
Abstract
A nationwide survey describing Swedish post-anaesthesia care units (PACUs), n = 75 was undertaken. The patients most commonly cared for at PACUs were patients who had undergone laparoscopic surgery, 69.3%, followed by patients who had undergone minor orthopaedic surgery, 68%. At the majority of the PACUs, 86.7%, the staff cared for emergency surgery patients and 48% for day surgery patients. In 31% of the PACUs, a pain relief service was offered through a specific pain service team. During the daytime, the anaesthetist in charge most frequently worked in the operating room 42.7%, and on call in the intensive care unit, 37.3% of the time. In 88% of the PACUs, either all or most registered nurses had a specialist education at an advanced level. The most frequent ratio of registered nurses to patients was 1 to 4, 37.3%. However, Swedish PACUS are also staffed by assistant nurses and the most frequent ratio of registered nurse to assistant nurse was 1:1. Thirty-three (44%) of the PACUs had access to a physiotherapist during the daytime. Almost all PACUs (93.3%) had predetermined discharge criteria but in the majority of PACUs' high-risk patients (68%) were not followed up by an anaesthetist after discharge from the PACU.
Keywords
Introduction
Shortly after the first anaesthesia was administered during surgery in 1846, Florence Nightingale recognised the need for special nursing care for patients recovering from surgery and the use of ether anaesthesia (Hatfield 2014, Odom-Forren & Drain 2008). The first post-anaesthesia care unit (PACU) was established in the USA in 1923 and the subsequent widespread use of anaesthesia care units has been attributed by some to a reduction in postoperative morbidity and mortality (Odom-Forren & Drain 2008, Waddle et al 1998). A modern PACU must be flexible, serve all types of patient with acuity and be of high quality (Odom-Forren & Drain 2008). The PACU should be staffed by registered nurses (RN) who aim to provide nurse-led, protocol-driven care for up to 24 hours postoperatively, including Phase I and II (Apfelbaum et al 2013, Australian 2018, Odom-Forren & Drain 2008, Simpson & Moonesinghe 2013, Vimlati et al 2009, Whitaker et al 2013). Patients generally require constant vigilance and observation and different variables are evaluated at PACUs with regard to obtaining and developing quality care, including monitoring of patient outcome measures, adverse events, medical interventions and nursing care (Australian 2018, Checketts et al 2016, Nilsson et al 2020, Whitaker et al 2013).
It is difficult to predict PACU staffing needs because of the marked variation in patient numbers and acuity over the course of just a few hours (Dexter 2007) with an indication of 1:1, 1:2 or 1:3 (maximum recommendation) nurse to patient ratios (Clifford 2018). All patients should also be the joint responsibility of the surgical team and either an intensivist or anaesthetist (Australian 2018, Simpson & Moonesinghe 2013, Vimlati et al 2009, Whitaker et al 2013).
By providing postoperative care with continuous evaluation and specialised care, PACUs can contribute to reducing healthcare expenses through early detection of signs of postoperative complications, thereby preventing them (Nilsson et al 2020). Procedures and competence in the early detection of signs of deterioration from the expected course are of crucial importance to the prevention of serious adverse events through early diagnosis and measures and by following the concept of failure to rescue (Apfelbaum et al 2013, Odom-Forren & Drain 2008, Vimlati et al 2009, Whitaker et al 2013). Optimising the overall postoperative care of the patient requires a multi-professional approach (Nilsson et al 2020) in which postoperative monitoring and continuous patient support are of great value to patient safety and satisfaction (Apfelbaum et al 2013, Australian 2018, Checketts et al 2016, Merry et al 2010, Odom-Forren 2012, Odom-Forren & Drain 2008, Ringvold et al 2018, Vimlati et al 2009, Whitaker et al 2013). A systematically implemented multimodal model for optimising patients for early mobilisation, return of autonomy and normal physiology (Nilsson et al 2020, Simpson & Moonesinghe 2013) such as Enhanced Recovery After Surgery (ERAS) (Ljungqvist et al 2017) should be used to reduce quality variation, prevent complications and provide shorter length of stay and lower costs (Simpson & Moonesinghe 2013).
It is hard to identify studies that present how PACUs and procedures in clinical practice are organised, although some international guidelines are available (Apfelbaum et al 2013, Checketts et al 2016, Whitaker et al 2013). At the time of the present survey, no Swedish guidelines were available. Thus, the present survey was conducted in order to compile such guidelines and to identify areas of clinical practice that need to be improved.
The aim of this nationwide survey was to describe PACU services in Sweden in 2017 – including their clinical commitment and how they are organised, equipped and staffed, as well as describe general procedures for communication and patient follow-up.
Methods
This was a descriptive national survey. From September to December 2017, a study-specific web-based questionnaire on postoperative care procedures was sent to 67 Swedish hospitals with one or more PACU units. The units were identified by the Swedish Society of Anaesthesia and Intensive Care (SFAI). The anaesthetist responsible for the PACU was asked to complete the questionnaire. Written reminders were sent three times to non-responders.
The questionnaire was designed for the purpose of the study and was based on consensus discussion among the first four authors. The questions addressed the following issues: (I) organisation and service; (II) monitoring equipment; (III) staffing and (IV) documentation and discharge criteria. The questions were multiple choices or open ended.
Example of questions:
Number of specialist nurses: All; a majority; a minority; none. How are handovers carried out? Structured handover with S-BAR, for example; no specific form of handover. Duration of stay at the PACU: <24 hours; 24 hours; 48 hours; ≥48 hours
Ethical considerations
According to the Swedish Act on the Ethical Review of Research, formal ethical approval was not required for this study because the responses to this survey did not include any sensitive information about patients.
Statistical analysis
Data were entered and analysed using descriptive statistics computed in the Statistical Package for the Social Sciences (SPSS version 25). Descriptive statistics were computed for all variables and were described using means, frequencies and percentages.
Results
The overall response rate was 65.7%, representing 44 of the 67 included hospitals. The questions were answered by 75 respondents who represented specific PACUs.
Organisation and service
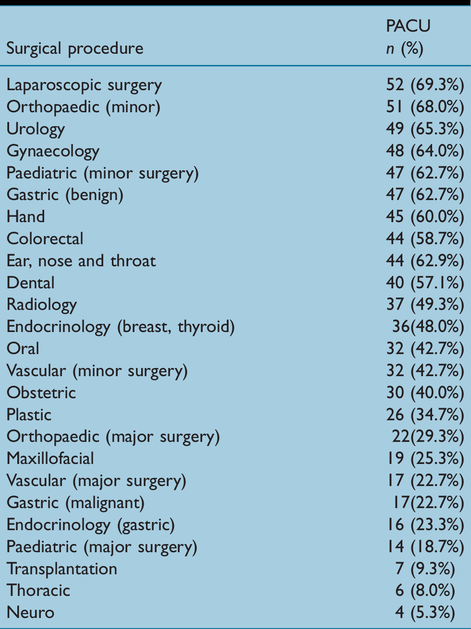
The hospitals had an average of 2.7 (range 1–7) PACU units and 8.8 (range 1–34) operating rooms. The PACUs were organisationally affiliated to the departments of anaesthesia, 30.7% (n = 23), intensive care, 28% (n = 21), surgery, 6.8% (n = 5), to a combination of anaesthesia/intensive care/surgery, 6.8% (n = 5) or were independent units not affiliated with another department, 28% (n = 21). The patients most commonly cared for at PACUs were patients who had undergone laparoscopic surgery, 69.3% (n = 51), followed by minor orthopaedic surgery, 68% (n = 51). The least common patients were patients who had undergone neurosurgery, 5.3% (n = 4) (Table 1).
Surgical procedures and the number and percentage of PACUs take taking care of patients undergoing these types of surgeries.
The most common opening hours were 24 hours per week, 36% (n = 27), followed by day and evenings on weekdays, 28% (n = 21), daytime on weekdays, 17.3% (n = 13), 24 hours on weekdays, 13.3% (n = 10) and days and evenings all week, 5.3% (n = 4). At the majority of PACUs, 86.7% (n = 65), the staff cared for emergency surgery patients and in 48% (n = 36) of the PACUs, the staff cared for day surgery patients. Thirty-one (31%) of the PACUs offered pain service by a specific pain service team.
In approximately 60% (n = 44) of PACUs, the average length of patient stay was less than 24 hours, followed by 24–48 hours, 28% (n = 21) and ≥48 hours, 13% (n = 10). Only six of the PACUs had access to isolation rooms. The most common bed space was 2 × 3m, 61% (n = 46), followed by 3 × 3m, 20% (n = 15), 3 × 4m, 11% (n = 8) and ≥4 × 4m, 8% (n = 6).
Monitoring equipment
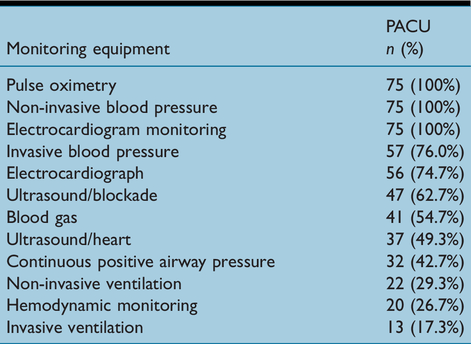
All PACUs were equipped with a pulse oximeter, non-invasive blood pressure monitors and an electrocardiogram (ECG), followed by invasive blood pressure monitors, 76.0% (n = 57) and diagnostic ECG, 74.7% (n = 56). The least common monitoring equipment was invasive ventilation, 17.3% (n = 13) (Table 2).
Numbers and proportions of monitoring equipment.
Staffing at PACUs
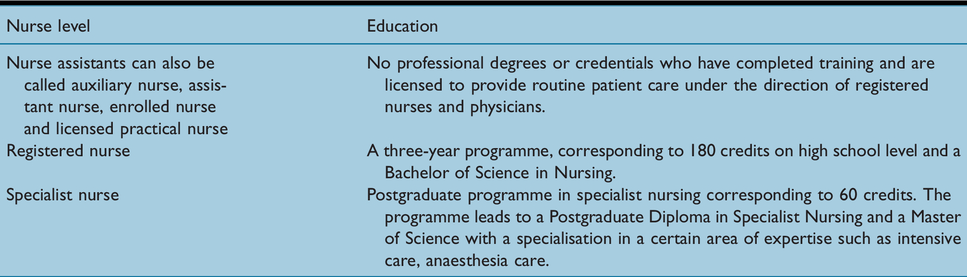
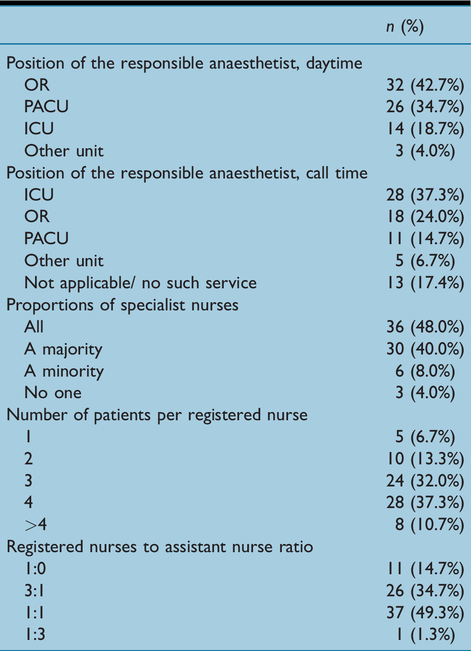
During the daytime, the anaesthetist in charge most frequently worked in the operating room (OR), 42.7% (n = 32) and on call time in the intensive care unit (ICU), 37.3% (n = 28). In 88% of the PACUs, either all or most registered nurses had a specialist education at an advanced level (Table 3, descriptions of range of nurse levels of education in Sweden). The most frequent ratio of RN to patients was 1 to 4, 37.3% (n = 28) and almost one half, 49.3% (n = 37) of PACUs had a 1 to 1 ratio of RN and assistant nurses (Table 4). Thirty-three, 44%, of PACUs had access to a physiotherapist during the daytime.
Descriptions of range of nurse levels of education in Sweden.
Staffing at PACUs.
Documentation and discharge criteria
A structured handover between staff was used in 85.3% (n = 64) of the PACUs when transferring a patient from the OR to the PACU and in 78.7% of the PACUs (n = 59) when transferring the patient to a general ward. In the majority of the PACUs, high-risk patients were not followed up by an anaesthetist after discharge from the PACU, 68.0% (n = 51). In the remaining PACUs (n = 24), the anaesthetist did not follow-up all patients, only specifically high-risk patients.
In 93.3% (n = 70) of the PACUs, predetermined discharge criteria were used by the staff. In the majority of the PACUs, 48% (n = 36), the RN used a combination of electronic and paper documentation in their medical records. Paper documentation only was used in 24% (n = 18) and electronic documentation only was used in 28% (n = 21).
Discussion
The aim of the present study was to gain insight into how Swedish PACUs are organised, equipped and staffed, as well as insight into general procedures for communication and patient follow-up.
In Sweden, an anaesthetist is responsible for care at a PACU. This is in line with the majority of PACUs in Europe (Vimlati et al 2009, Whitaker et al 2013). Within PACU, nurses are trained to take key responsibility for monitoring patient progress and for ensuring that an adequate management plan on the general ward is in place prior to discharge from the PACU (Odom-Forren & Drain 2008, Street et al 2017, Vimlati et al 2009). In the present study, we did not ask about the nurses’ type of specialisation. In Sweden, no specific specialisation for postanaesthetic/postoperative care is available. This is a limitation of the present study that should be addressed in future work. Our clinical experience is that the most common types of specialisation of nurses working at PACUs are nurse anaesthetists and intensive care nurses.
In the present study, we found that the most frequent ratio of registered nurses to patients was 1:4, 37.3%. Nurse to patient ratios of 1:1, 1:2 or 1:3 (maximum recommendation) have been proposed (Clifford 2018). However, 52% of Swedish PACUs had ratios of 1:1, 1:2 or 1:3 and were also staffed by assistant nurses, with the most frequent ratio of RN to assistant nurse of 1:1. As well as in most Swedish PACUs, there is a combination of both Phase I and Phase II patients. However, the staffing matrix should be flexible as the volume of patients changes, as well as the acuity of patients arriving at the unit (Clifford 2018, Dexter 2007, Luckowski 2019). Furthermore, excessive pain is a common issue and requires a relatively high amount of nursing care, particularly when combined with agitation (Cohen et al 1999). Also, high patient-to-nurse ratios in the general ward expose surgical patients to a high risk of mortality (Aiken et al 2002). In contrast, combining the minimum required number of nurses with a smooth patient transition from the OR to the PACU and the surgical ward is important for hospital managers, considering that personnel salaries account for the greatest expense of running a PACU (Kiekkas & Aretha 2018). Nevertheless, nurses are an obvious resource in a PACU with the goal of optimising cost-effectiveness by improving the use of limited resources without jeopardising patient safety (Clifford 2018). Even so, there is no international consensus regarding the education of the nurse working in the PACU.
In almost all PACUs (93.3%), the staff used predetermined discharge criteria. Recent studies have shown that the discharge criteria based on a predetermined physiological scoring system can reduce the length of stay in the PACU (Jain et al 2018, Street et al 2017, 2018) and is cost-effective (Street et al 2017). Furthermore, this method increases patient safety by identifying patients at a greater risk of adverse events, thereby decreasing the rate of clinical deterioration and cardiac events following discharge from the PACU (Nilsson et al 2020, Street et al 2017). Approximately 60% of PACUs had an average length of patient stay of less than 24 hours. However, we did not ask for a more accurate time frame than <24 hours although the length of stay for most patients at Swedish PACUs is 1–3 hours, depending on the surgical procedure, anaesthesia, age and comorbidities. It has been reported that the length of stay is not only affected by the duration of surgery (Weissman et al 2019), but also surgical procedure, anaesthesia, age and comorbidities, as well as the time of day and whether it is at the weekend (Mann-Farrar et al 2019).
In the present study, a structured handover was used by the staff in 85.3% of the PACUs when transferring the patient from the OR to the PACU and in 78.7% of the PACUs when transferring the patient to the general ward. Van Rensen et al (2012) observed that simultaneous transfer of patient information and equipment during patient handover is common in PACUs and that the handover of information often takes place in combination with a multitude of other activities. However, Street et al (2017) found that the post-anaesthetic care tool can assess readiness for discharge, thereby improving clinical care and reducing adverse events.
Early postoperative mobilisation is essential for rapid functional recovery after surgery. However, less than one half of the PACUs in the present study had access to a physiotherapist. According to the ERAS program, patients undergoing major surgery should be actively mobilised on the day of surgery whenever feasible and encouraged to meet daily mobilisation targets (Ljungqvist et al 2017). Early mobilisation can be performed even if no physiotherapist is present, although PACU staff must still be competent in it. It is therefore recommended that all PACUs have a physiotherapist present during the daytime. It is believed that successful postoperative care is best achieved by a coordinated and integrated multidisciplinary team, comprising surgeons, anaesthetists, nurses, physiotherapists and other clinicians. Such team-based care should be embedded in a clinical care pathway, such as the ERAS program, which focuses on enhancing patient recovery (Nilsson et al 2020).
This study has a number of limitations. First, the response rate was low, although the sample included PACUs that were representative of different sized hospitals and of different regions in Sweden. No analysis of the differences between the different PACUs were conducted because the sample size was small, and it was difficult to differentiate between the type and size of each PACU. The questionnaire was not psychometrically evaluated but was developed by four anaesthetists with many years’ experience of working in a PACU – and the questions related to clinical practice.
In conclusion, to our knowledge, this is the first nationwide survey to describe a country’s PACU services. In Sweden, the procedures, equipment, staffing and organisation of PACUs would appear to follow international recommendations. There are also areas that need to be improved, such as the frequency of following up high-risk patients by an anaesthetist after discharge, as well as access to a physiotherapist during the daytime. Further international studies are needed in order to describe and compare how other countries have organised, equipped and staffed their PACU. But also studies to identify the safest, best quality and most cost-effective PACU service.
No competing interests declared.