
Abstract
Myocardial injury after non-cardiac surgery is common and defined as myocardial ischaemia within 30 days after non-cardiac surgery. Diagnosis of myocardial injury after non-cardiac surgery is challenging as this could be clinically asymptomatic during the postoperative period due to many other factors. Role of high-sensitive cardiac troponin in diagnosing myocardial injury after non-cardiac surgery had been evaluated in several studies. Due to the fact that high-sensitive cardiac troponin remains positive for about two weeks in the body and is highly specific in diagnosing clinically silent myocardial injuries, it is recognised as the most useful biomarker in detecting myocardial injury after non-cardiac surgery. However, high-sensitive cardiac troponin is not well incorporated as a biomarker in current major perioperative guidelines or in clinical practice. The aim of this review is to discuss evidence and guidelines in this area in view of the use of high-sensitive cardiac troponin in early identification of myocardial injury after non-cardiac surgery.
Keywords
Introduction
From 2011 to 2012, 662,000 patients have undergone elective surgeries in Australian public hospitals. Out of those surgeries, more than 80% were non-cardiac procedures (Statistics AH 2012). Patients who undergo non-cardiac procedures carry an increased risk of major cardiovascular complications, including acute myocardial infarction (MI), heart failure, arrhythmia or stroke (Smilowitz et al 2017). Amongst postoperative complications, MI is the most common, with an associated increased risk of 30-day mortality (Devereaux et al 2012, Smilowitz et al 2017). Myocardial injury after non-cardiac surgery (MINS) is defined as MI within 30 days after a non-cardiac surgery and is a common and independent predictor of mortality during the postoperative period (Botto et al 2014, Thygesen et al 2018). However, MINS could be clinically asymptomatic, and about 80% failed to get diagnosed (Coetzee & Biccard 2018).
There are many reasons for MINS to be clinically silent and easily missed in the postoperative period (Devereaux et al 2011). Chest pain and other ischaemic symptoms are atypical during this phase due to pain medications and surgical stress, which mask distinctive presentations (Devereaux et al 2011). Other diagnostic criteria for detection of acute MI include electrocardiogram (ECG) and cardiac muscle enzymes such as cardiac troponin (cT). Ischaemic changes on ECG might not be evident by the time of taking the ECG in the postoperative period as the usual timing of ECG is 12–24h following a surgery and ECG poorly predicts cardiovascular outcomes after a surgery (Devereaux et al 2011, Garcia et al 2013). Therefore, cT is the key diagnostic tool for MINS where levels remain high in serum for two weeks following an ischaemic event (Botto et al 2014, Thygesen et al 2018).
cT (I and T) are heart muscle regulatory proteins released into the blood stream when muscle fibres are damaged due to an ischaemic injury (Thygesen et al 2010), and both I and T isotypes demonstrate similar abilities to predict myocardial damage (Kvisvik et al 2017). The primary benefit of high-sensitive cardiac troponin (hs-cT) is the amplification of the diagnosing sensitivity of myocardial damage compared to conventional troponin (Ndrepepa et al 2011). The role of hs-cT to identify those patients who are clinically asymptomatic with myocardial injury is being discussed in the literature. The aim of this review is to summarise current evidence and clinical guidelines, highlighting the use of hs-cT as a biomarker in the detection of MINS. In this review, the literature search was done through the Western Australia East Metropolitan Health library service for studies published on role of hs-cT in detection of MINS. Priority was given to randomised studies.
Myocardial injury versus MI
MI has been redefined recently and is different to myocardial injury by definition (Thygesen et al 2018). Myocardial injury (MN) is identified as an elevation of cT above the 99th percentile of the reference values. The rise and fall of serum cT levels is indicative of an acute MN, whereas clinically symptomatic acute MN (eg: chest pain, dyspnoea, fatigability, palpitation, syncope and sweating) is considered to be MI (see Table 1) (Thygesen et al 2018). Myocardial injury following non-cardiac surgery (MINS) is considered to be MN during the first 30 days following a surgical procedure (Botto et al 2014).
Fourth definition of acute MI (related to MINS)
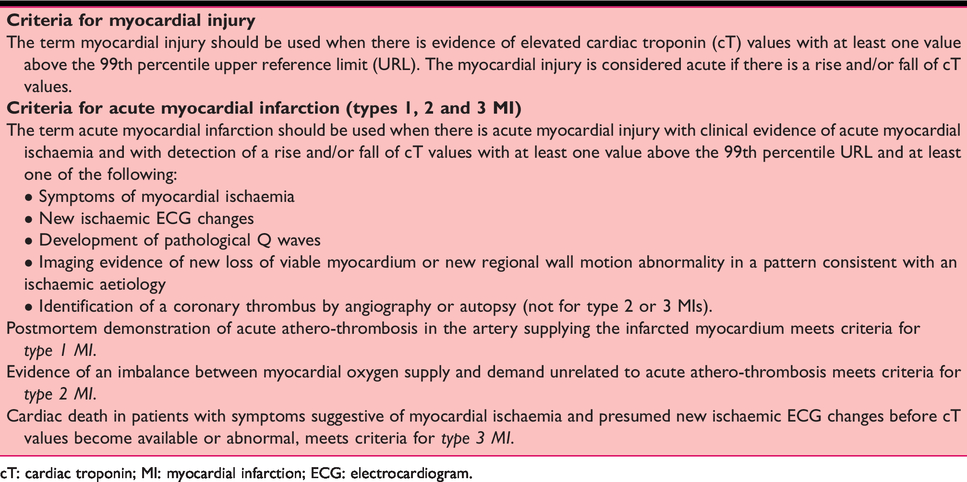
cT: cardiac troponin; MI: myocardial infarction; ECG: electrocardiogram.
As per the fourth definition of acute MI from the 2018 Joint Task Force of the European Society of Cardiology (ESC), the American College of Cardiology Foundation, the American Heart Association (AHA) and the World Health Federation, hs-cT is included in the diagnosis of MI and values above the 99th percentile of upper normal limit are a diagnostic indicator of MI (Thygesen et al 2018) (see Table 1). Furthermore, hs-cT is a better predictor of cardiovascular mortality than conventional cT measurements in stable coronary disease (Omland et al 2009).
Pathophysiology of MINS
The pathophysiology of MINS is multifactorial and currently evolving. Both plaque rupture (Type-1 MI) and a mismatch between oxygen supply and demand (Type-2 MI) are explained as the causes of myocardial damage after non-cardiac surgeries in most studies (Helwani et al 2018, Puelacher et al 2015). Perioperative hyper/hypotension, hypoxia/hypercarbia, anaemia, surgical stress with sympathetic hyperactivity and inflammation are some of the aetiologies besides thrombosis that contribute to myocardial damage in MINS (Biccard & Rodseth 2010). However, there are many other conditions which could cause myocardial injury (see Figure 1) and MINS is only one domain of the core pathology (Thygesen et al 2012).
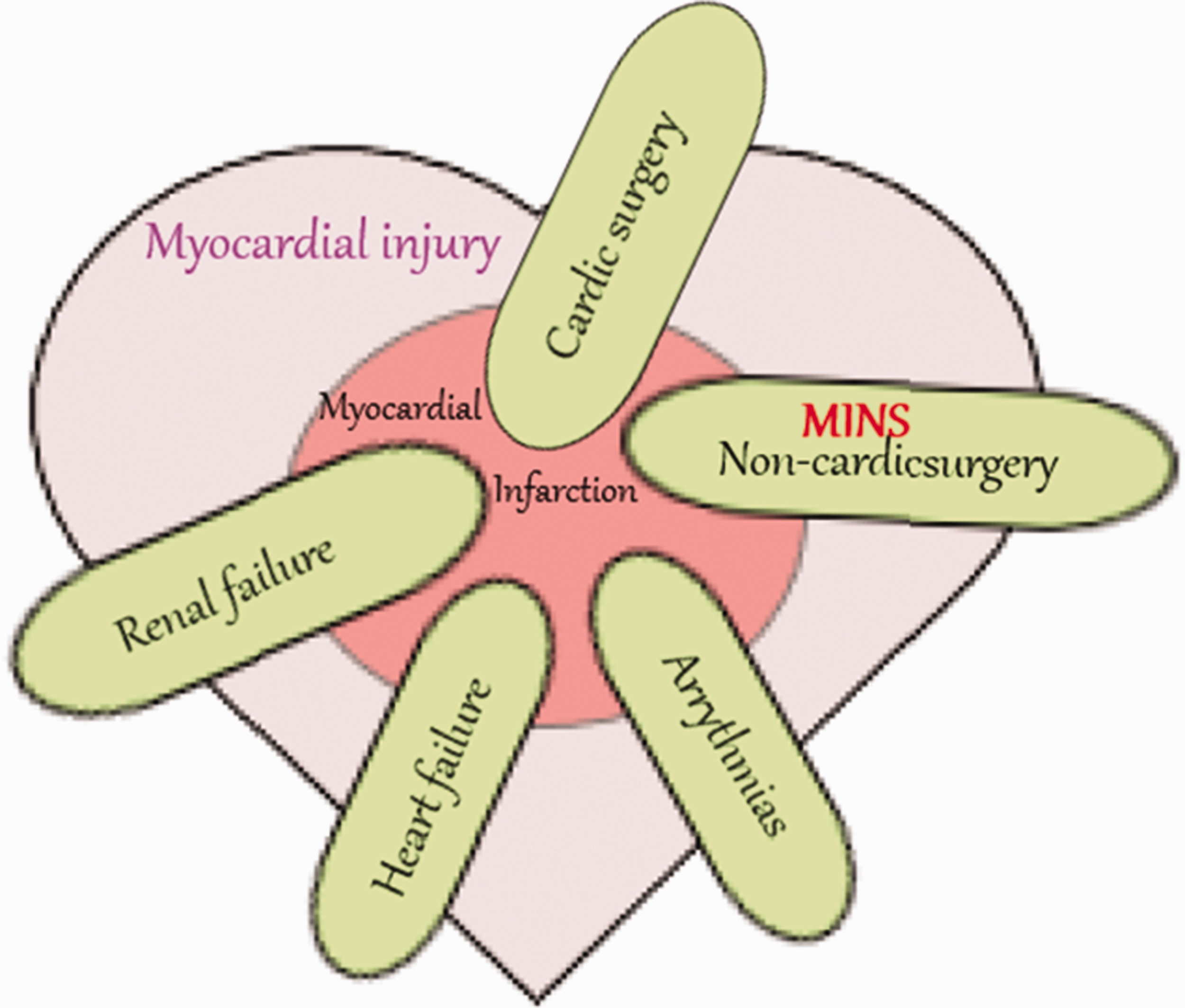
Myocardial infarction after non-cardiac surgery (MINS) pathophysiology
Current evidences for hs-cT in MINS
Most of the studies used conventional cT to diagnose myocardial injury after surgical procedures. In a single-centre observational study using 2232 intermediate- to high-risk (above 60 years of age) patients undergoing non-cardiac surgeries, conventional cT was measured on the first three days after surgery. Myocardial injury was found in 19% with associated increased mortality (Van Waes Judith et al 2013). There were few other single-centre studies which trialled conventional cT to diagnosed MINS and predicted adverse outcomes (Gorgun et al 2016, Kim et al 2016, Reed et al 2017). The Vascular Events in Non-cardiac Surgery Patients Cohort Evaluation (VISION) study is the largest prospective trial which assessed myocardial damage after non-cardiac surgeries and the place of cT in detecting MINS. The initial VISION study used conventional cT measurements on days one, two and three following non-cardiac surgeries, and 8% of the study population was diagnosed with MINS. Of those, 41% fulfilled the universal definition of MI (Botto et al 2014). In the second VISION study, hs-cT was used, which demonstrated that 17.9% suffered MINS (21.7% fulfilled the universal definition of MI) (Devereaux et al 2017). Accordingly, use of hs-cT increased the detection rate of MINS in comparable cohort of patients. A similar small study on 605 postsurgical patients demonstrated that use of hs-cT increased the diagnosis of MINS by two-fold, compared to conventional cT (Brown et al 2017).
Patients could have chronically elevated preoperative cT levels, which were not well evaluated in the literature for non-cardiac surgeries. There are many non-myocardial pathologies that could elevate cT levels such as renal disease, hypovolemia, atrial fibrillation, congestive heart failure, pulmonary embolism, myocardial contusion and sepsis (Jeremias & Gibson 2005). These conditions can lead to over diagnosis of MINS and should be taken in to account. As such, patients with chronic elevations may have led to a pointless delay to their procedures resulting in unnecessary investigations (Maile et al 2016). It is recommended to have baseline hs-cT levels done prior to a non-cardiac surgery (Thygesen et al 2018). However, when preoperative hs-cT levels are unavailable, it is advisable to confirm rising or falling hs-cT levels (see Table 1) to support the diagnosis of MINS (Thygesen et al 2018).
Troponin is useful in predicting adverse outcomes after non-cardiac surgeries in addition to its value in detecting MINS. Many studies demonstrated that hs-cT is an independent predictor of 30-day mortality following a non-cardiac surgical procedure (Botto et al 2014, Devereaux et al 2012, 2017, Kavsak et al 2011). Others performed conventional cT levels along with ECG in symptomatic and high-risk patients which positively correlates with 30-day postoperative mortality (Fleisher et al 2014). Another study found that 21% of high-risk patients had elevated conventional cT levels, which was associated with increased total mortality and a higher incidence of amputation in patients with peripheral vascular disease (Linnemann et al 2014). A similar study documented a 29% elevation of conventional cT in older patient cohorts with hip fractures, which predicted poor outcomes, including prolonged length of stay, increased residential care requirements and mortality (Fisher et al 2008, Puelacher et al 2018). Furthermore, increased postoperative hs-cT levels >14ng/L when compared to preoperative values are associated with short and long-term mortality (Kristensen et al 2014). However, most studies used conventional cT and further studies with hs-cT would be useful to validate its place in predicting adverse outcomes after non-cardiac surgeries.
International guidelines and recommendations
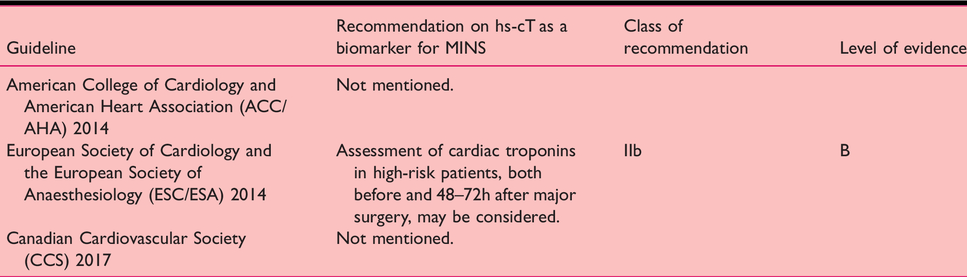
Major international guidelines do not currently provide clear recommendations for the usage of hs-cT in perioperative settings. The American College of Cardiology and AHA 2014 do not comment on the use of perioperative hs-cT (Fleisher et al 2014), whereas the ESC and the European Society of Anaesthesiology 2014 guidelines recommend preoperative and 48–72h postoperative hs-cT in high-risk patients undergoing non-cardiac surgeries (Kristensen et al 2014). The Canadian Cardiovascular Society 2017 guidelines recommend Brain natriuretic peptide (BNP) or N terminal pro-hormone BNP in high-risk patients but do not mention the use of hs-cT (Duceppe et al 2017) (see Table 2).
Major guideline recommendations on hs-cT in MINS
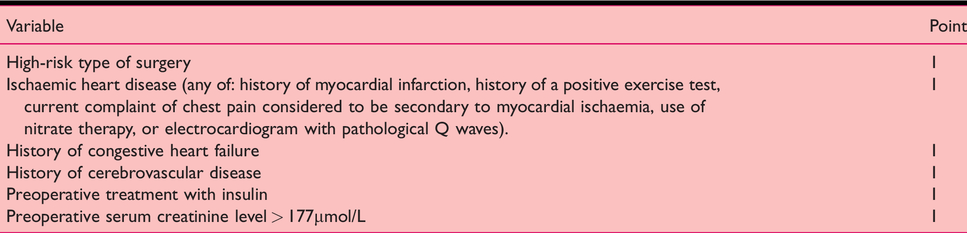
Revised Cardiac Risk Index (RCRI) (Lee et al 1999)
Discussion and recommendations
Several studies demonstrated the benefit of performing hs-cT levels in high-risk patients who are undergoing non-cardiac surgeries (Botto et al 2014, Kristensen et al 2014). However, routine use of hs-cT after a surgical procedure is not recommended to diagnose MINS and it should only be used with suspected high-risk patients (Fleisher et al 2014). There are many risk stratification tools which describe the identification of high-risk patients for adverse cardiac outcomes. American College of Surgeons National Surgical Quality Improvement Program (NSQIP) surgical risk calculator (Cohen et al 2013), NSQIP Myocardial Infarction and Cardiac Arrest calculator (Gupta et al 2011) and Revised Cardiac Risk Index (RCRI) (Lee et al 1999) are some of those tools used to predict adverse cardiac events after non-cardiac procedures. Amongst those, Cardiac Risk Index is the most popular and validated tool initially described by Goldman et al (1977) as a good predictor of perioperative mortality and major adverse cardiac events. Later, this tool was revised as RCRI (Lee et al 1999) (See Table 3). RCRI is now widely used by clinicians due to its simplicity and validity compared to abovementioned other cardiac risk stratification tools (Roshanov et al 2017, Singh and Zeltser 2018). The combined risk of non-fatal MI and cardiac death rate is 1% for one point in RCRI and 5.4% when three or more risks are present (Ford et al 2010). Weber et al (2013) demonstrated incremental value of adding hs-cT to RCRI in prognostication of adverse cardiac outcomes after non-cardiac surgeries.
Current evidence recommends that baseline hs-cT value is measured, followed by levels at 12, 24 and 48h following surgery, in asymptomatic patients, with high cardiac risk (Botto et al 2014, Devereaux et al 2012, Kristensen et al 2014). However, chronic troponin elevation needs to be excluded and for situations in which preoperative cT levels are not available, residual blood samples can be used to test baseline cT levels. An alternative is to monitor rising or falling hs-cT levels (Thygesen et al 2018). Patients with electrocardiographic changes or symptoms suggestive of MINS need serial hs-cT as in non-surgical situations. Those recommendations are based on current evidence and further large-scale studies are necessary to formulate a standard guideline for perioperative hs-cT in the detection of MINS.