
Abstract
Background:
Treatment for frozen shoulder (FS) focuses on pain control and restoring movement and strength through physical therapy. We aimed to evaluate the efficacy of pulsed radiofrequency (PRF) lesioning of the suprascapular nerve for the treatment of FS pain.
Methods:
Forty patients with FS were enrolled and randomly assigned into the intervention group (n = 20) that received PRF and a control group (n = 20) which received medical treatment (NSAIDs). Patients were followed-up for a total of three months. The primary outcome was the pain intensity, measured by the Numeric Pain Rating Scale (NRS). The secondary outcomes included shoulder range of motion (ROM) evaluation measured by simple shoulder test (SST); Likert-type-based patient satisfaction scale; and any adverse events (AEs) throughout the treatment period. All results were measured at baseline, at the end of one week, four weeks and 12 weeks after treatment.
Results:
At 12 weeks post-procedure, the intervention group significantly improved their pain (NRS dropped to 2.80 ± 0.5) and there was significant improvement in range of motion (SST from 6.55% ± 2.0% to 76.50% ± 6.5) compared to control group.
Conclusions:
PRF lesioning of the SSN is a fast and effective modality in treating frozen shoulder pain and improving ROM for three months.
Keywords
Frozen shoulder (FS) is one of the most prevalent and difficult clinical conditions seen in pain clinics. This is a condition that causes a significant reduction in the active and passive range of motion (ROM) of the glenohumeral joint, as well as pain. Adhesive capsulitis (AC), also known as frozen shoulder is a painful and disabling illness that affects the shoulder capsule and causes inflammation and stiffness. The discomfort is usually persistent, and it is exacerbated at night and in cold temperatures. The illness is thought to be triggered by an injury or trauma to the area, and it may also have an autoimmune component (Bridgman 1972).
Frozen shoulder can be a primary or idiopathic condition, or it can be linked to another systemic disorder, the most prevalent of which is diabetes. The incidence of FS is rising due to an increase in comorbidities and changes in lifestyle (Griggs et al 2000).
Treatment focuses on pain control and the restoration of movement and strength through physical therapy. Common conventional treatments for frozen shoulders consist of glucocorticoids, non-steroidal anti-inflammatory drugs (NSAIDs) taken orally or as intra-articular injections, and / or physical therapy (Wong & Tan 2010).
Depending on the patient’s symptoms and the stage of the condition, a variety of physical therapy and home exercises could be utilised as an initial treatment for AC (Hsu et al 2011).
The purpose of frozen shoulder surgery is to loosen and expand the rigid joint capsule. Manipulations under anesthesia (MUA) (Ewald 2011) and shoulder arthroscopy (Baums et al 2007) are the most widely used methods. Uncontrolled manipulation under anaesthesia could result in structural injury to the glenohumeral joint and surrounding soft tissues (Kraal et al 2019).
There are two methods of implicating radiofrequency (RF): continuous radiofrequency (CRF) and pulsed radiofrequency (PRF). CRF involves a high degree and continuous high temperature reaching up to 90°C, leading to direct tissue degeneration. CRF ablation has good outcomes in pain control, but has intolerable side effects as annoying numbness and dysesthesia (Van Zundert et al 2003).
PRF is recognised to have a pain-relieving effect comparable to that of a corticosteroid injection, with almost no major side effects. Therefore, it is often used to treat several types of pain, such as neuropathic pain, joint pain, discogenic pain and muscle pain (Park & Chang 2022). PRF is a variation of the conventional continuous radiofrequency (CRF) that was used since the mid-1970s. It offers the advantage of pain control without the tissue destruction and painful consequences associated with CRF. Which considered attractive in neuropathic pain management (Byrd & Mackey 2008).
It is difficult to eradicate chronic shoulder pain. The patient’s capacity to conduct physiotherapy is frequently limited by the pain. As a result, the authors planned to use a simple shoulder test to examine the efficacy of ultrasonography (USG)-guided PRF lesioning to the suprascapular nerve in alleviating pain in frozen shoulder patients (simple shoulder test (SST)).
Materials and methods
The Medical Research Ethics Committee Faculty of Medicine, Assiut University (Ref 17100442), approved this prospective randomised blind clinically controlled trial, which was registered at clinicaltrials.gov (NCT03456531) and follows the Helsinki Declaration standards.
This study was carried out at the Assiut University Hospital Pain Clinic, in the period from 15 March 2018 to 1 March 2020. After discussing the study in detail with the patient, a formal informed permission was obtained. Patients were advised that they had the option to withdraw their permission at any moment and that they could cancel their participation without having any negative consequences.
Study population
Forty adult patients with a frozen shoulder suffering for more than three months were enrolled. They were all over 30 years old, with ASA physical status I–II, and came from locations close to our hospital, making follow-up simple and thorough. Random blood glucose was measured before intervention. Those with history of trauma or fracture, coagulopathy or other bleeding diathesis, infection at site of injection, history of chronic opioid use, pre-existing neurologic deficit in targeted region, and those who declined to participate, were excluded from the study.
All of the patients were treated with pain-relieving physiotherapy. These exercises consist of gentle shoulder mobilisation exercises within the range of motion that can be tolerated (eg: pendulum exercise, passive supine forward lift, passive external rotation and range of motion with active support in extension, horizontal adduction and internal rotation). Before beginning these exercises, a hot pack was used as a pain reliever (Järvinen et al 2005). Then patients start with short movement exercises (1–5 seconds), with a somewhat pain-free range three frequently performed stretching exercises. Patients also tried the tolerated pulley exercises and the release of neck or shoulder blade muscles (Diercks & Stevens 2004). Forward shoulder support should be avoided by all patients because it can cause glenohumeral flexion and abduction to be lost. Isometric or static contractions, resistance band workouts, free weights and weight machines are all examples of strengthening exercises. The therapy protocol included rotator cuff exercises, as well as posture exercises and deltoid and thoracic muscle workouts (Donatelli et al 2014).
Home exercises should be continued within the tolerance level; it was indicated – specifically, stretching manoeuvres for the chest muscles and the muscles in the rear of the shoulder. Rotating before elevation exercises, such as an external rotation stretch, is indicated to reduce worsening discomfort and inflammation. Exercises that stretch the chest muscles, while also strengthening the scapular muscles, are known as scapular retraction exercises. External isometric rotation of the shoulder was also used for flexion or abduction within the available range. A physical medicine and rehabilitation specialist also accompanies home exercises in each face-to-face session beginning three months prior to RF registration and three months after RF enrolment.
These exercises were done five to six times per day. Patients were informed that several sessions of five to ten minutes a day are important as the shoulder becomes stiff again between sessions (Chan et al 2017).
Randomisation and blinding
The secretary of the pain clinic made a computer-generated random assignment. The instructions to do USG-guided radiofrequency to suprascapular nerve (SSN) or receive medical treatment were produced and sealed in opaque, sequentially numbered and coded envelopes. After randomisation, the patient data (demographic characteristics and Numeric Pain Rating Scale (NRS), and SST scores) were completed by another physician who did not know what treatment the patients would receive. The same doctor performed the post-treatment tests (PSTs) at one week, one- and three-month follow-ups, and the data were recorded.
The study participants were divided into two groups. Group A included 20 patients who received ultrasonography (USG) guided PRF for six minutes to SSN. Group B included 20 patients who received NSAIDs as part of their medical treatment.
Study protocol
Prior to the intervention, an intravenous cannula was put in place, and patients were monitored (pulse oximeter, non-invasive blood pressure (NIBP) and electrocardiogram (ECG)). All the procedures were undertaken by a single operator to reduce individual technical alterations
PRF to SSN technique:
The affected shoulder was wrapped with antiseptic bandages and draped. The SSN was located using a high frequency (5–12Hz) USG linear probe (with a sterile probe cover). To locate the suprascapular notch, the probe was put over the scapula’s spine. An in-plane method was used to introduce a long 22-gauge spinal needle from the probe’s medial side in an attempt to reach the suprascapular notch under the superior transverse scapular ligament. Following proper needle tip alignment, 2mL of 1% lidocaine was administered to anaesthetise the point of RF cannula entry through the skin. Then, a straight radiofrequency cannula (Neurotherm) with a 20-gauge needle, 5cm length, 5mm active tip, was inserted through the skin towards the suprascapular notch. Sensory and motor stimulation were conducted after satisfactory needle positioning. When the posterior region of the AC joint, the glenohumeral joint, and the shoulder component were stimulated at 50Hz with a current of 0.5mA, patients complained of paresthesia. Supraspinatus and infraspinatus contractions were identified after motor stimulation at 2Hz. The temperature was set to 42°C. The frequency was set to 2Hz with a pulse width of 20 millisecond. The Neurotherm 1100 Radio-Frequency Machine was used to do three cycles of 120 seconds of PRF lesioning. During and after the procedure, the patient’s vital signs were constantly monitored. One hour after the RF, patients in the PRF group were discharged. Patients were given diclofenac sodium 50mg tab (Voltaren, Novartis) for pain relief after meals if needed, and were told to keep note of their analgesic use.
Control group patients received NSAID diclofenac sodium 50mg tab (Voltaren, Novartis) after meals, three times daily for pain control and rebamipide 100mg (Mucosta, Otsuka) for prevention of gastritis.
Assessment parameters
Demographic and anthropometric data included patient’s age, sex, weight and height, address and contact information. All patients were asked to rate their pain before the procedure using a Numeric Pain Rating Scale (NRS) for pain rating where 0 = no pain and 10 = the most severe pain ever, NRS ⩾ 3 means significant pain and the patient was given analgesia (Paracetamol 500–1000mg) (Johnson 2005). Function of the shoulder and its range of motion were assisted prior to the intervention using the simple shoulder test (Minoughan et al 2018). The scoring was yes = 1 or no = 0 and the original score was 0 = worst and 12 = best, then transformed by the number of yes times / number of items completed × 100 =% of yes answers. All patients were followed up after one week, one and three months to rate their pain using the NRS scale and the function of the shoulder using the simple shoulder test. Patient satisfaction was assessed using the 3-point Likert-type satisfaction score (1 = dissatisfied, 2 = satisfied and 3 = very satisfied) during the follow-up period.
Sample size calculation
The sample size was calculated using the G*Power 3 programme [14]. A minimum sample size of 40 patients was required (split into two equal groups, group A received PRF to the suprascapular nerve (SSN) for six minutes and group B got NSAIDs as medical treatment).
Statistical analysis
The researcher verified the data, encoded it and analysed it with IBM-SPSS 21.0 (IBM-SPSS Inc., Chicago, IL, USA) Descriptive statistics are those that describe something (Ho & Yu 2015). The standard deviations and mean values were determined. The chi-square test was used to compare the frequencies of the different groups. To compare the means of dichotomous data, an independent t-test was employed, whereas for repeated measure comparisons, a paired sample t-test was utilised. Repeated-measure analysis of variance (ANOVA) was used to test the mean differences of data with repeated measures that followed a normal distribution (between groups, within groups and overall difference). A post hoc test was calculated using Bonferroni corrections for pairwise comparisons between the two research groups. It is considered significant when the p-value is equal to or less than 0.05.
Results
Seventy patients were recruited, 46 patients were randomised and 40 were included in data analysis. Four patients in the intervention group (group A) and two patients in the control group (group B) were excluded owed to loss of follow-up. The flowchart followed the EQUATOR guideline (Figure 1).
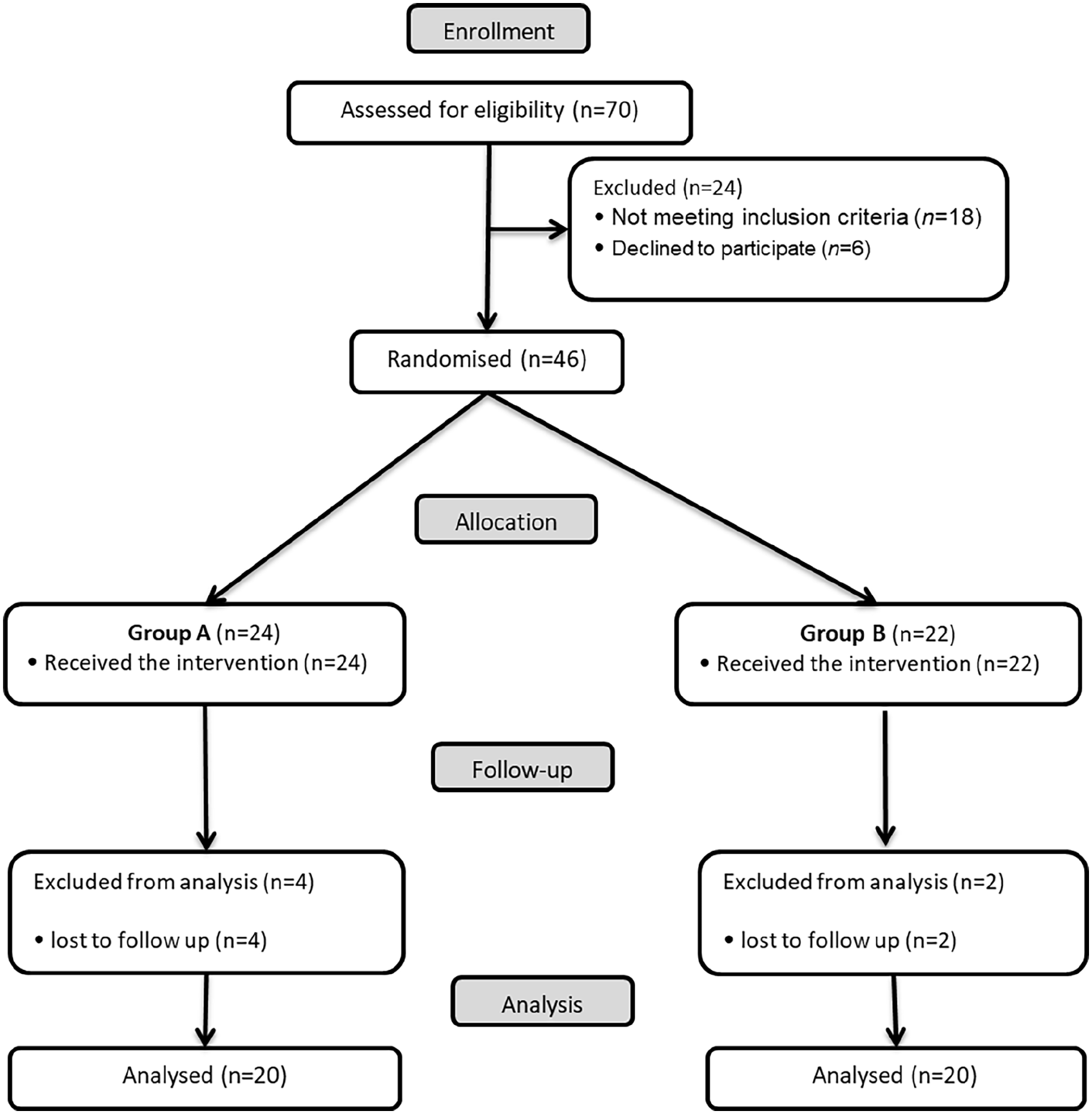
Flow diagram of the participants in this study
There were no significant differences among the groups with respect to age, sex, residence, weight, height, BMI, ASA physical status and random blood sugar (RBS) (Table 1).
Patients characteristics between the study groups
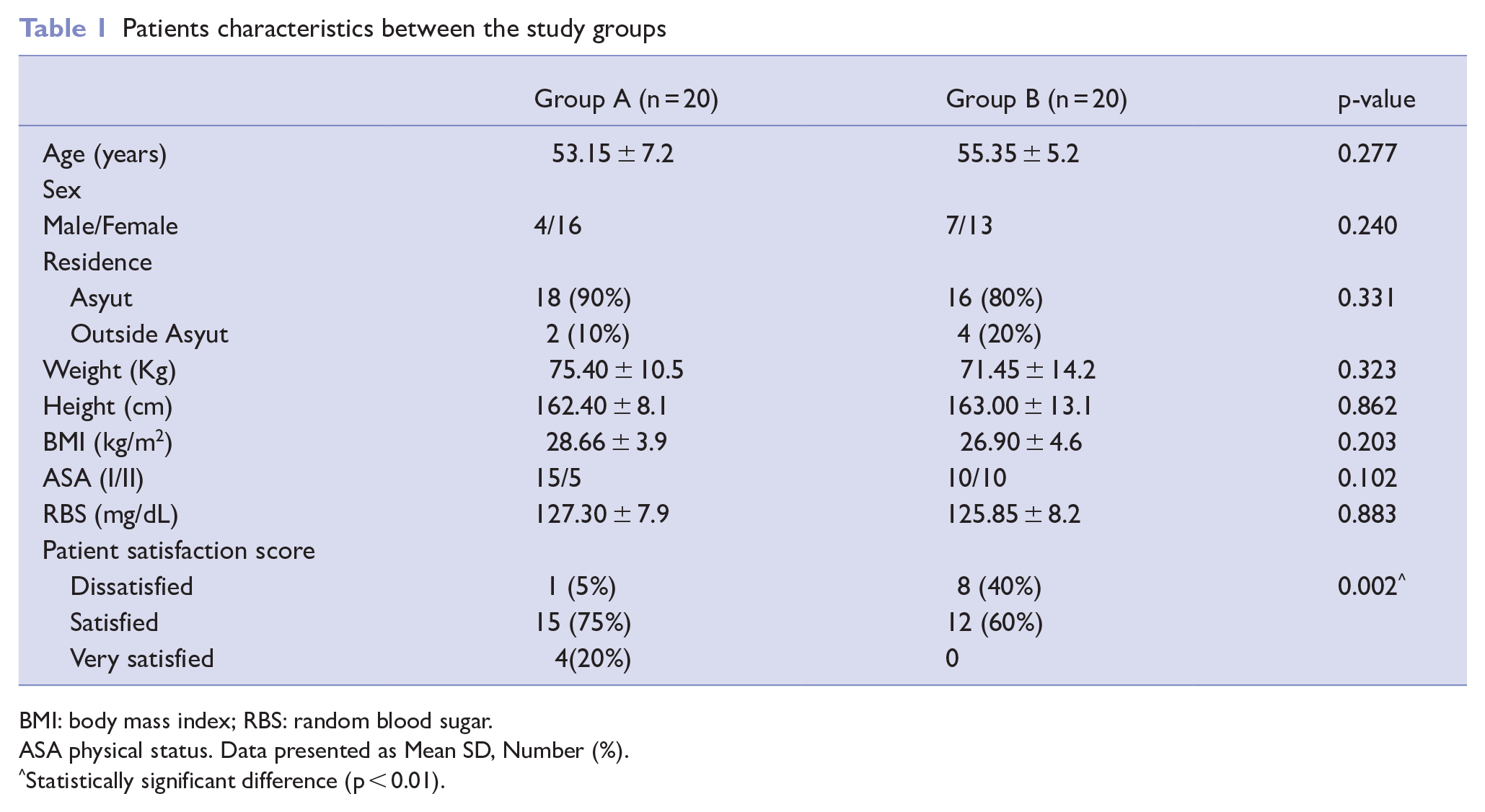
BMI: body mass index; RBS: random blood sugar.
ASA physical status. Data presented as Mean SD, Number (%).
Statistically significant difference (p < 0.01).
Regarding the NRS score it decreased significantly in group A at one week with p-value = 0.004, at one month with p-value < 0.001 and at three months with p-value < 0.001 compared to group B. Repeated-measure ANOVA show statistically significant difference in group A among the three months with p-value < 0.001 and also in group B with p-value = 0.012 (Table 2).
Numeric pain rating scale (NRS) comparisons between groups
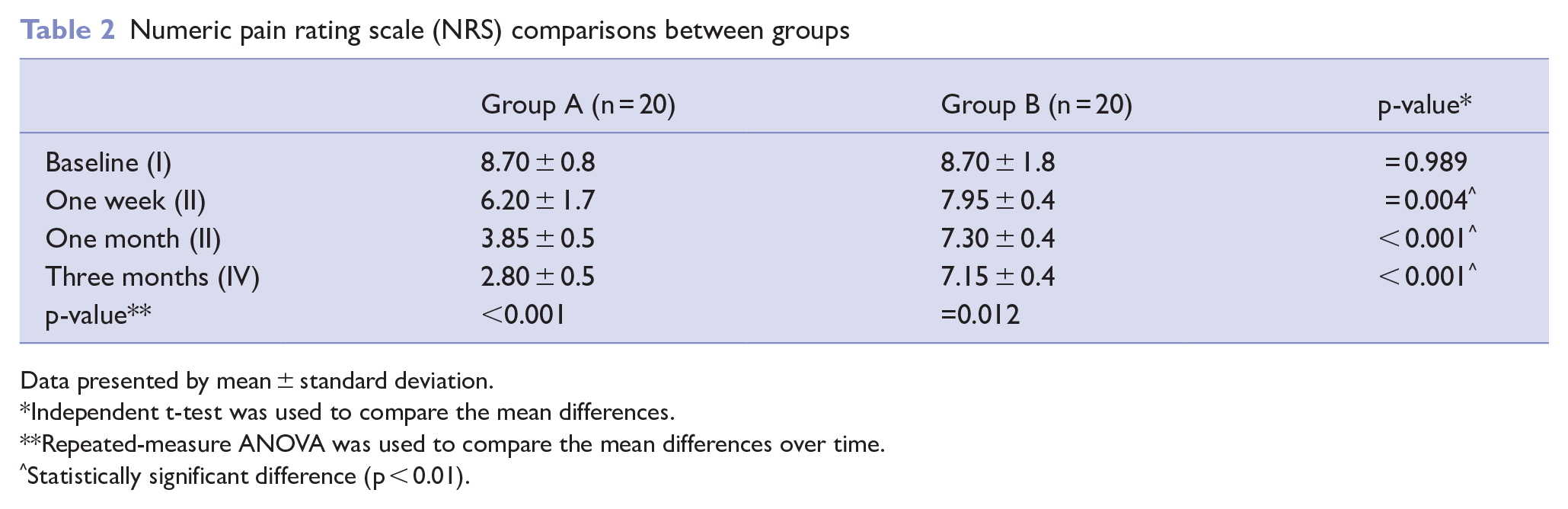
Data presented by mean ± standard deviation.
Independent t-test was used to compare the mean differences.
Repeated-measure ANOVA was used to compare the mean differences over time.
Statistically significant difference (p < 0.01).
Post hoc analysis of repeated-measure ANOVA to equate the mean differences of NRS over time which showed significant decrease between baseline and one week in group A p-value < 0.001, group B p-value = 0.003, between baseline and one month group A p-value < 0.001, group B p-value < 0.001, between baseline and three months in group A p-value < 0.001, group B p-value < 0.001, between one week and one month: in group A p-value < 0.001, group B p-value = 0.006, between one week and three months group A p-value < 0.001, group B p-value = 0.001, and between one and three months in group A p-value = 0.003, group B showed no statistical significance (Table 3).
Pairwise comparison of numeric pain rating scale (NRS) among groups
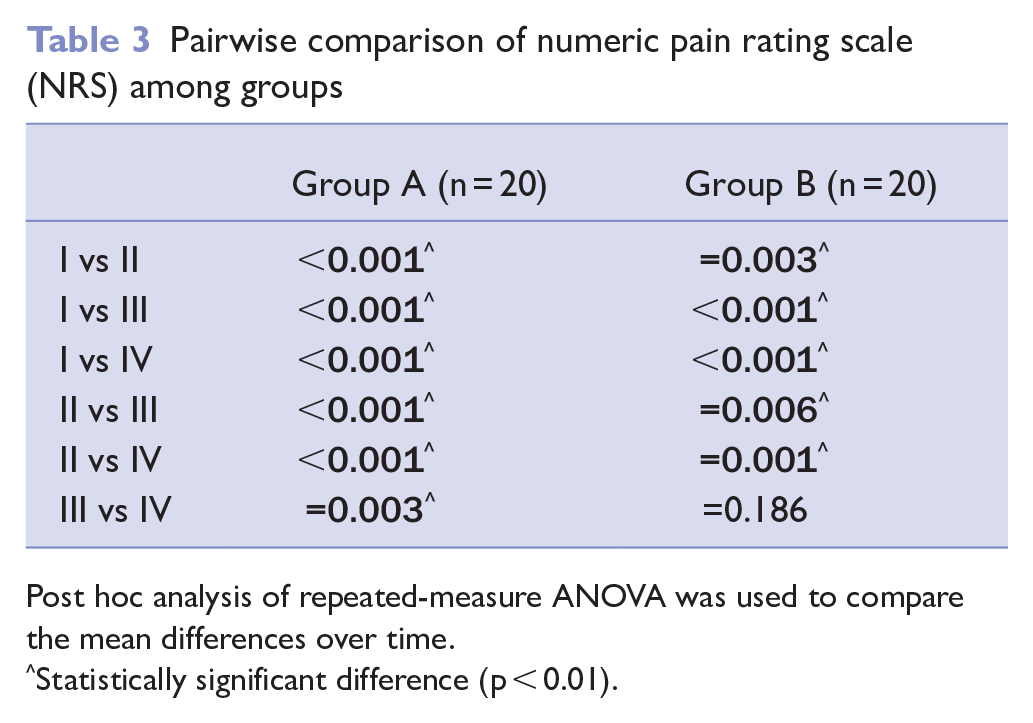
Post hoc analysis of repeated-measure ANOVA was used to compare the mean differences over time.
Statistically significant difference (p < 0.01).
Improvement of shoulder ROM was evaluated using Simple Shoulder Test (SST). Repeated-measure ANOVA showed a statistically significant improvement in group A among the three months with p-value < 0.001 and also in group B with p-value = 0.044 (Figure 2).
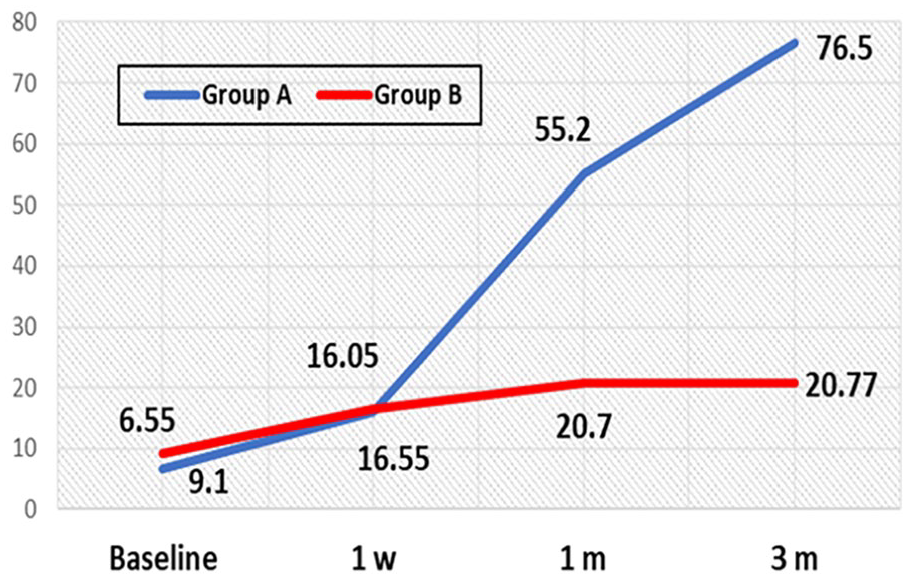
Simple shoulder test (SST) comparison between groups
Post hoc analysis of repeated-measure ANOVA to equate the mean differences of NRS over time which showed significant decrease between baseline and one week in group A p < 0.001 group B p-value = 0.010, between baseline and one month in group A p < 0.001 group B p-value < 0.001, between baseline and three months group A p < 0.001 group B p < 0.001, between one week and one month in group A p < 0.001 group B p-value = 0.038, between one week and three months in group A p < 0.001 group B p-value = 0.038, and between one and three months group A p < 0.001, while in group B show no statistically significance (Table 4).
Pairwise comparison of simple shoulder test (SST) between groups
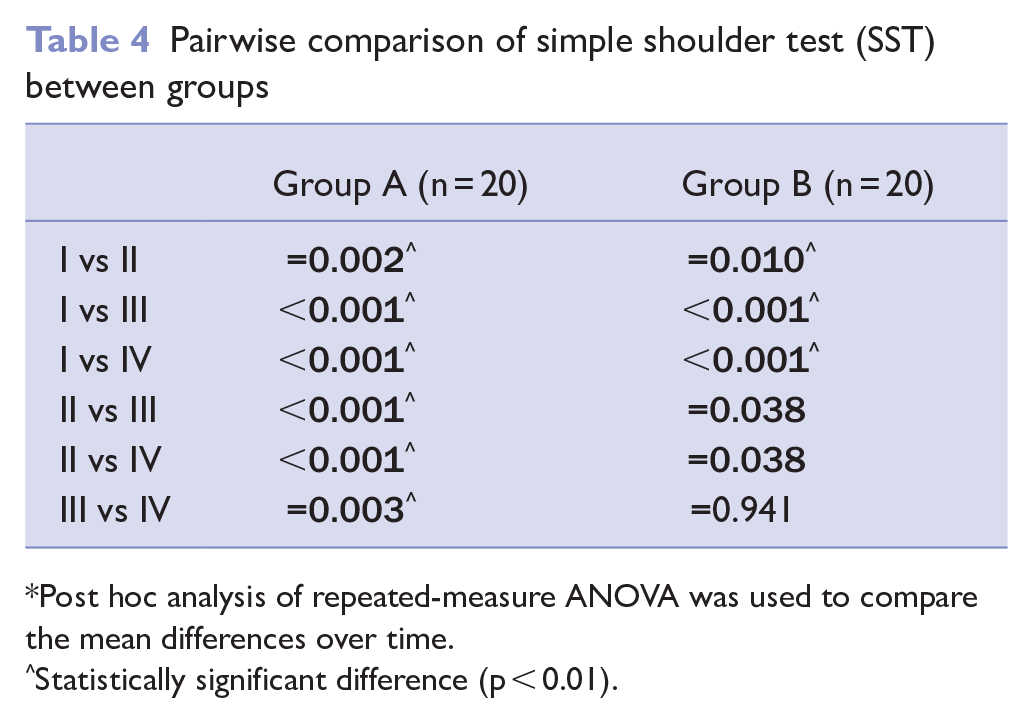
Post hoc analysis of repeated-measure ANOVA was used to compare the mean differences over time.
Statistically significant difference (p < 0.01).
Regarding patient satisfaction score, there was a significant difference between the two groups, where 19 cases in group A were satisfied and very satisfied compared to 12 cases in the group B with p < 0.001 (Table 1).
No major complications were detected in either group during the study period. However, three subjects reported slight pain in the PRF group requiring no treatment.
Only three patients in the study group utilised voltaren tablets 50mg to control their shoulder pain, one of them used it for eight days, while the other two patients continued to use it the whole study period for three months.
Discussion
‘A disorder of varied severity defined by the gradual progression of a total limitation of active and passive shoulder movement that lacks radiological signs other than osteopenia’, is how American Academy of Orthopedic Surgeons defines frozen shoulder.
The efficacy of PRF lesioning of the suprascapular nerve in treating pain in frozen shoulder was investigated in this study, as well as the patients’ shoulder range of motion after the procedure.
In this study, we recruited 40 patients complain of frozen shoulder pain. Twenty cases used PRF lesioning of the suprascapular nerve showed a clear benefit. Eighteen patients had significant pain relief lasting for three months, one patient had partial improvement in pain and ROM, and one patient had no significant change in pain and ROM. While the other 20 patients ‘control group’ received medical treatment ‘NSAIDs’.
The results of this study exposed that the mean numerical rating scale decreased significantly 12 weeks after the procedure. The change in the basic range of motion by SST also improved within three months.
In accordance with our results, in patients with AC, Wu and his colleagues found that using the SSN’s PRF lesion via a ultrasound guided (UG) technique in combination with physiotherapy provided better and faster pain relief, reduced disability and improved ROM than physiotherapy alone, with no complications or serious adverse effects in either group (Wu et al 2014).
Yan and Zhang stated that ultrasound-guided pulsed radiofrequency (UGPRF) showed favourable effects. At the end of six and 12 weeks, pain reduction was measured by visual analog scale (VAS) and progress in shoulder disorder was measured by the Shoulder Pain and Disability Index (SPADI) score (Yan & Zhang 2019).
Jang and partners suggested that PRF of the suprascapular nerve over a nine-month period was an effective treatment for chronic shoulder pain using a VAS and the Oxford Shoulder Score (OSS) (Jang et al 2013).
While Simopoulos et al (2012) tried continuous high-frequency lesions of the SSN, which appear to be a successful treatment for chronic shoulder pain after improving the ROM of the shoulder.
Gofeld with his partners stated that the NRS of the shoulder pain, the Constant Murley score and disability index improved significantly with lidocaine injections alone or in combination with the PRF. After one and three months, patients in the PRF group had satisfaction score more than those in the lidocaine group (Gofeld et al 2013).
Luleci and his coworkers reported that application of the pulsed radio frequency technique to the suprascapular nerve used for 480 seconds displays a notable progress in patients’ chronic shoulder pain using verbal numerical rating scale (VNRS) and modified MacNab score before and six months after the intervention (Luleci et al 2011).
In two patients with acute pain owing to a frozen shoulder, Huang and his assistants employed ultrasound guidance to perform a pulse radiofrequency lesion (PRF) of the suprascapular nerve. For five to six months, the patients had pain reduction and enhanced shoulder flexibility (Huang et al 2010)
Limitations of the current study are (1) small sample size and (2) short post-intervention follow-up time (3 months). Further studies should be done by larger sample size and longer postoperative follow-up.
In conclusion, this study revealed that PRF lesioning of the SSN is fast, safe and effective modality in treatment of frozen shoulder. It allowed good pain control and improved ROM.
Footnotes
Acknowledgements
The authors thank all nurses, residents and other personnel of the pain clinic for their generous cooperation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
The Institutional Research Board approval
The Medical Research Ethics Committee Faculty of Medicine, Assiut University (Ref 17100442).
The study registry
clinicaltrials.gov (NCT03456531).