
Abstract
Upper abdominal surgeries are associated with postoperative pulmonary complications. This study aimed to evaluate the effectiveness of preoperative chest physiotherapy on the clinical outcome in upper abdominal surgery patients. Fifty patients were equally randomised into control (general care) and intervention (preoperative chest physiotherapy) groups. Forced vital capacity, forced expiratory volume, incidence of postoperative pulmonary complications, duration of surgery and days spent in intensive unit care were recorded. The intergroup difference in the spirometric values was significant post-surgery. A total of 11 patients experienced postoperative pulmonary complications. Significant difference in the mean duration of surgery and duration of stay in the intensive care unit in both the study groups was observed. Incidence of postoperative pulmonary complications was significantly associated with number of days spent in the intensive care unit. Significant increase in the spirometric values post-surgery in the intervention group implies the importance of preoperative chest physiotherapy in reducing postoperative complications.
Introduction
Upper abdominal surgeries (UASs) are associated with high-risk postoperative pulmonary complications (POPCs), resulting in clinically significant disease or dysfunction, thereby adversely affecting the clinical course (Mohamady et al 2016). The reported incidence of POPCs ranges between 10 and 50% of patients (Boden et al 2018). Factors contributing to POPCs are anaesthesia, surgical duration (including estimated bleeding ≥500mL), perioperative blood transfusion, depressed mucociliary clearance, nociception impaired respiratory function, reduced lung volumes, anxiety levels of the patient and postoperative pain (Kodra et al 2016, Lunardi et al 2015, Patman 2017, Possa et al 2014, Yang et al 2015).
Multidisciplinary management commonly employed in preventing POPCs include enhanced recovery pathways, epidural analgesia, goal-directed fluid therapy, preoperative smoking cessation, early mobilisation, early extubation drug therapy optimisation and physiotherapy programmes (respiratory muscle training, neuromuscular electrical stimulation, breathing exercises) that result in early recovery of a patient after abdominal surgery (Abdelaal et al 2017, Makhabah et al 2013, Odor et al 2020). In response to deteriorating respiratory functioning, postoperative ventilatory support and inhaled therapies (in addition to usual drugs) are implemented. Beneficial POPC outcomes have been reported when using epidural analgesia and lung protective ventilation (Odor et al 2020). However, one of the widely accepted management programmes is physiotherapy (preoperative and postoperative) that aims to reduce the risk of POPCs by monitoring and reducing the risk factors, encouraging cessation of smoking, patient education and improving preoperative, intraoperative and postoperative pulmonary care (Makhabah et al 2013, Rodrigues 2018). This improves the patients’ quality of life and residual function along with avoiding frequent hospital visits post-surgery. These programmes are cost-effective therapeutic modalities that decrease complications and the patient’s dependency on a ventilator (Makhabah et al 2013).
Preoperative chest physiotherapy has earlier been reported to reduce incidence of POPCs, improve respiratory muscle strength and oxygen–haemoglobin saturation, and aid mobilisation post-abdominal surgery (Manzano et al 2008, Rodrigues 2018). The timing of initiating breathing exercises could be improved by educating patients and training them before surgery, so that they can perform these exercises immediately post-surgery to prevent POPCs (Boden et al 2018). Few studies have reported that preoperative education and breathing exercise training alone are associated with a 75% relative risk reduction and absolute risk reduction of 20% in POPCs (Boden et al 2018, Samnani et al 2014). The Lung Infection Prevention Post Surgery Major Abdominal with Pre-Operative Physiotherapy (LIPPSMAck-POP) trial aimed at testing a hypothesis that patient preoperative education and breathing exercise training within six weeks of surgery by physiotherapists reduces the incidence of POPCs after UAS (Boden 2018).
Chest physiotherapy employs the incentive spirometer, a lung expansion technique which is a relatively simple and safe method designed to induce sighing or yawning by encouraging the patient take in long, slow deep breaths, thereby encouraging the patient to achieve a pre-set volume or flow (Graham et al 2019, Kumar et al 2016). These exercises are also employed to assess lung function and to educate the patients preoperatively of their lung capacity. Patients can be motivated to reach the similar point postoperatively with continuing physiotherapy exercises.
The two spirometric variables commonly measured are, forced vital capacity (FVC) – the total volume of air forcibly exhaled in one breath (normal range: >80%) and forced expiratory volume in one second (FEV1) – the volume of air exhaled in the first second of forced expiration (normal range: >80%). This is known as the FEV1/FVC ratio (forced expiratory volume in one second over forced vital capacity (Tiffeneau-Pinelli index)) – the percentage of the FVC expired in one second (normal ratio: 0.7–0.8) (GOLD 2021). Disproportionate reduction in the FEV1 as compared to the FVC is reflected in the FEV1/FVC ratio and is the hallmark of obstructive lung diseases. Reduction in the FVC with a normal or elevated FEV1-to-FVC ratio should trigger further evaluation of total lung capacity (TLC) to rule out restrictive lung disease. Lower FVC is an independent risk factor for postoperative pulmonary infection, prolonged intensive care unit (ICU) stay and in-hospital death regardless of airflow limitation. Lower FEV1 is also an independent risk factor for postoperative infection (Park et al 2020).
In India, there is limited evidence that supports the use of incentive spirometry and breathing exercises, and studies here have focused on employing preoperative physiotherapy programmes to manage thoracic and upper gastrointestinal tract surgeries but few have employed the same for abdominal surgeries (Kale et al 2017, Kamarajah et al 2019, Kumar et al 2016, Sultanpuram et al 2016). The purpose of this study was to therefore assess the role of chest physiotherapy preoperatively in conjunction with incentive spirometry in relation to early surgical outcomes and recovery following UASs.
Methodology
Study design
The prospective interventional case–control study was conducted at a tertiary healthcare centre in Bengaluru, Karnataka, India, between January 2016 and July 2017. Approval from the Institutional Ethics Committee (STD-1/EC/034/2015) and written informed consent from participants were gained before the commencement of the study.
Study subjects
Patients aged between 18 and 80 years, scheduled to undergo primary UAS and elective midline laparotomy and ASA grade 1–3 classification were invited to take part in the study. Patients with any existing respiratory system disorder and those who had undergone abdominal surgery before were excluded.
The sample for the study was calculated based on the study conducted by Manzano et al (2008) where the control and chest physiotherapy groups presented decreased spirometry values post-surgery, but without any difference between them. The FVC was from 83.5 ± 17.1% to 62.7 ± 16.9% in the control group and from 95.7 ± 18.9% to 79.0 ± 26.9% in the study group. Therefore, by considering an effect size 0.6%, power of 90% and error of 5%, sample size was estimated at 50 for this study.
Study procedure
The patients in the study were divided into two groups by block randomisation method: control (n = 25, patients treated with standard care) and intervention group (n = 25, patients underwent chest physiotherapy preoperatively). All patients were thoroughly examined preoperatively by clinical, laboratory and radiological assessments. The smoking status of all patients was recorded. Blood investigations, chest X-rays and spirometry were conducted preoperatively and postoperatively. Postoperative spirometry was conducted on 15th day post-surgery. For spirometry, the technical procedures and the reproducibility and acceptability criteria were as per those recommended by the American Thoracic Society (Graham et al 2019). The variables recorded during spirometry were FEV1, FVC and FEV1/FVC ratio. The spirometry readings were recorded by a trained nurse in the respiratory clinic. The preoperative spirometry values were derived in preoperative clinic within the week prior to the surgery. Postoperative spirometry was done on the 15th day. Predicted normal values considered were as per Knudson et al (1976). The duration and type of procedures were recorded.
Patients in the intervention group underwent chest physiotherapy preoperatively. The chest physiotherapy methods included incentive spirometry; passive and localised exercises – localised breathing exercises associated with manual pressure performed by the physiotherapist on patients’ chest wall during expiration; deep diaphragmatic breathing – slow deep inspiration, where the patient was asked to expand the diaphragmatic region; followed by chest expansion exercises – deep inspiration followed by a three-second pause at maximal inspiratory volume attained, and then slow expiration (Manzano et al 2008).
These exercises were started at least two days prior to the scheduled surgery. The study was initiated with chest physiotherapy five days prior to the surgery and two patients had their surgery preponed for which they had only two days of preoperative chest physiotherapy. Physiotherapy was administered on an outpatient basis until the day before when they were admitted. Physiotherapy was performed for 30min, twice a day, under the supervision of a physiotherapist. Incentive spirometry was done at least five times in a day for a period of 3 to 4min each session with at least 1h gap between sessions. These sessions were unmonitored except when they were initially demonstrated and performed under observation on the first day following initial patient education.
Postoperatively, the chest physiotherapy was administered in graded manner with initiating diaphragmatic breathing, inspiratory holding followed by slow sustained exhalations by trained physiotherapists. Patients in the both the groups were examined for a period of 30 days. After discharge, patients were evaluated on an outpatient basis. POPCs were noted based on clinical status, chest X-ray and arterial blood gas analysis. The inpatients were physically examined for chest complications including overall outcome. The follow-up was noted on the day of surgery, at third and seventh postoperative day and at 15th day for postoperative spirometry values and at 30th day to determine their overall improvement. The examination included a thorough physical examination of the chest along with temperature recording and oxygen saturation using pulse oximetry. Patients suspected of atelectasis or consolidation underwent repeat chest X-ray.
Statistical analysis
Data was analysed using statistical software R version 3.6.3. As the data was normally distributed, Student t-test (two tailed, independent) was used to find the significance of study parameters on continuous scale between two groups (inter group analysis) on metric parameters, and Student t-test (two tailed, dependent) was used to find the significance of study parameters on continuous scale within each group. Chi-square/Fisher Exact test was used to find the significance of study parameters on categorical scale between the two groups. Level of significance was set at p ≤ 0.05.
Results
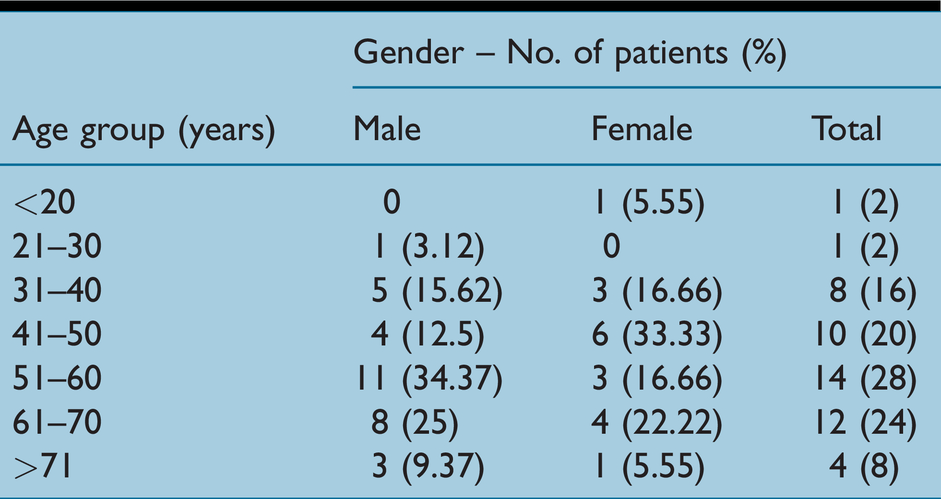
The mean age of the patients in this study was 53.5 ± 12.92 years. A greater number of patients belonged to the age group of 51–60 years (n = 14, 28%). Ten (26%) patients belonged to ASA grade 1, 27 (54%) to grade 2 and 13 (20%) to grade 3 classifications. The demographic data is presented in Table 1.
Demographic data of the study population
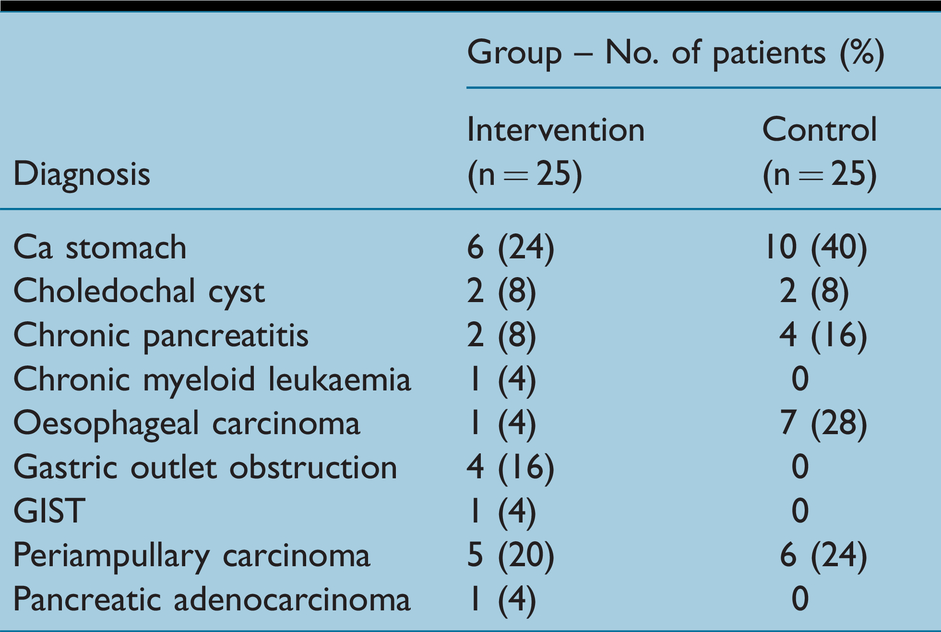
The procedures the patients underwent included Whipples surgery, hepatojejunostomy, jejuno-jejunostomy, partial gastrectomy or resection and anastomosis of small bowel, removal of gall bladder or oesophagectomy combined through abdominal and thoracic approach. The majority of patients were diagnosed with stomach cancer, followed by periampullary carcinoma and oesophageal cancer (Table 2).
Distribution of patients based on diagnosis
The association between the groups and preoperative FEV1, FVC and FEV1/FVC range were insignificant (p > 0.05). However, the association between the groups and postoperative FEV1 (p = 0.002), FVC (p = 0.02) and FEV1/FVC (p = 0.006) range were significant (Table 3).
Association of the preoperative and postoperative spirometry variables amongst the study population
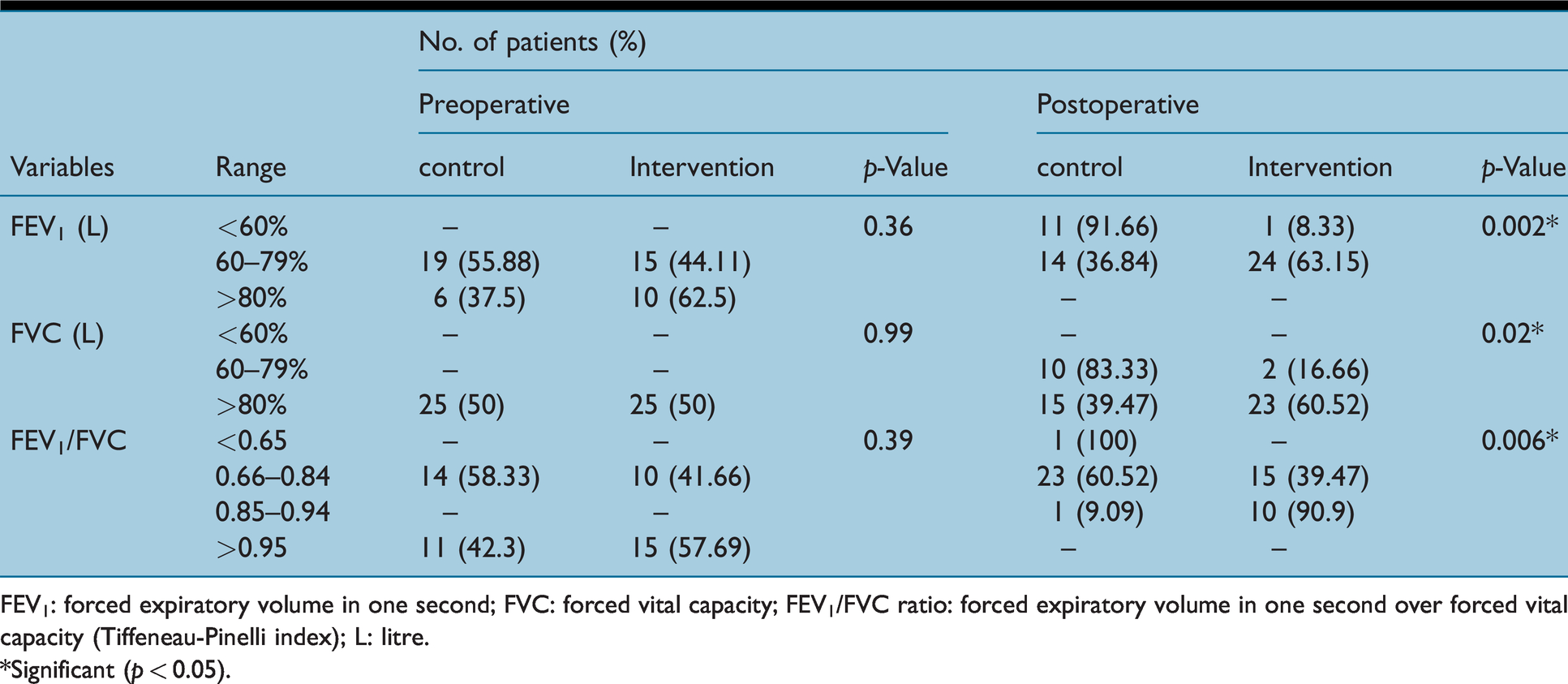
FEV1: forced expiratory volume in one second; FVC: forced vital capacity; FEV1/FVC ratio: forced expiratory volume in one second over forced vital capacity (Tiffeneau-Pinelli index); L: litre.
*Significant (p < 0.05).
With respect to the clinical outcome, significant differences between control and intervention group patients were observed for post-FEV1 (p = 9.23 × 10−5), post-FVC (p = 0.0008), pre-FEV1/FVC (p = 0.04) and post-FEV1/FVC (p = 0.002) values (Table 4).
Consolidated spirometry values in the study population
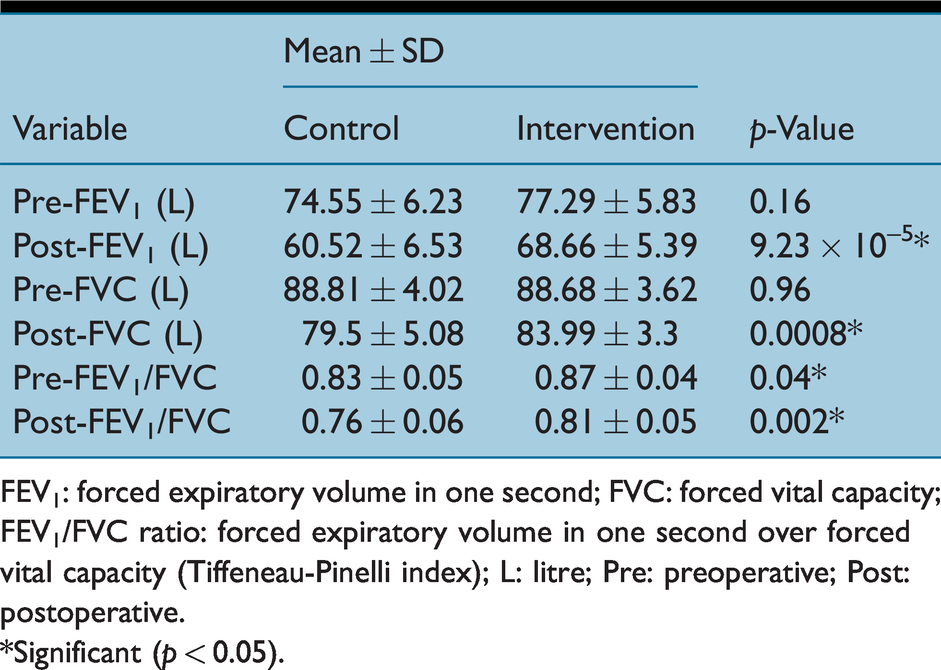
FEV1: forced expiratory volume in one second; FVC: forced vital capacity; FEV1/FVC ratio: forced expiratory volume in one second over forced vital capacity (Tiffeneau-Pinelli index); L: litre; Pre: preoperative; Post: postoperative.
*Significant (p < 0.05).
A total of 11 (22%) patients had POPCs, out of which, six (54.54%) patients were <60 years old. However, the association of POPCs with respect to age was insignificant (p = 0.47). In the control and intervention groups, POPCs were observed in nine (18%) and two (4%) patients, respectively. In the control group (n = 9), seven patients were female (77.77%) and two were male (22.22%), whereas both the patients in the intervention group were males. The association of the group and POPCs was significant (p = 0.04). However, association of POPCs and gender was insignificant (p = 0.07).
The difference in the mean duration of surgery between patients in the control group (197.6 ± 43.32min) and that in the intervention group (175.2 ± 41.44min) was significant (p = 0.04). The mean duration of surgery for patients with POPCs is (230.9 ± 22.56min) and without any POPCs is (173.84 ± 39.57min). The incidence of POPCs was significantly associated with the duration of surgery (p = 0.0002).
The difference in the ICU stay between patients in the control group (4.16 ± 1.37 days) and that in the intervention group (2.88 ± 0.97 days) was significant (p = 0.0006). The incidence of POPCs was significantly associated with the number of days patients spent in the ICU (p = 4.7 × 10−9) (Figure 1).
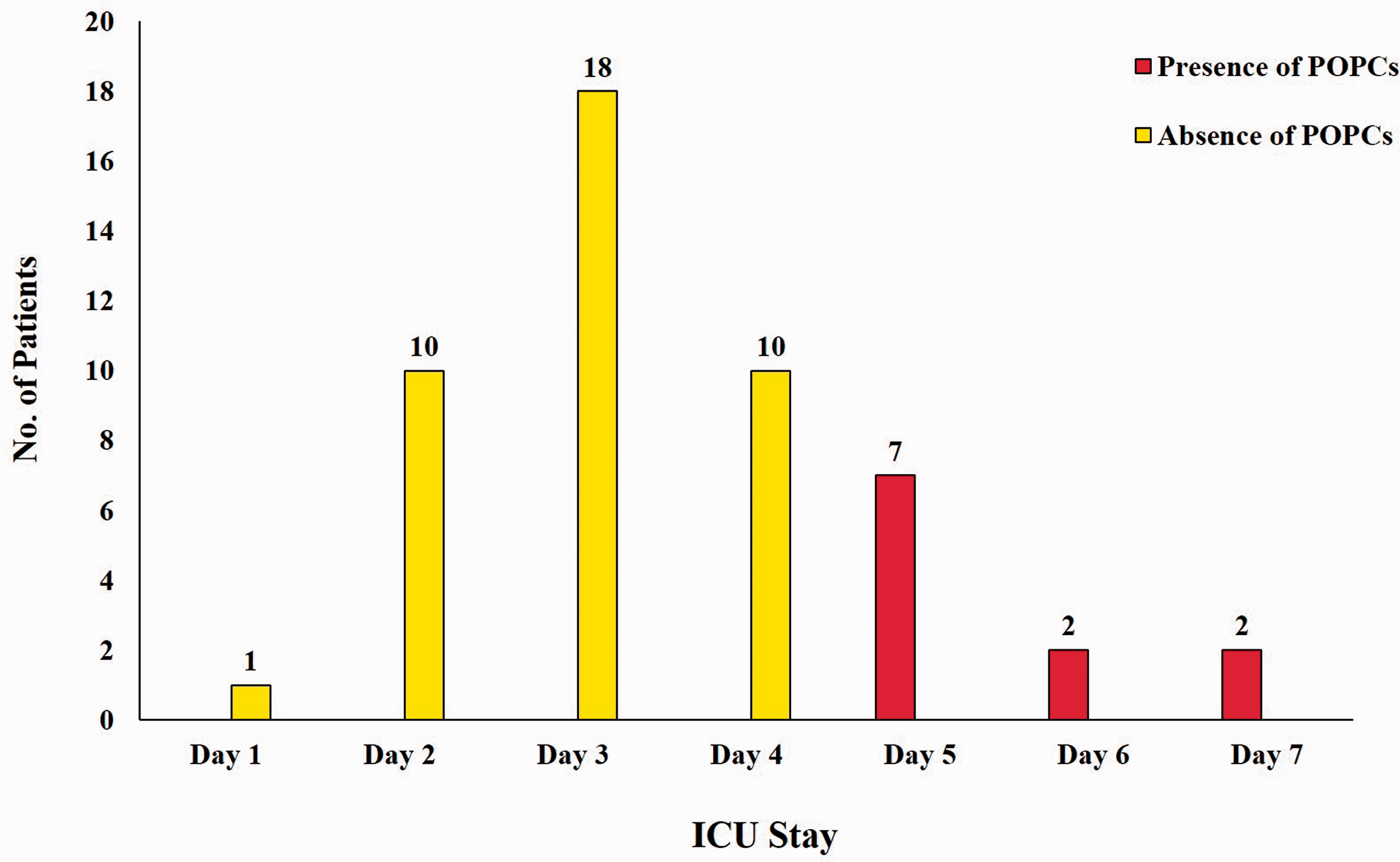
Association of POPC incidence in patients with ICU stay
Amongst the patients with POPCs (n = 11), one (9.09%) belonged to ASA grade 1, six (54.54%) to grade 2 and four (36.36%) to grade 3 classifications. History of smoking was noted in three (27.27%) patients who experienced POPCs and in ten (25.64%) patients who had no POPCs. Smoking history and POPC incidence showed no significant association (p = 0.99).
The difference in the duration of hospital in the control group (14.24 ± 4.58 days) and intervention group (11 ± 3.24 days) was significant (p = 0.005). The duration of stay in the hospital for patients who had POPCs (n = 11) was 11–15 days for two (18.18%) patients, 16–20 days for five (45.45%) and 21–25 days for four (36.36%) of them. For those who had no POPCs (n = 39), the stay was <10 days for 13 (33.33%) patients, 11–15 days for 15 (38.46%), 16–20 days for four (10.25%) and 21–25 days for seven (17.94%) of them. The association between the incidence of POPCs in patients and duration of their stay in the hospital was significant (p = 0.007).
With respect to pre and post-UASs, the difference in the mean spirometric values and other variables such as POPC cases, duration of surgery, stay in the ICU and hospital between the control and intervention groups was significant (p < 0.05) (Table 5).
Spirometry and other variables in the study groups before and after surgery
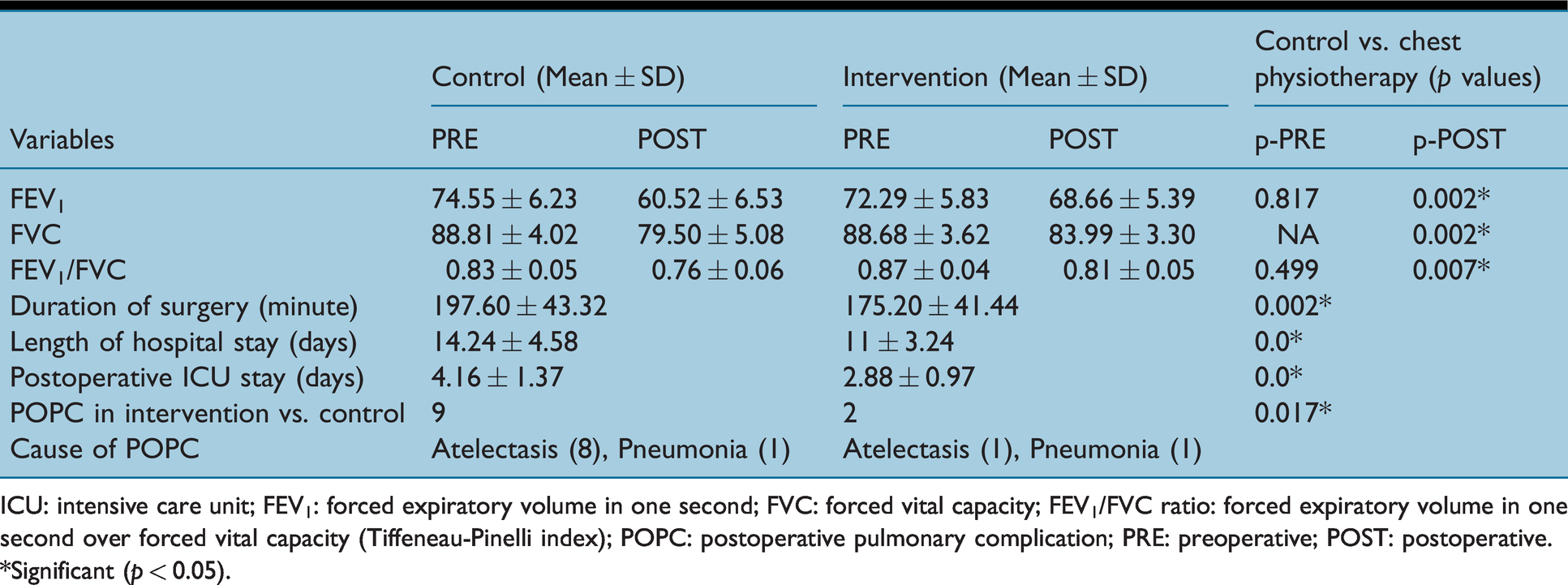
ICU: intensive care unit; FEV1: forced expiratory volume in one second; FVC: forced vital capacity; FEV1/FVC ratio: forced expiratory volume in one second over forced vital capacity (Tiffeneau-Pinelli index); POPC: postoperative pulmonary complication; PRE: preoperative; POST: postoperative.
*Significant (p < 0.05).
Discussion
UASs are the most frequent surgeries performed in developed countries (Weiser et al 2008). With UAS, comes POPCs, which is the most common serious complication post-surgery, strongly associated with increased morbidity, healthcare cost and mortality (Boden et al 2018, Fernandez-Bustamante et al 2017, LAS VEGAS Investigators 2017). Therefore, this study aimed to evaluate the clinical outcome of adult patients undergoing preoperative chest physiotherapy in primary elective UASs.
A greater number of patients belonged to the age group of 51–60 years. The patients, divided into control and intervention groups, were measured for their lung function pre and post-surgery. The different techniques of chest physiotherapy, either conventional, modern or instrumental, mainly assist the clearance of inflammatory exudates and tracheobronchial secretions, thereby decreasing airway resistance, improving gas exchange and making breathing easier (Chaves et al 2019, Morrison & Innes 2017, Roqué i Figuls et al 2016). The significant association between the groups and outcome and the significant difference in the range of spirometry parameters measured postoperatively such as FEV1 (p = 0.002), FVC (p = 0.02) and FEV1/FVC (p = 0.006) can be attributed to the implementation of chest physiotherapy.
Significant increase (p < 0.05) in the post-FEV1, post-FVC, pre and post-FEV1/FVC values were observed in the intervention group patients in comparison to the control group patients. However, Manzano et al (2008) reported insignificant (p > 0.05) increase in the postoperative values of FVC, FEV1 and FEV1/FVC between the control and intervention groups, with chest physiotherapy being performed post-surgery. The mean ratio of FEV1/FVC was well within the normal range for the patients in this study.
After major surgery, restoring the normal alveolar-to-arterial oxygen difference takes time, usually a few days, where hypoxaemia is a common occurrence. Within 24 to 48h post-UAS, the functional residual capacity reaches its lowest value and slowly returns to normalcy in one week’s time. During this time, atelectasis is also commonly seen and persists for at least 24h in most patients having major surgery, thereby making them more prone to POPCs (Miskovic & Lumb 2017). In this study, nine out of 11 patients who experienced POPCs were from the control group. The decrease in the number of patients experiencing POPCs could be attributed to the chest physiotherapy that the patients underwent prior to their scheduled surgery. In earlier conducted studies, the time point in initiating breathing exercises as part of the preoperative chest physiotherapy programme has been associated with reduction in the incidence of POPCs, which is in accordance with our results (Boden et al 2018, Patman et al 2017, Samnani et al 2014).
In our study, we concluded that POPC are more common in female patients and that the female sex is an independent risk factor for postoperative pulmonary events. Other variables like age >60 years and smoking does not increase POPC. Sakai et al (2007), however, concluded that in UASs under general anaesthesia, female sex, age >70, COPD and smoking were independent risk factors for intraoperative and postoperative pulmonary events.
The preoperative or the contributing factors for POPCs include age, positive for cough test, history of smoking, obesity, general health, asthma, chronic obstructive pulmonary disease and sleep apnoea (Kelkar 2015). Other contributing surgical factors for POPCs are type of surgery, duration, reoperation, type of anaesthesia and blood transfusion (Kelkar 2015, Miskovic & Lumb 2017). These factors might explain for the increased duration of surgery for the patients who experienced POPCs in comparison to those patients experiencing no POPCs in this study. The incidence of POPCs was significantly associated with the duration of surgery (p = 0.0002). Similar significance was also reported by Jin et al (2015) (p < 0.001). However, Owen et al (2013) reported independent association of the duration of surgery with increased risk of POPCs in laparoscopy and open colectomy. The risk of POPCs appeared to increase with every additional minute of operating time independent of other factors (odds ratio 1.01, 95% confidence intervals 1.00–1.02, p = 0.007). POPCs significantly increase the length of hospital stay (ten vs three days).
The difference in the ICU stay between the two groups was significant (p = 0.0006), with a longer ICU stay in the control group. The incidence of POPCs was also significantly associated with the number of days spent in ICU. This showed that physiotherapy in the intervention group promoted better recovery and was effective in decreasing the number of days required in the ICU post-surgery. The history of smoking in patients was insignificantly associated with the incidence of POPCs in our study (p = 0.99), whereas Sever et al (2016) reported a significant association (p = 0.02).
The overall duration of surgery, ICU and hospital stay in the intervention group patients were less in comparison to the control group patients, this could be attributed to the preoperative chest physiotherapy. Most of the patients had a prolonged stay in the hospital for up to 25 days as they had major diseases including malignancies, prolonging their post-operative recovery.
Limitations of this study are small sample size, reduced number of pre-surgery chest physiotherapy sessions and shorter duration of monitoring patient's postoperative follow-up. Education programmes should also be reviewed to ensure they explain and help patients understand and to spread awareness of the importance of chest physiotherapy for patients undergoing UAS.
Conclusion
We determined that preoperative chest physiotherapy is important in preventing POPCs, improving the clinical outcome of patients undergoing UASs. Female gender and prolonged surgeries are both risk factors. Age and smoking did not seem to contribute to POPCs in our study. However, further research is required to validate our findings.
No competing interests declared.