
Abstract
Background:
Posterior spinal fusion surgery for thoracolumbar scoliosis in the prone position, places the patient at high risk of pulmonary complications. The pressure-controlled ventilation volume-guaranteed mode regulates the inspiratory pressure limits to achieve a set tidal volume with the lowest airway pressure. We hypothesised that pressure-controlled ventilation volume-guaranteed mode would result in improved pulmonary mechanics, gas exchange and lower incidence of atelectasis than ventilation volume-guaranteed mode in patients undergoing corrective surgery for scoliosis in the prone position.
Methods:
Patients of thoracolumbar scoliosis scheduled for posterior spinal fusion surgery were randomly allocated to the ventilation volume-guaranteed (n = 24) or pressure-controlled ventilation volume-guaranteed group (n = 27). As primary endpoints, peak airway pressure (Ppeak), dynamic lung compliance (Cdyn) and arterial blood gas parameters were evaluated at predefined time points. Screening for atelectasis was done by lung ultrasonography on intensive care unit arrival.
Results:
Pressure-controlled ventilation volume-guaranteed resulted in significantly reduced Ppeak and Cdyn as well as lower PaCO2 and arterial to end-tidal carbon dioxide gradient. Both the groups were comparable with regard to oxygenation, hemodynamic variables and total lung ultrasound scores.
Conclusion:
Pressure-controlled ventilation volume-guaranteed confers significant advantages like improved airway mechanics and lower dead space ventilation in patients undergoing corrective surgery for scoliosis.
Keywords
Introduction
Congenital scoliosis (CS) is the failure of vertebral formation and segmentation, or formation or segmentation, during gestation and occurs with an overall incidence of approximately one in 1000 live births (Addai et al 2020). Many of these patients are offered posterior spinal instrumentation and vertebral fusion surgery for the prevention of further cardio-respiratory compromise as well as for cosmetic purposes (Kelly et al 2018).
Patients presenting for scoliosis repair surgery represent a complex clinical conundrum concerning their perioperative respiratory management. Depending on the severity of spinal deformity, these patients exhibit varying degrees of restrictive lung deficit. Furthermore, spinal fusion surgery for scoliosis repair mandates prolonged prone positioning, extensive tissue dissection with potential for blood loss, major fluid shifts, and transfusion of blood and blood products (Tambe et al 2018). The culmination of all these factors produces complex effects on pulmonary physiology and places these patients at a higher risk of postoperative pulmonary complications sometimes requiring ventilator support after the said surgery (Li et al 2020, Redding et al 2020).
The commonly used volume-controlled ventilation mode (VCV) entails the use of fixed-minute ventilation with airway pressure being influenced by pulmonary resistance or compliance. The pressure-controlled ventilation with volume-guaranteed mode (PCV-VG) compares the tidal volume of the previous breath and automatically regulates the pressure limits to achieve a set tidal volume with the lowest airway pressure (Li et al 2022).
Being a relatively newer mode of mechanical ventilation, there is no research as to whether it could provide ventilation benefits in patients presenting for scoliosis repair surgery in the prone position.
This study was conducted with the hypothesis that PCV-VG would result in improved pulmonary mechanics, more effective gas exchange and lower incidence of postoperative lung atelectasis than the conventional VCV mode of ventilation in patients undergoing corrective surgery for scoliosis in the prone position.
Methods
Study design and participants
This prospective comparative single-blinded randomised study trial was conducted after Institutional Ethical Committee approval and clinical trial registration CTRI/2022/02/040361.
Sixty patients scheduled for elective scoliosis repair in the prone position were screened for inclusion in the study.
The inclusion criteria were American Society of Anaesthesiologists (ASA) phyisical classification I and II, of either gender between the ages of 14 and 20 years undergoing posterior spinal fusion (PSF) and instrumentation for mid (T5-T8) and low thoracic (including T9-T12) scoliosis. The patients had a preoperative diagnosis of idiopathic, congenital or neuromuscular scoliosis. The exclusion criteria were body mass index >30kg/m2, concomitant lung disease, cardiovascular disease, preoperative forced expiratory volume in one second (FEV1), and forced vital capacity (FVC) less than 40% of the predicted, maximal inspiratory and expiratory pressures of less than 30cmH2O on pulmonary function test (PFT) and preoperative Cobb angle of >60°.
The dropout criteria included a change of surgical plan to an anterior approach, and unstable hemodynamics, defined as the inability to maintain vitals within 20% of the baseline despite fluid and vasopressor.
This was a patient and evaluator-blinded randomised trial, and randomisation was accomplished using a computer-generated random numbers chart.
Anaesthesia protocol
A standard anaesthesia protocol was used for the induction and maintenance of anaesthesia in both groups. Under ASA standard monitoring, IV propofol (2.5mg/kg) and rocuronium (1.0mg/kg) were administered for induction, and maintenance was achieved using propofol and fentanyl total intravenous anaesthesia (TIVA) as was the standard practice.
The appropriate-sized reinforced endotracheal tube (ETT) was used in all the patients in the study group. We used a bandage tie for securing the ETT as per the unit protocol. After intubation, a fixation bandage or tie was passed underneath the patient’s neck and the two ends were wrapped in front of their neck. A knot was then made around ETT at the desired depth between the incisors and the two ends fixed on the patient’s forehead. After the patient was turned prone, bilateral ventilation was reconfirmed by auscultation of the lung bases. Intraoperative neurophysiologic monitoring was used in all cases.
All the patients were ventilated with a Datex-Ohmeda AVANCE Anaesthesia workstation. In both VCV and PCV-VG groups, the tidal volume was set to deliver 7 mL/kg of ideal body weight, respiratory rate (RR) adjusted to maintain end-tidal CO2 levels of 35–40mmHg, a fraction of inspired oxygen (FiO2) of 0.4, positive end-expiratory pressure (PEEP) of 5mmHg and the inspiratory to expiratory time (I: E) ratio was fixed at 0.5. Hemodynamic variables, respiratory variables, that is, Peak airway pressure
(Ppeak), mean inspiratory pressure (Pmean), dynamic lung compliance (Cdyn), and arterial blood gases were measured in the supine position 15 minutes after the induction of anaesthesia, then at 30, 60, and 120 minutes after placement in the prone position, and finally in the supine position at the end of surgery.
Patients were reversed with neostigmine (0.02–0.04mg/kg) and glycopyrrolate (0.008mg/kg) when the train of four counts was at least three, followed by extubation on fulfilment of recovery criteria. All patients were transferred to the intensive care unit (ICU) for observation and further management.
Lung ultrasonography was performed in a supine position 30 minutes after ICU arrival with a 6- to 12-MHz linear transducer probe by the method described by Monastesse et al and the modified lung ultrasound score (LUS) calculated (Monastesse et al 2017). The magnitude of aeration loss was graded from 0 to 3 as 0 = ⩽2 B lines, 1 = ⩾3 B lines or ⩾1 subpleural consolidations separated by a normal pleural line; 2 = multiple coalescent B lines or subpleural consolidations separated by a thickened pleural line; 3 = consolidation or small subpleural consolidation exceeding 1 × 2cm in diameter. Atelectasis was considered significant when the score was ⩾2 in any region.
The primary outcome of our study was the ventilatory and gas exchange parameters in the intraoperative period. The secondary outcomes were changes in the intraoperative hemodynamics and modified LUS score at ICU arrival.
Statistical analysis
The sample size was determined based on a pilot feasibility study. A difference in Ppeak was observed (25 ± 7.8cmH2O in PCV-VG compared with 30 ± 6cmH2O in VCV). The effect size calculated from this data was 0.82. The sample size required to obtain an alpha error of 5% and power of 80% with an effect size of 0.82 with the allocation ratio of 1:1 was 25 in each group. Given the dropout rate of 10% due to uncontrollable causes, such as blood loss and other surgical complications, 60 patients were recruited and randomised into two groups, using computer-based randomisation. Numerical data were expressed as mean and standard deviation or median and interquartile range as appropriate. Qualitative data were expressed as frequency and percentage. To assess homogeneity of variance, Leven’s test has been performed.
For quantitative data, a comparison between the two groups was done using either the student t-test or the Mann–Whitney test (non-parametric t-test) as appropriate. Values of pre- and post-assessments were analysed by paired t-test or Wilcoxon signed-rank test as appropriate. The chi-square test was used to examine the relation between qualitative variables. The confidence interval was set to 95%, and the margin of error accepted was set to 5%. The p-value was considered significant if <0.05.
Results
A total of 51 patients were included in the final analysis with 24 patients in the VCV group and 27 patients in the PCV-VG group (Figure 1). Both groups were found to be normally distributed for Cobb angle, demographics, intraoperative hemodynamics, and total fluid requirement (Leven’s test) without any statistical significance (Table 1). There was no difference in the groups concerning intraoperative hemodynamics (Figure 2).
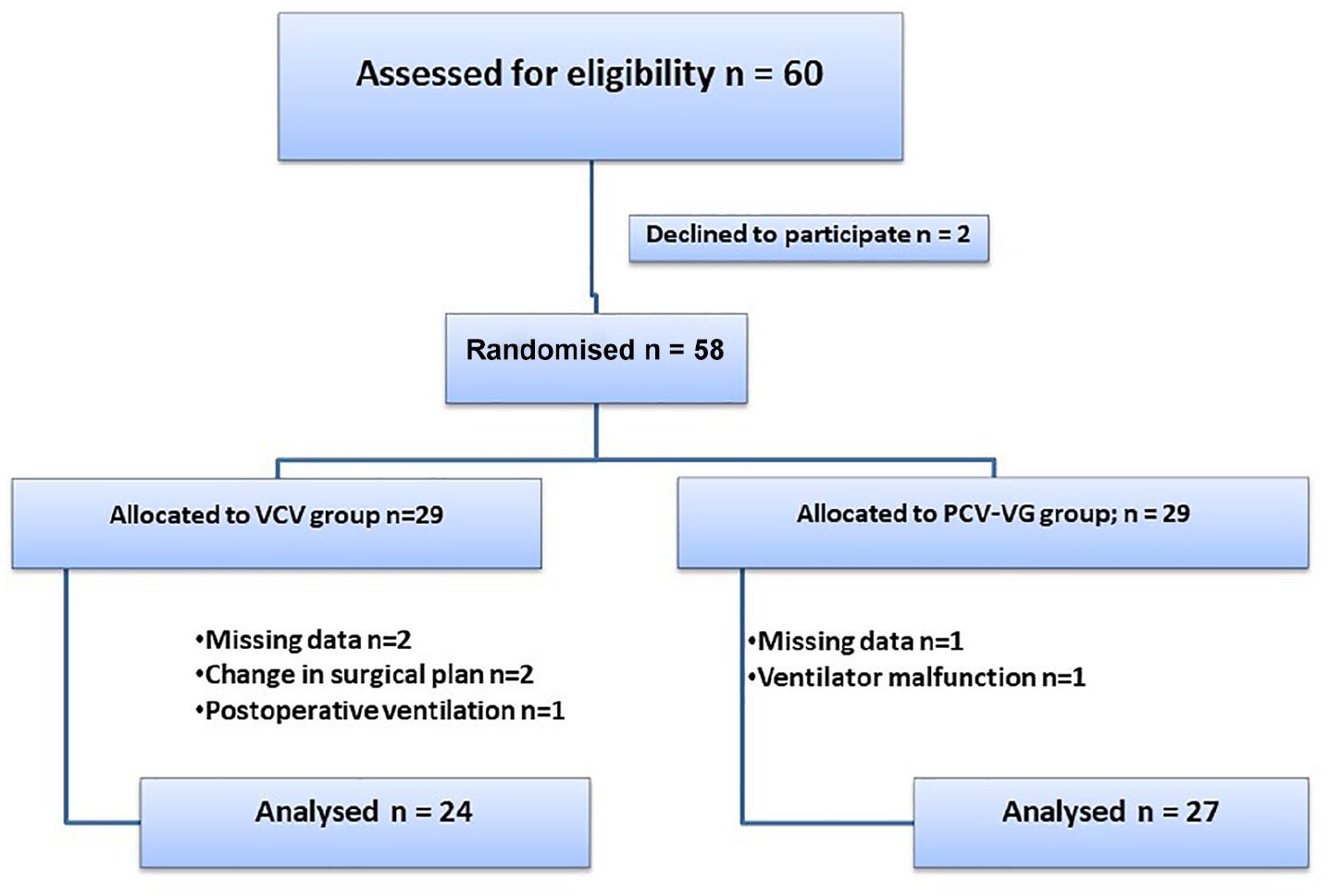
Consort flow diagram for patient recruitment and analysis
Demographic profile and Baseline characteristics
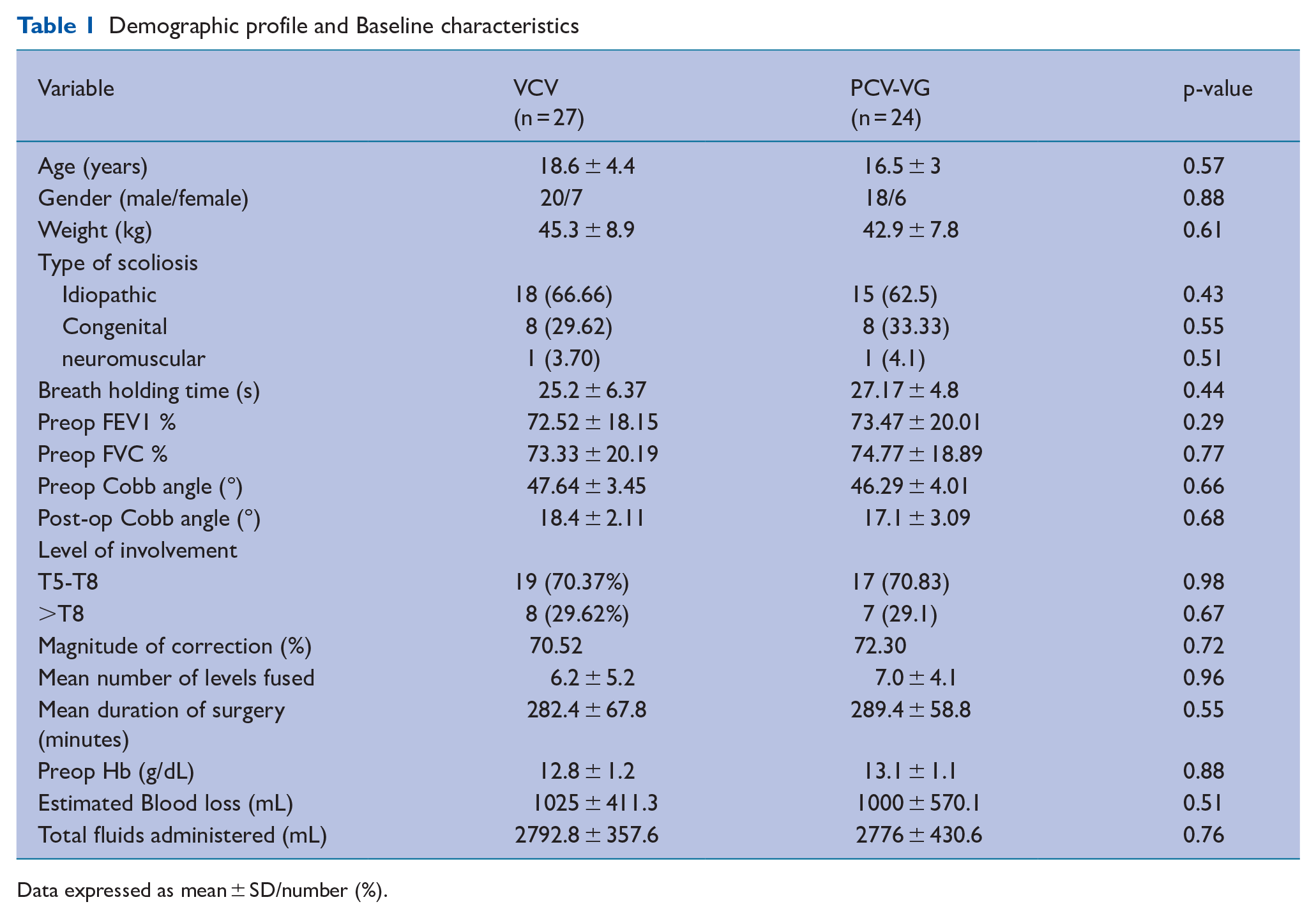
Data expressed as mean ± SD/number (%).
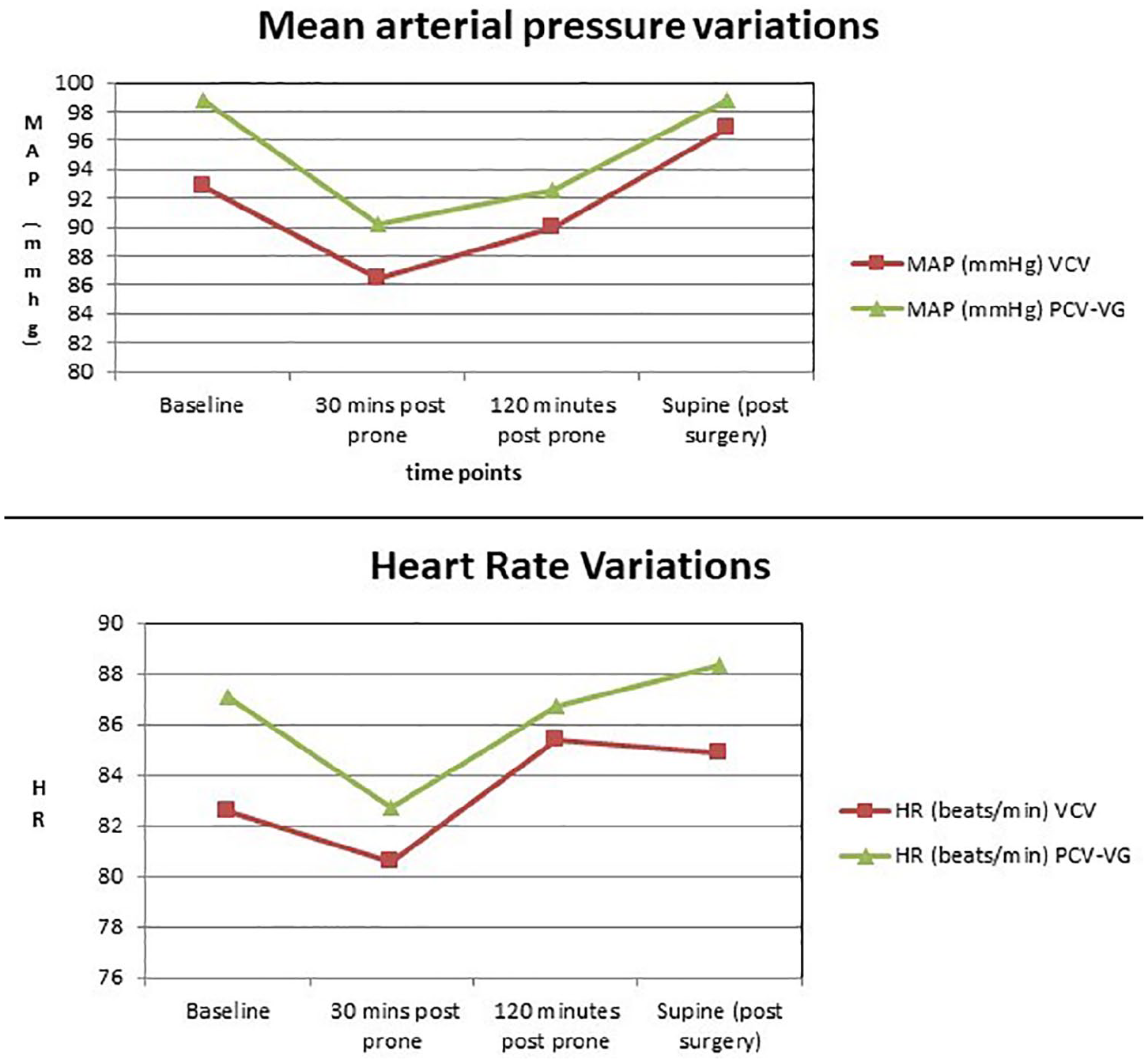
Hemodynamic outcomes
Analysis of the primary outcome, the lung mechanics, revealed that the peak inspiratory pressures increased after prone positioning in both VCV and PCV-VG groups. However, patients ventilated with PCV-VG exhibited lower Ppeak values than in the VCV group at all the recorded time points, which attained statistical significance. Further intragroup analysis revealed that in the VCV group, the peak airway pressures were significantly higher in the prone position as compared with the baseline in the supine position (Table 2).
Pulmonary mechanics
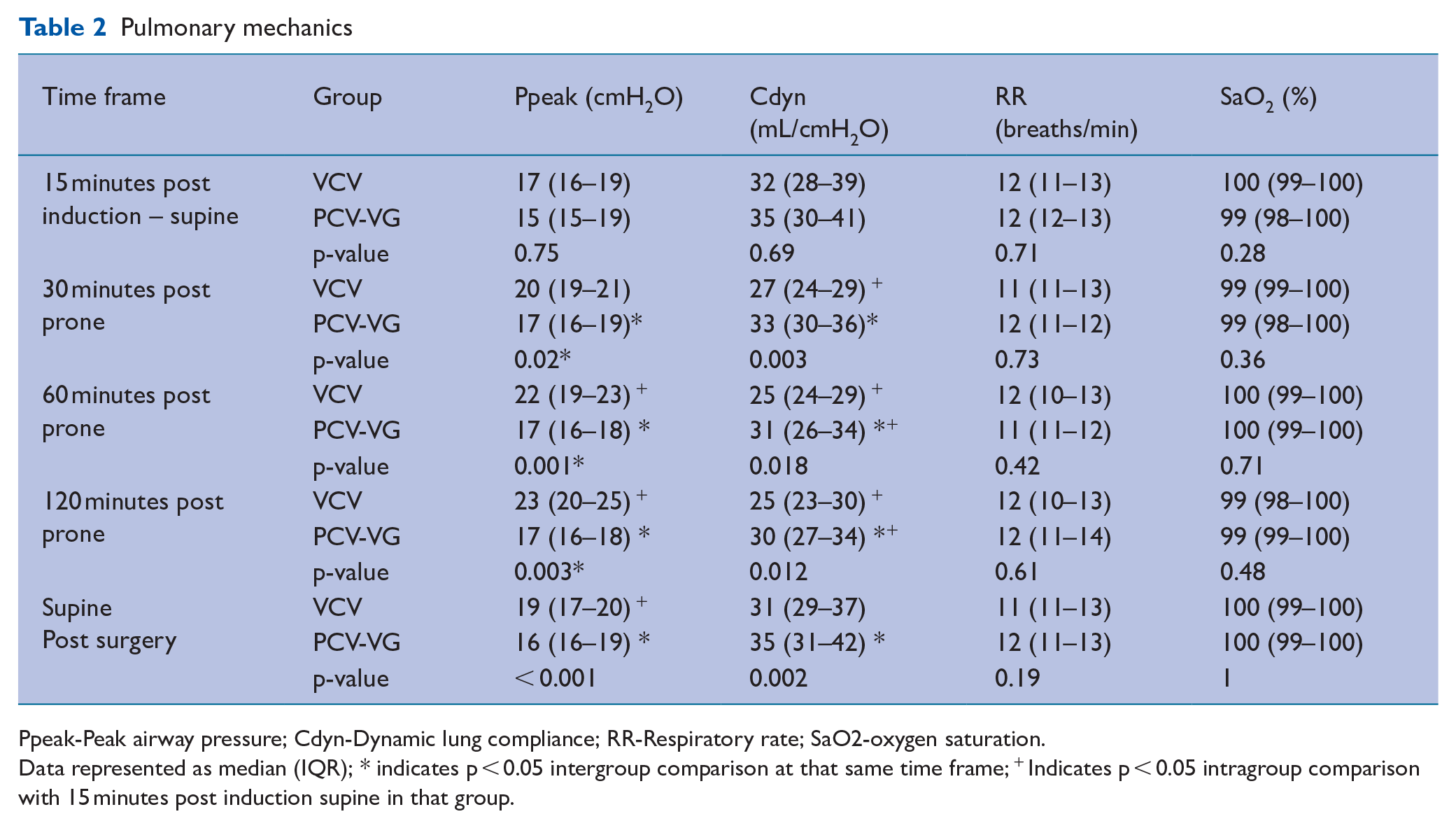
Ppeak-Peak airway pressure; Cdyn-Dynamic lung compliance; RR-Respiratory rate; SaO2-oxygen saturation.
Data represented as median (IQR); * indicates p < 0.05 intergroup comparison at that same time frame; + Indicates p < 0.05 intragroup comparison with 15 minutes post induction supine in that group.
The Cdyn values in the prone position were lower than the supine values in both groups throughout the surgery. There was a statistically significant intergroup variation between VCV and PCV-VG groups with Cdyn in the VCV group being significantly lower at all study points after prone positioning (Table 2).
Statistical analysis of the arterial blood gases, our other primary outcome, revealed that PaO2, PaO2/FiO2 ratio and pH values were comparable at all time intervals in both groups. The PaCO2 levels were significantly higher in the VCV mode at 120 minutes prone position and at the end of surgery. The arterial to end-tidal carbon dioxide gradient which represents the amount of dead space ventilation was lower in PCV-VG compared with VCV mode after 120 minutes of prone position and at the end of surgery after turning supine (Table 3).
Intraoperative ABG parameters
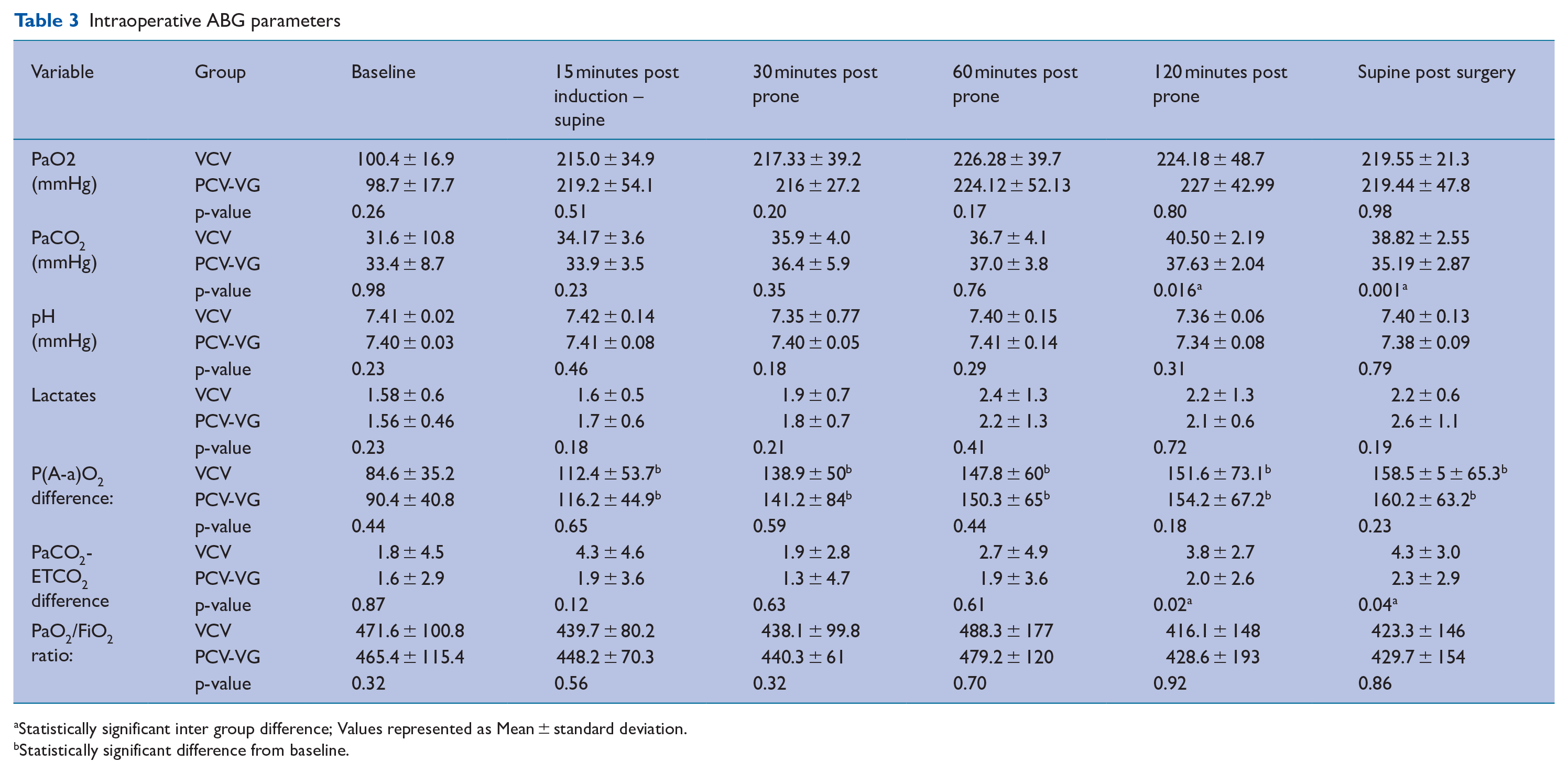
Statistically significant inter group difference; Values represented as Mean ± standard deviation.
Statistically significant difference from baseline.
The Alveolar-arterial gradient (A-a) O2 widened after intubation and was significantly different from the baseline at all time points in both groups. Though the P (A-a) O2 was lower in the PCV-VG group than in the VCV group, the difference between the groups was not statistically significant (Table 3).
There was no significant difference in the incidence of atelectasis and total postoperative lung ultrasound score ICU in the patients ventilated with either VCV or PCV-VG mode (p = 0.213) (Table 4). None of the patients in the study groups had grade 3 atelectasis. There was no incidence of desaturation (SpO2 < 92%) or reintubation and mechanical ventilation in any of the patients in the study population.
Postoperative Lung Ultrasound Score (LUS)
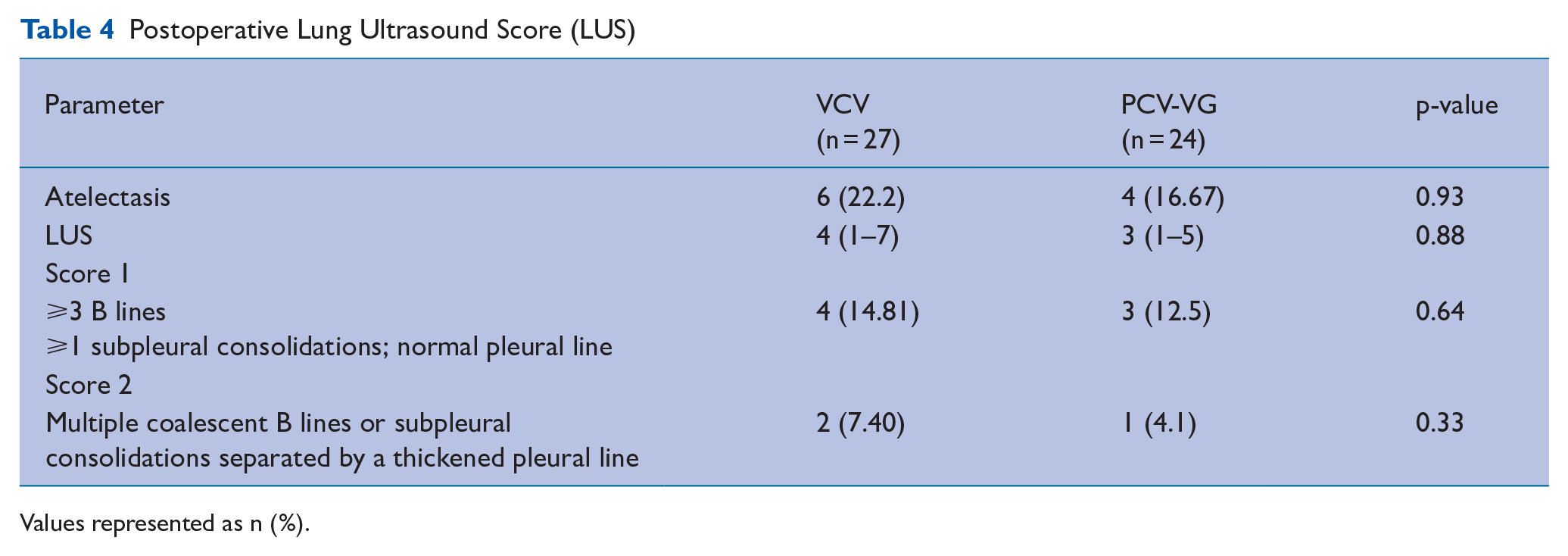
Values represented as n (%).
Discussion
Multiple factors interplay to make the perioperative ventilatory management of scoliosis surgical patients unique and more challenging than other procedures on the spine. The combination of a rigid thoracic curvature, varying degrees of restrictive lung pathology, prolonged surgery in the prone position, and potential for excessive blood loss with multiple vertebral fusions and osteotomy lead to a host of pulmonary repercussions and present themselves as a challenge to the perioperative physician (Ahmed et al 2021).
Thus, strategies aimed at improving the respiratory mechanics and gas exchange in this surgical cohort would form an intuitive goal for the anaesthesia team.
We found that the peak airway pressure of patients ventilated with PCV-VG mode was lower throughout the surgical duration than in the VCV group. This finding should be regarded with significance as any acute lung injury such as that caused by raised intraoperative peak pressures would be poorly tolerated in this particular surgical cohort of patients. The decelerating airway flow characteristic of pressure-controlled ventilation, and digital feedback mechanisms could explain the reduction of the peak airway pressure seen with the PCV-VG mode. Adding substance to our finding, Yao et al (2020) in their study have reported significantly reduced neutrophil elastase levels in patients ventilated with PCV-VG mode.
We established the superiority of the PCV-VG mode in the functional lung parameter dynamic lung compliance during intraoperative ventilation. Dynamic compliance is related not only to the elastic properties but also to the resistive elements of respiratory mechanics such as airway pressure (Ahn et al 2020). Thus, our finding can be substantiated by the fact that PCV-VG mode is designed to deliver the target tidal volume with the lowest possible airway pressure resulting in improved lung compliance.
Although there is no existing research on the topic in patients undergoing scoliosis surgery, similar studies comparing the two modes in other surgical cohorts show diverse results. A review by Schick et al (2021) assessing 929 patients from 17 randomised trials demonstrated that PCV-VG mode provided benefits like better airway dynamics, and improved oxygenation in one-lung ventilation for thoracotomy and laparoscopic surgery. However, the review included only one randomised control trial (RCT) that analysed the effects of PCV-VG mode on 36 patients undergoing lumbar spine surgery in the prone position (Lee et al 2019).
We did not find any benefit in terms of oxygenation between the two modes, though we did find improvements in CO2 removal. The amount of dead space ventilation represented by the arterial to end-tidal carbon dioxide gradient was also significantly lower in PCV-VG mode.
However, we excluded patients with high Cobb angle and poor preoperative pulmonary reserve. Given that this particular patient cohort could particularly benefit from PCV-VG, the effect of PCV-VG on oxygenation might have been underestimated in our study. We found no significant difference between the groups concerning immediate postoperative atelectasis. Although there is no existing literature to agree or refute this finding in scoliosis patients, a randomised control trial by Kim et al (2019) found that the PCV-VG group resulted in better LUS compared with the VCV group.
We did not find any intergroup differences in the two ventilation modes concerning intraoperative hemodynamics and blood loss. The closest reference we found in the literature was a study by Kang et al (2016) who found that PCV mode decreased intraoperative blood loss in patients undergoing posterior lumbar interbody fusion. The authors attributed their observation to the reduced PIP with resultant less inferior vena cava (IVC) compression and spinal venous engorgement seen with the PCV mode. However, we believe that such an inference needs further validation as PIP is not an accurate reflection of the alveolar pressure. To investigate the precise effects of lung expansion during IVC compression and spinal venous engorgement, alveolar and pleural pressures should be obtained and analysed.
Our study was not without limitations.
Double blinding was not possible due to our study design. This however could not have produced any subjective falsification of the data as the measurements of airway pressures, lung compliance, arterial blood gases, and LUS were performed using calibrated equipment.
We did not evaluate patients with higher Cobb angle and severe restrictive lung disease nor did we assess the long-term effects of the ventilation strategies (eg: VCV or PCV-VG).
Finally, to draw significant conclusions to suggest the incorporation of PCV-VG as the new standard for scoliosis surgery, large-scale research with diverse patient cohorts such as those with compromised lung function and neuromuscular scoliosis would be required.
The major strength of our investigation lies in the fact that all our primary and secondary endpoints are objective measurements recorded at definite time points in the intraoperative and immediate postoperative period. This leaves very little room for bias.
Conclusion
This randomised clinical trial suggests that in patients undergoing corrective surgery for scoliosis in the prone position, intraoperative ventilation with PCV-VG confers significant advantages concerning airway mechanics like peak airway pressure, lung compliance, and dead space ventilation as compared with VCV. This investigation did not find any benefit of PCV-VG in terms of oxygenation and immediate postoperative atelectasis. Further large-scale data in patients with compromised lung function and specific aetiologies of scoliosis need to be evaluated to guide clinical recommendations.
Footnotes
Author note
This study has NOT been presented in any conference/preprint servers/other social media and has not received any research grant.
Author contributions
Authorship was based on the following four criteria as per ICMJE (International Committee of Medical Journal Editors) recommendations: Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND drafting the work or revising it critically for important intellectual content; AND final approval of the version to be published; AND agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Institutional support in the form of providing equipment and drugs.
Ethical approval
The manuscript has been read and approved by all the authors, that the requirements for authorship as stated earlier in this document have been met, and that each author believes that the manuscript represents honest work.