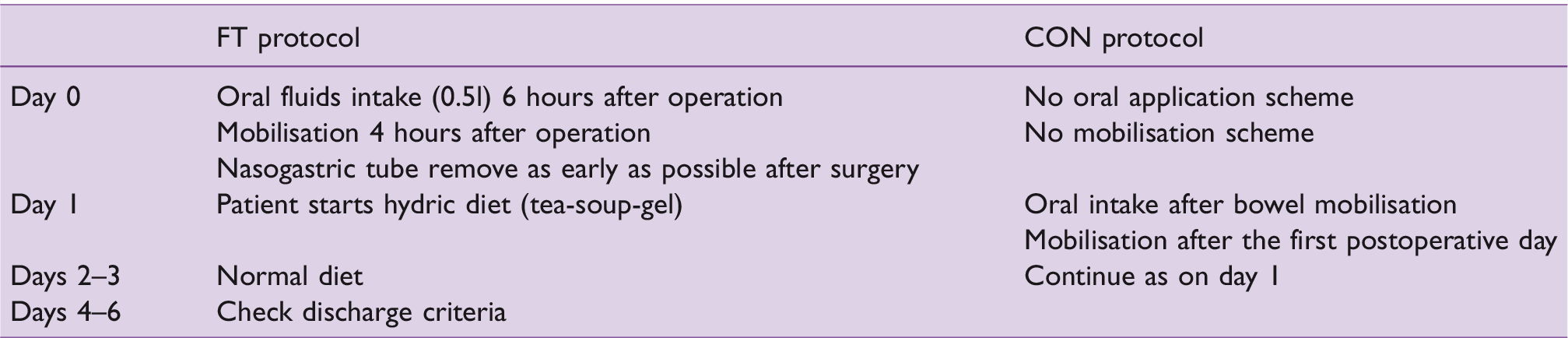
During the last two decades, enhanced recovery programs (ERAS) or fast-track protocols (FT) after surgery led to a significant evolution in patient’s treatment after carrying out multiple studies in different kinds of surgery, such as cardiac and colorectal. The widespread implementation of FT suggests possible benefits, by reducing length of hospital stay and hospital readmissions, correlating with fewer postoperative complications and improving patient outcomes (Paton et al 2014). FT protocol includes early oral nutrition (6 h after the surgery) in combination with early mobilisation and pain control, principally avoiding opioids, while the patient is hospitalised only for five to six days, postoperatively (Chen et al 2014). Contrarily, conventional postoperative treatment protocol (CON) comprehends oral diet after the mobilisation of colon, whilst the patient mobilises during the first or second postoperative day, progressively. Compared to CON, FT protocol’s implementation has shown less complications and postoperative hospitalisation for patients (Kehlet 2014).
Although there is some evidence evaluating ERAS programs in colorectal surgery, there is a paucity of data concerning FT recovery after major liver resection, particularly dealing with postoperative stress through serum cortisol and ACTH levels as well as post-hepatectomy analgesia. The ultimate aim of this research is to objectively assess the clinical condition of patients so as to improve the quality of their care and hospitalisation.
Material and methods
Research design
This is a randomised clinical study, with repeated measurements, comparisons and a prospective correlational design. The study was conducted at a major Oncological Hospital in Greece from May 2012 to March 2015, and it was part of a broader clinical trial (No clinicaltrials.gov, Registration Number: NCT02524925).
The two patient groups sample was generated through randomisation process using the ‘Random sampling’ tool from software SPSS 22.0 (IMB SPSS Software, Chicago, Illinois). The patients’ admission codes, which were generated through the program, determined the group that each patient should join after his/her appearance at the hospital.
Ethical review
The research was approved by the Scientific Committee of the Hospital (approval number: 4051/448) where it was conducted and the Ethical Committee of National and Kapodistrian University (approval number: 87).
In order to participate in the protocol, all participants were asked to sign an informed consent. A full respect of the confidentiality of information throughout the collection and procession of data was maintained. The study was carried out in compliance with the required ethical standards of the Declaration of Helsinki.
Sample of patients and control group
The sample size of the patients was based on Jones et al (2013). Ninety-seven consecutively admitted liver cancer patients, who should undergo hepatectomy, were assessed for eligibility according to the following inclusion criteria: normal level of consciousness and communication, aged 30–82 years old. Patients with chronic pain, kidney disease, neuropathy and systemic or chronic treatment with analgesics were excluded from the study, since these conditions interfere with the physiological mechanisms underlying the response to pain and stress. According to the abovementioned criteria, the study’s sample consisted of 88 patients who underwent hepatectomy and were randomised into two groups.
In the FT group, the FT perioperative nursing care protocol was applied, whereas in the CON group, the conventional one was applied. The two protocols followed are shown in Table 1 (Spelt et al 2011). In order to ensure homogeneity of surgical treatment and nursing care, all participants were operated by the same anaesthesiology and surgical team, consisting of specialists in liver surgery and surgical oncology, and nursing perioperative care took place in one hospital ward. The anaesthesia was standardised, so as to provide the same postoperative conditions, in both groups.
Comparative presentation of FT and CON protocols’ parameters followed during postoperative nursing care of patients underwent liver resection
Collection of data and blood samples
Patients’ anthropometric demographic and clinical data, such as gender, age body height, body weight, body mass index (BMI) and kind of surgery (right or left liver resection) were collected. Also, the postoperative day of mobilisation and resumption of normal diet were recorded, and total days of administrating intravenous fluids, day of removal of urinary catheter/nasogastric tube and amount of abdominal drainage, length of postoperative hospitalisation and the presence or absence of nausea/vomiting and complications (such as haemorrhage and cholera) were evaluated.
Peripheral blood samples were collected at three different time points: T1, the day of admission; T2, the day of surgery and T3, the day before discharging for FT group or the fifth postoperative day for the CON group. Collected blood samples were then centrifuged at 3000 r/min for 20 min, and the sera were stored at –80°C. ACTH (pg/ml) and cortisol (ng/ml) serum levels quantification were performed by ECLIA (electrochemiluminescence immunoassay). The biomarkers were analyzed in a private laboratory which developed its own ECLIA.
Assessment of pain, stress, emotional status and depression levels
Pain levels were assessed by (a) BPS (behavioural observation scale) (Puntillo et al 2001), which ranges 0–1 ‘no pain’, 2–4 ‘aching’ 5–7 ‘moderate pain’ and 8–10 ‘severe pain’. This scale was used only at the operation day (T2) because of patients’ impaired level of communication, due to anaesthesia (b) the self-assessment pain scale VAS (Visual Analog Scale, which is a horizontal line, 10cm in length, anchored by word descriptors at each end: ‘no pain’ (score of 0) and ‘worst imaginable pain’ (score of 10) (Wewers & Lowe 1990).
Moreover, patients’ emotional status levels were evaluated by 3 NAS (Numeric Analog Scale) question of self-reported numeric analogue scales (NAS: 0–10) questions (0 = Not at all to 10 = Very Much), simultaneously with the blood samples: ‘How sad are you feeling right now?’, ‘How stressed do you feel right now? and ‘How optimistic you feel, right now?’ These questions have been piloted in intensive care and have shown high correlations with established patient stress scales, such as Hospital Anxiety and Depression Scale and Hamilton scale and stress neuropeptides in patients’ sera (Kapritsou et al 2017; Kletsiou 2012; Mpouzika et al 2013). The analgesia administration followed the standard clinical practice in both groups.
Depression levels were evaluated using the Zung scale (Zung self-rating depression scale), which assesses depression levels with a score 25–49 for ‘normal level mood’, 50–59 for ‘mild depression’, 60–69 for ‘moderate depression’ and 70 + for ‘severe depression’ (Carrell 1978).
Zung and BPS scales have already been adapted to the Greek language and evaluated their validity and consistency (Kletsiou 2012; Mpouzika et al 2013; Papathanassoglou et al 2015) and calculated the internal consistency Cronbach’s α index, whose values were adequate:
✓ Cronbach’s alpha was:
– Zung scale: α = 0.789 – BPS scale: α = 0.754
Statistical analysis
Statistical analysis was performed by SPSS 22 (IMB SPSS Software, Chicago, IL) and the parameters were compared as described previously between the two groups of patients after conducting Kolmogorov–Smirnov test of normality. Comparisons were made using Fisher’s exact test, the chi-square test and Mann–Whitney test. Linear mixed models (LMM) were applied for repeated measurements. According the CONSORT statement, all LMM are reported unadjusted (independent variables; group, time, age and BMI) and adjusted for potential covariates. The models are adjusted for the following baseline measurements: age, gender and BMI as well as pain levels (VAS scale). The data are expressed as mean (SD), in significant level 0.05.
Results
Demographic data
Eighty-eight patients participated in the study (46 males and 42 females) that underwent hepatectomy and were randomised into two groups. In the ERAS group, 46 patients followed the ERAS protocol, while in the CON group, 42 patients applied the conventional (CON) protocol. The trial profile is reported in Figure 1. After randomisation, patients did not withdraw.
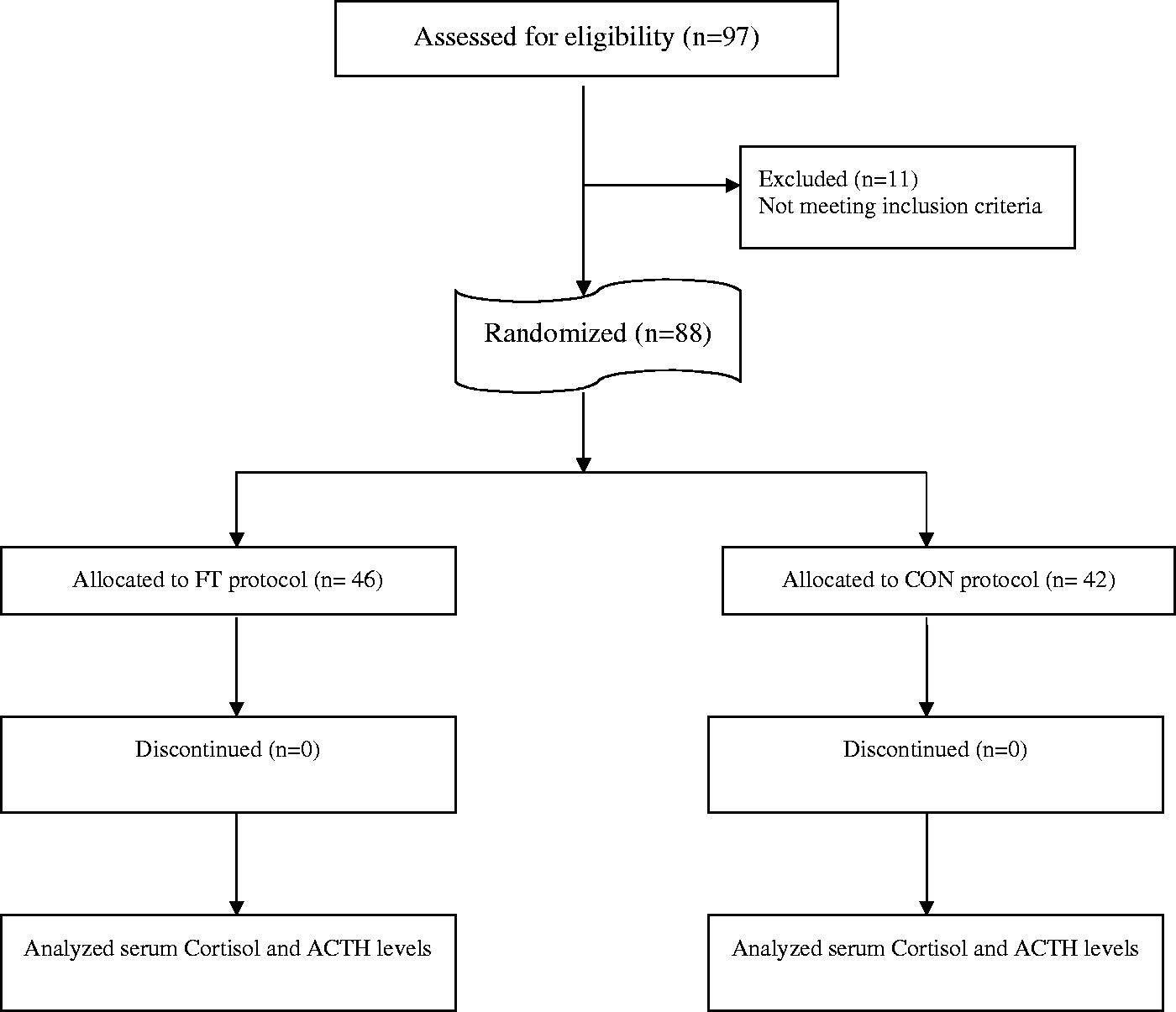
Flow-chart of patients’ sample
In group FT, 46 patients followed the FT protocol, while in the CON group, 42 patients applied the CON protocol.
The results of the demographic data are shown in Table 2. There was no significant difference in age, body weight, body height and BMI. Also, the kind of surgery is shown in Table 2, where there were no significant differences after adjusting for protocol with ANCOVA test (F = 0.393, p = 0.813).
Participants’ demographic anthropometric and clinical data showing that the two groups were adequately equivalent after randomization

Postoperative care recovery
There was significant difference in the days of early activity. Group FT had an average of 0.17 (0.4) and group CON 1.9 (1.99). Patients who participated in the FT protocol started to mobilise at least 4 h after the surgery, progressively, while patients in the CON group mobilised the first postoperative day (U = 141, p < 0.001).
A significant difference in the time of tolerating clear liquids was noted (U = 118, p < 0.001) with the average for group FT being 0.67 days (1.63) and for group CON being 3.6 days (0.25). In addition, there was a statistical difference in resuming a full liquid diet, as well, between the two protocols (U = 283, p < 0.001) for group FT being 2.15 days (1.38) and for group CON being 5.19 days (3.17). A significant difference in the time of tolerating normal meal, postoperatively, was also noted (U = 303, p < 0.001) with the average for group FT being 3.76 days (1.43) and for group CON being 6.76 days (3.12). Patients in the FT group had a meal at least one day earlier.
The overall length of intravenous fluid administration after surgery was an average of 2.5 days (1.37) for the group FT and was an average of 6.4 days (5.71) for group CON. The difference was significantly shorter (at least one day) in group FT (U = 330.5, p < 0.001).
The overall length of hospital stay, postoperatively, was 5.5 days in average (0.83) for group FT, and was an average of 11.2 days (6.05) for group CON. As of this, hospitalisation period was significantly shorter in the FT group, for at least two days (U = 180.5, p < 0.001).
Eleven out of 46 patients showed complications in the FT group; in particular, 8 patients had nausea/vomiting and 2 patients had fever. By contrast, 21 patients in the CON group had complications. Seven patients had nausea/vomiting, 8 fever, 2 rapture of anastomosis, 2 haemorrhage and 2 cholera. The percentage of complications for the patients treated in group FT was 23.9% compared to group CON, which was 50%. Hence, the risk was 2.09 higher in patients treated in group CON (chi2 = 7.68, df = 1, p = 0.007).
Four patients were readmitted to hospital during the first postoperative month, from group FT. In contrast, six had readmissions (chi2 = 0.681, df = 1, p = 0.409) in group CON that was noticed during that same period. Patients were readmitted because of fever and vomiting.
Evaluation of postoperative stress and pain levels
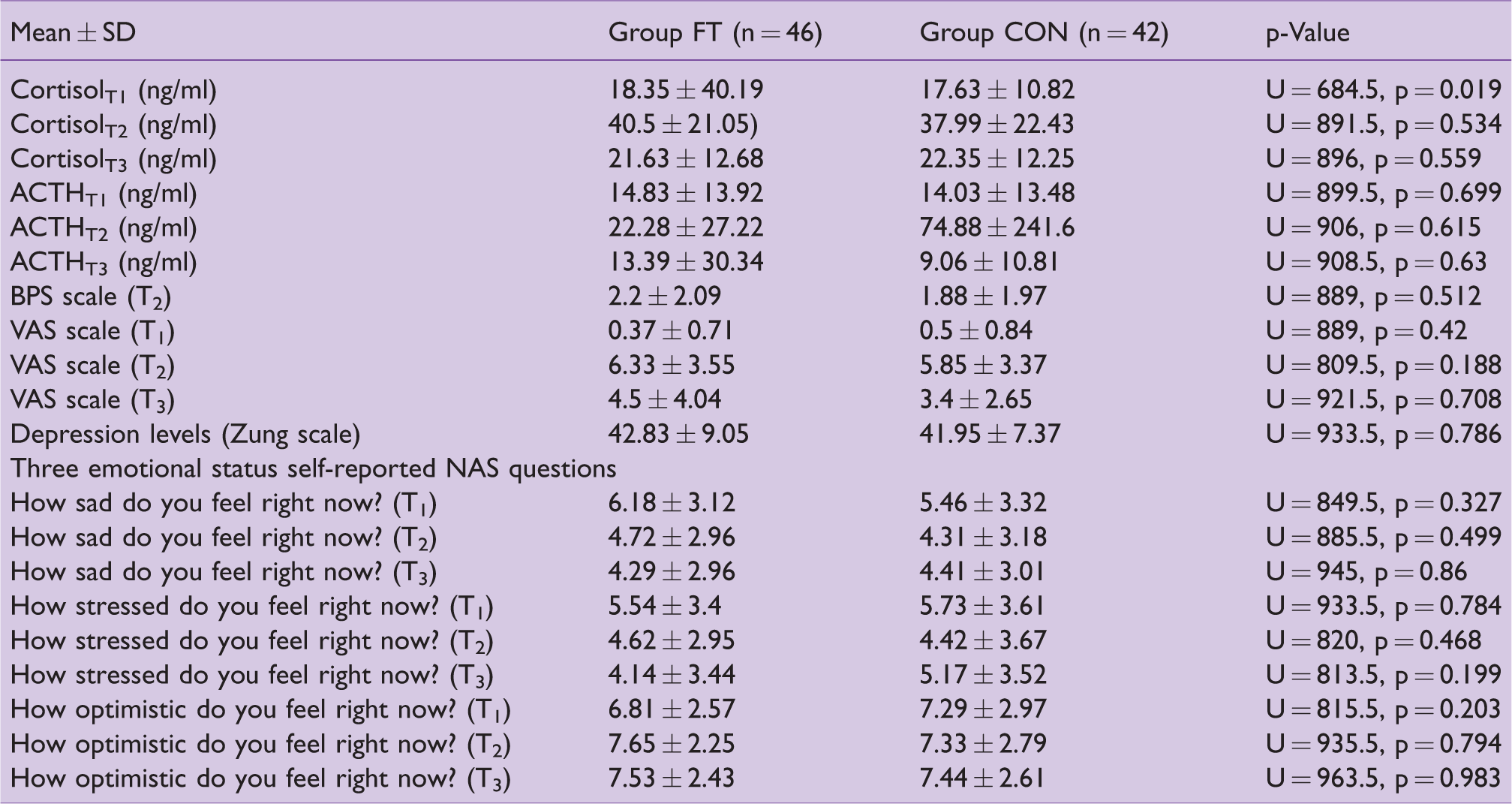
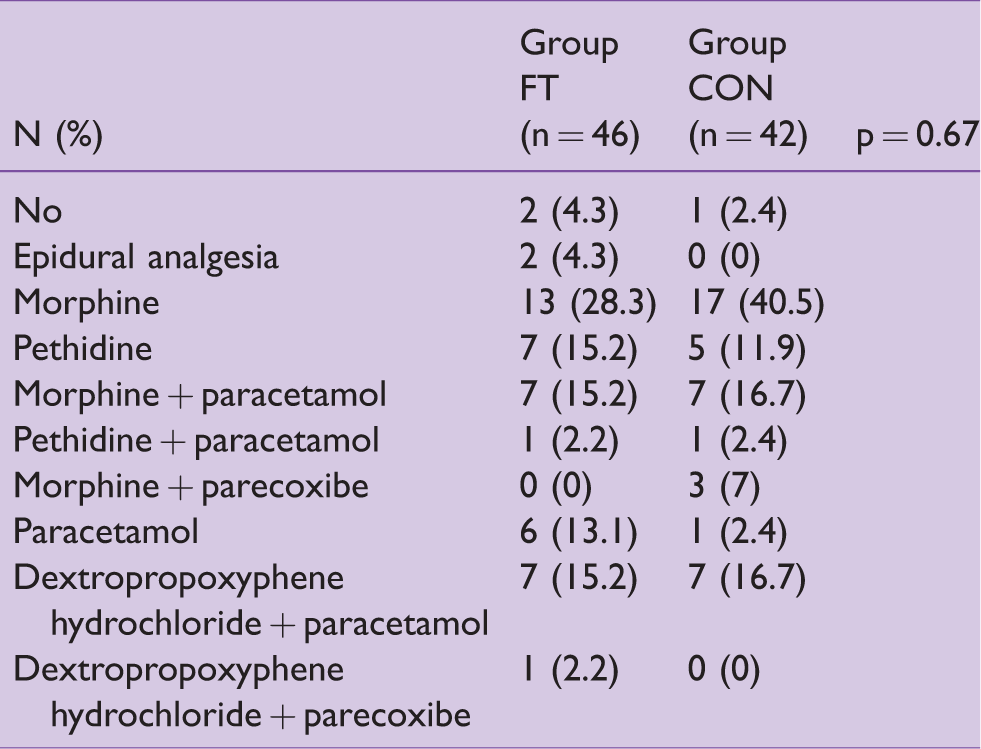
There was a significant difference in the serum levels of CortisolT1 and after adjusting for age, gender and BMI with ANCOVA test (F = 2.84, p = 0.095; F = 0.195, p = 0.66; F = 0.005, p = 0.946; respectively). The results of stress and pain levels are shown in Table 3. The pain scores were dynamic. The pain medication, which patients have received, is shown in Table 4.
Comparisons between the FT AND CON group patients for serum ACTH, Cortisol, pain, depression and emotional status levels at different time points
Participants’ pain medication
Bi-variate associations among stress and pain levels and cortisol and ACTH levels
In the FT group, no correlation was observed. But in the CON group, a positive correlation was noted between ACTHT3 and the NAS questions: ‘How sad are you feeling right now?’ T2; ‘How stressed do you feel right now?’T2 (ρ= 0.392, p = 0.01, ρ = 0.302, p = 0.05, respectively). Also, a positive correlation was observed between ACTHT3 and the NAS questions: ‘How sad are you feeling right now?’ T3, ‘How stressed do you feel right now?’ T3 (ρ = 0.352, p = 0.022, ρ = 0.416, p = 0.006, respectively), in CON group.
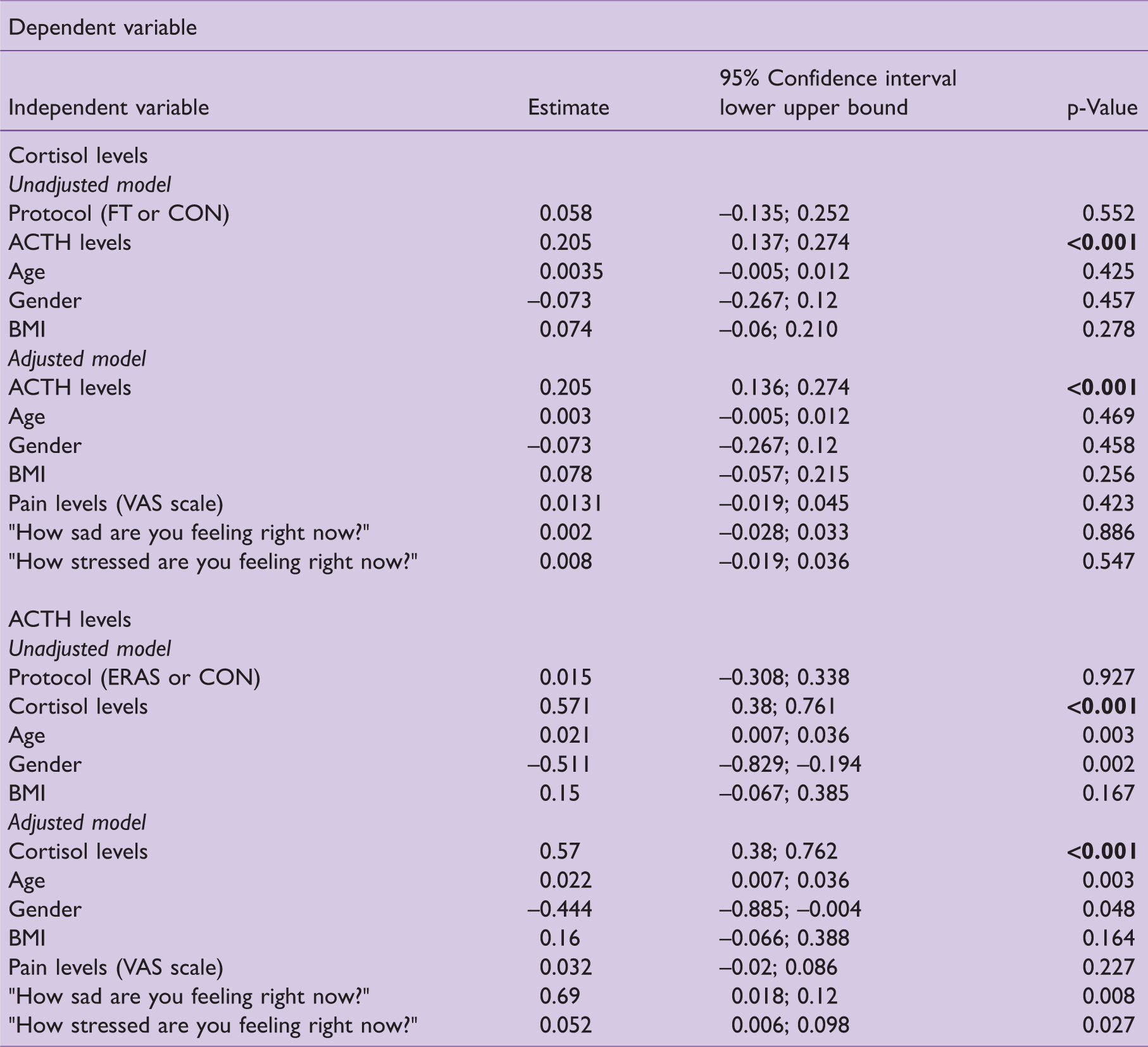
Linear mixed models for serum cortisol and ACTH levels
In Table 5, the interactions of cortisol and ACTH levels and the parameters of the two protocols are shown. In the adjusted model, for protocol ERAS or CON, it was shown that ACTH levels, age and gender interacted positively (p = 0.003 and p = 0.048, respectively). Furthermore, in the adjusted model, ACTH levels positively interacted with the NAS questions ‘How sad are you feeling right now?’ and ‘How stressed do you feel right now?’ (p = 0.008 and p = 0.027, respectively).
Linear mixed models for serum cortisol and ACTH levels
Discussion
This prospective study compares two different groups of patients surgically treated with liver resection for primary or metastatic cancer that followed either enhanced recovery or conventional treatment protocol. It mainly focused on measuring serum ACTH and cortisol levels during perioperative recovery as well as postoperative outcomes, including resumption of physical activity, beginning of oral alimentation, intravenous fluids administration and effective analgesia.
The basic findings of this study included: (a) a significant difference in serum cortisol levels in FT group during the day of admission, (b) FT protocol showed to be superior in important parameters of postoperative recovery after major liver resection, including earlier mobilisation and resumption of normal diet, as well as shorter length of postoperative hospitalisation, compared to CON post-operative nursing care protocol and (c) serum ACTH levels were positively correlated with the NAS questions ‘How sad are you feeling right now?’ and ‘How stressed do you feel right now?’ the day of the surgery and before discharge. The interpretation of these data needs to be considered with caution due to the limitations of the study, including the relatively restricted patient population.
Many studies and systematic reviews have evaluated safety and efficacy of ERAS programs after abdominal surgery, where FT programs were associated with beneficial clinical outcomes, such as less morbidity, early resumption of normal diet and mobilisation, and shorter postoperative hospitalisation. For these reasons, ERAS programs have been implemented in clinical fields, for example colorectal, hip and knee surgery, as well cardiovascular surgery and their application has been explored in hepatopancreatobiliary surgery (Braga et al 2014, Guan et al 2014, Hoffmann & Kettelhack 2012, Jones et al 2013, MacKay & O’Dwyer 2008, Zhao et al 2012).
Also, in the present study, patients had their first sips of water even (0.5l) 6 h after the surgery, resuming oral diet the second postoperative day. Stoot et al (2009) found that a shorter period to successful resumption of a normal diet was needed, in the FT group of patients. In the studies of Koea et al (2009), Stoot et al (2009) and Wu et al. (2015), patients started oral intake the day of the surgery. Early resumption of oral solid diet reduces the risk of onset of infection and the mean length of postoperative hospitalisation. Therefore, there is no risk for the anastomosis by the early resumption of oral diet (Maessen et al 2007).
Likewise, mobilisation of our patients occurred 4 h after the operation, while full ambulation was achieved during the first postoperative day, for at least four times daily. In other studies, patients were mobilised during the first, second and third postoperative days, such as in the study of Hall et al (2012). Insulin resistance and muscle loss could be caused from no immediate mobilisation, whilst pulmonary function and tissue oxygenation are decreased; in addition, increased risk of thromboembolism could be observed. Consequently, the implementation of FT protocols reduces the occurrence of such complications (Fearon et al 2005).
In the present study, the length of postoperative hospital stay was reduced by at least five to seven days in the FT group of patients, which is in agreement with other studies. Jones et al (2013) have shown a reduction of postoperative stay by at least three days (p = 0.02). Wu et al (2015) have shown that hospital stay was reduced from 11 to 7 days, but there were no significant differences in rates of readmission, morbidity and mortality between the two groups. In the study of Stoot et al (2009), the median hospital study was six days in the FT group compared with eight days in the control group (p-value < 0.001). Studies have shown that FT programs result in a significant reduction of hospital stay, at least five days postoperatively (Stoot et al 2009).
Perioperative mortality and morbidity were 50% and 21.7% for the CON and FT group, respectively, in our study. The complication rates correspond well with studies such as Stoot et al (2009) was 15.3% (FT) versus 15.3% (CON). Hendry et al (2010) calculated a 30-day morbidity rate to 17% for the FT group. In these studies, as well as in ours, there has been a significant trend in reducing postoperative morbidity in the FT group. In contrast, in the study of Clark et al (2016), there was no significant difference in morbidity between the two groups (p = 0.343).
There was no significant difference in the readmission rate between the two groups studied. In the study of Connor et al (2013), readmitted patients were 11% of 128 patients for the FT group, while Schultz et al (2013) observed a 6% readmission rate in the FT group.
Preoperatively, in the present study, a significant difference in cortisol levels was observed between the two groups. FT group had higher levels in comparison to the CON group (p = 0.019). One possible interpretation could be possibly attributed to the higher stress level after being informed for participation in the protocol.
Moreover, in our study, serum ACTH levels were positively correlated and interacted with sadness and stress levels. Like in the studies of Mpouzika et al (2013) and Papathanasoglou et al (2015) in critically ill patients, there was a positive correlation between ACTH levels and intensity of stress (r = 0.34, p = 0.05), and serum ACTH levels were higher the day of maximum severity, respectively.
In pain levels, evaluating with VAS scale, in our study, there was no significant difference between the two groups. But in the study of Liang et al (2016), there was a statistical difference between FT and control groups. In the FT group, lower pain levels (p < 0.001) was observed, probably due to the fact that postoperative pain control was managed with patient-controlled intravenous analgesia, but in our study, the standard clinical analgesia practice was followed (Liang et al 2016). Furthermore, after liver resection for cirrhosis, on the second and third postoperative intravenous (IV) fentanyl PCA epidural analgesia reduced pain scores slightly with no further benefits (Recommendation: Level II) (Fayed et al 2014).
Last but not least, there are many studies, which were debating the value of epidural analgesia, after hepatic surgery. In 2014, Rosero et al showed that this technique was infrequently used (5.9% out of 68,028 operations) (Recommendation: Level IV). Also, in the same study, the authors noted that implementation of epidural anaesthesia/analgesia was correlated with higher need for blood transfusion and longer postoperative hospital stay (Recommendation: Level III-2) (Rosero et al 2014), while in another study, two patients were required correction of coagulopathy prior to the removal of epidural catheter. The comparison with intramuscular administration of morphine, IV PCA fentanyl was not superior, only 12 h postoperatively, whilst reduced blood loss (Recommendation: Level III-2) (Kasivisvanathan et al 2014).
On the other hand, Mondor et al (2010) have found significantly improved analgesia effect and a 50% opioid-sparing effect (Recommendation: Level II). At the same time, epidural analgesia resulted in lower pain scores than continuous local anaesthetic wound infiltration, without any other significant outcome (Recommendation: Level II) (Revie et al 2012). Likewise, after liver transplantation, IV PCA opioids improved analgesia but no other outcomes were mentioned (Recommendation: Level III-2) (Clarke et al 2011).
To the best of our knowledge, this is the first study that evaluates serum ACTH and cortisol levels as postoperative markers of stress and pain response after implementation of FT protocols in patients undergoing major liver resection. The absence of significant differences in ACTH and cortisol measurements may be due to the smooth and harmless acceptance of the aggressive measures taken in the FT protocols. In line with that, those FT practices do not seem to compromise biologic or emotional stress after major liver resection.
Study limitation
The study has been conducted in the same hospital ward to avoid bias. The nurses of the clinical ward were receiving training to follow the protocol; in addition, information to complete the scales were given by the researcher to the patients.
Despite the careful preparation of this trial, the researchers were aware of the study limitations. It is difficult to generalise the results for the entire population of oncological patients, who undergo major liver resection, because they come from a single centre, which is the main limitation of this study. A larger sample size, originating from different clinics and various hospitals would help, significantly, to generalise the results.
Clinical and research direction
A future research could attempt to study the associations between pain scales and postoperative stress levels with various neuropeptides, such as substance P and other biomolecules. In addition, in the present study, all the parameters that could be included in FT protocols were not evaluated, so further investigation of all parameters could lead to new findings.
The ultimate goal will be to find objective stress and pain indicators, which will allow to the clinicians objective evaluation of patients, which due to their clinical condition’s severity, cannot verbally communicate. Also, major aim of this research is to objectively improve patient’s quality of care and hospitalisation.
Conclusion
FT recovery protocols seem to be associated with improvement in several clinical parameters, such as postoperative morbidity, feeding and ambulation, without compromising, biologic or emotional stress in patients undergoing major liver resection. Therefore, FT protocol replaces CON postoperative care in many hospitals, worldwide.
Summary statement
Fast-track protocol suggests benefits, such as reducing length of hospital stay and correlating with fewer postoperative complications
There is a paucity of data concerning FT recovery after major liver resection, particularly dealing with postoperative stress through serum cortisol and adrenocorticotropic hormone levels.
It will be to find objective stress and pain indicators, which will allow to the clinicians objective evaluation of patients, which due to their clinical condition’s severity, cannot verbally communicate.
No competing interests declared.
ORCID iD
Maria Kapritsou http://orcid.org/0000-0002-8187-4978 Margarita Giannakopoulou http://orcid.org/0000-0001-8781-0070