
Abstract
Background:
This study investigated the effectiveness of intratracheal dexmedetomidine in reducing untoward laryngeal responses in paediatrics undergoing lower abdominal surgeries.
Methods:
This trial included 60 patients divided into two groups scheduled for lower abdominal surgeries. Group D were given intratracheal dexmedetomidine at a dosage of 0.5mg/kg, while Group C received intratracheal saline (0.9%). The cough severity score, the Paediatric Objective Pain Scale for pain assessment, awareness, extubation, emergence agitation score, Ramsay sedation score and adverse effects were recorded.
Results:
There was a significant difference in the incidence of coughing severity between Groups D and C both at extubation and after five minutes of extubation (p < 0.001). The median scores of the Paediatric Objective Pain Scales and the median agitation scales of Group D were significantly lower over the first four hours (p < 0.050). The mean time to first request rescue analgesia was significantly longer in the D group than in the control group (p < 0.001). The mean total consumption of rescue analgesia in the first 24 hours postoperatively was significantly lower in the dexmedetomidine group (p < 0.050). Awareness and extubation times were comparable in both groups, and none of the subjects reported any adverse effects.
Conclusion:
In the current study, lower abdominal surgery patients who received intratracheal dexmedetomidine at a dose of 0.5mg/kg 30 minutes before the completion of the procedure experienced smooth extubation and balanced anaesthetic recovery.
Keywords
Introduction
On emergence from general anaesthesia, patients are often accompanied with adverse reactions, such as cough, agitation, hypertension and tachycardia, and the incidence of cough is up to 82.5% (Safavi et al 2016). The cough during extubation not only brings discomfort to patients, but also leads to hypertension, tachycardia, myocardial ischaemia, laryngospasm and other complications (Kim et al 2018). As a result, several anaesthesiologists have been looking for ways to reduce this laryngeal irritation to facilitate smoother extubation (Fan et al 2015). In addition, it has contributed to aggravating cough reflexes.
Numerous techniques, including intravenous (IV) lidocaine, remifentanil and dexmedetomidine, have been claimed to facilitate smoother extubation (Kim et al 2016). Sedation is produced without respiratory depression by dexmedetomidine, a highly selective α2-adrenergic agonist. It decreases preoperative anxiety when taken before surgery (Sheta et al 2014), lowers the anaesthetic need and increases the level of anaesthesia (Yao et al 2014). Clinical studies have extensively studied IV dexmedetomidine to reduce airway and circulatory reflexes throughout extubation (Yao et al 2014).
It has been reported that intratracheal local anaesthetic instillation is efficient at preventing unwanted laryngeal reflexes (Jee & Park 2003). However, the procedure still needs to be thoroughly studied, and the effectiveness and safety profile of the intratracheal dexmedetomidine application still needs to be discovered. This current study was carried out to assess the efficacy of intratracheal dexmedetomidine to reduce, or prevent, undesirable laryngeal reactions in paediatric patients emerging from general anaesthesia.
Patients and methods
After receiving approval from our local institutional ethics committee of the faculty of medicine and clinical trial registration, this prospective, randomised, double-blind, placebo-controlled study was planned. It was carried out in the operating room of the paediatric surgery unit in a paediatric hospital.
The legal guardians of the patients provided written informed consent, which was obtained following the Helsinki Declaration and the appropriate CONSORT criteria.
The present study enrolled 60 male patients (ages one to six years) planned for lower abdominal surgeries, for example, congenital hernia repair and palpable un-descended testes under general anaesthesia (GA). All patients had American Society of Anaesthesiologists (ASA) scores of I or II.
The exclusion criteria were as follows: younger than one year and older than six years, parental rejection, allergy or contraindication to the drugs or anaesthetics under study; Patients with respiratory and cardiac diseases may be at risk of complications of dexmedetomidine, such as bradycardia and hepatic or renal insufficiency.
Randomisation and blinding
The children were assigned to one of the two groups via a computer-generated randomisation plan. The randomisation plan was kept in opaque, sealed envelopes and released by an anaesthetist who was not involved in the study, but only prepared the study drugs. An anaesthetist who was not convoluted in the study of drug administration, or envelope coding, collected anaesthetic technique and outcome data. Neither the anaesthetist who administered the anaesthesia, nor the patients themselves, were aware of the group assignment to ensure the blindness of the study.
Patients
Sixty patients were registered in this study. They were equally allocated into two groups:
*
*
Anaesthetic technique
The preoperative anaesthetic clinic served as the location for the preoperative assessment and evaluation of the study participants. The legal guardians of the participants were made aware of the study’s methodology and told they could withdraw at any time without losing access to medical care.
All patients received no premedication. Standard intraoperative monitors, such as heart rate (HR), non-invasive arterial blood pressure (NIABP), electrocardiogram (ECG), O2 saturation (SpO2) and end-tidal CO2 (ETCO2) were recorded. IV fluid administration (0.9% NaCl) was started at the calculated volume and rate. Anaesthesia was induced with fentanyl (1μg/kg), lidocaine (0.5mg/kg) and propofol (2–3mg/kg) administered to facilitate endotracheal intubation. Sevoflurane maintained anaesthesia in 100% oxygen (O2) with an infusion of cisatracurium (0.15mg/kg). The patient was intubated with an appropriate endotracheal tube according to age. Thirty minutes before the end of the operation, the drugs in both groups were injected into the patient’s intratracheal tube. IV neostigmine (0.05mg/kg) and atropine (0.01mg/kg) were administered to reverse the muscle paralysis. The recovery process was monitored, and data were collected.
Assessment parameters
The demographic and intraoperative variables were recorded, together with age, weight, the duration of anaesthesia and surgery and the time to extubation (from the end of the surgery to extubation).
Mean arterial blood pressure (MBP), HR and SpO2 values were recorded at baseline (preinduction of anaesthesia), instantly after dexmedetomidine administration, every five minutes until the end of the surgery, at the point of extubation, every five minutes until 30 minutes after extubation.
The severity of the cough was assessed using the four-point scale assessed during the recovery period from the time of consciousness to five minutes after extubation: 0 = no cough, 1 = minimal (single) cough, 2 = moderate (⩽5 seconds) cough and 3 = severe (> 5 seconds) cough (jerking). Grades 2 and 3 were considered clinically harmful (Minogue et al 2004).
The awareness time and extubation time (minutes), agitation score.
Consequently, postoperative pain scores (the Paediatric Objective Pain Scale) were assessed after extubation, every one hour until four hours, then every six hours until 24 hours.
Time of first rescue analgesic requirement, the number of patients who required IV paracetamol as emergency analgesics in the first 24 hours. The total amount of paracetamol doses (15mg/kg per dose) as an emergency analgesic was required after the onset of pain in the first 24 hours.
Postoperative sedation was measured with the Ramsay sedation score (RSS) in the first 24 hours after the operation. The RSS was recorded at 0 (upon arrival to the postanaesthesia care unit (PACU)), 30 minutes, one, two, four, six, 12 and 24 hours postoperatively.
Adverse effects like bradycardia, tachycardia, the postoperative nausea and vomiting (PONV), hypertension and hypotension were noted and compared. Bradycardia and tachycardia were demarcated as an HR < 50 or > 100 beats/minute. Hypertension and hypotension were demarcated as an MBP < 30% or > 30% from the baseline for five minutes.
Parent satisfaction. At the end of the 24-hour study period, the subjects’ parents graded their satisfaction with the analgesia on a five-point Likert-type scale (1 = very dissatisfied, 2 = unsatisfied, 3 = neutral, 4 = satisfied and 5 = very satisfied).
The day after surgery, all parents were called by the same convalescent nurse and asked if they had seen any side effects. At discharge, all children were given oral paracetamol (20mg/kg) as desired (a maximum of four doses in 24 hours).
Outcomes
The primary outcome was the extent of coughing between the two groups.
Secondary outcomes were the awareness time, extubation time, agitation score, paediatric Objective Pain Scale, time for first analgesic request, total analgesic requirements/24 hours and adverse effects.
Sample size
The G Power 3.1.9.7 application was used to calculate the sample size. A power analysis assessed that a sample size of 26 patients in each group would have an 80% power at a 0.05 significance level to identify a difference of 0.7 effect size in the coughing severity between the two groups. Thirty subjects were enrolled in each group to reward patients’ dropouts.
Statistical analysis
Using Microsoft Excel 2016 for Windows, a component of the 2016 Microsoft Office suite from the United States-based Microsoft Corporation, data were gathered, coded and then input as a spreadsheet. The IBM Statistical Package for Social Sciences for Windows, version 26.0, Armonk, NY: IBM Corp., was used to analyse the data. The distribution’s normality was assessed using the Kolmogorov–Smirnov test. While categorical data were expressed as percentages and numbers, continuous data were expressed as mean, standard deviation, median and interquartile range. The 0.05 cutoff was chosen as the statistical significance level. The chi-square test was used to examine the relationship between two qualitative variables. Student’s t test was used to compare two investigated groups using quantitative variables that are regularly distributed. To compare two groups that looked at quantitative variables with different distributions, we used the Mann–Whitney test.
Results
Among the 88 individuals evaluated for eligibility, 60 were enrolled in the current study; patients were divided into two groups of 30 each (Figure 1).
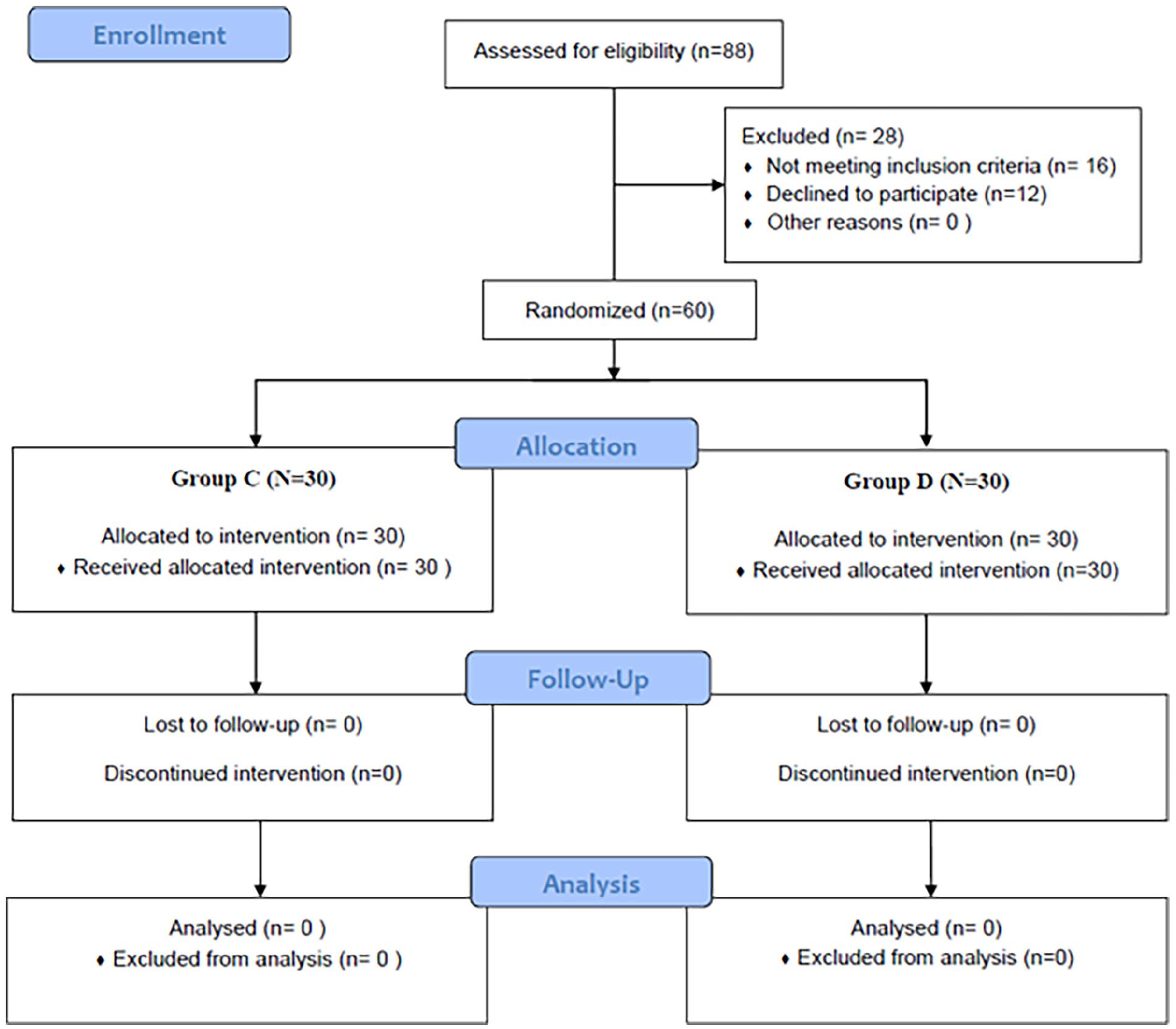
CONSORT flow diagram
There were no statistically significant differences in age, weight, ASA, duration, type of operation or anaesthesia (Table 1).
Demographic and clinical characteristics among the studied groups
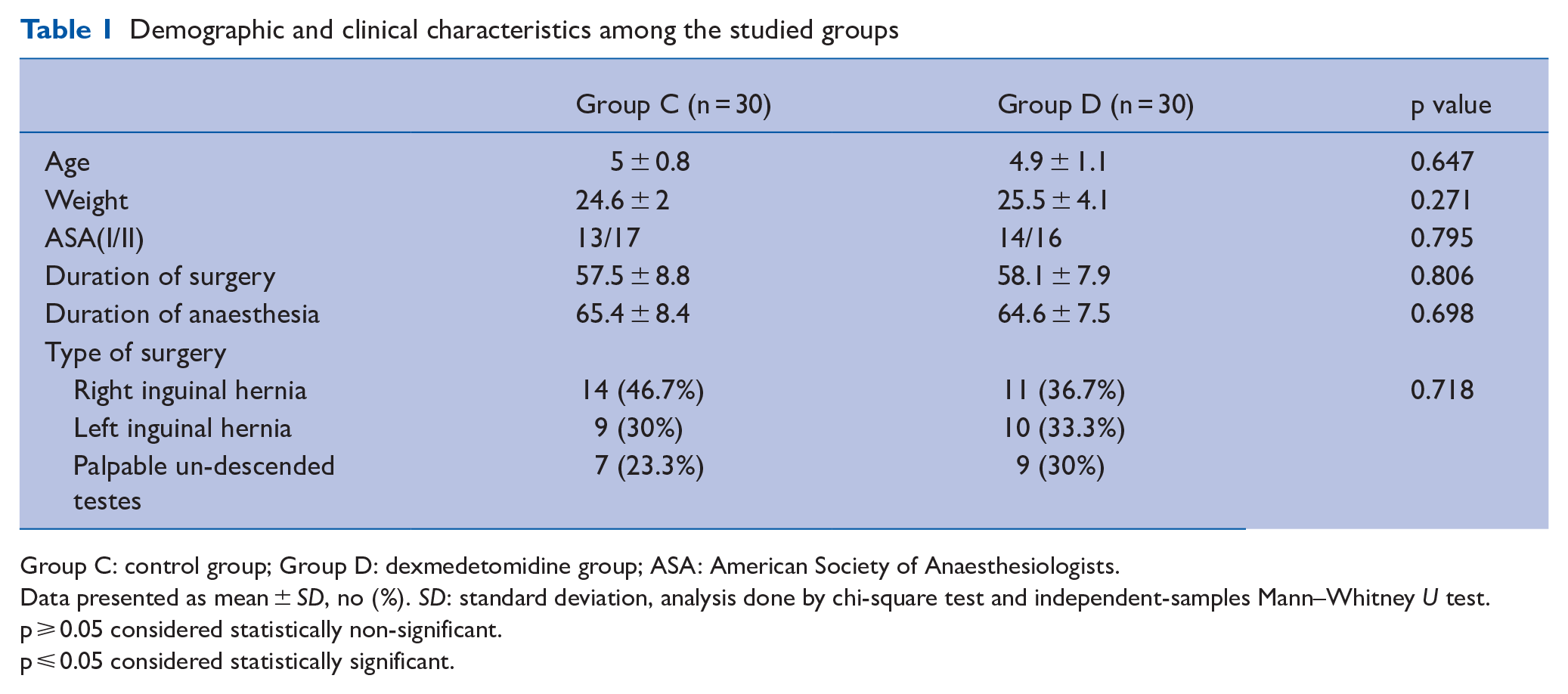
Group C: control group; Group D: dexmedetomidine group; ASA: American Society of Anaesthesiologists.
Data presented as mean ± SD, no (%). SD: standard deviation, analysis done by chi-square test and independent-samples Mann–Whitney U test.
p ⩾ 0.05 considered statistically non-significant.
p ⩽ 0.05 considered statistically significant.
Haemodynamics
There was no statistically significant difference between the two groups concerning HR and MBP at preoperative, after induction of anaesthesia and immediately after administration of the drug. There was a significant decrease in HR and MBP in the D group at ten, 15, 20, 30 minutes, end of the operation, at extubation, at PACU, 15 minutes, 30 minutes, one hour (p < 0.001) (Figure 2(a) and (b)).
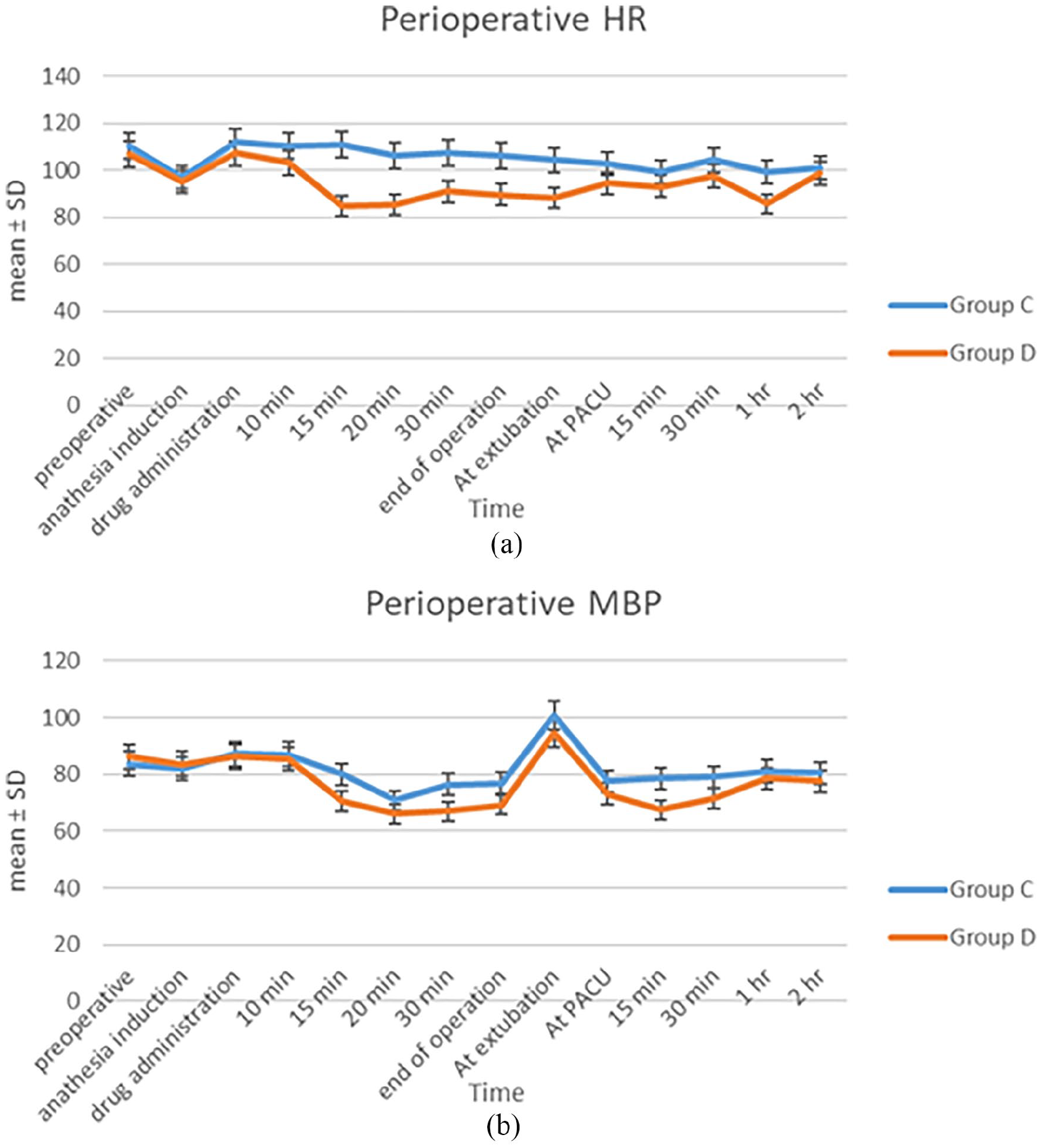
(a) Comparison between the studied groups regarding heart rate at different follow-up periods. (b) Comparison between the studied groups regarding mean blood pressure at different follow-up periods
Cough severity score
When patients were being extubated and five minutes after being extubated, the dexmedetomidine group’s cough score was considerably lower than that of the control group (p < 0.050). In addition, the proportion of Grade 2 and 3 patients in the control group was 33.3% (10/30), which was significantly greater than the percentage in the dexmedetomidine group, which was 10% (3/30), at the time of extubation. While at five minutes after extubation, they represented 26.7% (8/30) and 3.3% (1/30) of patients in the control and dexmedetomidine groups, respectively. Intratracheal administration of dexmedetomidine significantly reduced mean time to awareness and time to extubation compared to controls (p < 0.001). Agitation during recovery occurred in 13.3% (n = 4) of patients in the dexmedetomidine group and 43.3% (n = 13) in the control group (p = 0.020). Agitation scores were significantly lower (p < 0.050) in patients of dexmedetomidine group (Table 2).
Comparison between the two groups as regards cough severity score, awareness time, extubation time and agitation scale
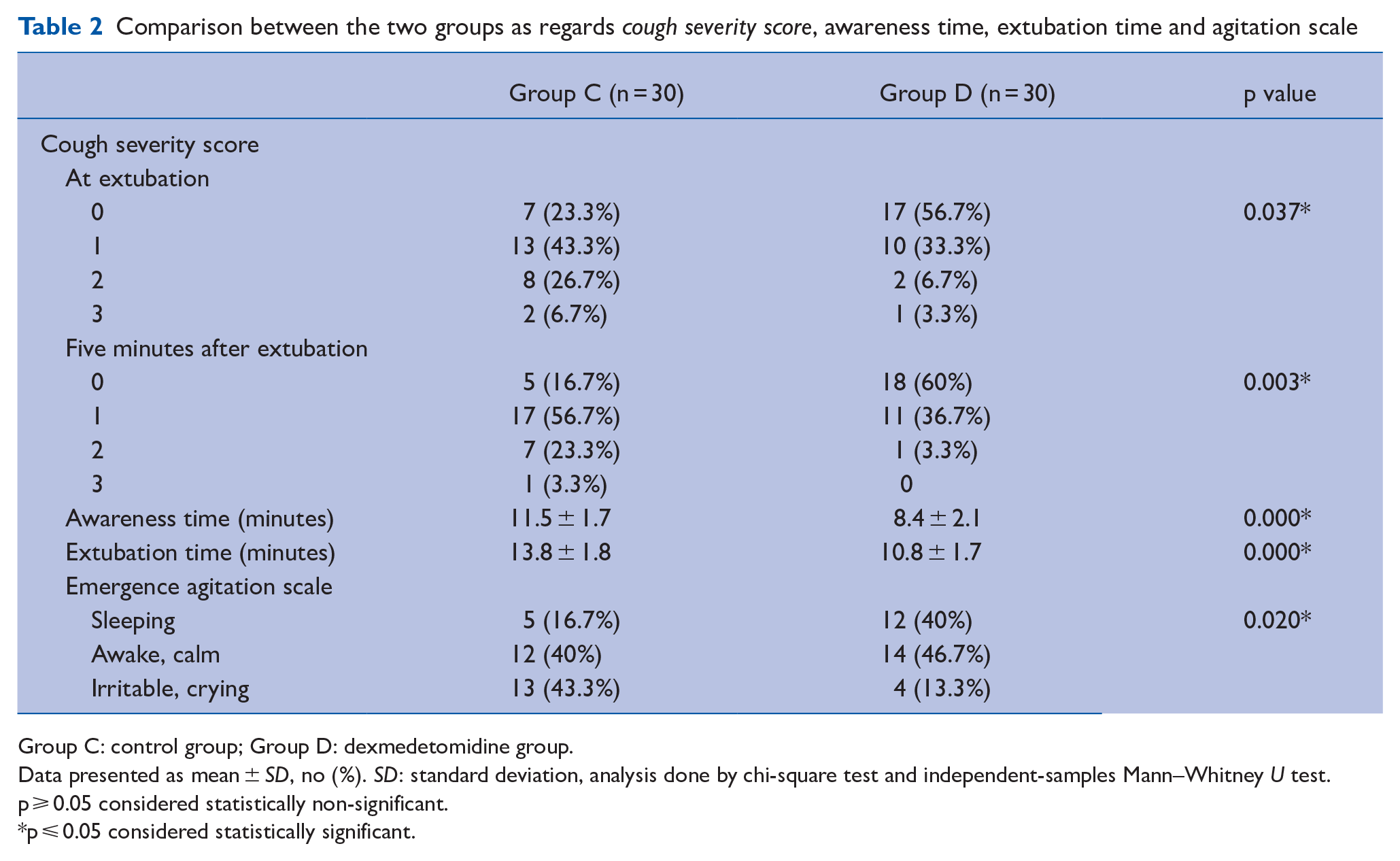
Group C: control group; Group D: dexmedetomidine group.
Data presented as mean ± SD, no (%). SD: standard deviation, analysis done by chi-square test and independent-samples Mann–Whitney U test.
p ⩾ 0.05 considered statistically non-significant.
p ⩽ 0.05 considered statistically significant.
Postoperative pain profile: the Paediatric Objective Pain Scale: In the postoperative period, the pain scores in the dexmedetomidine group were significantly lower. It was statistically significant over the first four hours, from baseline to four hours, with a p value of < 0.050. The difference in pain scores between the two groups converts statistically insignificant at other study time points with a p value of > 0.050 (Figure 3).
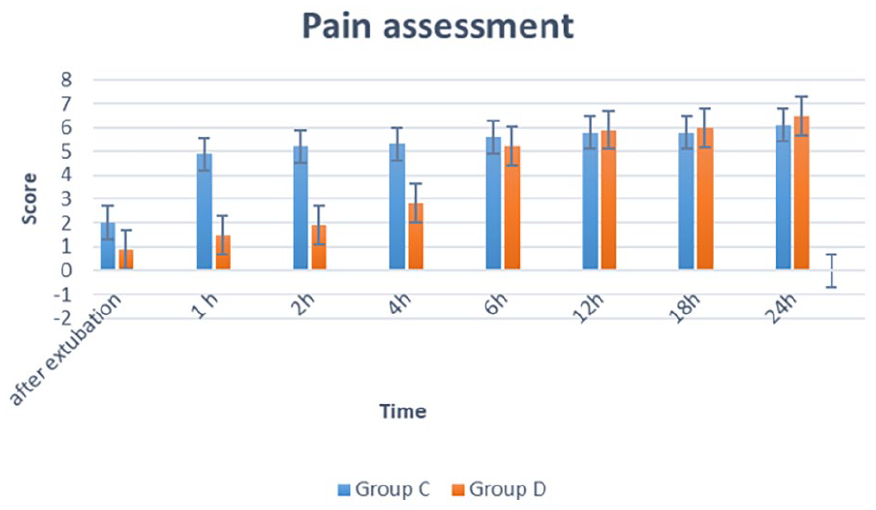
Comparison between the studied groups regarding pain at different follow-up periods
Analgesic request and consumption: The mean time to first request for IV paracetamol rescue analgesia was significantly longer in the dexmedetomidine group (188.9 ± 32.9 minutes) than in the control group. (34.9 ± 6.6 minutes; p < 0.001). The mean total consumption of rescue analgesia in the first 24 hours postoperatively was significantly lower in the dexmedetomidine group (p < 0.050) (Table 3).
Comparison between the two groups as regards time to first rescue analgesics, total analgesic consumption, number of analgesic doses/24 hours, satisfaction score
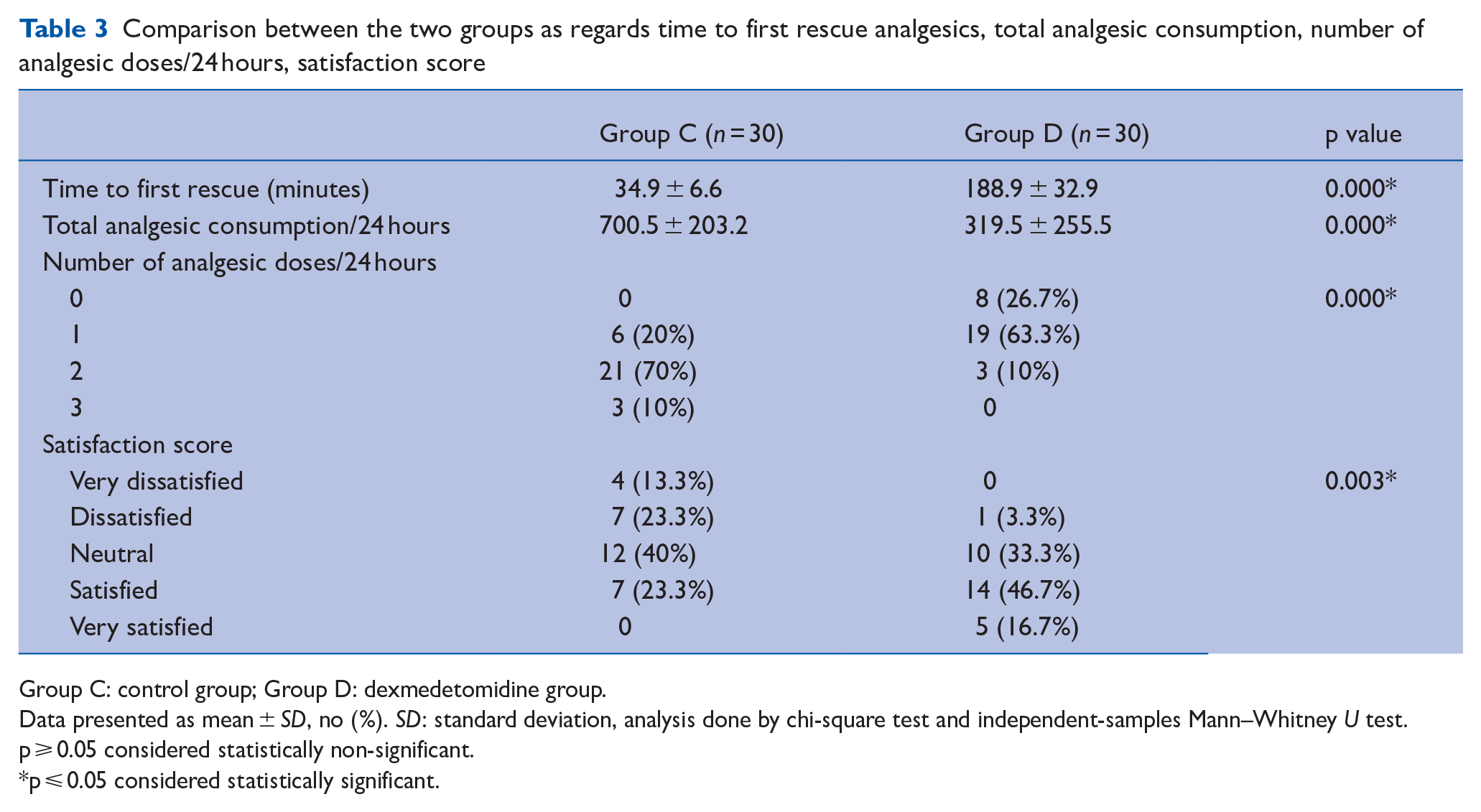
Group C: control group; Group D: dexmedetomidine group.
Data presented as mean ± SD, no (%). SD: standard deviation, analysis done by chi-square test and independent-samples Mann–Whitney U test.
p ⩾ 0.05 considered statistically non-significant.
p ⩽ 0.05 considered statistically significant.
Side effects: There was no statistically significant difference in the incidence of adverse effects, such as hypotension or bradycardia. The frequency of PONV did not vary between the two groups.
RSSs in the first 24 hours postoperatively declined in both groups. The mean sedation values in the dexmedetomidine group were significantly higher until almost one hour postoperatively (p < 0.001). Different study time points showed no statistically significant change (p > 0.05).
Parent satisfaction: Measured using the Likert-type scale, was acceptable (very satisfied, satisfied, or neutral) in 96.6% of patients in the dexmedetomidine group compared with 63.3% of patients in the control group (p = 0.003) (Table 3).
Discussion
The findings of this study show that, as compared to the control group, intratracheal administration of dexmedetomidine decreased the severity of cough seen in patients recovering from abdominal surgery at the time of extubation. Dexmedetomidine, when administered intratracheally in the current trial population, did not cause any undesirable reactions in the airways, and also stabilised haemodynamic effects, enhanced the quality of early recovery and lowered the patient’s pain score. The present study found that intratracheal administration of dexmedetomidine is also an effective way to prevent the laryngeal reactions observed upon recovery from GA.
When IV delivery is not possible in an emergency, it has been observed that intratracheal medicine can give a quick way to penetrate systemic circulation (Wang et al 2018). Intratracheal administration has been effectively used to give a wide range of medications in various clinical contexts, such as employing lidocaine sprays during tracheal intubation (Mussavi et al 2015). When an IV line cannot be established, the intratracheal delivery of dexmedetomidine may serve as an alternative procedure.
The safety and efficacy of administering intratracheal dexmedetomidine during recovery from GA have only been the subject of a small number of investigations. According to Patton et al, the lung is a natural fast absorption site for several small-molecule and therapeutic medicines. At a molecular weight-dependant rate, hydrophilic and hydrophobic peptides and proteins might pass through the pulmonary epithelium (Patton et al 2004).
We assumed that dexmedetomidine, a tiny hydrophilic molecule, was absorbed intratracheally in the current study to produce its pharmacological properties.
Previous study has shown that dexmedetomidine, when administered intravenously at a dose of 0.5μg/kg, might considerably enhance recovery by lowering the frequency of emerging agitation in children (Hauber et al 2015).
According to the present study, a single dose of intratracheal dexmedetomidine (0.5μg/kg) was utilised to significantly reduce postoperative pain and coughing, without experiencing any serious adverse effects. To the best of our knowledge, this was the first randomised controlled trial to investigate how paediatric patients recovered from GA using intratracheal dexmedetomidine.
The decrease in sympathetic and sensitivity of the laryngeal nerve after extubation following intratracheal dexmedetomidine treatment, may be partially responsible for these results (Bhutia & Rai 2017). It is thought that intratracheal dexmedetomidine quickly passes via the bronchial and alveolar capillary network to have its desired effects, such as preventing the rise in HR and blood pressure that occurs in reply to sympathetic signals (Chen et al 2016). Dexmedetomidine has also been demonstrated to reduce the likelihood of traumatic injuries to the throat and vocal cords, reduce hyperalgesia and pain stimulation, and provide global haemodynamic stability (Yang et al 2017, Yuan et al 2017).
In particular, previous studies have established the efficacy of intranasal dexmedetomidine as a sedative premedication to induce beneficial perioperative anxiolysis (Lu et al 2016) and decrease emergence agitation through recovery from GA (Mukherjee et al 2015). Rani et al (2016) also found that a single dose of dexmedetomidine administered intravenously 15 minutes before extubation could prevent the airway reflex during the GA recovery period.
Dexmedetomidine is a highly selective α2 adrenoceptor agonist that has also been shown to stimulate α2a adrenoceptors in the locus coeruleus and have hypnotic effects (Khan et al 1999). Dexmedetomidine can thus facilitate an early and pain-free recovery in addition to its hypnotic and possibly analgesic benefits in reducing postoperative pain (Panchgar et al 2017). The potential side effects of dexmedetomidine include hypotension, bradycardia and delayed recovery (Geng et al 2016, Wu et al 2016). In our current trial, none of these side effects were observed, which may be partly attributed to the appropriate dose of dexmedetomidine (0.5μg/kg). In addition, because there were only 30 participants in each group, some uncommon, or less common, unfavourable side effects from dexmedetomidine administration intratracheally may have not been visible. Three patients had PONV, although it was rather mild, and they all recovered on their own.
Limitations
This study has some limitations, which need to be considered. First, intratracheal dexmedetomidine administration’s absorption characteristics, pharmacokinetics and pharmacodynamics still need more exploration. This was a preliminary study, and more evidence is now essential to support the broader clinical use of this method. Second, only 60 paediatric patients were included in this study, and a larger number of patients, from several centres worldwide, are now needed to settle the results and noted frequent adverse side effects from dexmedetomidine intratracheally. Third, the existing study only verified a single dose of dexmedetomidine (0.5μg/kg). Therefore, the dose-dependent effects of intratracheal dexmedetomidine on airway reflexes should be discovered soon.
Conclusion
The present study provided new visions into the perioperative use of dexmedetomidine. It was shown that intratracheal dexmedetomidine at a dose of 0.5μg/kg, 30 minutes before the end of surgery, resulted in smooth extubation and balanced anaesthesia recovery during lower abdominal surgery. Therefore, intratracheal dexmedetomidine may be another method to avoid the laryngeal reaction arising from GA.
Key points
The present study provided new visions into the perioperative use of dexmedetomidine.
It was shown that intratracheal dexmedetomidine at a dose of 0.5μg/kg, 30 minutes before the end of surgery, resulted in smooth extubation and balanced anaesthesia recovery during lower abdominal surgery.
Therefore, intratracheal dexmedetomidine may be another way to avoid the laryngeal reaction from general anaesthesia.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Contributorship
MMAR is responsible for design, concept, literature search, manuscript preparation, editing, review and final drafting. GMAE is responsible for classification of academic content, literature search and manuscript review. WNA is responsible for clinical studies, editing and review. FBM is responsible for literature search and review. EAO is responsible for clinical studies, methodological design and final drafting.
IRB
17101206.
Clinical trial registration
NCT04385602.