
Abstract
The ‘Guinea Pig Club’ has been described as the most exclusive club in the world, but the entrance fee is something most men would care not to pay, and the conditions of membership are arduous in the extreme. The Guinea Pig Club was formed in July 1941 to support aircrew who were undergoing reconstructive plastic surgery after receiving burn injuries in the Second World War. This paper will explore the novel surgical techniques employed to treat the Guinea Pig Club members, their experiences at the hospital and their lives after the war and how Sir Archibald McIndoe and the Guinea Pig club members revolutionised burns plastic surgery as we know it today.
We are McIndoe’s army We are his Guinea Pigs With dermatomes and pedicles, Glass eyes, false teeth and wigs. And when we get our discharge We’ll should with all our might! ‘Per ardua ad astra’ We’d rather drink than fight! (Maegraith 2003: p1) The Guinea Pigs – any member of allied aircrew who had been ‘mashed, boiled or fried’ (McConville 2018: p1) and who had undergone at least two operations at the cottage Hospital, Queen Victoria Hospital, East Grinstead for burns or other crash injuries. ‘The Scientists – Doctors, Surgeons and other medical staff’. ‘The Royal Society for the Prevention of Cruelty to Guinea Pigs – Friends and Benefactors who made the life of a Guinea Pig a happy one’.
Moreover, East Grinstead Museum (2021: p1) continue and state ‘all members were to pay an annual fee of 2/6d (equivalent to 12.5 pence in today’s money). Women were not able to be members although could attend some special “ladies” evenings’. The Guinea Pig club was only intended to continue until the end of the Second World War. However, at the end of the war, there were 649 Guinea Pig Club members in total (QR Memories N/D), so it was decided to keep the club running. It went from strength to strength and will celebrate its 80th anniversary in 2021.
Born out of necessity
Medical science makes its greatest advances in the greatest time of need. One of the greatest advances of the 20th century was the speciality of plastic surgery. Plastic surgery is derived from the Greek term ‘Plastikos’, which means ‘to mould’.
Today, plastic surgery is now synonymous with cosmetic surgery. It was just a few years ago that cosmetic surgery was only available to the rich and the famous. Due to technological advances and social acceptance, cosmetic surgery is being made available to the masses to remove the ravages of time, with a nip here and a tuck there, from smoothing wrinkles on the face with an injection to a full body lift requiring major surgery. Many are, however, unaware that plastic surgery as a speciality was born in the affliction of war.
The ravages of war
During the 1930s, on the brink of the Second World War, the government was concerned about the casualties of war, in particular the large numbers of burn victims that were anticipated due to aerial combat and air raids. The Queen Victoria Hospital in East Grinstead was one of four Hospitals designated to receive and treat burns casualties and others. Three new army wooden huts were constructed and made into wards: Ward one – For dental and jaw injuries Ward two – For women and children – mostly air raid casualties Ward three – For officers and the most severely burned and injured service personnel
Thousands of Royal Air Force (RAF) and British Commonwealth aircrew, many of these young men, still in their teens, survived being shot down during flying raids over Germany or during the Battle of Britain. Many of these service men were badly burnt and transferred to the Queen Victoria Hospital, East Grinstead, Ward three. These air crash survivors often presented with horrendous burns and disfigurement. Faces were often weeping unrecognisable messes without lips, eyebrows, eyelids, noses and ears. Sometimes fingers were replaced by burnt stumps on disfigured hands. The proximity of the fuselage in planes meant that faces and hands of these airmen were particularly vulnerable due to petrol flames and bomb flashes. Treating burns was difficult due to the limited knowledge about burns casualties.
The treatment of burns prior to the Second World War
The state of plastic surgery and burns treatment prior to the Second World War was at its infancy. In 1934, five years before the outbreak of the Second World War, John Dunbar, a resident surgeon of the Royal Glasgow Infirmary conducted a study of burns patients admitted to his hospital over the last century. According to his research and analysis of Medical Research Council records (Medical Research Council 1945: p60). Of 3437 fatal cases, 65% of deaths had occurred within two days of injury. In particular, between 1937 and 1941 of 1200 burns admissions, half of deaths (49%) had occurred within twenty-four hours and 72% within three days. Only 4% of these patients received serum or plasma intravenously.
There did not seem to be any problem about the prolonged treatment of major burns because very few survived. According to Jackson (1978: p335) ‘it was not the horrific burns that led to the demise of patients, but the shock that was incurred was the commonest cause of death’.
The treatment of burns and burns shock therapy is well documented through history. However, it was two years before the Battle of Britain that Wilson et al (1938) described how burns and secondary burn shock could be treated effectively. When burns patients were admitted to hospital, immediate intravenous therapy was administered to try and improve circulation and elevate shock. This usually consisted of one or two small infusions of 400ml of gum saline or dextrose saline. Burns were then debrided and tanned under general anaesthesia. Tannic acid, known as ‘life-saving’, was applied in the form of a gel known as ‘Tannafax’ directly over the burn. This created a hard protective shell over the wound which protected against further fluid loss, relieved pain and prevented infection. Tannic acid was combined with antiseptics such as Mercuric Chloride and coal tar dyes and other coagulants such as triple dye and 10% Silver Nitrate (Ashwood & Philpott 2010). Utilising these methods had serious complications. The intravenous burn therapy saw transient improvements in patients, however, more often than not, patients’ circulation collapsed which prolonged inadequate resuscitation producing a generalised illness known as toxaemia – known today as untreated shock. Toxins absorbed from the tannic acid into the liver was also a contributing factor to circulation failure (Ashwood & Philpott 2010). If patients did survive, areas where Tannafax had been administered to the burn made reconstruction difficult due to the skin contracting. Archibald Hector McIndoe (1940), a consultant surgeon at the Air Ministry, realised that all these treatments were inadequate to deal with the horrific injuries of the airmen who were being presented for treatment. He believed in providing continuous, comprehensive care of his patients from the time of their injury to their full return to society.
Sir Archibald McIndoe
Archibald McIndoe (Figure 3) was born in 1900 and attended medical school in his native New Zealand, but later decided he wanted to develop his surgical skills. He obtained fellowship at the Mayo Clinic in San Francisco to further his studies. Initially he undertook the role of first assistant in Pathology and Anatomy, moving later into the position of assistant surgeon, where he specialised in the architecture of the liver and surgery of liver for carcinomas. He achieved fame and tenure in the United States of America, but his ultimate ambition was to move to the United Kingdom. Upon arrival in London in 1930, McIndoe found it difficult to secure employment in general surgery. By a chance meeting with his cousin Sir Harold Gillies, McIndoe was persuaded to undertake a career in plastic surgery. Upon this advice he secured a position at St Bartholomew’s Hospital in the department of plastic surgery as a clinical assistant. In 1932, he gained entry into the Royal College of Surgeons after passing the fellowship examination, whereby he obtained his first consultancy post of lecturer and general surgeon at the Hospital of Tropical Diseases (East Grinstead Museum 2021). His time spent there enabled the sharpening of skills under the supervision and mentorship of Sir Harold Gillies. Ashwood and Philpott (2010: p251) identified that ‘soon after, he was appointed as a consultant plastic surgeon, not only at St Bart’s, but other hospitals including Staffordshire Royal Infirmary and Chelsea Hospital for Women’. At the time of his appointment, plastic surgery was in its infancy as a speciality. Within the Royal College of Surgeons, there was no faculty of plastic surgery. It should be remembered that plastic surgery procedures known at that time were developed out of necessity due to the horrendous burn injuries from servicemen during the First World War. According to Ashwood and Philpott (2010: p252) ‘during this time Sir Harold Gillies was a captain in the Medical Core and has been accredited as being the first pioneer of plastic surgery’.

The Guinea Pig Club emblem
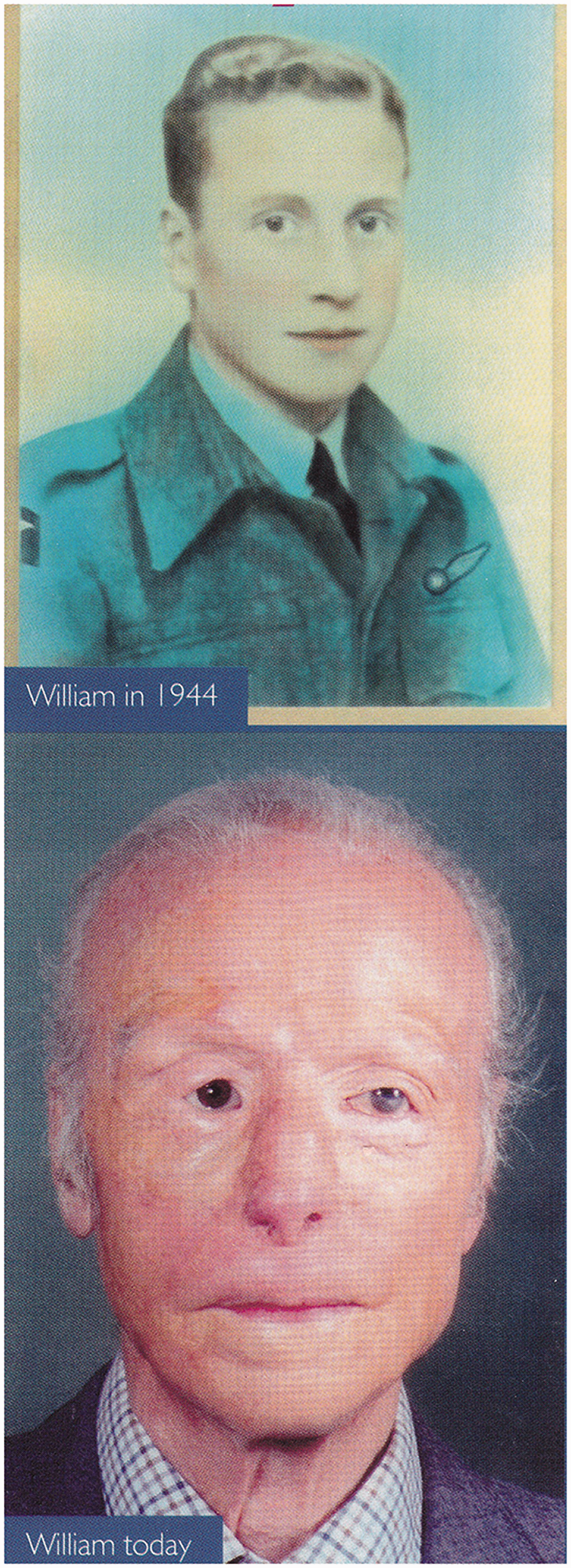
William (Bill) Foxley before and after images
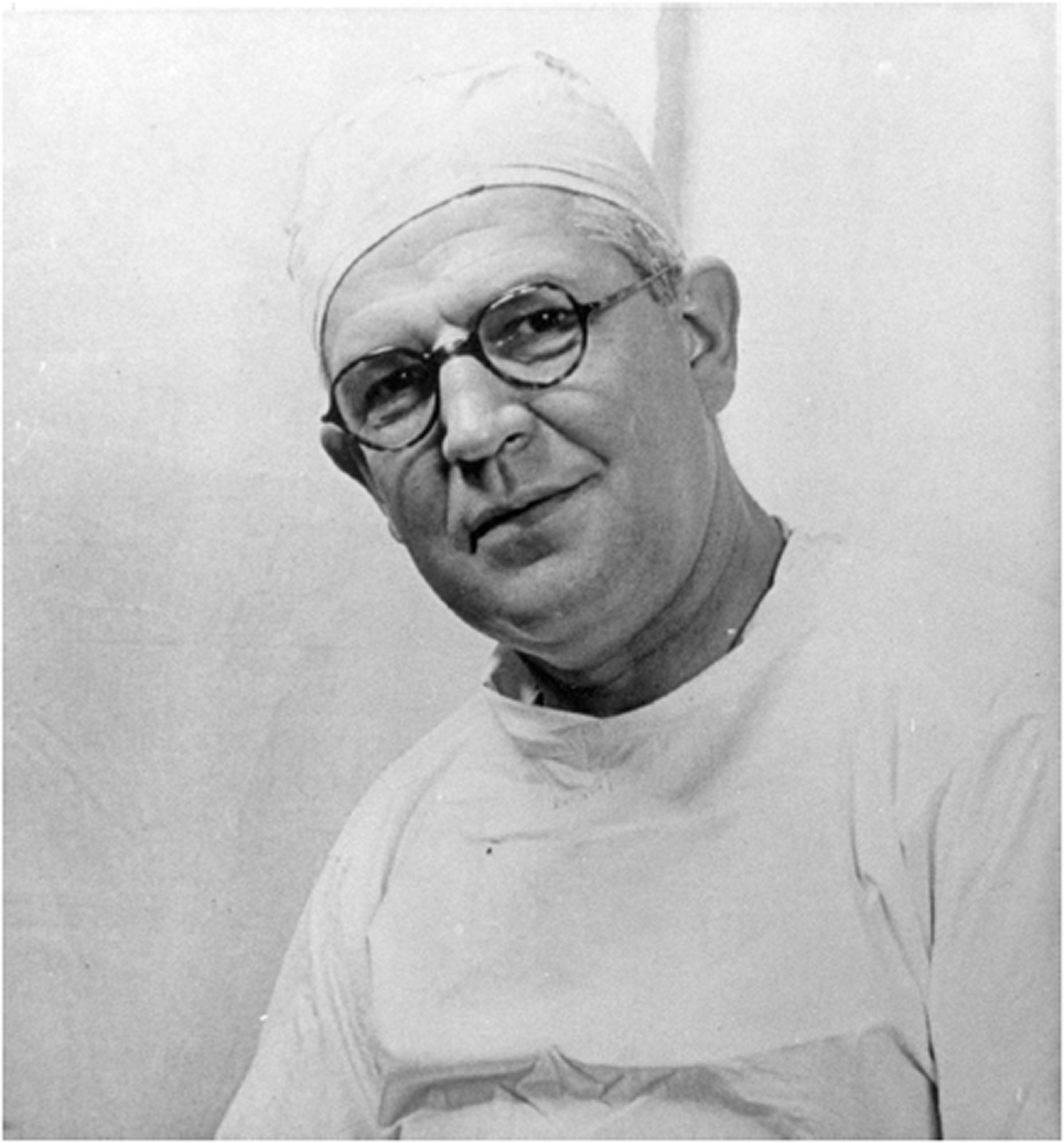
Sir Archibald McIndoe
The RAF appointed McIndoe as Civilian Consultant in 1938 (East Grinstead Museum 2021). As the Second World War erupted, McIndoe was appointed as the charge surgeon of the Maxillofacial unit at the Queen Victoria Hospital, East Grinstead. Here he would be responsible for treating the most serious burns servicemen with only the inadequate methods and drugs available at that time.
Inadequate treatment
Shock therapy and coagulants for treating burned airmen at East Grinsted Hospital were considered inadequate by McIndoe. In particular, the use of tannic acid, ‘Tannafax’, had long-term complications for full thickness burns to the hands (McIndoe 1940) (Figure 4). This method of treatment required the fingers to be fixed in flexion in hard crusts for weeks, which inevitably led to sepsis. This left the hands crippled and clawed. Before any reconstructive surgery could commence, the hard casing had to be removed. McIndoe observed how painful this was for his patients. It should also be noted that reconstruction and skin grafting techniques were also at their infancy, with often poor results which were not aesthetically pleasing. Upon treating many burned airmen, McIndoe discovered that the burnt hands of airmen who had crash landed in the sea recovered differently from those that had crashed on dry land. In light of this discovery, the use of coagulants and tannic acid was abandoned in 1940 in favour of saline baths.
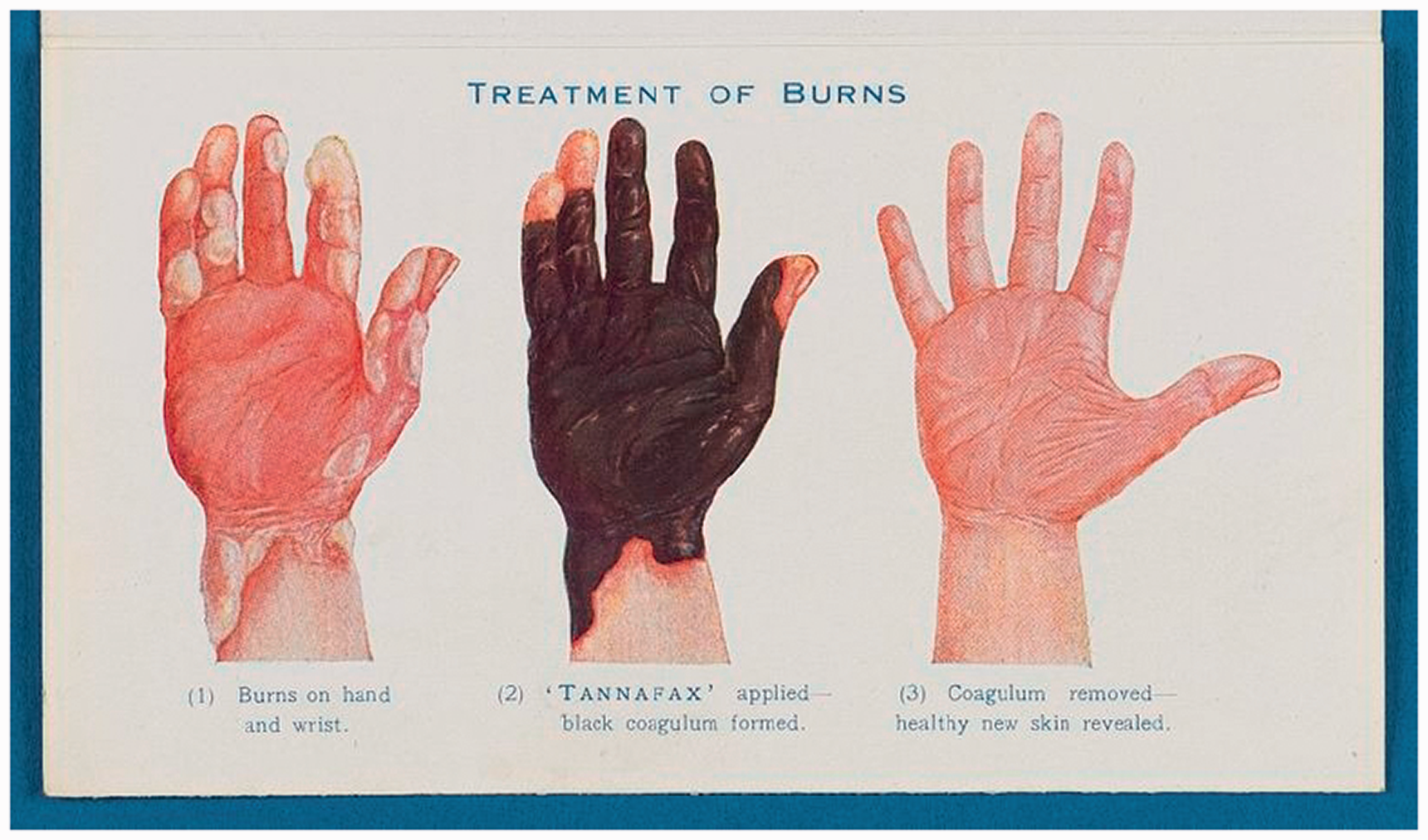
The use of Tannic Acid
Progress born of war
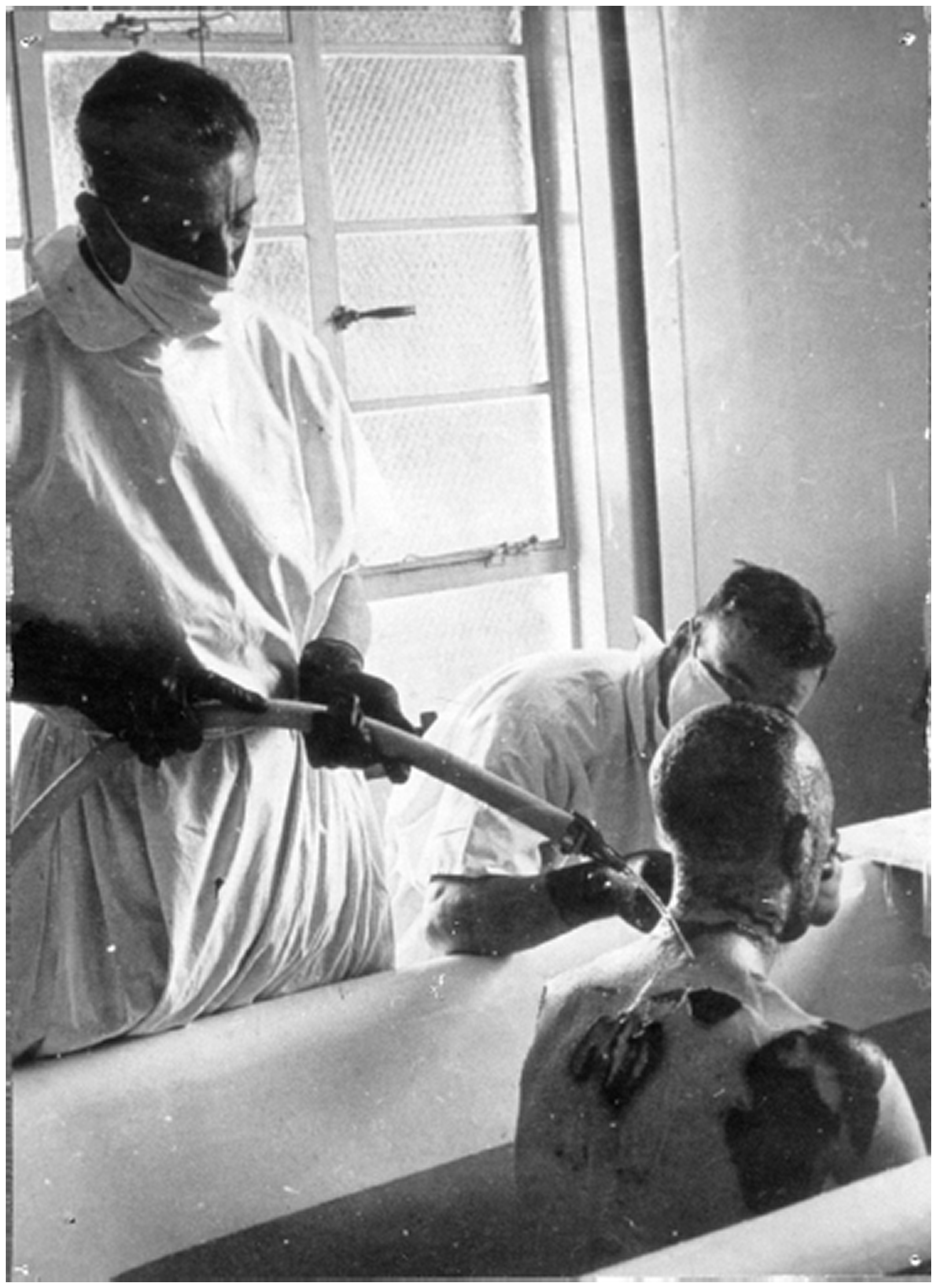
From 1940, treatment for burns patients slowly started to advance. From McIndoe’s discovery, saline baths were introduced to burnt hands. Ashwood and Philpott (2010: p253) state that ‘hands were soaked in saline for 1 hour, 2–3 times per day’. This, combined with other treatments, which included elevation of the arm to reduce oedema. A plastic bag containing Sulphanilamide powder was wrapped around the burnt hand to prevent sepsis. Also, between saline treatments the burn was dressed in tulle gras and saline compressions which were renewed once every two hours. According to Buner (1972) and Jackson (1979), the grafting of skin should be undertaken as soon as possible after the surgery. Patients were actively encouraged to move their hands and participate in rehabilitation activities. Mechanical cleaning, bathing and dressing burns was a very labour-intensive process, which yielded good results. These principles of burns management were also utilised for burned faces and bodies (Figure 5) and was continued for many years (Bruner 1973).
A photograph of a patient being treated in a saline bath
Patients’ who had endured bodily burns were treated with saline baths. Strong, male orderlies were trained in the saline bathing process (Figure 6). Orderlies were expected to lift the patients in and out of the baths and return them to their bed in a safe and effective manner and to minimise any discomfort. The baths were specifically designed in ebonite which was saline proof. They were easy to use, some had wheels so that they could be moved about. All baths were temperature controlled. Due to saline being a conductive agent, saline levels were monitored. All baths were required to be earthed to prevent patients being electrocuted during their treatment.
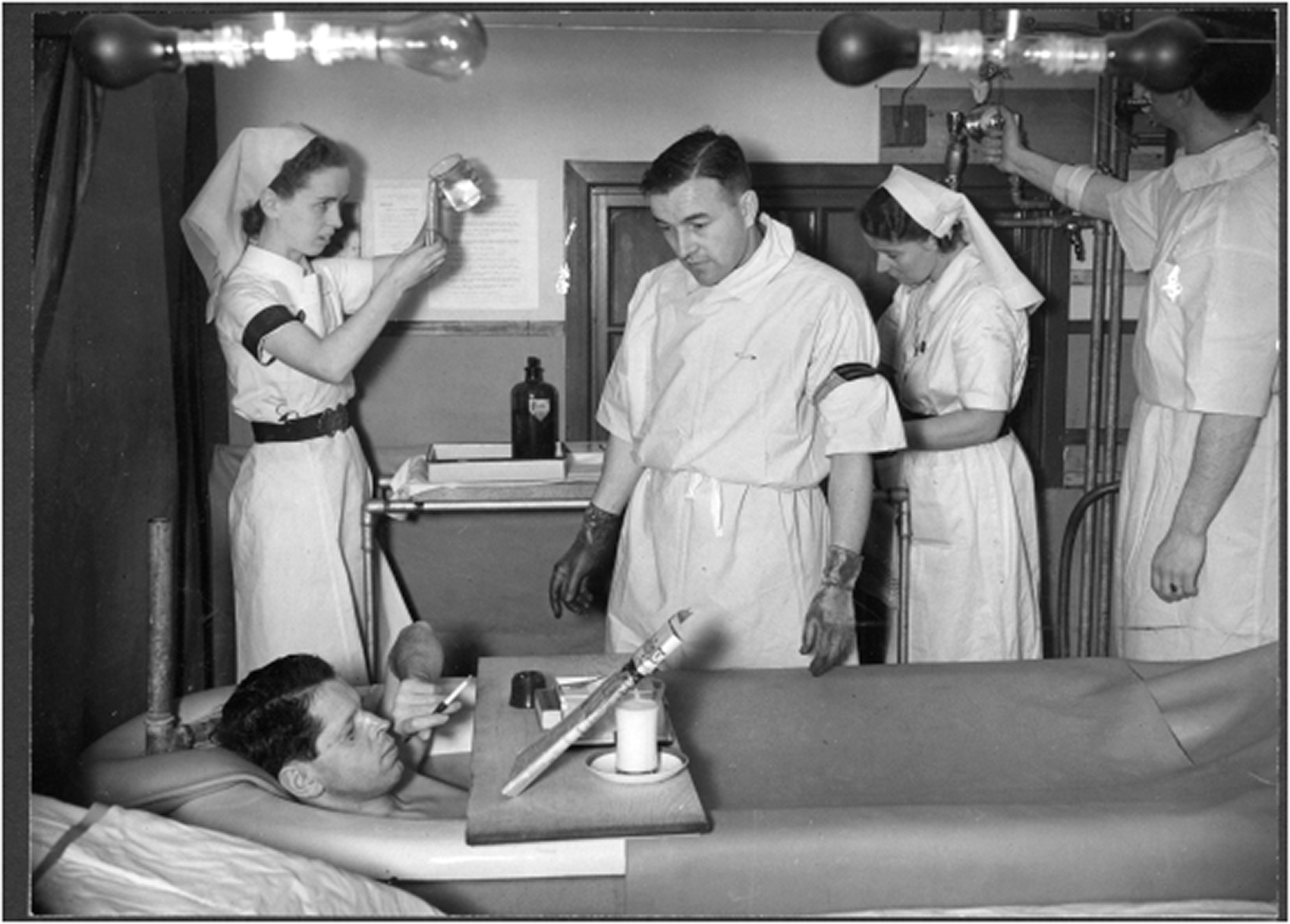
A photograph of Chief Flight Sergeant Salmon (Senior Saline Bath Technician), treating a patient in a saline bath
Reconstruction of face and hands
During his residence at East Grinstead Hospital, McIndoe operated on hundreds of patients with major burns to hands, faces and bodies. It was here that new techniques were developed which were more efficient and quicker than procedures used in the past. Having already a good understanding of the surgical procedure of the tube pedicle procedure, learnt from Sir Harold Gillies, McIndoe was able to refine the procedure to reconstruct hands and face. During the First World War, the tube pedicle technique, developed by Gillies was utilised during a skin grafting procedure. The construction of the tube used healthy skin from the leg or chest of the patient which was cut into a flap and stitched into a tube. Over a few weeks, McIndoe with extreme care and precision detached the tube at one end and reattached it to another part of the body nearing the area which required the walking-stalk skin graft. In between moving the pedicle up the body to the burn site, the blood supply needed to establish itself and it took three weeks to do so. During this time, patients were required to hold themselves in awkward positions and restrict their movements so that the pedicle was not damaged or compromised in anyway. Figure 7 shows airmen waiting for their surgeries to have their pedicles removed from various sites on their bodies to be reconstructed into their new features, this included new noses, eyelids, lips, chins and foreheads.
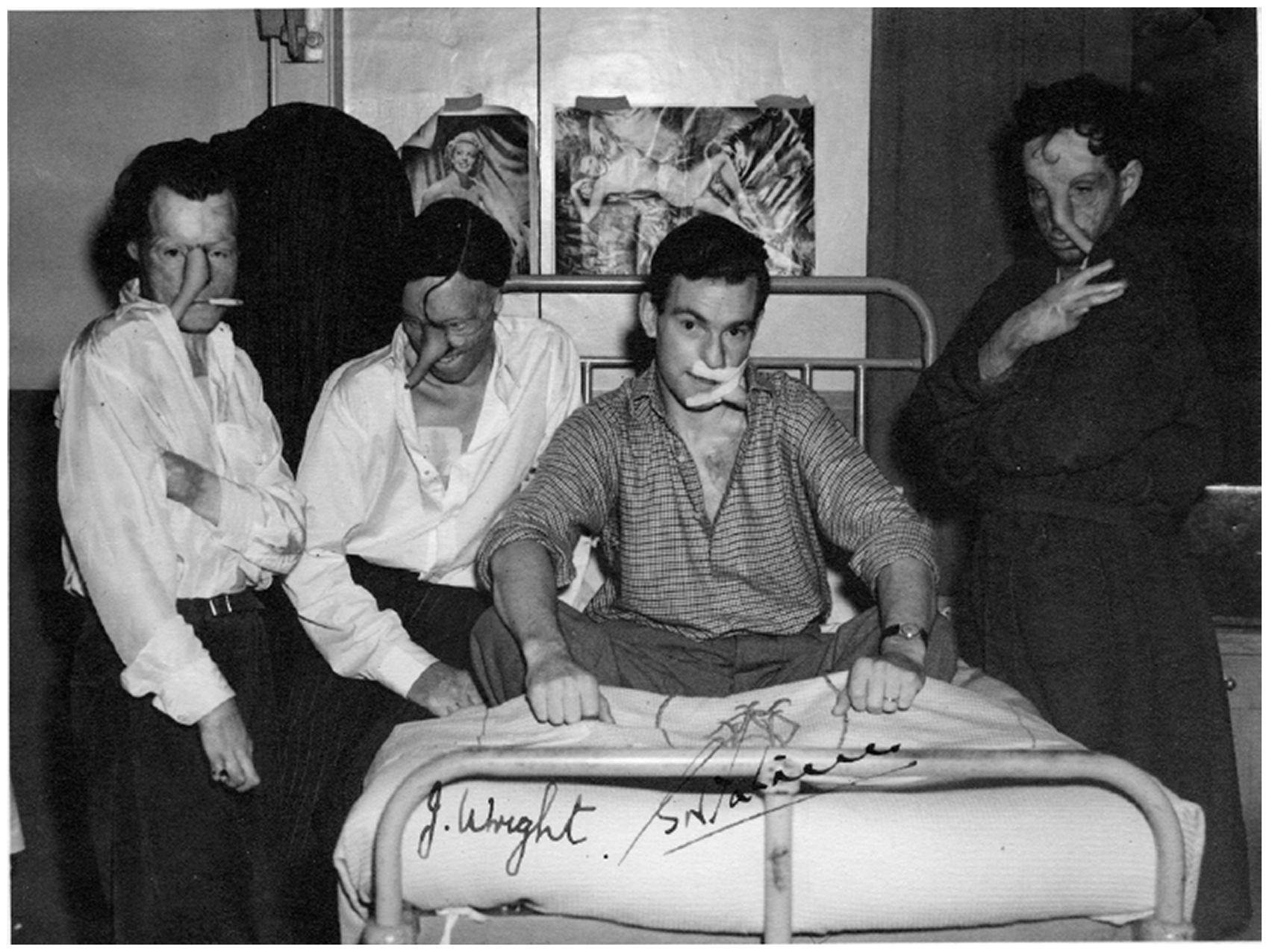
An image of four patients with pedicles. Far right: Steven Molivadas (the only Greek Guinea Pig, died August 2010), signed J Wright
Fostering a positive environment
McIndoe believed that a positive fostered environment would be an essential part of his patients’ physical and emotional rehabilitation. According to Barron (1985) cited in Ashwood and Philpott (2010: p254) McIndoe had two mantras that he liked to install in all those that came into contact with his patients, from doctors, anaesthetists, surgeons, cleaners, nurses and orderlies – ‘Total patient care’ and ‘It takes a team to treat a patient’. Ward three was unlike the rest of the hospital. The walls were painted with vibrant pinks and greens with homely chinz curtains. McIndoe was keen to have ‘the ward as comfortable as possible’. Barrels of beer and a piano were regularly found on the ward, where often a blind eye was turned by Matron. McIndoe was determined not to let his patients give up on life. McIndoe visited shops and pubs in East Grinstead, asking that people treat his patients with dignity, and not stare, and to treat them as normal human beings. The town of East Grinstead became known as ‘the town that didn’t stare’. He fought bureaucracy for their right to wear their uniforms with pride instead of the despised ‘Hospital blues’. This holistic approach was utilised to restore the Guinea Pig Club members masculinity and moral. It is reported that McIndoe often reminded his patients that they were young men in the prime of their life and they were at that age where they should be ‘drinking and flirting’. Pretty nurses were purposively selected to work on Ward three. They needed to a strong character to deal with the horrific injuries presented, but a strong resolve was also required to bat away patients advances. One nurse described ‘Some women were coerced into things they didn’t want to do. But it was probably what saved those young men’s lives and made them want to live. It’s an interesting moral dilemma isn’t it?’ (East Grinstead Museum 2021). Visitors to Ward three were surprised to hear the chatter, rasping laughter, the odd profanity and obscenity and the occasional drone of the radio. Eloquently expressed by Alan Morgan, Flight Engineer, as ‘It sounded like a nuthouse!’ (East Grinstead Museum 2021, Figure 8)
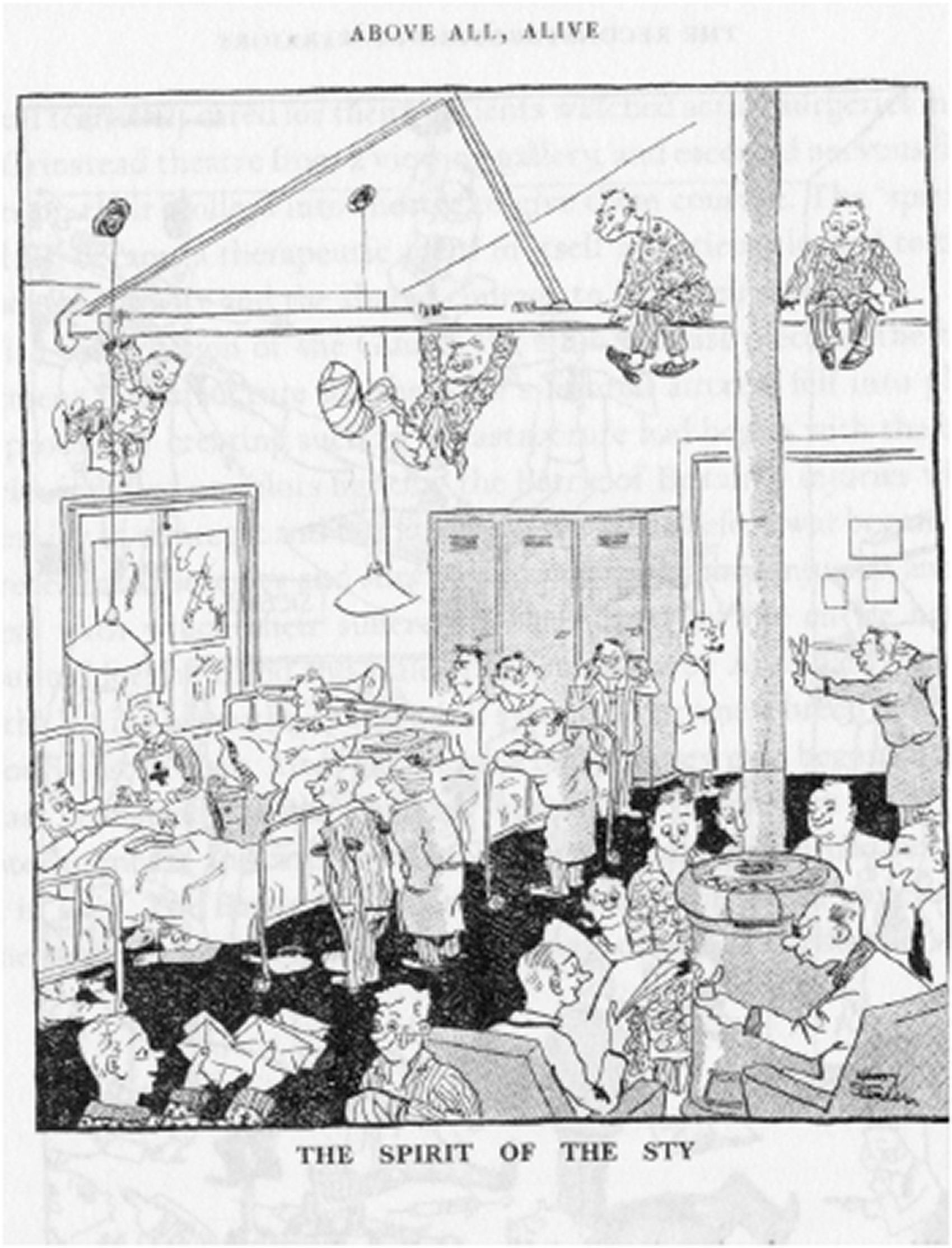
Cartoon of Ward three, nicknamed ‘The Sty’ by Sergeant Henry Standen
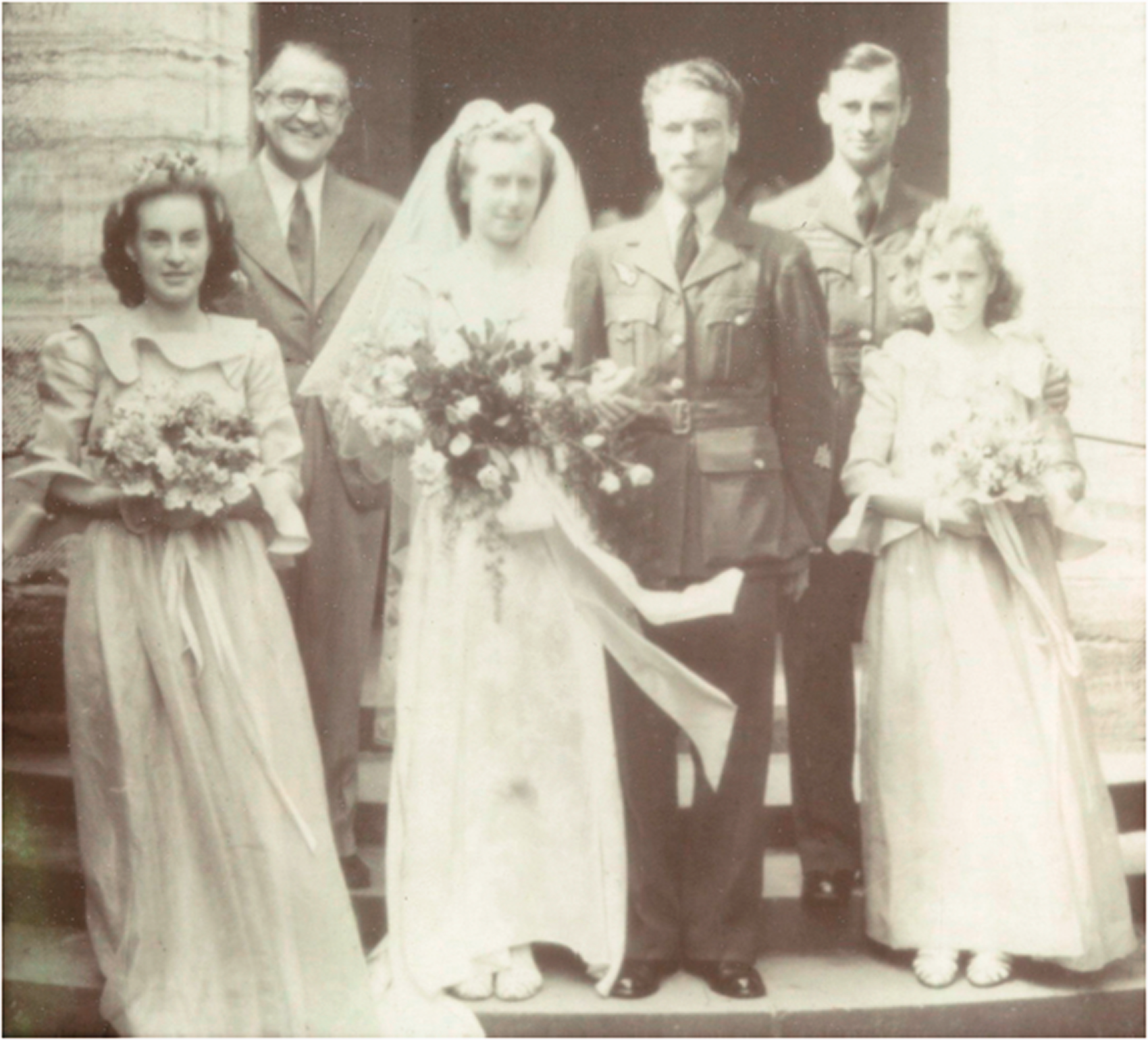
Black and white formal group wedding photography of William (Bill) Foxley and his bride in group, including Sir Archie McIndoe, leaving the church
Beginning a new life
Many Guinea Pig Club members underwent many surgical operations to treat their injuries and went on to make a good recovery. Scars healed, although not surprisingly, emotional difficulties with former wives and girlfriends were encountered. As a result, many relationships broke down. New relationships formed with nurses who had cared for them during their recovery and inevitably sometimes marriage occurred. Some were eager to return to the service, after, which, sadly, more than a few were severely burnt for a second time (Daniel 2004: p1). Above all, members belonged to a lifelong membership club where comradeship and friendship were of paramount importance.
At the end of the war, McIndoe and his team acquired many accolades from many countries, including his fellow surgical community for recognising his pioneering outstanding work carried out upon injured service men. However, without these brave men and their willing to be experimented upon, using unproven techniques with uncertain results could have hindered the surgical technological advancements that we know today. These forces and factors revolutionised burns plastic surgery. As a consequence of such discovered techniques by McIndoe, these have been utilised as a springboard to foster new research. There have been research institutions named in honour of McIndoe. These include The Gillies McIndoe Research Institution and The Blond McIndoe Research Foundation, respectively, which was set up in 1961, where pioneering research is still undertaken to continuously improve wound healing. Research and results generated have had a worldwide impact in treating and caring for patients.
The Guinea Pig Club today
There are around five original Guinea Pig members left, with the youngest being 99! (The uncertainty comes from only being able to currently contact four, with the fifth living in Greece). The last time the club met formally was in 2007, but they have gathered for events since then. The most recent of those was in 2016 when some of the members came together for the unveiling of their memorial at the National Memorial Arboretum, which was unveiled by Prince Philip before he stepped down from public roles. Officially, as the club stopped acting as a formal charity a few years ago, they did not celebrate their 80th anniversary themselves. However, as the work of the club is informally split between the East Grinstead Museum (who look after the historic and engagement work of sharing the stories of the Guinea Pig Club members) and the RAF Benevolent Fund (who help provide the Guinea Pig members day to day care needs as they are veterans), some joint celebrations were conducted online. A celebratory event for the families of the Guinea Pig Members had been planned but they were unable to hold it due to concerns around Covid-19. Officially, the club had ended as a charity, but the remaining members feel that the Club remains going as long as two of them could meet up and raise a glass to each other. In the longer term, one of the aims of the Museum is to ensure that we can tell their stories and be somewhere that the families of Guinea Pig members are proud of.
It should be remembered that the members of the Guinea Pig Club not only served their country with honour and pride, but they also were instrumental in the advancements of plastic surgery and the techniques which we know and are synonymous with today’s plastic and cosmetic surgery, respectively. We owe them a huge debt of gratitude, and I for one, an avid fan would like to raise a glass and say, ‘thank you’.
No competing interests declared
{kind=link}