
Abstract
The aim of this study is to evaluate compliance and outcomes with implementation of an enhanced recovery surgical protocol in older women undergoing pelvic reconstructive surgery. This is a retrospective cohort study of women undergoing pelvic reconstructive surgery after implementation of the pathway over a 12-month period. Overall compliance was defined as a categorial variable requiring adherence to all of the selected bundle components in patients <65 years old compared to those ≥65. Intraoperative and 30-day postoperative complications were also compared and were reviewed by organ system, these were categorized using the Clavien-Dindo Classification system. There was no significant difference in overall compliance in patients <65 compared to ≥65. Factors that increased compliance in patients ≥65 include laparotomy, hysterectomy, hyperlipidaemia, time after implementation of the protocol and primary surgeon. There was an increase in compliance from 19% to 77% over the 12-month study period. Intra and postoperative complications were similar between the two groups. Enhanced recovery in older patients undergoing pelvic reconstructive surgery is feasible with similar rates of compliance and complications compared to younger patients. Compliance with the protocol increases as time after implementation of the protocol increases in all patients.
Introduction
Enhanced recovery after surgery (ERAS®) is a multi-disciplinary effort utilising a standardised protocol aimed at improving perioperative care (Kehlet and Wilmore 2008). It incorporates evidenced-based, multi-modal intervention in the preoperative, intraoperative and postoperative settings (Bardram et al 1995, Ljungqvist et al 2017). Although some institutions have adopted the ERAS® pathway in its entirety, others have modified the elements as appropriate for specific institutions, patients and surgeries (Zhuang et al 2013, Carey and Moulder 2018).
The published benefits of these pathways include increased patient satisfaction and quality of life, while reducing perioperative morbidity, cost, length of hospital stay, readmission and opioid usage in multiple surgical fields, including gynaecologic surgery (Modesitt et al 2016, Ljungqvist et al 2017). Even with guidelines in place and strong evidence of improved outcomes, implementation and compliance with an enhanced recovery pathway encounters significant barriers, especially in the early stages (Ljungqvist et al 2017, Carey and Moulder 2018). These are especially challenging in an older population (Feroci et al 2013).
Age is a risk factor for both pelvic organ prolapse (POP) and urinary incontinence (UI) (Hendrix et al 2002). Wu et al (2014) showed that the estimated lifetime risk of having surgery for either condition up to the age of 80 years is 20%. Given frequent underlying comorbidities and low physiological reserve, older patients are more likely to develop postoperative complications and have longer hospital stays after surgical procedures (Turrentine et al 2006). Therefore, it is especially important to tailor perioperative management to these patients. There is evidence in the surgical literature that patients >70 years of age have similar postoperative complication rates, length of hospitalisation and readmission rates when placed on enhanced recovery protocols compared to younger patients, with similar rates of compliance (Jeong et al 2016). There is limited evidence in the female pelvic reconstructive literature evaluating compliance with enhanced recovery protocols among older patients. The aim of this study is to analyse compliance with an enhanced recovery surgical pathway in older women undergoing pelvic reconstructive surgery over the course of implementation based on adherence to the bundle set in place. We hypothesised that older patients would have a lower compliance rate compared to younger patients.
Materials and methods
This is a retrospective cohort of female patients undergoing pelvic reconstructive surgery by the four members of the division of Female Pelvic Medicine and Reconstructive Surgery (FPMRS) on the gynaecologic surgery enhanced recovery pathway at an academic institution from 1 February 2018 to 31 January 2019. The date of 1 February 2018 was chosen as it marked one month after the official implementation of the enhanced recovery pathway, thereby allowing for dissemination and distribution of pathway information throughout the departments of Obstetrics and Gynecology and Anesthesiology. Patients were flagged preoperatively for eligibility on the enhanced recovery pathway based on CPT codes which include all laparotomies, hysterectomies and complex pelvic reconstructive procedures (Supplementary Table 1). Patient data are stored in a REDcap (Research Electronic Data Capture) electronic database hosted at our institution of all patients ≥18 years of age who were identified to be on the enhanced recovery pathway (Harris et al 2009, 2019). Exclusion criteria include patients <18 years old, cancer as indication for surgery, combined cases where a FPMRS faculty member is not the primary surgeon, and unplanned surgery. The data were collected prospectively from the electronic medical record (EMR) throughout implementation to track compliance and outcomes in real time for quality improvement purposes. REDCap is a secure, web-based software platform designed to support data capture for research studies, providing (1) an intuitive interface for validated data capture; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for data integration and interoperability with external sources.
Patient demographics and perioperative variables were collected from the EMR. The Charlson comorbidity index (CCI) score was used to stratify patient’s general health status based on their 10-year mortality (Charlson et al 1987). Patients were divided into two groups: those <65 years old and those ≥65. The primary outcome was overall compliance with the complete bundle in patients <65 years old compared to those ≥65. Secondary outcomes include compliance with separate bundle components, factors related to increased compliance in older patients, and perioperative complications. Overall compliance was defined as a categorial variable requiring adherence to all of the selected bundle components. Bundle components included in the primary analysis were preoperative education (nursing visit or phone call), carbohydrate load (both the night prior to surgery and morning of surgery), infection prevention with preoperative cleansing wipes for those undergoing abdominal procedures (both the night prior to surgery and morning of surgery) and appropriate antibiotics and dosing (as well as redosing if necessary), preoperative oral pain medications including acetaminophen and gabapentin, use of appropriate venous thromboembolism prophylaxis, and use of intraoperative multimodal neuraxial anaesthesia (lidocaine and/or ketamine drip) (Figure 1). All components listed above had to be complete to be considered compliant with the overall bundle. Though other components presented in Figure 1 were part of our enhanced recovery pathway, they were not selected for analysis as they were considered part of our standard perioperative care prior to initiation of the enhanced recovery pathway. Postoperative multimodal and neuraxial anaesthesia (lidocaine drip, epidural) were included in the analysis as they are also part of the enhanced recovery bundle, but were not considered necessary for the completion of the entire bundle. Intraoperative and 30-day postoperative complications were reviewed by organ system and also included blood transfusion, surgical site infection (SSI), venous thromboembolism (VTE), ambulatory surgical patients converted to inpatient stay, reoperation, readmission and mortality. Any postoperative complications in the 30 days following surgery were categorised using the Clavien-Dindo Classification system (Dindo et al 2004).
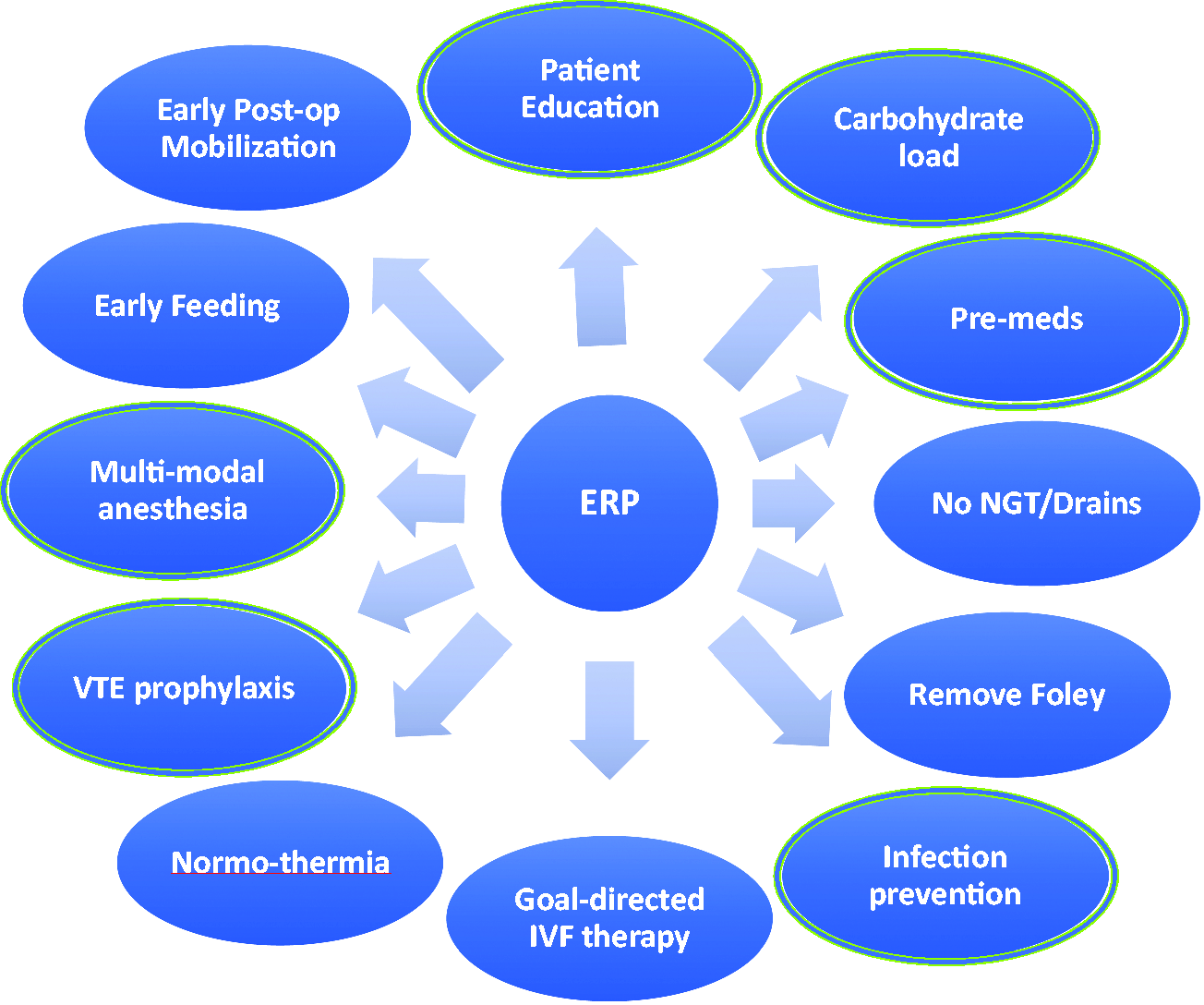
Components of enhanced recovery pathway. Those circled were included in the primary analysis. ERP: enhanced recovery pathway; VTE: venous thromboembolism.
Descriptive statistics were used to summarise demographic, clinical and surgical characteristics. Data are represented as number of patients in each category grouped by age (<65 or ≥65 years old) with percentages. Mean and standard deviations or median with inter-quartile range are presented where appropriate. Wilcoxon rank-sum and Fischer’s exact test were used to compare continuous and categorical data respectively. A univariate and multivariate logistic regression was used to model the logit of the probability of compliance. A saturated model including all factors with a p ≤ 0.20 was built and backward elimination used in a multivariate analysis to construct a parsimonious model, removing factors one at a time until all remaining factors remained statistically significant. Factors included in the regression included demographic and intraoperative characteristics. Findings were considered statistically significant when the p-value was less than 0.05. Analysis was performed using STATA™ 15.1 for Macintosh (StatCorp LP, College Station, TX). Approval for this study was obtained from the Institutional Review Board (IRB#180953).
Results
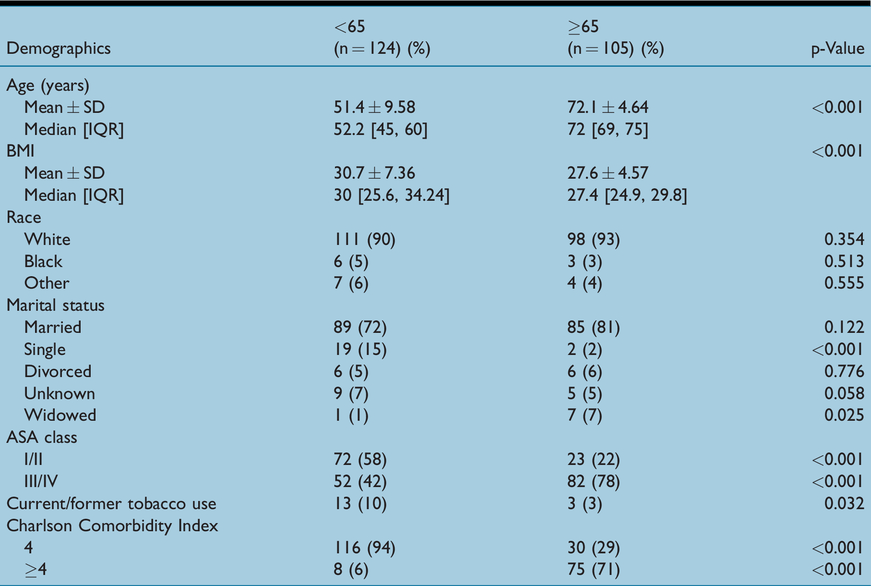
A total of 229 patients met our criteria for inclusion criteria into the study; 124 patients in the <65-year-old group and 105 in the ≥65-year-old group. The <65 group had a higher BMI (30 vs. 27; p < 0.001), single marital status (15% vs. 2%; p < 0.001), and was more likely to be a current or former smoker (10% vs. 3%; p = 0.03) (Table 1). The ≥65 group had higher ASA class (ASA III/IV: 42% vs. 78%; p < 0.001), were more likely to be widowed (1% vs. 7%; p = 0.025), and had higher CCI score (≥4: 6% vs. 71%; p < 0.001). No other significant differences in baseline characteristics were found.
Demographics and preoperative characteristics.
Intraoperative variables were similar between the two groups for timing of the case, surgical time, wound classification, surgical approach and length of stay (Table 2). Patients in the <65 group had higher rates of hysterectomy (p < 0.011) and uterosacral suspension (p = 0.008), but lower rates of colpocleisis (p = 0.001). Estimated blood loss was higher in the <65 group (150mL vs. 100mL; p < 0.001).
Intraoperative variables.
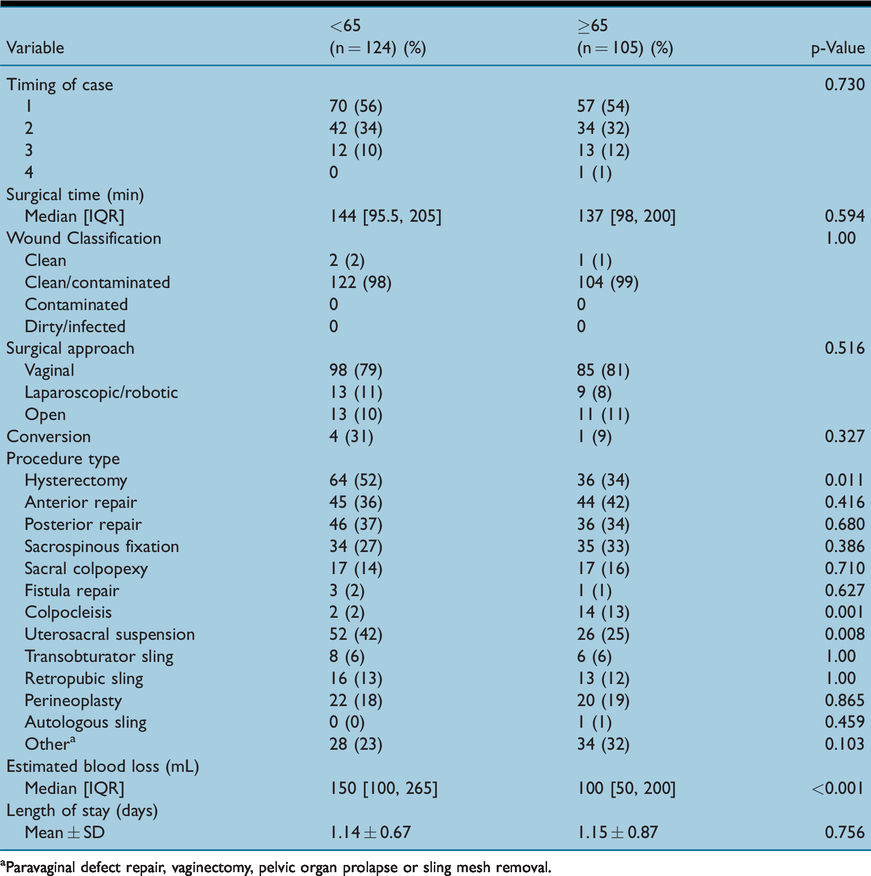
aParavaginal defect repair, vaginectomy, pelvic organ prolapse or sling mesh removal.
Regarding the primary outcome, overall compliance with the complete bundle was 52% for all patients. Among all patients, there was a significant increase in complete bundle compliance between the first six months of the study period and the latter six months (37% vs. 63%; p < 0.001) (Figure 2). Overall compliance with the bundle did not differ between the two age groups (53% vs. 50%, OR 0.89, 95% CI 0.53, 1.51). Use of preoperative cleansing wipes was higher in patients ≥65 both at home and in the hospital prior to surgery. Gabapentin administration prior to surgery was higher in patients. There were no other statistically significant differences between the groups for any other separate bundle components (Table 3).
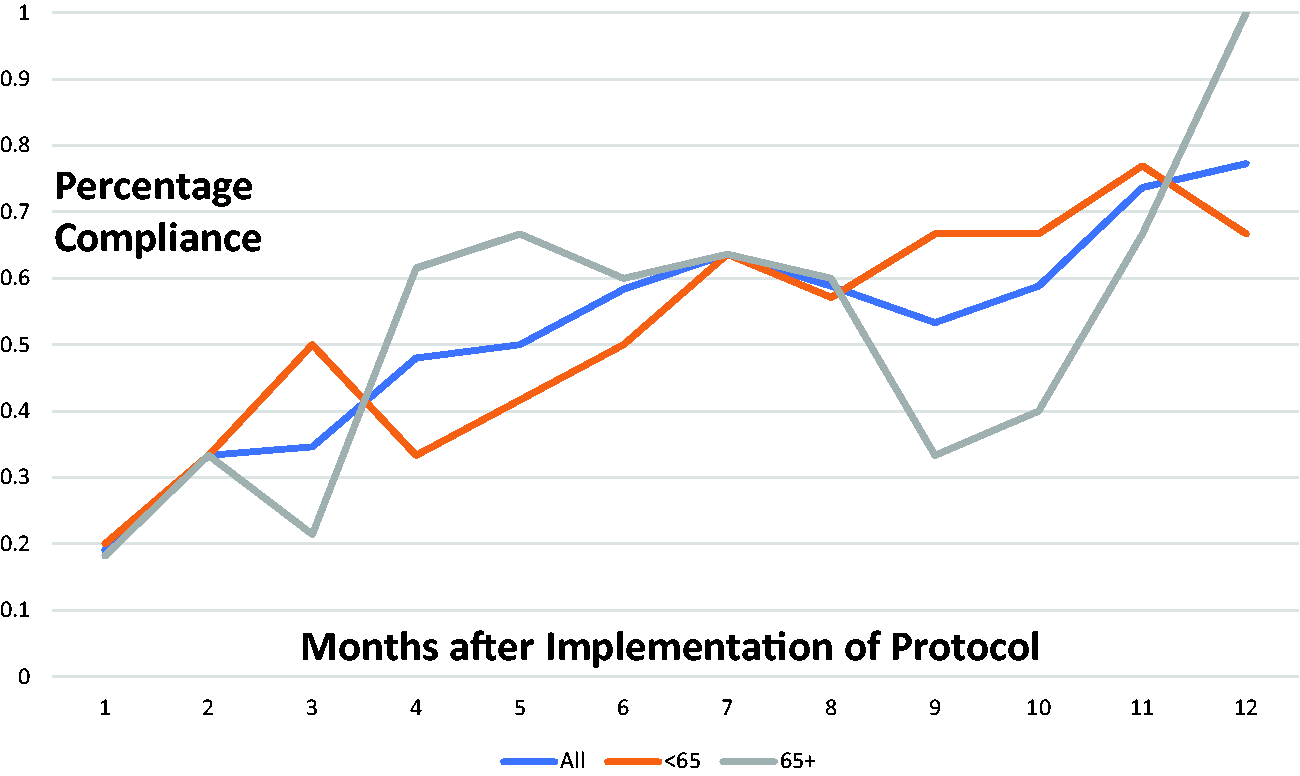
Compliance with overall bundle by month after implementation of protocol. All patients had an increase in compliance over time. There was no significant difference in compliance between age groups over time.
Compliance with enhanced recovery protocol.
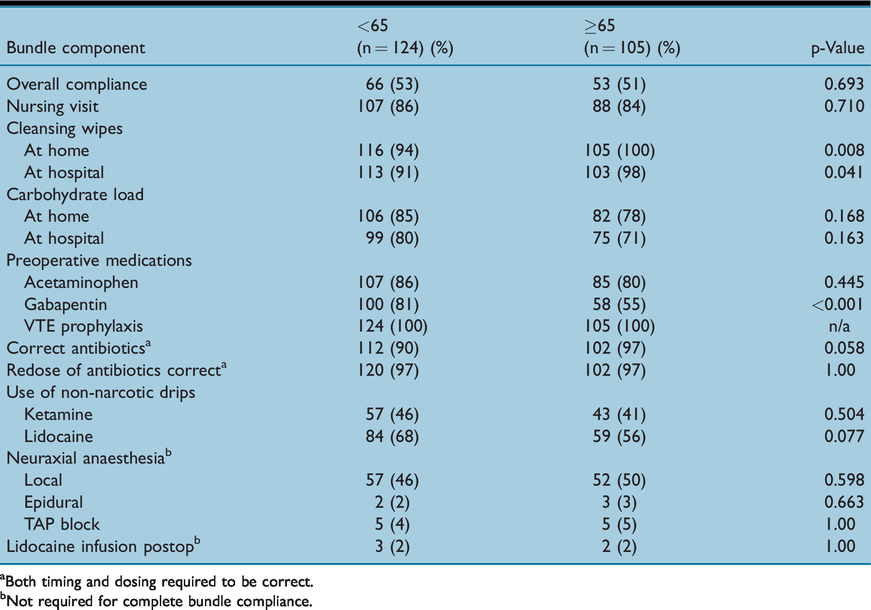
aBoth timing and dosing required to be correct.
bNot required for complete bundle compliance.
In the multivariate logistic regression model after controlling for demographic and surgical characteristics, factors associated with compliance in the older group were hyperlipidaemia (OR 1.88, CI 1.00, 3.53), laparotomy (OR 3.54, CI 1.26, 9.98), hysterectomy (OR 2.18, CI 1.19, 4.03), primary surgeon (OR 2.70, CI 1.14, 6.42) and date of surgery further from enhanced recovery implementation (OR 3.02, CI 1.71, 5.33).
Intraoperative complications were similar between the two groups (6% vs. 1%; p = 0.073) (Table 4). In the <65 group there were three patients requiring blood transfusion, four patients requiring conversion from minimally invasive procedure to exploratory laparotomy due to uncontrolled bleeding, two cystotomies and one retropubic midurethral sling bladder perforation. For patients ≥65, there was one cystotomy. Total postoperative complications were similar between the two groups (18% vs. 26%; p = 0.150). When Clavien-Dindo Classification was applied there was no difference between the two groups. There were more cardiovascular (0% vs. 4%; p = 0.043) and genitourinary (4% vs. 18%; p < 0.001) complications in the ≥65 group. The cardiovascular complications included one arrhythmia, one myocardial infarction, a case of hypertensive crisis and one case hypotension requiring medical intervention. The genitourinary complications included one case of acute kidney injury and 18 urinary tract infections. There were more patients who required admission (two-night stay) to the hospital after initially being scheduled as an ambulatory surgical patient (one-night stay) in the <65 group (8% vs. 1%; p = 0.012). Reasons for admission included conversion to laparotomy (four), fever with subsequent negative work up (two), dizziness (two), hypotension (one) and one patient who had to stay for social reasons. One patient was admitted for an inpatient stay in the ≥65 group for postoperative hypotension requiring medical intervention. In the <65, there were five postoperative urinary tract infections. Two patients required postoperative blood transfusion and five patients had surgical site infections (one superficial, two deep and two organ space). There were no wound disruptions, respiratory, cardiovascular or nervous system complications. There were three cases of ileus and one case of nausea and vomiting that required an overnight stay in the hospital. There was one case of hyperglycaemia (four values >200mg/dL). There were eight readmissions, for three hematomas, two pelvic abscesses, two ileus and one for pain requiring return to the OR and removal of a uterosacral suture. Three other patients required return to the operating room (four in total) all for drainage of pelvic abscesses/hematomas. There were no VTE or mortalities in either group.
Intraoperative and postoperative complications.
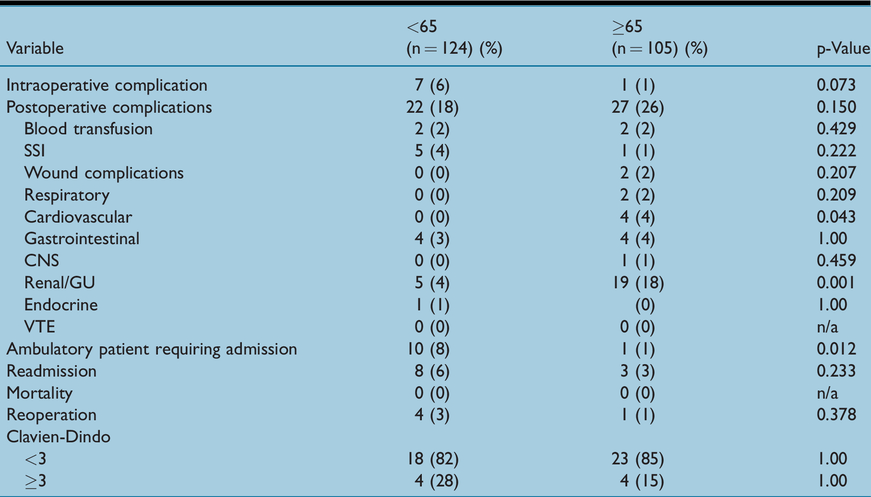
In women ≥65, two patients required postoperative blood transfusions and there was one superficial surgical site infection. There were two wound complications, one superficial separation that did not require surgery and one dehiscence that required emergent return to the operating room. This was the only reoperation in the older patient group. This patient also had a postoperative pneumothorax. There was one neurological complication involving right leg pain that resolved with physical therapy. There were three readmissions for a pneumonia, wound dehiscence (as above) and small bowel obstruction. Gastrointestinal complications included constipation requiring digital disimpaction, small bowel obstruction treated conservatively, nausea and vomiting requiring an extra night in the hospital, and outpatient nausea and vomiting requiring ED observation at an outside hospital. There were no endocrine complications in this group.
There was no difference in mean length of stay (days) between the two groups (1.14 ± 0.67 and 1.15 ± 0.87; p = 0.756).
Discussion
Our results show that an enhanced recovery surgical protocol is feasible in an older population, with similar rates in compliance compared to a younger population in women undergoing pelvic reconstructive surgery.
There is a large body of evidence from outside the gynaecologic literature that compliance with enhanced recovery guidelines is important for achieving improved outcomes (Pisarska et al 2019, Gianotti et al 2019). de Nonneville et al (2018) showed within gynaecologic oncology that enhanced recovery after surgery is feasible and safe in older patients. While there have been studies on the benefits of a specific enhanced recovery pathway for female pelvic reconstructive surgery, there are limited data in the regarding compliance with such pathways (Carter-Brooks et al 2018).
It has been shown in gynaecologic oncology that active structured implementation of an enhanced recovery protocol is necessary, even in hospitals where enhanced recovery protocols are already established in other surgical departments (de Groot et al 2014). At our institution enhanced recovery protocols have been used for many years in other departments such as colorectal surgery. Our enhanced recovery perioperative team had several members who were already involved with enhanced recovery in other departments. Even with their guidance, our overall compliance with the protocol was lower than anticipated in both groups. However, rates of overall compliance improved from the first six months of the study to the latter six months in all patients. This is consistent with previous reports (Lohsiriwat 2019). Lohsiriwat showed that 76 colorectal operations were required for a multidisciplinary team to achieve a significantly higher rate of optimal recovery and high compliance with enhanced recovery programs for colorectal surgery. The improvement at our institution is likely due to intramural education with staff and providers in the outpatient setting as well as in the hospital. Scheduled meetings were held to track our compliance and review the protocol with team members. This likely contributed to our increased compliance over time.
We found several factors that increased compliance in the older patient group including: laparotomy, hysterectomy, hyperlipidaemia, primary surgeon and time of surgery further from implementation. While it is likely that a history of hyperlipidaemia’s effect on compliance rates is spurious, laparotomy and hysterectomy were likely easier for team members and staff to recognise as more complex surgeries, therefore requiring placement on the enhanced recovery pathway. Recognition of patients on the enhanced recovery pathway was aided by our prospective data collection and monthly assessment of compliance and outcomes. Our dedicated enhanced recovery perioperative team was comprised of attending physicians, staff, nurses and trainees who met monthly in order to discuss and resolve any issues relating to dissemination of the protocol throughout the perioperative process. Patient education also plays a role in compliance and has improved over time through outpatient nursing education and the development of standardised instructions given preoperatively. The primary surgeon likely played a role, as those surgeons who were involved in the implementation of the pathway would be more likely to be certain patients were compliant.
Strict criteria were used in the evaluation of compliance with the entire bundle, which may contribute to the lower documented success rates. The higher rate of gabapentin administration to patients <65 is likely related to an item in the protocol that states a lower dose may be considered in patients >65 (100mg vs. standard 300mg) or may be omitted in patients >75 years old. However, we considered this when evaluating compliance with gabapentin administration in our analysis.
Since there was no difference in overall intraoperative or postoperative complications between the two groups, the enhanced recovery pathway appears to be safe, even in older patients with a higher CCI score. This is consistent with the literature (Jeong et al 2016, de Nonneville et al 2018).
Our study is limited by its retrospective nature and the limitations regarding accurate data collection from the electronic medical record. Nonetheless, our data were collected in a prospective fashion on a month by month basis and checked for accuracy and consistency in order to improve compliance with the protocol and monitor outcomes, therefore bias should be limited. It is susceptible to reporting bias as the information recorded was obtained from each provider’s documentation in the EMR. Our study is a population of women undergoing pelvic reconstructive procedures, most commonly for pelvic organ prolapse, and therefore may not be generalisable to all benign gynaecologic surgery or gynaecologic oncology patients. Further study with a larger number of women and more varied preoperative indications for surgery would likely be more generalisable and is an area marked for further research by our group.
The strengths of our study include a large volume of FPMRS patients over a year of implementation. Prospective data collection and analysis allowed for rigorous data review, which should eliminate errors. There was a variety of surgical case types, surgeons and approaches which helps in the generalisability among pelvic floor reconstruction.
Overall, our study shows that enhanced recovery protocols in older, more medically complex patients is both possible and safe with similar compliance and complication rates compared to a younger cohort. Additionally, compliance with gynaecologic surgery enhanced recovery protocols increases from time of implementation in all patients, regardless of age.
No competing interests declared
Footnotes
Acknowledgments
The entire enhanced recovery team including faculty physicians in the departments of Obstetrics and Gynecology and Anesthesia, administrators, perioperative nursing, fellows and residents should be acknowledged for their help in implementation of the protocol.
ORCID iDs
Joseph Panza https://orcid.org/0000-0003-2870-0773 Laura Sorabella ![]()