
Abstract
Background
The UK practice of laparoscopic cholecystectomy has reduced during the COVID-19 pandemic due to cancellation of non-urgent operations. Isolated day-case units have been recommended as ‘COVID-cold’ operating sites to resume surgical procedures. This study aims to identify patients suitable for day case laparoscopic cholecystectomy (DCLC) at isolated units by investigating patient factors and unexpected admission.
Method
Retrospective analysis of 327 patients undergoing DCLC between January and December 2018 at Ysbyty Gwynedd (District General Hospital; YG) and Llandudno General Hospital (isolated unit; LLGH), North Wales, UK.
Results
The results showed that 100% of DCLCs in LLGH were successful; 71.4% of elective DCLCs were successful at YG. Increasing age (p = 0.004), BMI (p = 0.01), ASA Score (p = 0.006), previous ERCP (p = 0.05), imaging suggesting cholecystitis (p = 0.003) and thick-walled gallbladder (p = 0.04) were significantly associated with failed DCLC on univariate analysis. Factors retaining significance (OR, 95% CI) after multiple regression include BMI (1.82, 1.05–3.16; p = 0.034), imaging suggesting cholecystitis (4.42, 1.72–11.38; p = 0.002) and previous ERCP (5.25, 1.53–18.00; p = 0.008). Postoperative complications are comparable in BMI <35kg/m2 and 35–39.9kg/m2.
Conclusions
Current patient selection for isolated day unit is effective in ensuring safe discharge and could be further developed with greater consideration for patients with BMI 35–39.9kg/m2. As surgical services return, this helps identify patients suitable for laparoscopic cholecystectomy at isolated COVID-free day units.
Keywords
Introduction
Cholelithiasis affects approximately 20% of the population (Rance & Jones 2016) and is a common acute surgical presentation in the UK with over 600,000 operations performed annually (Beckingham 2017). Laparoscopic cholecystectomy (LC) is widely considered as the gold standard for treating symptomatic gallstone disease (NICE 2014b) with fewer postoperative complications and shorter overall admissions compared to equivalent open procedures (Antakia et al 2014).
The British Association of Day Surgery (BADS) recommends 60% of LCs be performed as day cases (Solodkyy et al 2018). This is dependent on maintaining patient safety in same-day discharges. Currently, the North West Wales NHS Trust does not have standardised selection criteria for day-case elective LC. This makes identifying appropriate patients challenging, based on clinical judgement alone, for procedures performed at isolated day-case units which do not have the capacity for overnight admission. For hospitals accomodating inpatients, the use of satellite day-units helps to reduce the burden and growing demand placed on surgical services.
With the rapid development of the COVID-19 pandemic, current practice of minimally invasive surgery in the UK has dramatically changed. All non-urgent elective procedures have been cancelled, with only emergency and/or cancer surgery continuing (Brindle & Gawande 2020, Zheng et al 2020). The Royal College of Surgeons recommend that elective procedures can resume provided there is physical separation of COVID-19 positive and negative patients (RCSE 2020). Intercollegiate General Surgery guidance suggests the use of isolated day-case units as COVID-cold sites. The provision and protection of these ‘cold’ sites to deliver elective surgery is considered an absolute priority (Fearnhead et al 2020).
This study examines patient factors associated with successful day case laparoscopic cholecystectomy to identify suitable patients for operation at an isolated day unit.
Methods
This retrospective analysis included all laparoscopic cholecystectomies performed at Ysbyty Gwynedd (YG) and Llandudno General Hospital (LLGH) between 1 January and 31 December 2018. Both surgical day-case units at YG and LLGH close at 20:00 hrs. Patients unable to meet discharge at YG can be hospitalised onto another inpatient surgical ward. However, patients requiring admission at LLGH isolated unit must be transferred by ambulance approximately 22 miles to YG, as LLGH has no capacity for overnight admissions.
Relevant patient identification numbers were obtained from the local NHS Trust. The project was registered with the hospital audit department. Paper medical records and local online informatics tools, including the Welsh Clinical Portal and Unisoft Gastrointestinal Reporting Tool, were used to collect data.
Variables collected included sex, age, body mass index (BMI), comorbidities, ASA grade, previous abdominal surgery, smoking status, preoperative imaging results (cholelithiasis, common bile duct stones, gall bladder status), prior pancreatitis and endoscopic retrograde cholangiopancreatography (ERCP) procedure. The Charlson Comorbidity Scoring system (Charlson et al 1987) was calculated to compare the severity of each patient’s comorbidities. The ASA Grade (Doyle & Garmon 2019) was calculated where this was insufficiently documented. The Cholecystectomy As A Day Case (CAAD) Scoring system (Table 1) was also applied to each patient (El-Sharkawy et al 2019).
The Cholecystectomy As A Day Case (CAAD) scoring system (El-Sharkawy et al 2019)
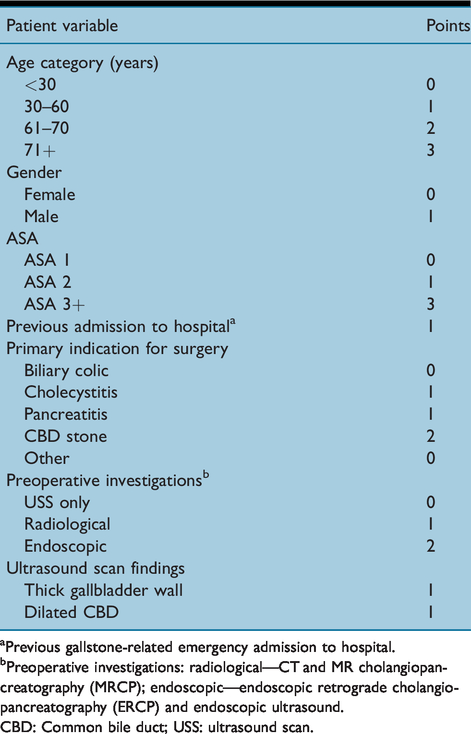
Previous gallstone-related emergency admission to hospital.
Preoperative investigations: radiological—CT and MR cholangiopancreatography (MRCP); endoscopic—endoscopic retrograde cholangiopancreatography (ERCP) and endoscopic ultrasound.
CBD: Common bile duct; USS: ultrasound scan.
Statistics
Demographic data were compared using the chi-square test. A binary linear logistic multiple regression was used to ascertain the magnitude of the association among the significant predictors, based on the chi-square test. An odds ratio with 95% confidence interval was generated using SPSS Statistics to determine likelihood of successful DCLC.
Results
Ysbyty Gwynedd versus Llandudno General Hospital
A total of 327 laparoscopic cholecystectomies were performed during the study period across both hospitals (Table 2). Thirty (9.2%) procedures were performed at LLGH isolated unit; 297 (90.8%) were performed at YG district hospital; and 245 (82.5%) LCs at YG were planned as elective day cases; however, only 175 (71.4%) patients achieved this. LLGH displayed 100% successful day case rates.
Laparoscopic Cholecystectomies performed between January and December 2018
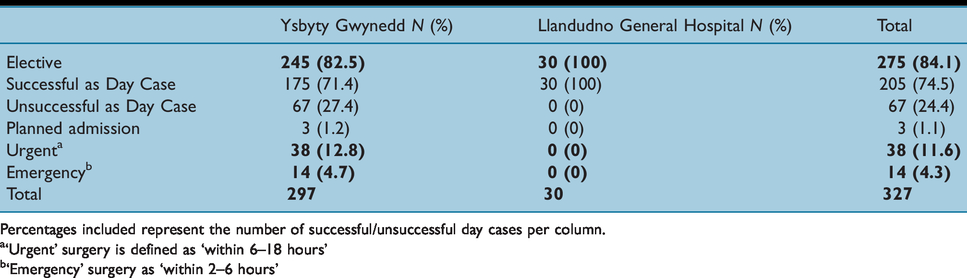
Percentages included represent the number of successful/unsuccessful day cases per column.
‘Urgent’ surgery is defined as ‘within 6–18 hours’
‘Emergency’ surgery as ‘within 2–6 hours’
Patients in YG were older than in LLGH with a median age of 56 years (range 20–92 years) compared to 46 years (23–69 years). Median BMI at YG and LLGH were 29.8kg/m2 (16.4–48.5kg/m2) and 29.95 kg/m2 (19.9–37 kg/m2), respectively. Median BMI for successful and unsuccessful elective DCLC across both hospitals were 30.2 kg/m2 (16.4–47.8 kg/m2) and 29.6 kg/m2 (17.9–48.5 kg/m2), respectively. Most patients scored ASA 2: 188 (63.3%) at YG and 26 (86.7%) at LLGH. The four remaining patients operated at H2 were ASA I. Patients scoring ASA > 2 do not undergo LC at the isolated unit.
Patient demographics
Baseline variables are presented in Table 3. In the study, 242 (74.0%) patients were females and 85 (26.0%) were males. The rate of unsuccessful DCLC was similar between males (23.6%) and females (25.0%). Increasing age is associated with greater risk of unsuccessful DCLC (p = 0.004). Also, 64.3% of patients ≥80 years of age failed discharge, compared to 19.6% of patients who were in the age group of 20–39 years.
Patient demographics of all Laparoscopic Cholecystectomies performed at Ysbyty Gwynedd and Llandudno General Hospital between January and December 2018

Note: Percentages included represent the number of successful/unsuccessful day cases per row.
Prior pancreatitis represent patients with any previous episode of pancreatitis in recent or remote past.
Increasing BMI is also significantly associated with higher likelihood of failed DCLC: 56.3% of morbidly obese patients (≥40kg/m2) achieved DCLC compared to 91.9% with a ‘desirable’ BMI of 18.5–24.9kg/m2 (p = 0.01) (Table 3) (NICE 2014a). However, the rate of unsuccessful DCLC in patients with BMI 35–39.9kg/m2 (28.9%) is comparable to patients with a BMI of 25–29.9kg/m2 (25.6%) (Table 3). BMI 25–29.9kg/m2 represented most unexpected overnight stays (32.8%) (Table 3). Of these 23 patients, eight had ASA III, eight had previous abdominal surgery, four reported cholecystitis and ten reported thick-walled gallbladders on imaging. Twelve patients were reported to have significant comorbidities including myocardial infarction, angina, stroke, chronic obstructive pulmonary disease, obstructive sleep apnoea and diabetes mellitus (T2). Worsening ASA is another significant factor related to admission (p = 0.006), with 41.5% of ASA III and 66.7% of ASA IV patients being admitted compared to 11.4% and 21.7% of patients scoring ASA I and II, respectively. Previous ERCP is significantly associated with increased rate of failure (p = 0.05).
The following variables were not significantly associated with failure rate: Charlson Comorbidity Score (p = 0.062), previous abdominal surgery (p = 0.16) and smoking status (p = 0.40). Although not significant, result trends suggest that lower comorbidity scores (0–2) correlated to higher DCLC success rates (80.1%) (Table 3).
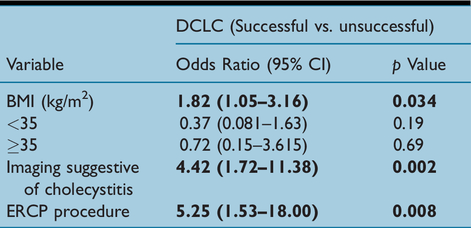
Following the application of a multiple binomial regression on patient variables in Table 3, the factors that retain significance are BMI, previous cholecystitis and previous ERCP (Table 4). Further grouping and regression of BMI into categories according to the current Royal College of Surgeons guidelines for day surgery (Humphreys & Stocker 2019), BMI <35kg/m2 and BMI ≥35kg/m2 do not retain significance (BMI <35kg/m2 p = 0.19; BMI ≥35kg/m2 p = 0.69).
Multiple logistic binomial regression: factors significantly associated with unsuccessful DCLC
Cholecystectomy As A Day Case scores
According to El-Sharkawy et al, a CAAD Score of ≤5 points can be used as a positive predictor for successful DCLC (El-Sharkawy et al 2019). The percentage of patients operated electively at YG hospital was 72.7% and 90.0% of patients at the LLGH isolated unit had CAAD score ≤5 (Table 5). Three patients were operated at LLGH with scores >5. These patients scored additional points due to previous admissions for cholecystitis; prior ERCP and CT radiological imaging; and previous episodes of pancreatitis.
CAAD Score for elective laparoscopic cholecystectomy at Ysbyty Gwynedd and Llandudno General Hospital
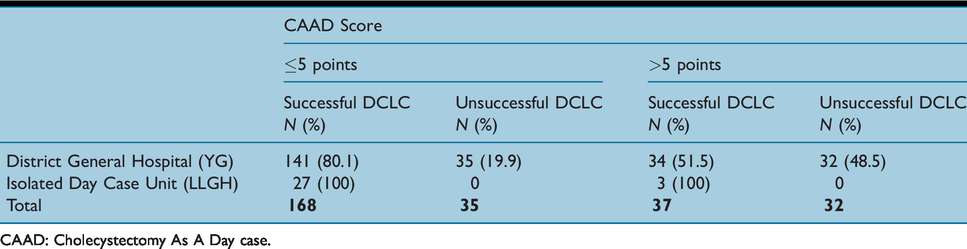
CAAD: Cholecystectomy As A Day case.
A total of 134 (79.8%) patients suceeding day-case discharge with CAAD scores ≤5 points had BMI ≤35kg/m2. Twenty-seven (73.0%) patients with CAAD > 5 points achieving DCLC had BMI ≤35kg/m2.
Surgical factors
In total, 326 patients had preoperative imaging: 271 (82.9%) abdominal ultrasound scans, 26 (7.6%) CT scans and 29 (8.9%) had both. Note that 198 (74.7%) elective patients reporting cholelithiasis were successfully operated as DCLC (Table 3). DCLC was achieved in all seven elective (100%) CBD stone cases, with one performed at LLGH. Also, 199 ‘thin-walled’ gallbladders were operated on electively: 133 successful DCLC at YG and 23 at LLGH isolated unit. Forty-eight (64.0%) ‘thick-walled’ gallbladders were successful DCLCs: 41 at YG and seven at LLGH. Those suffering pancreatitis prior to surgery saw a 72.7% successful DCLC rate, with two performed at LLGH day-case site. Previous ERCP was found in 27 (8.3%) patients. Five (18.0%) had multiple attempts. DCLC success rates differed from 61.1% with ERCP to 76.4% without (p = 0.05). 185 (78.7%) successful DCLCs did not have imaging findings suggestive of cholecystitis, as the primary indication for elective procedure was management of biliary colic. Almost half (45.9%) of patients reporting cholecystitis on imaging failed DCLC.
Previous admissions for acute cholecystitis
Of the 79 patients presenting with imaging suggestive of thick-walled GB and/or cholecystitis, 27 had an electronically documented admission for acute cholecystitis prior to elective DCLC. Of these, 10 (37.0%) failed DCLC. Thirteen (50.0%) patients with no previous admission for cholecystitis failed DCLC. Eight (30.1%) patients with one previous admission and two (7.1%) patients with two previous admissions failed DCLC. The median length of stay after failed DCLC in patients with no prior admission was one (range 1–6) day. In patients with one prior admission, the median length of stay was 4.5 (range 1–16) days. In patients with two prior admissions, the median length of stay was three (range 2–4) days.
Reasons for overnight stay
Sixty-seven elective DCLC patients were admitted overnight at YG district hospital: the mean length of stay was 4.1 days (range 1–44 days). About 19.1% of YG patients with CAAD Score ≤5 points did not achieve successful DCLC (Table 5).
Reasons for unexpected admission in planned elective day case procedures
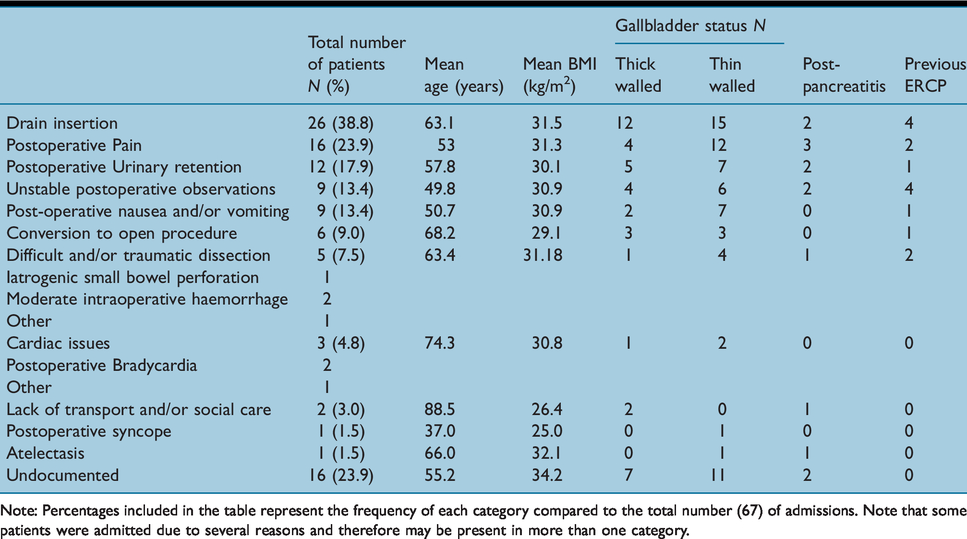
Note: Percentages included in the table represent the frequency of each category compared to the total number (67) of admissions. Note that some patients were admitted due to several reasons and therefore may be present in more than one category.
The most common reason for unexpected admissions was drain insertion due to intraoperative bleeding. One hundred percent of drains inserted were in patients over a desired BMI of 18.5–24.9kg/m2. Thirteen patients with drains inserted (50.0%) had CAAD score ≤5 points: nine (69.2%) had BMI ≤35kg/m2. Of the remaining 13 (50.0%) drains inserted in with CAAD scoring > 5 points, 11 (84.6%) had BMI ≤35kg/m2. The largest proportion of drains inserted (50%) were found in patients with a BMI of 25–29.9kg/m2: four of these patients had thin-walled gallbladders with no past pancreatitis/ERCP. Amongst the nine remaining, five (38.5%) thick-walled gallbladders and three (23.1%) cases of cholecystitis were reported on imaging, two (15.4%) suffered pancreatitis and one (7.7%) underwent ERCP before surgery. Patients with a BMI > 35kg/m2 represented 19.2% of drains inserted, suggesting no increased risk in this group.
All (100%) laparoscopic procedures converted to open surgery were in patients with BMI 18.5–24.9kg/m2: two had CAAD score ≤5 points and four had >5 points. Of the six cases converted to open, two (33.3%) had evidence of cholecystitis on preoperative imaging, with one thick and one thin-walled gallbladder. Of the remaining four (66.6%) with no evidence of cholecystitis, two patients had a thin walled gallbladder and two had a thick-walled gallbladder, with one of these having undergone an ERCP prior to surgery. None of the six patients converted to open showed CBD dilation.
No correlation between number of previous abdominal surgeries and complications were found. 23.9% of unexpected admissions were insufficiently documented.
Operating times
The majority of elective procedures were performed during morning operating lists, before midday (Table 7). A total of 106 (51.7%) successful DCLCs were performed during the morning list, compared to 32.9% of unsuccessful DCLCs. Thirty-three (47.1%) of unsuccessful DCLCs were performed in the afternoon. At the LLGH isolated unit, 18 (60.0%) procedures were performed in the morning and seven were performed (23.3%) in the afternoon.
Time of elective DCLC procedures
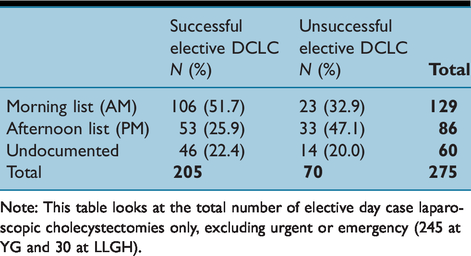
Note: This table looks at the total number of elective day case laparoscopic cholecystectomies only, excluding urgent or emergency (245 at YG and 30 at LLGH).
Discussion
The majority of patients undergoing an operation at the isolated unit meet the Royal College of Surgeons guidelines eligibility for day surgery (Humphreys & Stocker 2019). All (100%) of the elective laparoscopic cholecystectomies in LLGH isolated unit and 71.4% at YG district general hospital were completed as day cases.
Recent guidelines published by the British Association of Day Surgery state that day surgery ‘works best’ when provided at self-contained ambulatory units (Bailey et al 2019). The current study demonstrates this, along with similar successes in existing literature (Van Caelenberg et al 2019). With the current pandemic, the high demand for inpatient beds is limiting the number of DCLCs that can be performed, further exacerbated by the occupation of elective surgical beds by emergency or medical patients (Wales Audit Office 2016).
Our results are consistent with other centres regarding DCLC failure rates (Donkervoort et al 2016, Gill et al 2016). The CAAD Score (El-Sharkawy et al 2019) shows that scores ≤5 are significantly associated with successful DCLC: 82.9% of our patients with CAAD score ≤5 achieved same-day discharge. Three patients operated at LLGH isolated unit had CAAD scores > 5 and still achieved successful DCLC. This demonstrates that although the CAAD score is useful in guiding judgement on patients operated at isolated units, surgeon discretion is still a major component of selection. However, it is difficult to extrapolate this further with only three patients in this study.
The original CAAD Scoring System does not include any indication on how BMI contributes to the likelihood of unsuccessful DCLC. Our study found increasing BMI to be associated with greater risk of failure (p = 0.010), which is supported in the literature (Chávez et al 2018). However, patients with BMI 35–39.9kg/m2 could be considered for DCLC at isolated day units, as no significant differences in postoperative complications or re-admission rates were observed compared to BMI <35kg/m2. BMI above and below 35kg/m2 did not retain significance after applying the binomial multiple regression, suggesting that BMI in isolation is not solely responsible for DCLC failure. With the correct expertise and equipment (Gregori et al 2018), DCLC at satellite units is safe for patients with BMI over 35kg/m2 and is beneficial by reducing the demand for elective/inpatient beds at main hospitals and achieving higher patient satisfaction through early postoperative mobilisation, accelerated recovery and reduced risk of hospital-acquired problems (Gogna & Latifi 2019, Gregori et al 2018, Jain et al 2005, Tandon et al 2016, Wales Audit Office 2016). Furthermore, the addition of BMI to the CAAD Scoring system may further separate patients into more accurate predictive groups for DCLC failure, as similar success rates were seen with CAAD Scores of ≤5 (79.8%) and > 5 (73.0%) points when BMI ≤35kg/m2.
BMI 25–29.9kg/m2 and ASA II saw the largest proportions of admitted elective patients. This is partly due to greater representation in the study. Nevertheless, the majority of individuals failing DCLC in these groups possessed multiple risk factors, including systemic disease and gallbladder complexity, which are likely to have contributed to admission.
Many unsuccessful DCLCs were performed during the afternoon when there is less available time to meet discharge criteria on the day-case wards. A postoperative period of four hours is required for observation before discharge, which can be difficult if procedures are performed later in the afternoon (Seyednejad et al 2017, Van Caelenberg et al 2019). Patients with higher BMI, ASA and other identified risk factors should be prioritised on operating lists for earlier start times.
ERCP prior to LC should be viewed with caution when selecting patients for isolated centres. The procedure promotes the formation of adhesions at Calot’s Triangle, increasing the technical complexity of the LC (Baghdadi et al 2019, Mann et al 2013). Thickened gallbladder walls on preoperative imaging are also clinical predictors for difficult LC (Baghdadi et al 2019, Da Costa et al 2018) and conversion to open cholecystectomy (Da Costa et al 2018). However, ERCP and thick-walled gallbladders should not be complete contraindications for DCLC at satellite unit as they do not demonstrate higher postoperative complications in our study, despite associations with failed DCLC (ERCP p = 0.008). Previous admission for cholecystitis is also not a risk factor for DCLC in our results, contradicting existing literature (Alore et al 2019, El-Sharkawy et al 2019).
As surgical practice slowly returns in the UK following the coronavirus pandemic, we advocate the use of isolated day-case units for laparoscopic cholecystectomy in COVID-19 negative patients who are appropriately selected. Current literature supports the separation of hospitals into COVID-19 ‘positive’ and ‘negative’ hubs to avoid cross contamination between patients and staff (Brindle & Gawande 2020, Zheng et al 2020). The use of off-site satellite units for ‘clean’ surgery has the advantage of separation from the ‘dirty’ coronavirus-dedicated wards in main hospitals. The use of isolated facilities for elective procedures, such as LC, will support the continuation of surgical services in the UK for non-urgent procedures.
Limitations
The main limitation of our study is that our conclusions are drawn from a relatively small cohort of participants. Within 2018, 327 patients underwent a laparoscopic cholecystectomy. As North West Wales is a rural NHS Trust, both the Ysbyty Gwynedd and Llandudno General Hospital are low volume centres with smaller surgical day units and operating teams. In a 2013 Cochrane review, the use of day-surgery versus overnight admission for laparoscopic cholecystectomy was shown to be just as safe with comparable effects on patient-oriented outcomes (Vaughan et al 2013). However, the impact of patient factors on this was not investigated, unlike in our study.
Inadequate documentation was another common finding throughout this study, causing difficulty obtaining data on the reasons why patients breached day case targets. Patients with unknown cause for failed same-day discharge represent the second largest cohort in postoperative admissions analysed. Further investigation into documentation practice by surgical and nursing staff would allow more detailed conclusions, as well as improve clinical practice at YG and LLGH.
We acknowledge that rate of drain insertion in failed elective DCLCs was 38.8%. This outcome was obtained from a heterogenous sample and is likely due to surgeon preference and intraoperative factors, which were not examined in this study. In addition, although we collected data on ITU admission and readmission rates (Appendix 1), further work with a greater data set is required to understand the significance of these.
78.7% of successful DCLCs had imaging not suggestive of cholecystitis, which suggests that disease severity impacts rates of DCLC. In future work, the use of the Tokyo Guidelines score would be useful in assessing cholecystitis status versus patient demographics on same-day discharge (Kiriyama et al 2018). Data on the number of previous episodes of cholecystitis would have been useful in order to assess the impact of such episodes on rate of successful day case surgery. The use of the Charlson Comorbidity Score was also limiting although useful for comparison. The scores were restricted to specific comorbidities which left other significant conditions, such as Parkinson’s disease, unconsidered. Anaesthetic factors considering suitability for day-case unit were also not investigated which would greater support our findings. It is important to note that the median BMI for unsuccessful DCLCs across both hospitals (29.6kg/m2) has been skewed by the increased rate of failed DCLC in patients with BMI <18.5kg/m2.
Further work
The strict use of an effective postoperative scoring system could be one method implemented at YG and LLGH to increase the proportion of successful DCLCs. The ‘Chung Score’ suggested by Greilsamer et al (2018) is a post-anaesthetic discharge criteria that evaluates patients’ fitness following day-case surgery (Daradkeh et al 1998). Its use has shown to significantly increase the success of outpatient DCLCs by providing a clear, succinct pathway towards safe and appropriate discharge (Greilsamer et al 2018, Randhawa & Pujahari 2009).The current surgical day-case wards at YG and LLGH follow a discharge criterion with some similarities to the Chung Score (such as postoperative mobility, nausea/vomiting and pain). It also includes factors not considered by the Chung Score (such as postoperative urination). Some of the reasons for unexpected admission in our study can be considered as surgically unavoidable and unpredictable: intervention prior to surgery is unlikely to lead to reductions in admission rates. However, further research to assess the efficacy of the current discharge objectives employed at YG and LLGH would be beneficial to understand whether all parameters assessed postoperatively are required in order to make a safe discharge and how this would impact the number of patients admitted following elective DCLC.
Further research into operating surgeon grade would also be useful. As LC is one of the first procedures performed by surgical trainees (Greilsamer et al 2018), surgeon experience for the failed DCLCs at YG and LLGH may provide insight and reasoning behind intra/postoperative complications, conversions to open LC and readmissions seen. Although operation times are longer in LCs performed by trainees compared to consultant level surgeons, Atta et al suggests no differences in complication rates when trainees are observed by their seniors (Atta et al 2017, Greilsamer et al 2018). Investigation into LC operation waiting times after acute cholecystitis presentation or following ERCP would also benefit practice by creating an optimum time frame for these patients selected for LC surgery at LLGH isolated day unit.
Conclusion
The practice of day case laparoscopic cholecystectomy in Ysbyty Gwynedd and Llandudno General Hospital meets the British Association of Day Surgery standards with combined success rates of 62.7% overall. Current patient selection for procedures at the isolated unit is effective in ensuring safe discharge. Factors such as increasing age, BMI, gallbladder thickness and ERCP procedure should not be complete contraindications for surgery at isolated unit but should be considered in combination with all other affecting parameters. Existing selection processes should be continued, however further work towards selection for isolated unit should be made with consideration to patients with higher BMI measurements (35–39.9kg/m2). More effort into utilising satellite day-surgery units should be adopted for laparoscopic cholecystectomy, especially during times of inpatient bed shortages. The use of isolated surgical units should be considered to support the return of non-urgent elective procedures following the coronavirus pandemic.
No competing interests declared.
Footnotes
Appendix 1
ITU Admission
Nine patients were admitted onto ITU/HDU at YG with mean admission time of 3.8 days (range 1–13 days). The mean age of patients was 64.9 years (41–79 years) compared to 58.7 years in normal admission. Patients with BMI of 35kg/m2 generally stayed the longest in ITU: mean length of stay was 5.3 days compared to four days <35kg/m2. The patient staying the longest in ITU (13 days) was the oldest at 79 years. ASA 4 represented 22.2% of ITU patients, compared to 0% in normal admission.
Readmission rates
Thirty patients were readmitted within 30 days to YG district general hospital following LC: one emergency, five urgent and 24 elective procedures, with 12 (50%) having had successful DCLC. Reasons for the 24 elective readmissions included seven surgical site infections; four subcapsular/gallbladder fossa collections; three recurrent right upper quadrant pain; one chest pain; one musculoskeletal pain; one pancreatitis; one hospital-acquired pneumonia and six undocumented. One readmitted patient with wound infection was operated at the LLGH isolated unit. 54.2% of elective patients readmitted scored BMI >30kg/m2.