
Abstract
Surgeons instruct the patients to avoid postoperative bathing and dress the wounds until the sutures are removed. All wounds were sutured at the end of surgery and kept undressed. Participants received a tap water body bath where the water covered the wound after 24h of surgery. The control group were asked not to wet the dressed surgical site until wound inspection on days 3 and 5. The patients were followed up in the surgery clinic on days 14 and 30 after surgery, when age, sex and type of surgery-matched controls’ surgical site infection was significantly high in clean/contaminated and contaminated appendicectomy, breast lump excision, inguinal herniotomy and tendon repair surgeries. In contaminated appendicectomy, clean/contaminated and contaminated herniotomies postsurgical infections other than surgical site infection were significantly low in test groups. Early mobilisation, keeping the surgical wounds moist and providing a clean environment are suitable to minimise the surgical wound and other associated infections.
Introduction
The surgical site infection (SSI) is a major postoperative complication (Gupta et al 2014). Usually, at the end of the surgery, before the patient leaves the operating theatre, surgical wound is covered using gauze, adhesive tape or a pad and sometimes, an antibiotic is topically applied. Traditionally, the surgeons instruct the patients to keep the surgical incision covered, dry and avoid bath until the sutures are removed (Dayton et al 2013).
The prophylaxis of topical application of antibiotics for surgical wounds increases the evolution of antimicrobial resistance (Engelbert et al 2014). Staphylococcus aureus, coagulase-negative Staphylococci, Enterococcus sp. and Escherichia coli remain the most frequently isolated pathogens from infected surgical wounds. An increasing proportion of SSIs caused by antimicrobial-resistant pathogens, such as methicillin-resistant S. aureus or by Candida albicans, have been reported (Beena et al 2014, Wijesekara et al 2017). This increased proportion of SSIs caused by resistant pathogens reflects the impact of widespread use of broad-spectrum antimicrobial agents. The outbreaks have been traced to contaminated adhesive dressings, elastic bandages and colonised surgical personnel (Beena et al 2016; Feilmeier et al 2014).
Sometimes, wound covering causes problematic wound healing that could lead to serious conditions such as necrosis and infection. Wounds that are kept moist typically heal with less complications and pain than desiccated or dry wounds (Dart et al 2016). There are reports which indicate that early postoperative bath does not increase the SSIs (Toon et al 2015). However, these reports have been produced with regard to clean or minor surgeries. Therefore, the previous findings are yet to be included in the guidelines of postsurgical care, and the medical practitioners are reluctant to practice according to those findings without having solid evidence (Dinah and Adhikari 2016). The reports of keeping the surgical site open immediately after surgery without antibiotics are scanty (Harrison et al 2016).
Early postoperative bathing and keeping surgical wounds uncovered do not increase the incidence of SSI regarding clean surgeries (Dumville et al 2014; Feilmeier et al 2014). However, still the predominantly practicing protocol depends on the concept of ‘keeping the surgical wound dry and covered’ (Feilmeier et al 2014; Harrison et al 2016). The US Center for Disease Control and Prevention Guidelines for the Prevention of Surgical Site Infection, 2017 do not describe postsurgical bathing and wound covering (Berríos-Torres et al 2016). The dressing sometimes can act as a focus for infection by allowing growth of residential skin flora (Dinah et al 2016, Dumville et al 2014). Early postoperative bathing would increase early mobilisation; early discharge from the hospital can thereby reduce the nosocomial infections. Early mobilisation provides mental satisfaction and would enhance perfusion to surgical site as well as prevent postural pneumonia, deep vein thrombosis and bed sores (Gupta et al 2014; Dayton et al 2013). Here, we have assessed the postsurgical wound and other infections in clean, clean-contaminated and some contaminated surgeries after the stitched surgical incision was kept open and after the subjects had taken body bath including the surgical site after 24h of surgery.
Material and methods
This was a preliminary study. The study was conducted in crowded and busy settings at a teaching hospital in Sri Lanka. All consenting subjects with elective clean, clean contaminated and contaminated thyroidectomy, appendicectomy, breast lump excision, tendon repair and herniotomy surgeries were included, while septic patients following surgery were excluded from the study. The patients (1252 in total) who have undergone elective clean, clean contaminated and contaminated thyroidectomy, appendicectomy, breast lump excision, tendon repair and herniotomy surgeries were evaluated for SSIs. Age, sex and type of surgery including site (as thyroidectomy, appendicectomy, breast lump excision, tendon repair and herniotomy)-matched patients were allocated. In the test group, stitched surgical incisions were kept open without application of any dressing, while on the next day (24h after surgery), the patients were asked to have a full body bath as a hygienic measure by cleaning their body including the surgical site. General body soap and tap water were used for the bath. By this practice, the surgical site was kept clean and moist. In the control group, stitched surgical incisions were closed with the application of dry dressing. They were advised not to wet the surgical site and further asked to avoid bath until surgical site inspection on at days 3, 5 and 7 or prior to discharge. Patients were prepared while asking them to have a body bath day prior to the surgery. Further, surgical site body hair shaving was not done in both test and controls. Optimisation of glycaemic control and blood haemoglobin was done as preoperative preparations. All anaemics (Hb < 9g/dL) were transfused with red blood cells, and haemoglobin optimisation was done (Hb >9g/dL). According to the surgical guidelines, preoperative antibiotic prophylaxis was given (Empirical and prophylaxis use of antibiotics. National guidelines, 2016). However, during postoperative period, no antibiotics were prescribed in clean and clean/contaminated surgeries. Only in contaminated surgeries, postoperatively, antibiotic was continued for three days. Intravenous (i.v.) cefuroxime 750mg t.d.s, i.v. metronidazole 500mg t.d.s was given. The patients were followed up with monitoring body temperature, haemodynamic status, surgical site examination for any discharge or gaping, pain score and inflammatory markers (C-reactive protein (CRP) and full blood count (FBC)). Non-sedative analgesics were prescribed for complaints of pain. Control group dressing change was done at day 3 and prior to discharge. Further, all the patients were followed up after discharge and reviewed on days 7, 14 and 30 at the surgery clinic for any related complications including the signs of infection and CRP/FBC. Demography, comorbidities, clinical sign/symptoms including initial surgical condition, sign/symptoms related to surgical site and other infections and predisposing factors (lifestyle – smoking, tobacco consumption, alcohol consumption) for surgical-related infections were collected using the administered directed questionnaire by the investigators.
Statistical analysis
Statistical analysis was performed using SAS (New Jersey, 2005) (SAS® 9.1.3, 2005). Demography data were expressed in measures of central tendency. Conditional logistic regression was performed to assess the statistically significant factors (comorbidities and lifestyle) related to SSI in age, sex and surgery-matched test and controls. For the initial screening, factors with p < 0.1 was taken and further analysis was done to develop a model.
Results
Demography, comorbidities and lifestyle in the study population with regard to the type of surgery are displayed in Table 1. All included surgical morbidities other than inguinal hernia were significantly (p < 0.05) presented in middle and young aged patients. In terms of gender, male predominance was observed (p < 0.05) in all surgical morbidities except breast lump excision patients. Considering comorbidities in the study population compared to other surgical morbidities, diabetes mellitus was significant (p < 0.05) in inguinal hernia patients. Further, anaemia was significant (p < 0.05) in complicated inguinal hernia patients. Considering lifestyle, smokers were significantly high (p < 0.05) among complicated inguinal hernia patients, while alcohol consumption was significantly high (p < 0.05) in appendicitis and inguinal hernia patients.
Demography, comorbidities and lifestyle in the study population with regard to the type of surgery
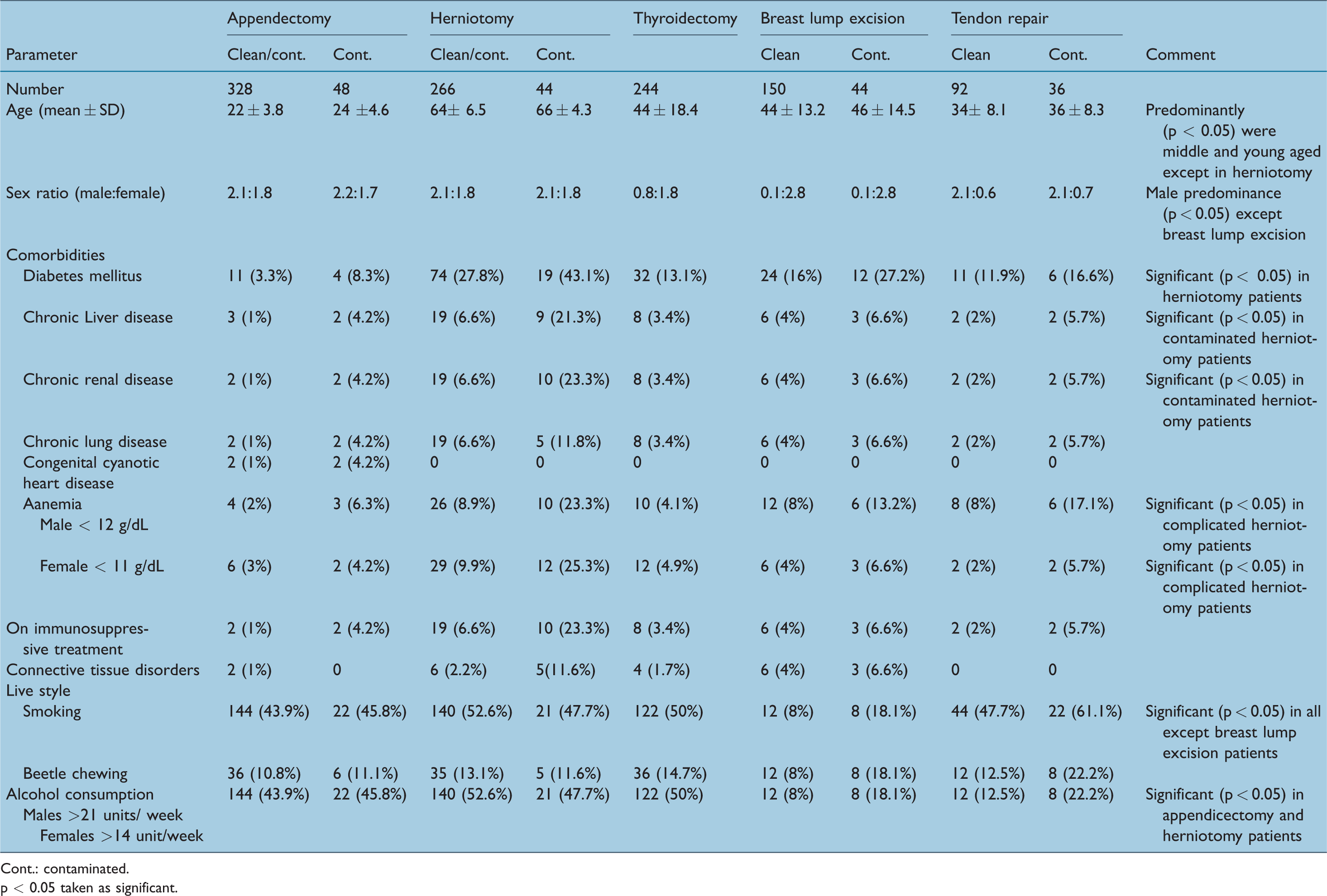
Cont.: contaminated.
p < 0.05 taken as significant.
Comparison was made between age, sex and the type of surgery -matched test and control groups in view of SSIs following day 30 postoperation and is displayed in Table 2. Compared to the test group (keeping the stitched surgical wound undressed and having a bath at 24h following surgery), in controls, SSI was significantly high in all included surgeries except thyroidectomy patients. In appendicectomy patients, clean/contaminated and contaminated categories SSI were significantly (Chi-square = 8.64 (p = 0.003); Chi-square = 8.54 (p = 0.003)) low in test groups. SSI was significantly (p < 0.05, p < 0.05) high in controls following contaminated appendicectomy (45.8%) and contaminated herniotomy (36%) surgeries. Further, postsurgical infections were significantly (p < 0.05) high following contaminated herniotomy (41%) surgeries. Urinary tract infection (54%), cannula site infection (32%) and pneumonia (22%) were predominant among contaminated herniotomy surgeries.
Comparison between age, sex and the type of surgery-matched test and control groups in view of surgical site infections up to postoperative day 30
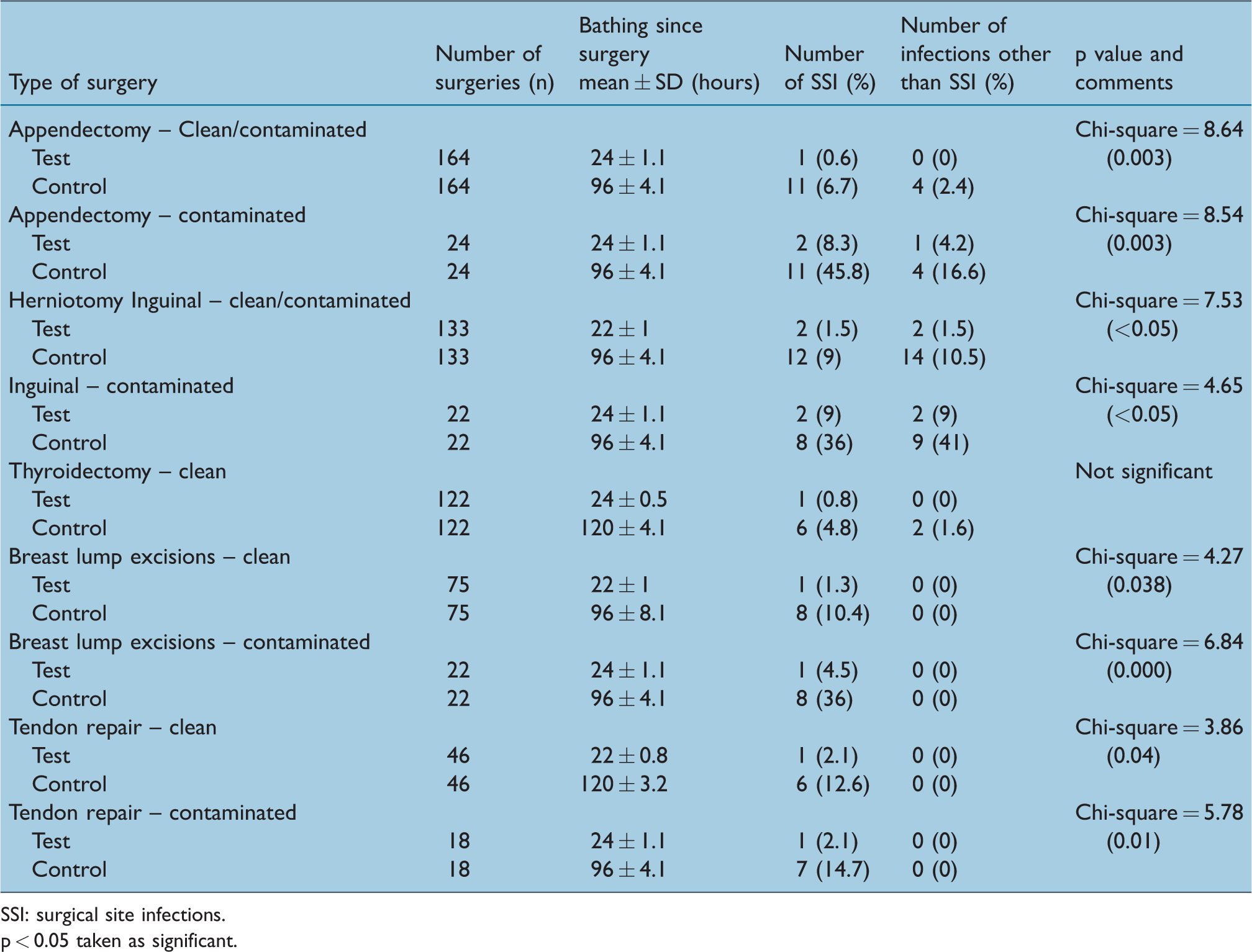
SSI: surgical site infections.
p < 0.05 taken as significant.
When considered the factors related to SSI in age, sex-matched clean/contaminated appendicectomy surgery, the SSI was significantly low in the test group (odds ratio and p value was 0.12 (p = 0.02)). SSI was significantly low in the contaminated appendicectomy surgery test group as well (odds ratio and p value was 0.14 (p = 0.02)). Also, clean/contaminated inguinal herniotomy surgery and contaminated inguinal herniotomy test groups’ SSI was significantly low (odds ratio and p value was 0.16 (p = 0.03); odds ratio and p value was 0.4 (p = 0.04)), respectively. Following clean and contaminated breast lump excision surgery, SSI in test group was significantly low (odds ratio was 0.18 (p = 0.03); odds ratio was 0.16 (p = 0.02)). Further, among clean and contaminated tendon repair surgery, SSI in test group was significantly low (odds ratio was 0.24 (p = 0.03); odds ratio was 0.32 (p = 0.04)).
In addition, in test groups following contaminated appendicectomy, clean/contaminated and contaminated herniotomies postsurgical infections other than SSI were significantly low (odds ratio was 0.33 (p = 0.02); odds ratio was 0.36 (p = 0.04); odds ratio was 0.42 (p = 0.04)).
Discussion
Among test subjects, there was no significant increase in SSI in clean, clean/contaminated and contaminated (thyroidectomy, appendicectomy, breast lump excision, tendon repair and herniotomy) surgeries. Allowing patients to bath or shower as a part of their normal daily hygiene in the early period after surgery indicated that minimal to no risk of increased SSI exists after clean surgeries (Dayton et al 2013, Feilmeier et al 2014). Proper approximation with suturing is the key to enhance the healing with low frequency of SSI (Dayton et al 2013, Gupta et al 2014). Despite these evidence, surgeons tend to follow the classic teaching of dry surgical wound care (Dinah et al 2016). A trial of 857 patients with minor skin excision surgery has been conducted to evaluate the effect of postsurgical bathing. Of those, 415 patients were instructed to remove their dressing and bath after 12h of surgery, 8.8% were found to have SSI. This percentage did not show any statistically significant difference between the other categories of patients who were instructed to avoid bathing while keeping the surgical wound dressing (Harrison et al 2016).
Another study has been conducted by Goldberg and colleagues about head or neck surgical wounds to evaluate the effect of postsurgical washing of surgical site. In their study, one group was instructed not to wet the surgical wound until the removal of the suture and the other group was instructed to wash surgical site on the next day morning after surgery. None of the 200 patients who participated in both groups developed SSIs (Dumville et al 2014). The earliest postsurgical bathing has been conducted just after 6h of surgery (Noe and Keller 1998). A study conducted by Wukish shows that showering after 12h and 48h of surgery shows a similar rate of SSI with the patients who did not shower. The percentages of SSI were 8.4% and 9%, respectively, for the showered group and the group that did not shower. However, this study was conducted with regard to simple clean surgeries involving skin and did not associate with clean-contaminated surgeries. Early postoperative bathing enhances the early mobilisation of the patient (Beena et al 2014; Ireland et al 2007). However, the studies about postsurgical bathing regarding clean contaminated or major surgeries are scanty.
Anderson and colleagues have showed that the use of sterile bandages for longer than 24 to 36h postoperatively was not necessary and using sterile bandages for longer than 36h did not reduce the number of surgical wound infections (Anderson et al 2014). Many other studies indicate that keeping wound dressing after 48h of surgery is not necessary (Harrison et al 2016). Keeping surgical wounds undressed reduces the hospital costs (Heal et al 2006).
A study of cleft lip repair surgery shows that there is no difference in the SSI rate and wound dehiscence rate between the groups that had gentamycin wound dressing and those who kept with only the initial gauze covering (Karolina 2014). Avoiding prophylaxis of antibiotics minimises the evolution of antibiotic resistance (Gbolahan et al 2009). However, still, keeping the wound covered and dry with topical application of antibiotics is the predominantly practiced protocol (Dinah et al 2016, Dumville et al 2014, Jayaweera et al 2017a, 2017b, Meir and Livne 2004). A rapid wound healing can be achieved because of sweat accumulation, applying extra pressure on the wounds causing a reduced blood supply and lack of air to the tissues is eliminated by keeping the surgical wounds open (Dumville et al 2014). Therefore, surgical wounds require facilitating the natural healing mechanisms rather than taking unnecessary precautions to prevent infections. The rate of SSIs in contaminated surgeries was quite high. This was the alarming sign to change the postoperative wound care practice in the busy and crowded surgical ward settings.
In conclusion, keeping the wounds moist and uncovered while providing a clean environment is the most suitable procedure for rapid healing of surgical wounds. In addition, early mobilisation would reduce the other associated infections in postsurgical patients. In future, with a randomised large-scale control trial for clean/contaminated and contaminated thyroidectomy, appendicectomy, breast lump excision, tendon repair, herniotomy and many other surgeries are needed to evaluate to optimize the common practices of postsurgical care.
As limitations, bio-physical quality of water which is used for body bath, needs to be assured. We have not tested the microbial content and concentration of Chlorophyll in tap water. Preventing uncovered wounds from contamination by microbial biomass which resides in faeces, urine and hospital beds is useful. Patients need to be advised to stay in a fairly clean environment following precautions. In fact, we have not advised them as such. An exact reason behind SSI among controls needs to be evaluated.
Key Phrases
Traditionally, the surgeons instruct the patients to keep the surgical incision covered, dry and to avoid wet until the sutures are removed. We have assessed the postsurgical wound and other infections in clean, clean-contaminated and some contaminated surgeries after the stitched surgical incision was kept open and after the subjects had a tap water body bath including the surgical site after 24h of surgery. When age, sex and type of surgery matched controls SSI was significantly high in clean/contaminated and contaminated appendicectomy, breast lump excision, inguinal herniotomy and tendon repair surgeries. In contaminated appendicectomy, clean/contaminated and contaminated herniotomies, postsurgical infections other than surgical site infection were significantly low in test groups. Keeping the wounds moist and uncovered while providing a clean environment is the most suitable procedure for the rapid healing of surgical wounds. In addition, early mobilisation in the test group would reduce the other associated infections in postsurgical patients.
Availability of data and material
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Declarations
Competing Interests
None declared.
Funding
None declared.
Ethics approval and consent for participation
Ethical approval was obtained from the Ethics and publication committee, Faculty of Medicine and Allied Sciences. Rajarata University of Sri Lanka, Saliyapura and informed written consent was obtained from each study participants
Contributorship
AJ, SH, JAASJ and WWK conceived and designed the experiments; AJ and SH performed the experiments; JAASJ analysed the data; JAASJ and WWK wrote the article.
Footnotes
Acknowledgements
We thank the surgical unit and all the staff members of the Teaching Hospital Karapitiya, Galle, Sri Lanka.