
Abstract
Here we present a case of an elderly man who underwent cardiac stress testing as a preoperative evaluation prior to femoral-popliteal bypass surgery. He subsequently underwent a preoperative coronary angiogram after a high-risk stress test with the latter demonstrating obstructive three-vessel coronary artery disease. We discuss the clinical challenges that such a common clinical scenario presents particularly when it comes to preoperative coronary revascularisation prior to vascular surgery. We examine the case within the framework of the latest revascularisation guidelines and discuss the available evidence for preoperative revascularisation and its limitations.
Clinical scenario
The patient is a 78-year-old man with a history of hypertension, hyperlipidaemia, carotid artery disease, and peripheral artery disease (PAD) with multiple prior percutaneous interventions to the left lower extremity, who presented for evaluation of left lower extremity claudications. He was evaluated by a vascular surgeon who recommended femoral-popliteal bypass of the left lower extremity. He was assessed by a general cardiologist in the preoperative clinic for any further testing or optimisation. The patient could not walk more than a block at a slow pace before stopping due to significant claudications. Given that his functional capacity was less than four metabolic equivalents for task (METs) and based on the clinical assessment, he was referred for a preoperative echocardiogram and pharmacological nuclear stress test. Of note, the patient described no angina or anginal equivalent symptoms at the level of exertion he was able to tolerate. Stress testing at an outside hospital revealed moderate size reversible defects in the inferoseptal and inferolateral myocardial walls. No further details of the test were available. An echocardiogram showed an ejection fraction of 50% with hypokinesis of the basal inferoseptal and basal inferior walls. After discussion with the patient, he was referred for invasive coronary angiography (CA) for further risk stratification. The patient underwent CA which revealed three-vessel coronary artery disease (CAD) with chronic total occlusion (CTO) of the mid-right coronary artery (RCA). It also showed a 90% stenosis of the mid-left circumflex (LCx) and a 70% mid-left anterior descending coronary artery (LAD) stenosis which was also haemodynamically assessed with resting (non-hyperaemic) fractional flow reserve index (Pd/Pa) and deemed significant.
Guideline recommendations
The current case represents a common preoperative scenario where there is a gap in clinical evidence to guide best practice. The patient was planned to undergo an elective but major vascular surgery. He did not have any known active cardiac conditions, yet his symptom assessment was limited due to low functional capacity. This is a common scenario in patients who experience significant mobility issues such as claudications. Current American College of Cardiology/American Heart Association (ACC/AHA) guidelines for preoperative risk assessment prior to non-cardiac surgery assign class 2A recommendation for patients who are at an elevated risk to undergo non-invasive testing if their functional capacity is less than 4METs, and if it will change management (Fleisher et al 2014). Similarly, appropriate use criteria assign class 2A recommendation for patients with a functional capacity less than 4METS to undergo non-invasive stress testing for further risk stratification prior to vascular surgery (Wolk et al 2014). Hence, it was reasonable for this patient to undergo cardiac stress testing with the knowledge that a high-risk test may lead to further invasive testing and delay surgery. The patient’s CA revealed three-vessel CAD including a CTO of the RCA. Of importance, the patient did not experience clinical angina symptoms and his left ventricular ejection fraction was preserved. Recently published ACC/AHA revascularisation guidelines assign class 2B recommendation for either percutaneous or surgical revascularisation in patients with multivessel CAD to reduce mortality or risk of myocardial infarction (MI) and class 1 recommendation to reduce refractory angina symptoms (Lawton et al 2022). In an asymptomatic patient, and based on the available guidelines, any mode of revascularisation would yield minimal benefit for the patient. The more important question arises is whether it is appropriate to undergo high-risk non-cardiac surgery without further coronary revascularisation.
Available evidence
The results of the recent ISCHAEMIA trial, multiple prior randomised controlled trials, and large meta-analyses provide reassurance that managing patients medically with stable three-vessel CAD and moderate to large area of ischaemia on stress testing could be appropriate (Bangalore et al 2020, Maron et al 2020, Vij et al 2021). This applies as long as patients have minimal symptoms, and no significant left ventricular dysfunction, or ischaemia-driven arrhythmias. In regard to preoperative revascularisation in such patients, from the limited randomised data (CARP and DECREASE -V pilot study) (Table 1 in Appendix 1) there does not appear to be a significant benefit of prophylactic coronary revascularisation prior to surgical intervention (McFalls et al 2004). Our patient does fit the criteria for both trials as ISCHAEMIA included patients with three-vessel CAD including 36% of patients with proximal LAD disease. In addition, 33% of patients included in the CARP trial and 67% in the DECREASE-V Pilot Study had three-vessel CAD. However, now that we know that the patient has multivessel CAD, what is the cardiovascular perioperative risk of this patient if he undergoes vascular surgery and how do we guide a patient-centred discussion regarding the associated risks?
Perioperative risk
Offering a patient with three-vessel CAD to vascular surgery may be challenging for both the patient and the treating physicians. There may be hesitancy from the surgical team to operate on a patient with extensive CAD which is not revascularised. In addition, there may be a lot of hesitancy from the patients and their families too. The idea of prophylactic preoperative coronary revascularisation is based on the assumption that perioperative MI occurs at the site of the stenotic artery and arises from reduced flow across the lesion during increased myocardial oxygen demand (Poldermans et al 2007). The clinical credence of this concept was based on a retrospective subgroup analysis of 1834 patients with PAD enrolled in the Coronary Artery Surgery Study (CASS) registry which demonstrated that patients who underwent coronary artery bypass surgery (CABG) had better survival at four years relative to patients who were medically treated (88% vs 73%, p < 0.01) (Rihal et al 1995). Yet, the real mechanism of myocardial injury and MI post-vascular surgery is not fully understood. Partially, it could be related to demand ischaemia, namely type 2 MI, as defined by the fourth universal definition of MI (Thygesen et al 2018), especially in case of operative hypotension, desaturation, or any postoperative complications like pulmonary embolism or infections. On the contrary, vascular surgeries can create a highly inflammatory milieu and a pro-thrombotic state which can lead to plaque rupture hence, type 1 MI as defined by the fourth universal definition of MI (Thygesen et al 2018) even in a non-obstructive plaque. In addition, the effects of endothelial dysfunction and microcirculation in patients with extensive CAD and its contribution to postoperative cardiac events are also poorly understood. Yet, whatever the mechanism of injury or infarction is, it is well known that perioperative MI is associated with significantly worse postoperative outcomes (Landesberg et al 2001, Ultee et al 2015). Hence, what is the risk of MI or death in the perioperative period in patients with obstructive CAD? The main evidence for the risk of developing perioperative MI comes from two randomised controlled trials, namely the CARP trial and the DECREASE-V Pilot Study (McFalls et al 2004, Poldermans et al 2007). Both trials included only patients undergoing vascular surgery. CARP trial showed that within 30 days postoperatively, 11.6% of patients who underwent revascularisation had elevated troponins and 8.4% of patients met criteria for MI (elevated troponins with ECG changes) as compared to 14.3% and 8.4%, respectively in medically managed patients (McFalls et al 2004). This difference was not significant. The overall death rate was also similar between the groups at approximately 3% at 30 days. It should be noted that approximately half of the patients in either group were on statin therapy, three quarters were on aspirin, and just over 80% were on beta-blockers. Importantly, one should add a 6% MI rate in patients who underwent revascularisation by CABG or percutaneous coronary revascularisation (PCI) before undergoing vascular surgery. In addition, there did not appear to be a long-term mortality benefit at 2.7-year follow-up in the revascularisation group as compared to medical therapy. DECREASE-V Pilot Study included overall Higher-risk patients than the CARP trial did (67% with three-vessel CAD and 43% with left ventriclular ejection fraction (LVEF) < 35%) with evidence of extensive ischaemia on non-invasive stress testing. At 30 days postoperatively, there was statistically no difference in the overall mortality and rates of MI between the revascularisation and medical therapy groups (22.5% vs 11.5% and 34.7% vs 30.8%), respectively. At one-year, there remained to be no significant difference between the two groups (Poldermans et al 2007).
Two other non-randomised studies evaluated the effect of coronary revascularisation on postoperative survival after vascular surgery. Back et al found that coronary revascularisation within five-years prior to vascular surgery offered only modest improvement in survival compared to those who underwent revascularisation more than 5 years, and those who did not undergo revascularisation (73% vs 58% vs 62% 5 year survival) (Back et al 2004). Ultee et al demonstrated that the most common cause of death in the perioperative period was related to ischaemic cardiac events. In patients who received coronary revascularisation, there was less death related to ischaemic heart disease; however, overall mortality was not statistically different (Ultee et al 2015). Patients who underwent coronary revascularisation had a similar ischaemic event rate compared to patients who had no known ischaemic heart disease. The authors noted that the patients in the coronary revascularisation group died more often of non-cardiac ischaemic events, predominantly related to PAD. The authors, however, provide no explanation for that latter finding which could be merely related to the overall statistically low number of events.
Limitations of the preoperative cardiovascular risk assessment and data
There are several major limitations in assessing patients prior to vascular surgery. A major emphasis relies on the patient’s functional status which remains a subjective measure. Several studies demonstrated that using patient-reported functional capacity as a tool to predict METS correlated poorly with postoperative outcomes (Reilly et al 1999, Wiklund et al 2001). Similarly, utilising exercise testing or cardiopulmonary testing to assess symptomatology is often limited by the patient’s vascular or other comorbidities. There is also significant variability between various cardiovascular guidelines when it comes to preoperative risk assessment. For example, the Canadian Cardiovascular Society emphasises the role of using certain biomarkers for heart failure such as N-terminal pro-brain natriuretic peptide (NT-pro BNP) for screening in patients older than 65 and elevated risk defined by revised cardiac risk index ⩾ 1. In addition, they recommend against resting echocardiography or any type of stress testing to better risk-stratify patients (Duceppe et al 2017). European Society of Cardiology (ESC), on the contrary, assigns class 2B recommendation for screening only high-risk patients with NT-pro BNP and class 2B recommendation for obtaining preoperative echocardiogram before high-risk surgery (Kristensen et al 2014). ESC recommendation on preoperative stress is similar to that of ACC/AHA (Fleisher et al 2014, Kristensen et al 2014). In addition, there remain to be significant limitations of the previously discussed studies on preoperative revascularisation as their findings cannot be generalised to all the patients undergoing perioperative risk assessment. Only 33% of CARP trial patients had three-vessel CAD and revascularisation decision was not guided by the extent of ischaemia but rather angiographic stenosis. The use of physiology to identify haemodynamically significant lesions was also limited. In a subgroup analysis of the CARP trial involving patients who underwent stress testing and had evidence of myocardial ischaemia, at 30 days, there was no difference in mortality, yet there was a trend towards reduction in non-fatal perioperative MI in the revascularisation group. Long-term follow-up at 2.7 years showed that there are two multivariate predictors of freedom from death and MI, namely coronary revascularisation (p = 0.03) and the absence of anterior ischaemia (p = 0.07). This was a small patient subgroup (n = 109) and the findings are hypothesis-generating at best (Garcia et al 2011). DECREASE-V study was a pilot study and not statistically powered due to the low sample size with only 101 total randomised patients. Two of the deaths in the revascularisation group happened prior to vascular surgery and were due to ruptured aortic aneurysms which, in this low-powered study, could have significantly skewed the results. The very high perioperative mortality in the DECREASE 5 study does not correspond to current standards of care. In addition, patients who were randomised in the study with extensive ischaemia and reduced LV function, in current practice, would undergo revascularisation regardless as there is a significant mortality benefit of revascularisation in those patients. The lack of clear clinical benefit of revascularisation could be related to the risk of coronary revascularisation itself, whether it is CABG or PCI, which adds up to the postoperative risk after vascular surgery. Hence, periprocedural MI may cancel the benefit of reducing postsurgical MI risk which has been observed in patients undergoing routine coronary revascularisation. The mechanism of MI post-surgery is also probably related to plaque rupture in non-obstructive lesions observed in at least half of MIs (Cohen & Aretz 1999), a risk which should be reduced by CABG as opposed to PCI (Doenst et al 2019). This latter finding has been confirmed in a subgroup analysis of the CARP trial where patients who underwent CABG had lower rates of periprocedural MI as compared to PCI (Ward et al 2006). Finally, not all vascular surgeries carry the same cardiovascular risk. Major vascular surgeries with large fluid and haemodynamic shifts such as open aneurysm repair may theoretically carry a higher periprocedural risk than more contained surgeries such as femoral-popliteal bypass. The available studies did not stratify the cardiovascular risk based on the type of vascular surgery performed hence, the specific risk of each type of surgery is unknown and may warrant future studies.
It remains unclear what is the optimal strategy to identify the appropriate patient cohort which would benefit the most from coronary revascularisation. Clinical decision-making based on certain high-risk features could prove beneficial. For example, a large area of ischaemia on non-invasive testing, the presence of multiple haemodynamically significant proximal lesions on physiological assessment during the angiogram, and vulnerable plaque identification angiographically or with intracoronary imaging may further help physicians identify this patient cohort.
Conclusion
The current patient had an intermediate syntax score and subsequently underwent three-vessel CABG. Syntax score is a comprehensive angiographic tool that grades the complexity of CAD and is useful in predicting long-term adverse cardiac and cerebrovascular events. His postsurgical recovery period was complicated by an episode of atrial flutter requiring cardioversion. He is currently planned to undergo left femoral-popliteal bypass surgery for refractory claudications. Based on the current evidence, it is unclear whether the current management would significantly reduce patients’ perioperative cardiovascular risk. It remains unclear how we can best identify the cohort of patients who will benefit the most from preoperative coronary revascularisation. From the available evidence, only patients with unstable ischaemic heart disease seem to benefit from preoperative coronary revascularisation. Hence, routine revascularisation for asymptomatic patients may not be warranted. However, surrogate markers including large ischaemic burden on stress testing and those who would qualify for revascularisation regardless of surgery (significant left main disease or patients with reduced ejection fraction) should be considered. In addition, given the high risk of perioperative mortality and morbidity in high-risk patients, endovascular strategies for vascular procedures should be considered whenever possible.
Footnotes
Appendix 1
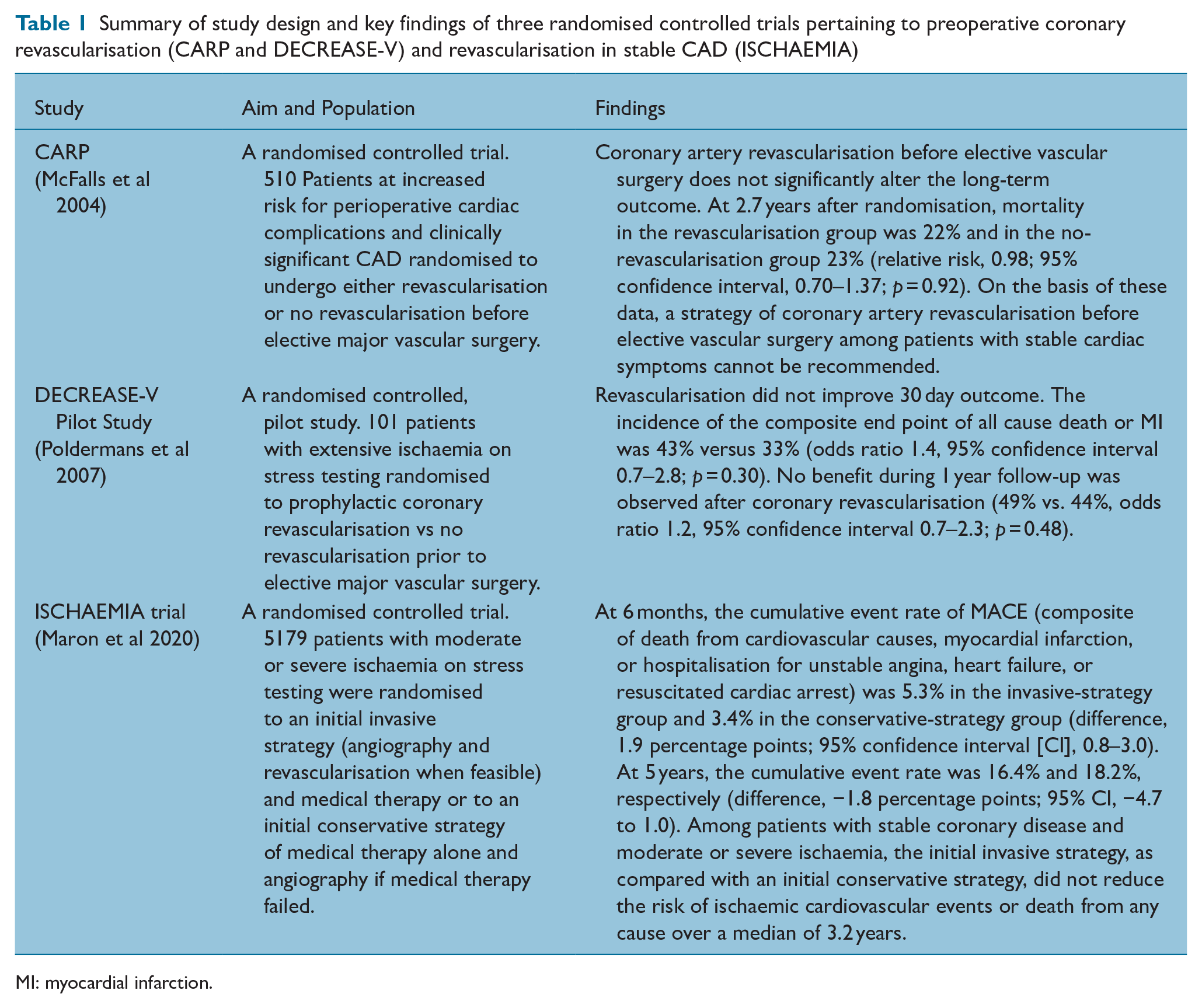
Summary of study design and key findings of three randomised controlled trials pertaining to preoperative coronary revascularisation (CARP and DECREASE-V) and revascularisation in stable CAD (ISCHAEMIA)
| Study | Aim and Population | Findings |
|---|---|---|
| CARP (McFalls et al 2004) |
A randomised controlled trial. 510 Patients at increased risk for perioperative cardiac complications and clinically significant CAD randomised to undergo either revascularisation or no revascularisation before elective major vascular surgery. | Coronary artery revascularisation before elective vascular surgery does not significantly alter the long-term outcome. At 2.7 years after randomisation, mortality in the revascularisation group was 22% and in the no-revascularisation group 23% (relative risk, 0.98; 95% confidence interval, 0.70–1.37; p = 0.92). On the basis of these data, a strategy of coronary artery revascularisation before elective vascular surgery among patients with stable cardiac symptoms cannot be recommended. |
| DECREASE-V Pilot Study (Poldermans et al 2007) |
A randomised controlled, pilot study. 101 patients with extensive ischaemia on stress testing randomised to prophylactic coronary revascularisation vs no revascularisation prior to elective major vascular surgery. | Revascularisation did not improve 30 day outcome. The incidence of the composite end point of all cause death or MI was 43% versus 33% (odds ratio 1.4, 95% confidence interval 0.7–2.8; p = 0.30). No benefit during 1 year follow-up was observed after coronary revascularisation (49% vs. 44%, odds ratio 1.2, 95% confidence interval 0.7–2.3; p = 0.48). |
| ISCHAEMIA trial (Maron et al 2020) |
A randomised controlled trial. 5179 patients with moderate or severe ischaemia on stress testing were randomised to an initial invasive strategy (angiography and revascularisation when feasible) and medical therapy or to an initial conservative strategy of medical therapy alone and angiography if medical therapy failed. | At 6 months, the cumulative event rate of MACE (composite of death from cardiovascular causes, myocardial infarction, or hospitalisation for unstable angina, heart failure, or resuscitated cardiac arrest) was 5.3% in the invasive-strategy group and 3.4% in the conservative-strategy group (difference, 1.9 percentage points; 95% confidence interval [CI], 0.8–3.0). At 5 years, the cumulative event rate was 16.4% and 18.2%, respectively (difference, −1.8 percentage points; 95% CI, −4.7 to 1.0). Among patients with stable coronary disease and moderate or severe ischaemia, the initial invasive strategy, as compared with an initial conservative strategy, did not reduce the risk of ischaemic cardiovascular events or death from any cause over a median of 3.2 years. |
MI: myocardial infarction.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.