
Abstract
Preoperative checklists have demonstrated efficacy in improving patient care in the surgical setting. While the assessment of perioperative risks through patient inquiry is extensive, the menstrual status of the patient is one question that is not frequently discussed. If a patient is menstruating during their surgical procedure, unknown use of an intravaginal menstrual hygiene product, such as a tampon or menstrual cup, places the patient at risk of infection. This review seeks to bring attention to these risks by exploring Boyer v. Morimoto, a case where a patient developed toxic shock syndrome after a tampon was left in after surgery. We conclude with recommendations for standardised documentation of intravaginal menstrual hygiene products, with the aim to minimise perioperative risks.
Keywords
Introduction
The implementation of preoperative checklists has demonstrated efficacy in improving patient care in the surgical setting (Bergs et al 2014). Guided by a standardised set of questions, health care practitioners prepare patients for surgery and reinforce the notion that patient safety is paramount. Patients are often asked the same questions multiple times by staff in different roles to ensure accuracy and appropriate intervention. For example, patients are routinely asked about their medical history, recent tobacco and substance use, and the time of their last meal.
While the assessment of perioperative risks through patient inquiry is extensive, the menstrual status of the patient in non-gynaecologic cases is one question that is not frequently discussed. A 2022 study of menstrual product use in 7394 participants through the Apple Women’s Health Study found that 47% of women used tampons and 19% utilised internal cup menstrual collection devices (Harvard T.H. Chan School of Public Health 2023). If a patient is menstruating during their surgical procedure, the use of an intravaginal hygiene product, such as a tampon, menstrual cup or sponge, may place the patient at risk. Unknown use of a tampon or menstrual cup during emergent or scheduled surgery could place the patient at an increased risk of infection and menstrual toxic shock syndrome (mTSS) (Atchade et al 2024).
Recognition of mTSS did not occur until the late 1970s and early 1980s, as tampon-users began to prolong use due to improvements in absorbent technology. The use of intravaginal hygiene products, such as tampons, creates an oxygen-rich vaginal environment suitable for Staphylococcus aureus (S. aureus). While vaginal colonisation by S. aureus is typically benign, strains of S. aureus that produce toxic shock syndrome toxin-1 (TSST-1) can facilitate toxin-mediated shock by binding to vaginal epithelial cells and crossing the vaginal mucosa. With the prolonged use, the bacteria can multiply and trigger an uncontrolled immune response. This can result in mTSS, characterised by symptoms such as fever, rash, tachycardia, abdominal pain and hypotension that can require vasopressor support.
Changes in tampon absorbency and advocacy efforts have resulted in a decrease in the incidence of mTSS; recent studies estimate an incidence between 0.03 and 0.07/100,000 individuals in the United Kingdom, with the highest proportion of cases in women 13 to 24 years of age (Sharma et al 2018). The United States Federal Drug Administration recommends never wearing a tampon for more than 8 hours at a time (U.S. Food and Drug Administration 2020). Nevertheless, while mTSS can pose a risk if intravaginal menstrual hygiene products are left in during surgery, additional complications can occur if these products are lost or left after surgery. While rare, prolonged retention for days to weeks can result in disruption of the normal vaginal flora due to microbial contamination and the proliferation of bacteria and yeast, including Escherichia coli, Streptococcus pyogenes, Pseudomonas aeruginosa and Candida (Atchade et al 2024).
This review seeks to bring attention to the risks associated with undocumented intravaginal menstrual hygiene product use during the perioperative period. We will examine the case of Boyer v. Morimoto, in which a female patient was diagnosed with TSS after her surgical team failed to communicate with her and each other about her use of a tampon during surgery (Boyer v. Morimoto 2019). We will also discuss recommendations for standardised documentation of intravaginal menstrual hygiene products.
Boyer v. Morimoto
The publicly available case of Boyer v. Morimoto serves as a harrowing example of the critical importance of incorporating menstrual status and intravaginal sanitation reporting into preoperative assessments (Boyer v. Morimoto 2019). In September 2015, after significant weight loss, Kathie Boyer consulted with a plastic surgeon to express interest in cosmetic abdominoplasty and breast augmentation. During the consultation, she mentioned her previous breast implant surgeries and expressed concerns about rippling in her right breast. In October 2015, Boyer underwent an abdominoplasty, breast implant replacement and mastopexy with liposuction. The day of her procedure, Boyer informed her surgical team that she was menstruating, and she was told that it was permissible to wear a tampon during the procedure (Boyer v. Morimoto 2019).
In the days following her operation, Boyer experienced extreme, persistent pain and fatigue. Nine days after surgery, she felt fluctuating hot and cold sensations in her toes and was rushed to an emergency room. Ultimately, the patient was given a diagnosis of hypoxia, cyanosis, acute renal failure and liver injury. Examinations by emergency medicine and infectious disease physicians also revealed a critical oversight from her surgery team—a tampon had been left inside Boyer’s vaginal vault.
Boyer’s subsequent treatment journey underscores the gravity of this oversight; she required intensive care where physicians determined the likely cause of her illness as staphylococcal TSS, most likely related to the retained tampon. Ultimately, Boyer underwent multiple surgeries, including the removal of the distal portions of most of the toes on her right foot.
Boyer filed suit against her surgeon, alleging that they failed to comply with the applicable standard of care. Boyer also contended that nursing staff committed acts of negligence, for which the hospital was vicariously liable. Boyer claimed that her surgeon and the nursing staff agreed to attend to her menstrual cycle during surgery (Boyer v. Morimoto 2019).
Discussion
Boyer’s case highlights the need for transparent communication between patients and medical professionals and robust preoperative protocols that consider all aspects of a patient’s medical history, including menstrual status and use of intravaginal sanitation products. Failure to account for these products can have profound consequences for patient safety and wellbeing, emphasising the urgency of implementing the relevant preoperative screening practices to mitigate risks and ensure optimal surgical outcomes.
In 2014, after a similar incident at Children’s Minnesota Hospital (CMH), when a paediatric patient was left in the paediatric intensive care unit for over 24 hours with a tampon in place, a group of hospital leaders put together a protocol to prevent future harm (Children’s Hospitals and Clinics of Minnesota 2014). This protocol, ‘Tampon Use in the Operating Room,’ notes that tampons, menstrual cups and sponges should be removed before induction of anaesthesia based on the surgeon and anaesthetist’s agreement (Children’s Hospitals and Clinics of Minnesota 2014).
Recommendations
It is not clear how prevalent screening for intravaginal menstrual hygiene product placement is within preoperative checklists. Most perioperative checklists are institution-specific and based on a modified version of the World Health Organization’s safety checklist (Treadwell et al 2014, World Health Organization 2008). Some major health systems and private practice groups recommend avoiding tampon use in favour of menstrual pads in their patient education forms and web pages (OrthoBethesda n.d., PRMA Plastic Surgery n.d., Naval Hospital Lemoore n.d.). Some institutions also include menstrual care-related questions during the preoperative assessment and removal of tampons as an item to be confirmed by a nurse, but this does not appear universal (Gillette Children’s Specialty Healthcare n.d., West Hertfordshire Hospitals NHS Trust 2011).
The protocol utilised by CMH should be considered at other medical facilities where surgeries are performed. This protocol screens for menstrual hygiene product use and requires that patients be provided with a safe alternative (mesh underwear and sanitary pad). In addition, the completion of this step must be documented in the electronic medical record (Children’s Hospitals and Clinics of Minnesota 2014). Therefore, the implementation of an intravaginal menstrual hygiene product removal protocol within the electronic medical record is possible in certain systems.
The CMH protocol includes a statement about informing the patient that the removal of menstrual products is for their safety. Thus, it may be valuable to include brief patient education with an explanation of the risks associated with leaving menstrual products in place during surgery, as patient awareness may help to lower the risk of future adverse events. In addition, the CMH protocol advises staff to remove intravaginal menstrual hygiene products identified in the operating room, thereby eliminating ambiguity on how staff should proceed if a tampon is not removed prior to surgery. Accordingly, the authors encourage medical institutions to share their perioperative protocols for intravaginal menstrual hygiene product removal with the broader community in order to facilitate the standardisation of best practices (Children’s Hospitals and Clinics of Minnesota 2014). Furthermore, the most successful approach to achieving widespread implementation of a preoperative menstrual product safety protocol involves directives from the professional perioperative practice organisations. Perioperative organisations such as the Association for Perioperative Practice (AfPP) and Association of Perioperative Registered Nurses (AORN), which have long histories of improving the standards of surgical practice, are in the ideal positions to influence practice changes. A classic example of this process was the implementation of The Universal Protocol, developed by The Joint Commission in 2004, which eliminated nearly two-thirds of wrong-site, wrong procedure and wrong-patient surgeries (Kwaan et al 2006). Emulating this model, a multidisciplinary approach should be utilised, where perioperative staff receive education and standardised protocols are developed jointly by hospital and national safety officers.
Finally, it is important to recognise that the risks associated with prolonged use of menstrual hygiene products can extend to all individuals with a uterus. Thus, the authors encourage broad consideration of menstruating individuals who do not present as female, including transgender men and non-binary individuals, when incorporating intravaginal menstrual hygiene products into preoperative checklists. The American College of Radiology’s (ACR) Safety Screening Form for Magnetic Resonance Procedures is an example of a best practice checklist asked regardless of patient gender identity or charted sex (American College of Radiology 2024). Every checklist item must be asked and completed with a ‘yes’ or ‘no’ answer – blank responses are not acceptable. The screening form includes questions related to items such as penile implants, intrauterine devices, tissue expanders (eg: breast) and diaphragms or pessaries (American College of Radiology 2024).
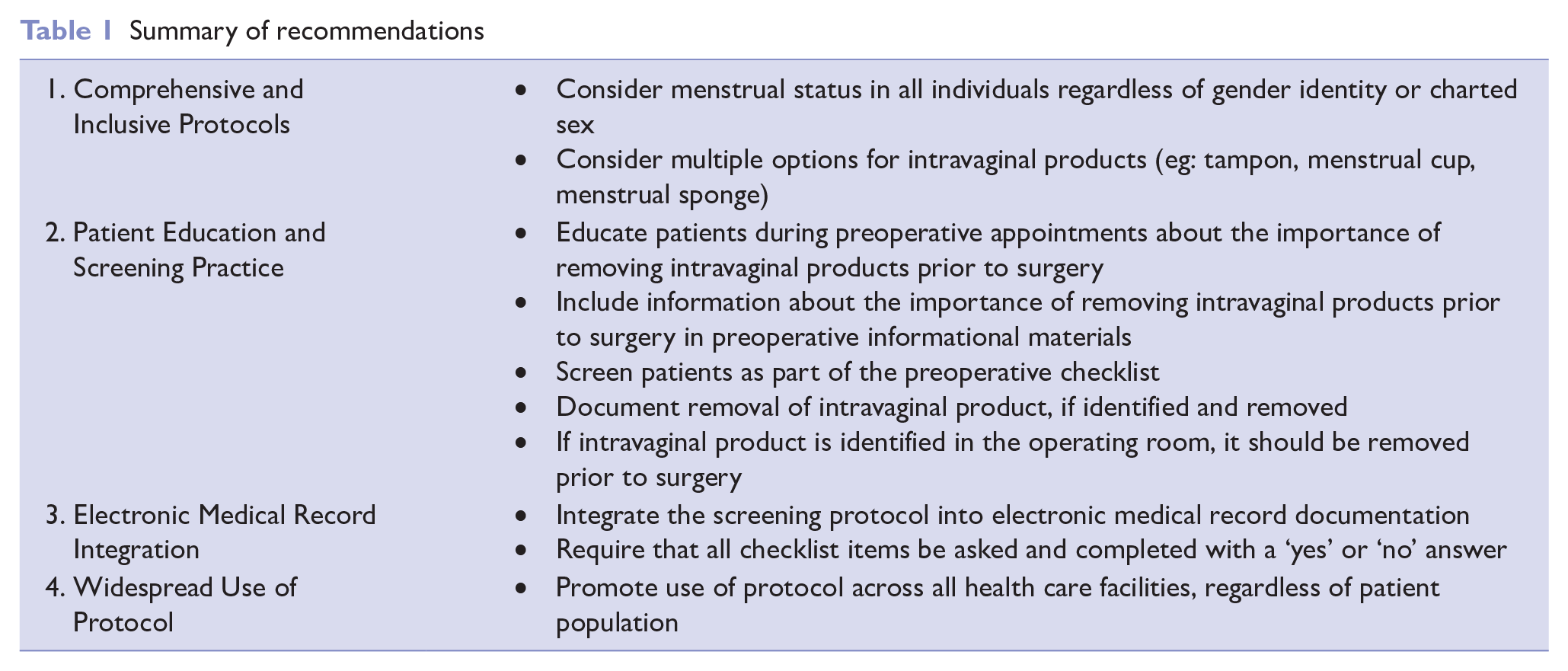
A complete summary of the aforementioned recommendations can be found in Table 1. A sample preoperative checklist incorporating these concepts is included in Figure 1. This checklist is an adapted version of The George Washington University Nursing Preoperative Checklist (The George Washington University n.d.).
Summary of recommendations
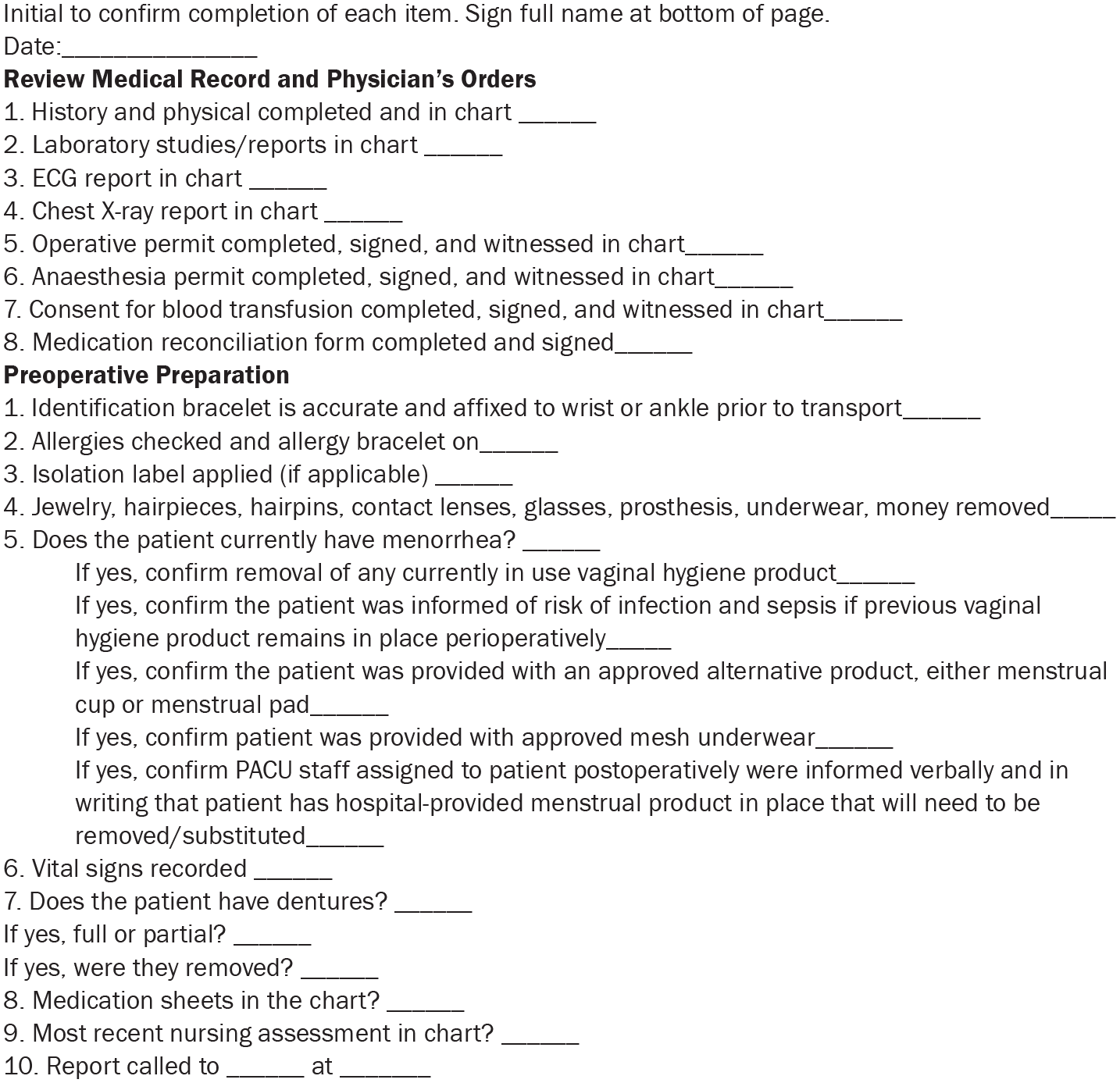
Sample preoperative checklist
Conclusion
There are clear risks of extended use of menstrual hygiene products placed in the vagina by patients during the perioperative period. Standardised documentation of product use or removal prior to surgery should be implemented to avoid these risks. Preoperative checklists should include a question to explicitly ask about the presence of these items, regardless of charted sex or gender identity.
Key points
While the assessment of perioperative risks through patient inquiry is extensive, the menstrual status of the patient is one question that is not frequently discussed.
If a patient is menstruating during their surgical procedure, unknown use of an intravaginal sanitation product, such as a tampon or menstrual cup, places the patient at risk of infection.
Patients are at risk for toxic shock syndrome and infection when intravaginal menstrual hygiene products are left for an extended period of time.
Standardisation of intravaginal menstrual hygiene product reporting has the potential to minimise perioperative risks.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.