
Abstract
Background
Patients undergoing surgery for oesophageal cancer are at high risk of malnutrition due to pathology and neoadjuvent therapy. This study sought to determine if oesophageal cancer patients undergoing oesophagectomy achieve superior clinical outcomes when preoperative nutritional counselling is performed.
Methods
Oesophageal cancer patients undergoing oesophagectomy were retrospectively divided into cohorts based on those who received (n = 48) and did not receive (n = 58) preoperative nutritional counselling. We compared weight loss, length of stay, 30-day readmission related to nutrition or feeding tube problems, and 90-day mortality.
Results
Per cent weight loss was less in patients who received preoperative nutritional counselling. There was a trend toward decreased mean length of stay and there were fewer readmissions for feeding tube-related complications in patients who received counselling.
Conclusions
Nutritional counselling before surgery may lead to decreased weight loss and reduced readmissions for feeding tube-related complications in patients with oesophageal cancer undergoing oesophagectomy.
Introduction
Oesophageal cancer patients are at high risk of malnutrition due to potential obstruction of the oesophagus from tumour and radiation-related changes that can occur in neoadjuvant treatment. Malnutrition is associated with worse outcomes in patients undergoing major surgery, particularly upper gastrointestinal surgery such as oesophagectomy (Steenhagen et al 2017). Multiple guidelines and previous evidence support nutritional therapy in the preoperative period for patients undergoing oesophagectomy; however, the extent of nutritional intervention needed is unknown (Ligthart-Melis et al 2013, Liu et al 2018, Ljungqvist et al 2017, Low et al 2019, Wang et al 2018, Weimann et al 2017, Qiu et al 2020).
A minority of gastrointestinal and oncologic surgeons in the United States utilise any formal nutritional assessment and therapy in clinical practice despite demonstrated effectiveness (Williams & Wischmeyer 2017). To be successful, any intervention must be supported and utilised by the surgeon in order to have an impact on patient care, and this has led to the recent increased interest in implementation science in surgical care (Hull et al 2017, Rapport et al 2018). While recent guidelines recommend nutritional support for patients, specific examples of formal programs may be helpful in promoting implementation, particularly among thoracic surgeons treating patients with oesophageal cancer.
Given the low implementation rates of formal nutritional programs in surgery in the United States, as well as the recent publication of guidelines developed specifically for oesophagectomy patients, we sought to evaluate our single-institution experience with implementation of a formal nutritional counselling program for the routine care of oesophageal cancer patients and to describe how this could be implemented at other centres (Liu et al 2018, Low et al 2019). We hypothesized that by implementing a formal nutritional counselling program for oesophageal cancer patients, we would observe improved short-term outcomes.
Materials and methods
In 2017, registered dietitians in the clinical oncology department at our academic medical centre in the United States began routine counselling of oesophageal cancer patients in the thoracic surgery clinic preoperatively and became familiar with their nutritional needs. For patients who received nutritional counselling, dietitians assessed their oral intake and caloric needs prior to surgery and provided recommendations for nutritional optimization, including tube feedings if needed. Table 1 shows the nutritional interventions performed. Based on the dietitian’s initial evaluation at the preoperative visit, nutrition regimens were personalized and closely monitored. They also provided education regarding postoperative nutritional concerns, such as jejunostomy tube use and troubleshooting, as well as dietary modifications. They continued following patients after surgery, including at the two-week postoperative clinic visit and by phone on a weekly basis as needed. Patients were able to contact dietitians outside of scheduled visits via a phone line reserved for cancer patients who had nutritional issues during the perioperative period.
Nutritional intervention by a specialized dietitian in the preoperative period for patients undergoing oesophagectomy.
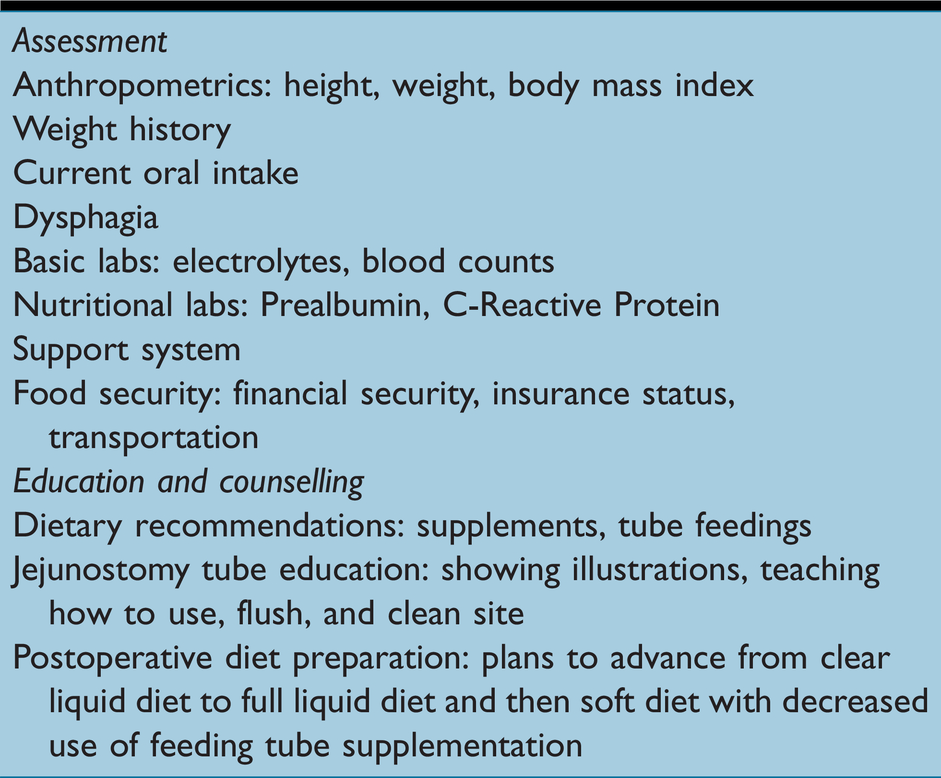
Most initial consultations by the dietitian occurred in the outpatient surgical clinic at the time of the initial visit with the surgeon. However, some patients were seen initially by dietitians in the radiation oncology department during neoadjuvant treatment or in the inpatient setting if they presented with obstructing oesophageal cancer to the emergency department. All dietitians who provided a consultation were familiar with oesophageal cancer and oesophagectomy. Dietitians in the thoracic surgery clinic provided specialized oral and written instructions about the use and troubleshooting of feeding jejunostomy tubes, as it is our routine practice to place these in all patients at the time of oesophagectomy. The dietitians’ consultations occurred before or after the surgeon met and examined the patient, whichever fit best with the clinic flow that day.
Before initiating the study to evaluate effectiveness of the intervention, we obtained approval from our Institutional Review Board. We compared outcomes of patients who received nutritional counselling to those who did not. We conducted a retrospective cohort study by searching patient records and querying the Arkansas Clinical Data Repository database. We used Current Procedural Technology codes for oesophagectomy (43107, 43112, 43117) to identify the oesophagectomy population. Patients treated for disease other than oesophageal cancer were excluded. We included 106 patients who underwent oesophagectomy at our institution between 2014 and 2019.
Patients were divided into two cohorts based on those who received (n = 48) and those who did not receive (n = 58) nutritional counselling by a registered dietitian before oesophagectomy. Outcomes evaluated were per cent weight change, mean length of stay (LOS), 30-day readmission related to malnutrition or feeding tube problems, and 90-day mortality. Weights at the time of surgical consultation were compared to weights at the first follow-up visit after hospital discharge following oesophagectomy.
Statistical analysis was completed using statistical analysis software (SAS). Characteristics for several variables were measured to evaluate the entire sample at baseline and to determine similarity between groups. Outcomes were similarly reported and compared. For categorical data, frequencies were reported, and Chi square tests or Wilcoxon rank tests were used to determine significance. For quantitative data, means and ranges were reported, and t tests were used to determine significance.
Results
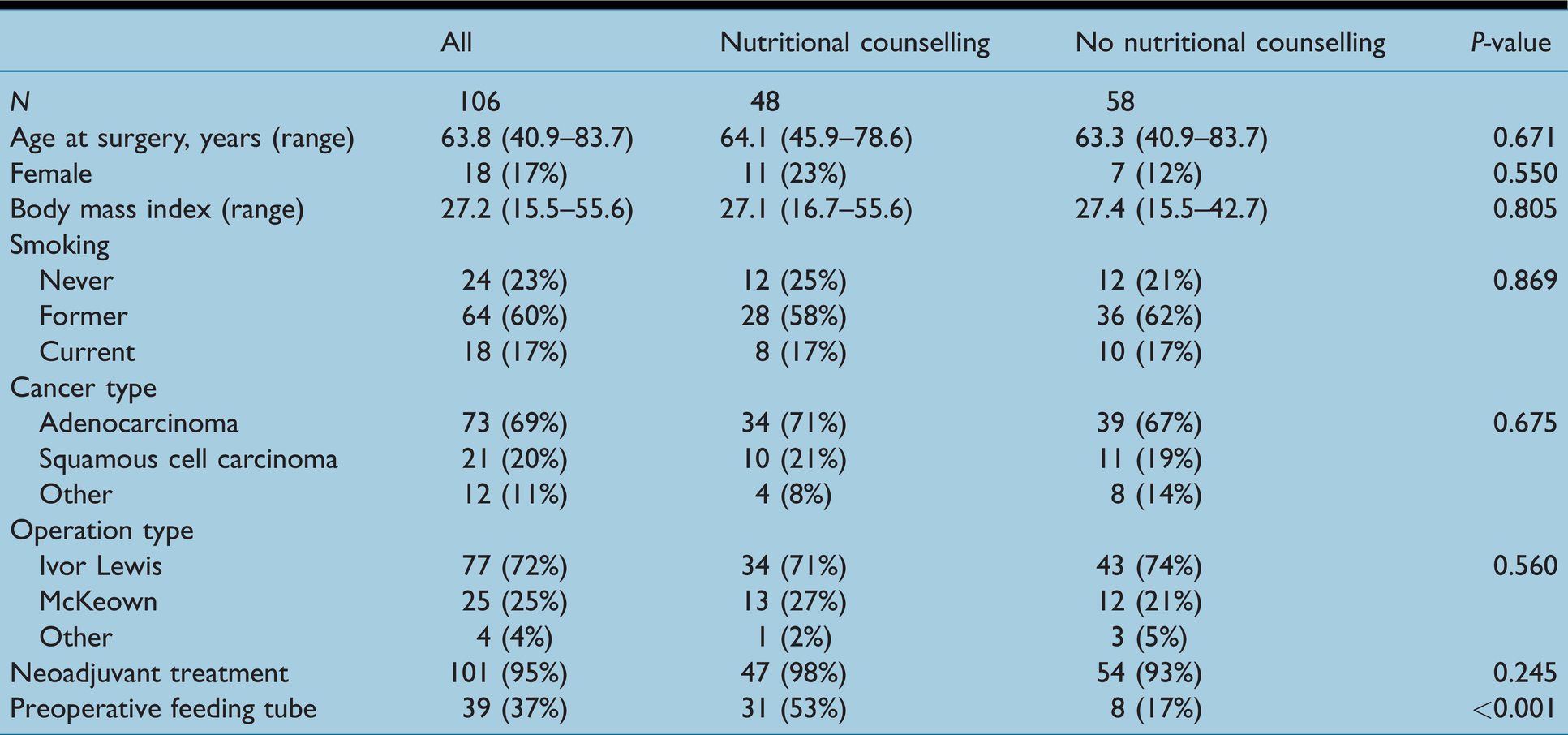
Baseline characteristics of the sample and of each group were compared. Both groups of patients were similar with respect to age, gender, smoking status, cancer type, type of operation, and neoadjuvant treatment (Table 2). The only identified difference between the two groups was having a feeding tube preoperatively, which was most commonly a gastrostomy tube. Patients in the counselling group were more likely to have had a feeding tube (P ≤ 0.05).
Baseline characteristics of all patients, those who received counselling, and those who received no counselling.
Outcomes of patients in each group (preoperative counselling versus no preoperative counselling) were compared (Table 3). Per cent weight change from the initial weight to the weight at the first postoperative visit was significantly less in patients who received preoperative counselling with any dietitian (6.29% vs. 8.71%, P = 0.036). There was a trend towards a decreased LOS in patients who received preoperative nutritional counselling (17.41 ± 10.65 days vs. 21.82 ± 15.81 days, P = 0.130), but the difference did not meet statistical significance. Nutrition-related readmissions were not significantly different (6.67% vs. 13.79%, P = 0.205). Mortality was not significantly different between groups (P = 0.753).
Comparison of outcomes of patients who did and not receive preoperative nutritional counselling.

Among the 106 patients in the study, there were 26 readmissions (24.5%) within 30 days of discharge. In the nutritional consultation group, there were zero readmissions for feeding tube problems. In the group who did not receive counselling, there were six readmissions for feeding tube problems (P ≤ 0.001).
We performed post hoc analysis to analyse the effects of preoperative tube feeding on outcomes. There was no significant difference in weight change between patients who had a feeding tube preoperatively (P = 0.090). There was also no difference in mean LOS (P = 0.820), 30-day readmission related to nutrition (P = 0.719), or 90-day mortality (P = 0.432).
Discussion
This study addresses the knowledge gap of surgical outcomes from implementation of nutritional counselling by a specialized clinical dietitian into oesophageal cancer care in the preoperative setting. We observed a statistically significant improvement in weight in patients who received preoperative nutritional counselling. A trend toward decreased LOS was also observed but did not reach significance. Post hoc analysis showed that fewer patients who had received nutritional counselling were readmitted for jejunostomy tube malfunction.
While others have described improved outcomes with surgical patients who receive preoperative nutritional counselling (Daphnee et al 2018, Ehresman et al 2020, Novelli et al 2020), we analysed the impact of this intervention specifically in oesophageal cancer patients who were intended to undergo resection. In comparing the groups who did and did not receive counselling, we found that they were also different in terms of preoperative feeding tube placement. This led us to complete further analysis, which indicated that having a feeding tube did not have an independent significant effect on outcomes. More data are needed to explore the benefits of various combinations of nutritional intervention.
A previous report by Ligthart-Melis et al (2013) described improved clinical markers with general surgical patients who receive preoperative nutritional counselling, but our report is different in several ways. First, the interventions were not identical. Our independent variable was whether a patient met with and received counselling by a dietitian preoperatively. This was in contrast to more structured intensive nutritional support described in the previous study (Ligthart-Melis et al 2013). Second, the outcomes were not identical. Both studies found decreased weight loss, but ours did not find a significant difference in LOS, unlike the first. There are several possible explanations for the differences in outcomes, including those that related to the study intervention and those related to unexplored differences in characteristics of the patient populations.
Incorporating specialised registered dietitians into the preoperative evaluation and management of patients with oesophageal cancer is simple and inexpensive if the clinic or hospital has a dietitian on staff. It is helpful for consistency to have the same dietitians working in the thoracic surgery clinic routinely. The thoracic surgeon must initially invest some time to educate the dietitians about the oesophageal cancer disease process. Although a nutritional assessment can be performed by any licensed dietitian, knowledge of where the patient is at in the neoadjuvant treatment cycle, if indicated, may alter recommendations of the dietitian. Therefore, it is important to explain the treatment algorithm by stage to the dietitian, who may not be familiar with the specific needs of these patients. The surgeon must also take time to explain to the dietitian how the anatomy is altered after oesophagectomy and the impact of the operation on the patients’ diet thereafter. In our experience, this process of familiarising the dietitian with oesophageal cancer patients’ needs requires little time. After working together with just a few patients, the dietary consultation becomes more seamless. Online resources and support groups are also now readily available to help educate the dietitian as to how to better help oesophageal cancer patients. Dietitians who have experience on surgical wards and knowledge of feeding tubes are likely to be most suited to the thoracic surgery clinic, but we have been able to help patients using dietitians who work primarily in outpatient settings, such as radiation oncology, who see more patients with oesophageal cancer that are not suitable for surgery. Once the dietitian becomes proficient with the basics of oesophageal cancer and knows which questions are important regarding dysphagia, diet, and weight loss, then the dietitian’s assessment, recommendations, and teaching can take less than 20 minutes in the outpatient setting. Although having a dietitian who can meet with patients in person is desirable, a phone interview with the patient asking questions about their oral intake, weight, and nutritional parameters is enough to allow the dietitian to make recommendations. If the same dietitian who sees the patient preoperatively can see the patient post operatively, then an appreciation for the needs of the patients who undergo oesophagectomy can be fully realized. In the US, some insurance companies reimburse for dietary consultations (Current Procedural Terminology code 97802 for initial consultation, 97803 for follow up), which can defray institutional costs of employing the registered dietitian.
Limitations of our study include that it was a single centre analysis, that it was performed in retrospect without randomisation, and that charts were reviewed by a single individual. Our study may be susceptible to bias related to time; most of the patients in the nutritional counselling group were treated later than the control group. This could correlate with general changes in practice over time, or with improvements in outcomes as experience with the operation increased. Obtaining patient weights and accurate documentation in the medical record is dependent on those health care providers who do so. It could be considered a limitation that we evaluated a small number of patient factors and outcomes. We simplified our data collection to focus on specific, widely used variables that would allow us to determine whether our intervention had a clinically measurable effect. Studies that use similar methods but incorporate additional variables will be important in the future.
Discussion of feeding tube placement, both preoperatively and postoperatively, is important for interpretation of our study results. The group who received counselling had a higher rate of preoperative feeding tube placement. A possible explanation for this could be based on referring provider preference, as the treating medical oncologists at our institution typically request feeding tube placement before starting neoadjuvant therapy, regardless of the patient’s degree of dysphagia. At our institution, patients often have a gastrostomy tube placed by a gastroenterologist or interventional radiologist prior to initial consultation with the thoracic surgeon. Interestingly, some patients in our study had gastrostomy tubes placed preoperatively and never used them during neoadjuvant treatment (data not shown). Post hoc analysis of our data showed that the intervention of preoperative gastrostomy tube placement as an independent variable did not have a statistically significant effect on weight change, nor did it have an effect on LOS, readmissions, or mortality in our study. Previous studies have shown that preoperative feeding tubes are safe and may have nutritional benefit (Bhatti et al 2015, Siddique et al 2019). However, there is currently no universal standard of care regarding preoperative feeding tube placement or use before oesophagectomy (Huddy et al 2018). Future studies should consider the role of feeding tubes in the neoadjuvant setting, alone and in combination with other interventions, such as nutritional counselling.
All patients who undergo oesophagectomy at our institution have a feeding jejunostomy placed at the time of oesophagectomy, which may affect the rate at which patients return to preoperative weight. This could limit the generalizability of our study. Individual institutions vary in preference for or against routine jejunostomy placement at the time of oesophagectomy (Álvarez-Sarrado et al 2019, Ireland & Jaunoo 2020, Purkayastha et al 2019). The optimal route of nutrition immediately postoperatively after oesophagectomy remains to be determined (Carroll et al 2020, Holmén et al 2020, Zheng et al 2021). Current data suggest that an individualized approach to postoperative nutrition that accounts for patient nutritional status and surgery technique should be used (Zheng et al 2019). One of the most common reasons for return to the emergency department following oesophagectomy is jejunostomy tube problems (Kidane et al 2018). In our study, there were no readmissions for jejunostomy tube malfunction in the group that received preoperative nutritional counselling, which included explanation and written literature about jejunostomy tube use postoperatively.
Overall LOS in all patients was higher in our study than previously published by others (Chen et al 2016, Goel et al 2020). We used mean LOS for each group for analysis, so the values were likely skewed by a few patients with extended LOS, but the following additional reasons could have also contributed. Most patients (>95%) had an open approach to their oesophagectomy, which may impact LOS (Biere et al 2012, Nason 2016). The average body mass index (BMI) of our sample was high, which has been associated with increased incidence of some postoperative complications (Gao et al 2018, Mengardo et al 2018), which also impact LOS. Our patients live in a rural state and often have poor access to medical care. Our group performs the majority of oesophagectomies in the state, yet less than 10 per cent of patients live within 80 kilometers (50 miles) of our medical centre. Thus, we choose to keep patients hospitalised slightly longer than most to ensure all medical and surgical issues had resolved at time of discharge. Longer LOS can be associated with reduced rates of readmission (Sundaram et al 2015). We are working to implement enhanced recovery pathways to lessen our LOS while providing the same rate of readmission.
Future aims include analysis of patient factors that could be associated with benefit from nutritional counselling, including socioeconomic status, BMI, ideal body weight, location and stage of cancer at diagnosis, nutritional labs, and weight lost at the time of diagnosis. Additionally, cost-benefit analysis could demonstrate the cost-effectiveness of nutritional counselling, particularly regarding readmissions. The cost of readmission following oesophagectomy was estimated to be £6,850 (US$9660)* in an analysis of patients readmitted between 2010 and 2014 (Goel et al 2020). Nutritional interventions involve relatively small financial investments, so strong evidence that these interventions impact readmissions could be impactful. Other important focuses that continue to evolve include specific dietary interventions, such as immunonutrition (Kanekiyo et al 2019) and high-protein diets (Ligthart-Melis et al 2013, Steenhagen 2019) and screening methods and prognostic tools for predicting malnutrition and related complications (Nakatani et al 2017).
Our study supports the practice of routine dietary counselling from specialized dietitians in the preoperative period for patients undergoing oesophagectomy. This intervention is supported by evidence and international guidelines, cost of the intervention is low, and there is essentially no risk to the patient. Based on our findings, we plan to continue using preoperative counselling with specialised registered dietitians for all preoperative oesophageal cancer patients undergoing oesophagectomy. The specifics of nutritional interventions are likely best if customized for each surgeon’s practice. Several aspects should be considered, including patient population (access to care, average BMI, etc.), practice type, and other factors associated with patient, surgeon, and practice. We will consider expanding and improving our methods of nutritional counselling, including incorporating telephone and videoconferencing sessions after patients’ initial in-clinic visit in order to more closely follow their progress.
Key phrases
Oesophageal cancer patients treated by oesophagectomy are at high risk of malnutrition.
Preoperative nutritional consultation is an inexpensive and low-risk intervention.
We compared patients who did and not receive nutritional counselling by dietitians.
Patients who received nutritional counselling had improved short-term outcomes.
Nutritional counselling should be part of preoperative care before oesophagectomy.
Footnotes
Acknowledgments
Data for the study were provided by the Arkansas Clinical Data Repository (AR-CDR) maintained by the Department of Biomedical Informatics in the College of Medicine at the University of Arkansas for Medical Sciences (UAMS). The AR-CDR is approved to operate as an enterprise data resource to support research across UAMS. Data in the AR-CDR comes from UAMS Electronic Medical Record (EMR), tumour registry, billing, and cancer genomic data and comprises encounters since 05/01/2014.
Competing interests
No competing interests declared.
Funding
None declared.
Contributorship
MAG performed the literature search, data collection, analysis and interpretation, and writing the manuscript. JLM conceived of the project and oversaw study design, data interpretation, analysis, and writing. RJR performed statistical analysis and editing. PCC contributed to study design and conceptualization. KWS participated in the study design and data interpretation. KAM and MAS contributed to conceptualization of the project, as well as data interpretation. All authors were involved in drafting the manuscript.