
Abstract
Background:
Identifying early predictors of postoperative complications is paramount in frail patients. While the American Society of Anaesthesiologists classification is subjective, the 5-factor modified frailty index is simpler and associated with promising results in predicting morbidity and mortality in various surgical specialities.
Methods:
This prospective observational study assessed the comparative utility of 5-factor modified frailty index and American Society of Anaesthesiologists classification in predicting intensive care unit admission and revision surgery in 220 patients following arthroplasty with standardised anaesthesia techniques under the same group of surgeons. The 5-factor modified frailty index and American Society of Anaesthesiologists class were assessed 1 day before surgery, and postoperatively, all the patients were followed up for 30 days.
Results:
American Society of Anaesthesiologists and 5-factor modified frailty index had a significant association with postoperative intensive care unit requirements (odds ratio = 7.5, 95% confidence interval 1.3 to 42.4 and odds ratio = 8.3, 95% confidence interval 1.6 to 17.6, respectively). Only the 5-factor modified frailty index was significantly associated (odds ratio = 5.3, 95% confidence interval 1.3 to 9.7) with revision surgery. Patients with the 5-factor modified frailty index value of 3 had the best predictive odds for postoperative intensive care unit admission (odds ratio = 73.6, 95% confidence interval 7.5 to 718.8) and revision of surgery, particularly during total hip replacement (odds ratio = 54, 95% confidence interval 3.3).
Conclusion:
The 5-factor modified frailty index exhibited a more robust predictive capacity for postoperative intensive care unit requirements and the likelihood of revision surgery, particularly a 5-factor modified frailty index score of 3 in total hip replacement procedures.
Keywords
Introduction
Arthroplasty is a surgical procedure to reconstruct or replace a damaged or diseased joint with artificial components to relieve pain, restore joint function, and improve the overall mobility of patients with arthritis or joint injuries. Total hip and knee arthroplasties are cost-effective interventions for improving the quality of life in patients with end-stage degenerative joint disease (Ethgen et al 2004, Jones et al 2000). Still, complications can lead to increased morbidity, mortality, and treatment costs (Mantilla et al 2002). Frailty, characterised by reduced physiological reserve and multisystem affliction, is a reliable predictor of risk (Rockwood et al 2004). It is independent of the normal course of ageing. The ‘Canadian Study of Health and Aging’ first introduced the ‘Frailty index (FI)’, based on 70 variables. It predicted survival outcomes in the elderly population reliably (Rockwood et al 2004, Searle et al 2008). Later, the ‘American College of Surgeons National Surgical Quality Improvement’ derived 11 factors that modified the frailty index (mFI) (Shin et al 2016). The retrospective analysis of the ‘ACS-NSQIP’ database (Bellamy et al 2017) and another recent study have shown that the 11-factor mFI is superior in predicting readmission and revision surgery following arthroplasty (Runner et al 2017). This was modified to include only five variables as the 5-factor modified frailty index (5-mFI). While the mFI includes activity changes, medical history (diabetes, hypertension, chronic or acute lung disease, cardiac conditions, transient ischemic attack, stroke), cognitive impairment, and decreased peripheral pulse, the 5-mFI focuses only on the presence of five comorbid variables: diabetes mellitus, congestive heart failure, chronic obstructive pulmonary disease or current pneumonia, hypertension requiring medication, and assistance in daily activities. It has demonstrated remarkable sensitivity and specificity in predicting outcomes related to arthroplasties, such as readmission and revision surgery (Traven et al 2019).
The American Society of Anesthesiologists (ASA) classification is widely used across surgical specialities. It categorises patients based on their overall health status and organ system disease. It uses a scale from ASA I (healthy) to ASA V (a severe systemic disease that is a constant threat to life) to predict perioperative mortality better than other established cardiac risk indices (Menke et al 1993, Prause et al 1997). However, it primarily focuses on organ system disease and expected survival rather than specifically assessing frailty. However, it may not fully capture a patient’s functional status or physiological reserve, limiting its comprehensive assessment of frailty. Thus, it may not be as specific or sensitive in predicting outcomes directly related to arthroplasty procedures.
Both 5-mFI and ASA have strengths and limitations, and a comprehensive comparison of them is yet to be done. Thus, a comparative study was needed to determine which factor has a better predictive value for postoperative complications. Hence, this study aimed to compare the risk of intensive care unit admission, readmission, and revision surgery following arthroplasty associated with preoperative individual 5-mFI score and ASA classification. These scores were analysed separately to ascertain which value indicated the highest risk in a particular type of arthroplasty.
Methods
This prospective, cross-sectional, observational study was carried out after obtaining institutional ethics committee approval (IEC-326/03.05.2019 dated 07.05.2019) in 220 patients who underwent total joint arthroplasty between 2019 and 2021 by the same group of surgeons in a tertiary care hospital of northern India. All willing adult patients with written informed consent who underwent arthroplasty were included without any restriction except the patient’s refusal.
Primary objective
Comparing the predictive utility of 5-mFI and ASA classification preoperatively for Clavien-Dindo grade IV complications (any life-threatening condition involving single or multi-organ dysfunction warranting intensive care unit (ICU) management), revision surgery, and 30-day postoperative mortality.
Secondary objective
Compare the risk associated with every possible value of both 5-mFI and ASA classification among the included population to identify the maximum likelihood of ICU admission, revision of surgery, and mortality for the specific value of specific scoring systems.
Measurement
Data for the patient’s age, gender, type of surgery, preoperative 5-mFI score, and ASA class were noted during the pre-anaesthetic checkup 1 day before surgery and intraoperative blood loss from the anaesthesia chart. All patients were followed up 30 days after their index surgery for ICU admission, surgical site infection, complications related to the cardio-pulmonary, renal system, deep vein thrombosis, the incidence of readmission, revision surgery, period of hospital stay, and mortality.
The 5-MFI was calculated for all participants based on five comorbid variables: diabetes mellitus, congestive heart failure, chronic obstructive pulmonary disease or current pneumonia, hypertension requiring medication, and assistance in daily activities. In addition, participants were classified according to the ASA classification, ranging from Class I (healthy), Class II (mild systemic disease), Class III (severe systemic disease), Class IV (severe systemic illness, constant threat to life), to Class V (moribund, unlikely to survive without operation).
Anaesthesia management
All the patients received standardised regional or general anaesthesia techniques, depending upon the anaesthetist’s discretion. A lumbar epidural catheter was placed in all the patients before induction. Ringer lactate, or Plasmalyte-A or Sterofundin, were used for maintenance fluid at the discretion of the treating anaesthetist according to the Holliday Segar formula. The postoperative analgesia was achieved with epidural morphine 50 mcg/kg/12 hourly. The rescue analgesia was intravenous fentanyl boluses (0.5 mcg/kg) if the VAS > 4.
Sample size estimation
Based on a previous study (Traven et al 2019) with an expected similar incidence of 5-mFI of 3, assuming a relative risk of 2 and a power of 0.8, a total of 218 patients was required. In view of potential attrition, 250 patients were recruited.
Statistical analysis
We used the Windows programme SPSS 15.0 for the statistical analysis. Kolmogorov-Smirnov test and Shapiro-Wilk Test were used to assess the normality, and internal consistency was assessed by estimating Cronbach’s alpha (0.73). Descriptive statistics were provided in numbers and percentages for categorical variables and mean and standard deviation for the continuous variables. A comparison of two independent groups of variables was carried out using the t-test and Wilcoxon rank-sum tests accordingly. The chi-square analysis evaluated the differences between categorical variables. We also used bivariate analyses using a simple logistic regression model to determine the relationship between outcomes and 5-mFI. The statistical significance level was considered with the p-value < 0.05.
Results
Initially, 250 patients were recruited, considering potential attrition. However, due to the loss of 30 days of follow-up and patients’ refusal finally, 220 patients were analysed. Among these 220 patients, 105 (47.7%) underwent total hip replacement (THR), and 115 (52.3%) underwent total knee replacement (TKR).
The median patient age was 58 years, and 51.4% were female. Most patients were ASA class I (48.2%) or II (46.8%). The most common complications were a requirement of ICU due to any life-threatening condition involving single or multi-organ dysfunction (4.6%), and the overall period of hospital stay was 5 (5–7) days. Nine patients underwent revision surgery due to pre-existing conditions, (severe osteoporosis (n = 2), rheumatoid arthritis (n = 1)), traumatic dislocation (n = 1), periprosthetic fracture (n = 2), and infection (n = 3). There was no incidence of mortality in 30 days of follow-up (Table 1).
Demographic variables and complications
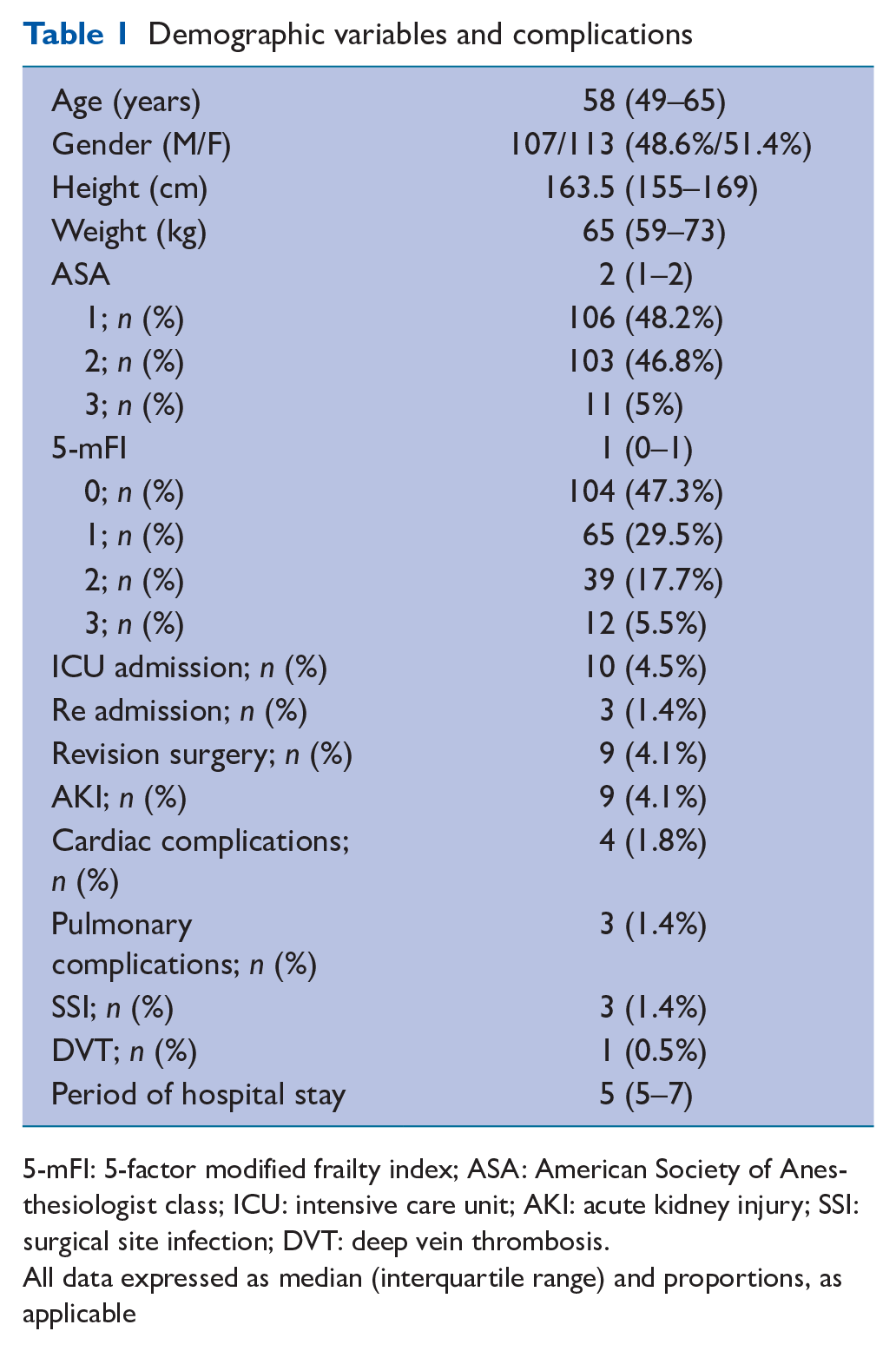
5-mFI: 5-factor modified frailty index; ASA: American Society of Anesthesiologist class; ICU: intensive care unit; AKI: acute kidney injury; SSI: surgical site infection; DVT: deep vein thrombosis.
All data expressed as median (interquartile range) and proportions, as applicable
The predictive odds of 5-mFI status for postoperative complications involving cardiac, pulmonary, and renal systems, the requirement of ICU admission, readmission, and revision of surgery were significant (Table 2).
Association of 5-mFI with different complications
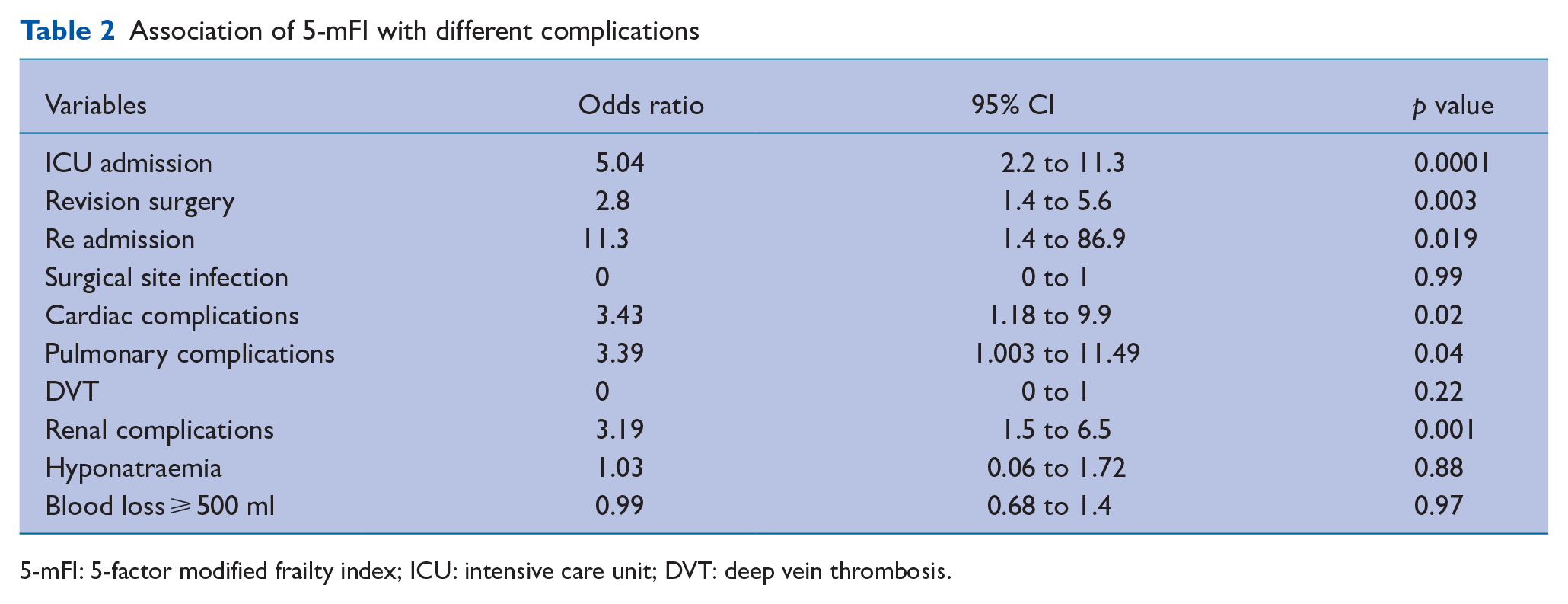
5-mFI: 5-factor modified frailty index; ICU: intensive care unit; DVT: deep vein thrombosis.
In multivariable logistic regression analysis, both ASA and 5-mFI had a significant association with postoperative ICU requirement, (odds ratio (OR) = 7.5, 95% confidence interval (CI) 1.3 to 42.4 and OR = 8.3, 95% CI 1.6 to 17.6, respectively), indicating holding other variables constant, individuals with a one-unit increase in ASA have a 7.5 times higher odds of ICU admission and one unit increase in 5-mFI have 8.3 times likelihood of ICU admission. The blood loss and age of the patient had no significant association. Similarly, a one-unit increase in 5 mFI resulted in 5.3 times higher odds of undergoing revision surgery (Tables 3 and 4).
Multi variable logistic regression analysis for ICU admission
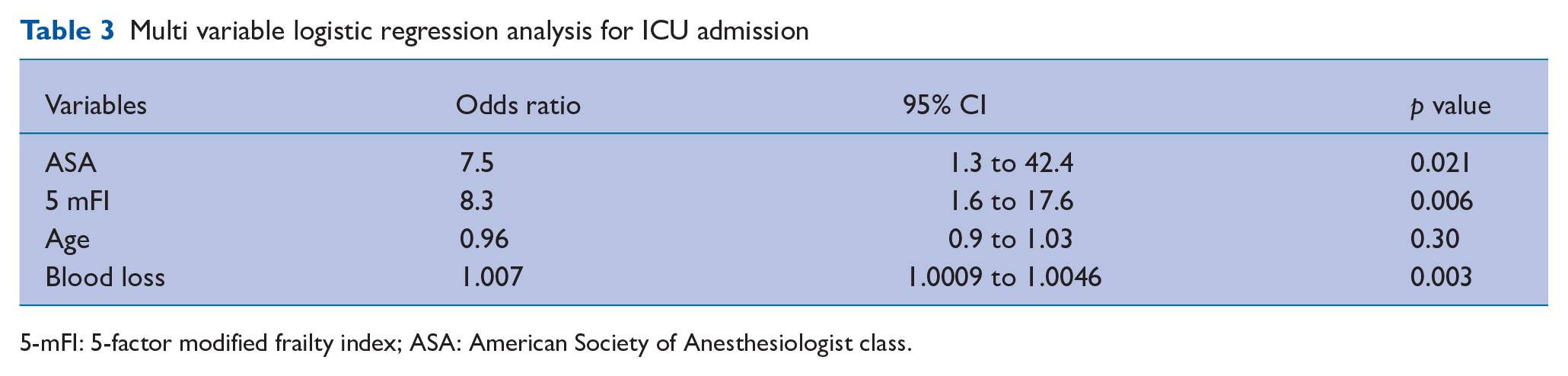
5-mFI: 5-factor modified frailty index; ASA: American Society of Anesthesiologist class.
Multi variable logistic regression analysis for revision surgery
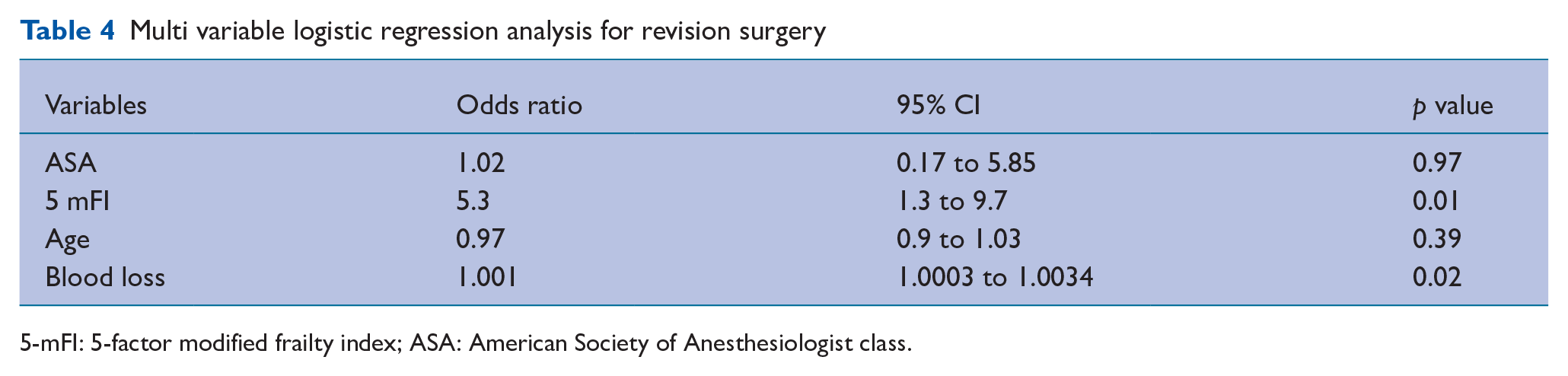
5-mFI: 5-factor modified frailty index; ASA: American Society of Anesthesiologist class.
Patients with a 5-mFI value of 3 and 2 had a significant risk of postoperative ICU admission (OR = 73.6, 95% CI 7.5 to 718.8 and OR = 8.6, 95% CI 8.8 to 85.2, respectively) compared to patients with 5-mFI value 0. The risk was also significant in ASA 3 patients (OR = 58.9, 95% CI 5.8 to 599.6).
However, the 5-mFI value 3 had a better predictive role than ASA grade 3 during THR (OR = 54, 95% CI 3.3 to 874.4 and OR = 18, 95% CI 0.9 to 363.6, respectively). However, in TKR, both had similar odds (Table 5) (Figure 1).
Comparative evaluation of 5-factor modified frailty index with ASA classification for ICU admission
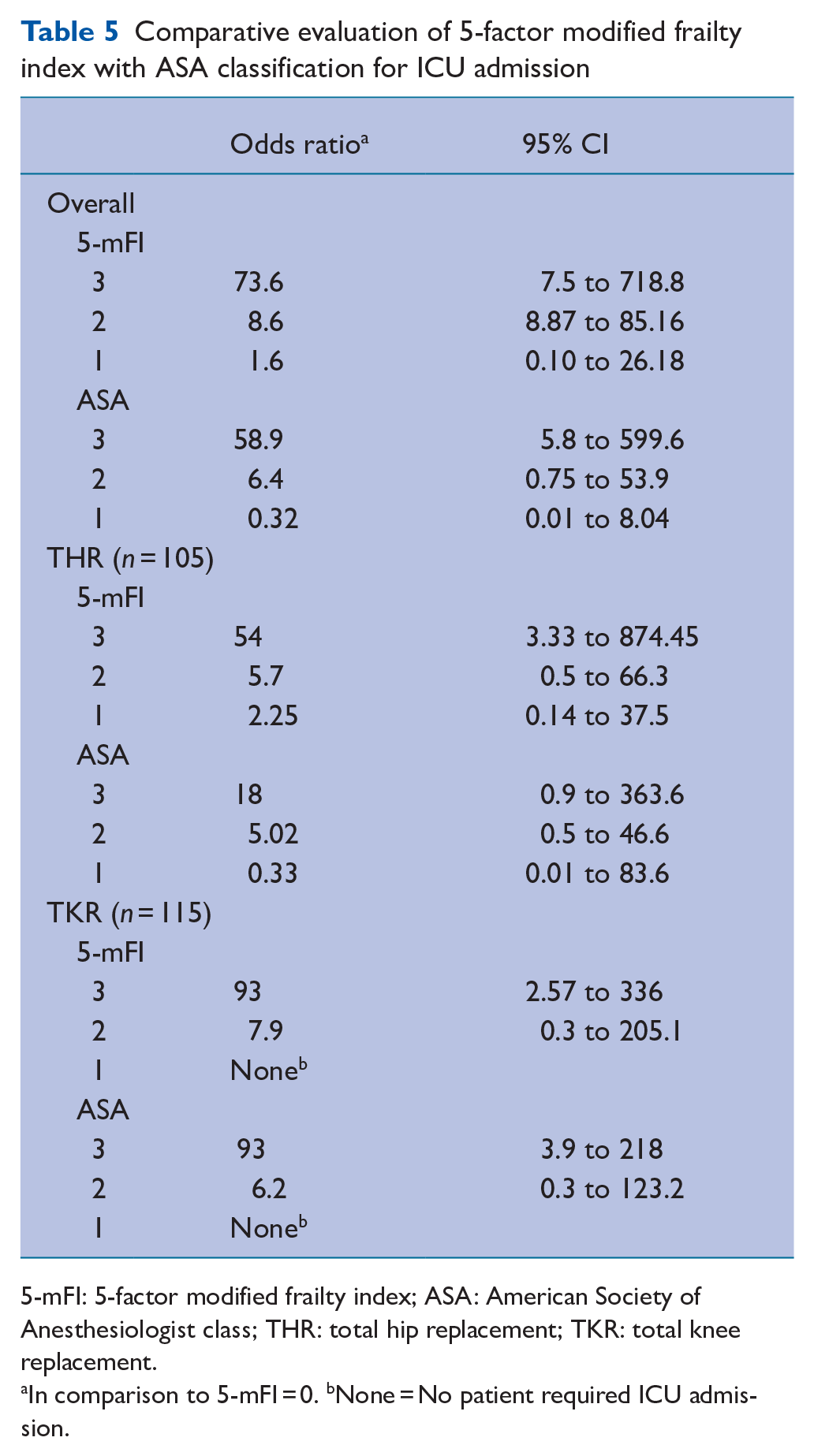
5-mFI: 5-factor modified frailty index; ASA: American Society of Anesthesiologist class; THR: total hip replacement; TKR: total knee replacement.
In comparison to 5-mFI = 0. bNone = No patient required ICU admission.
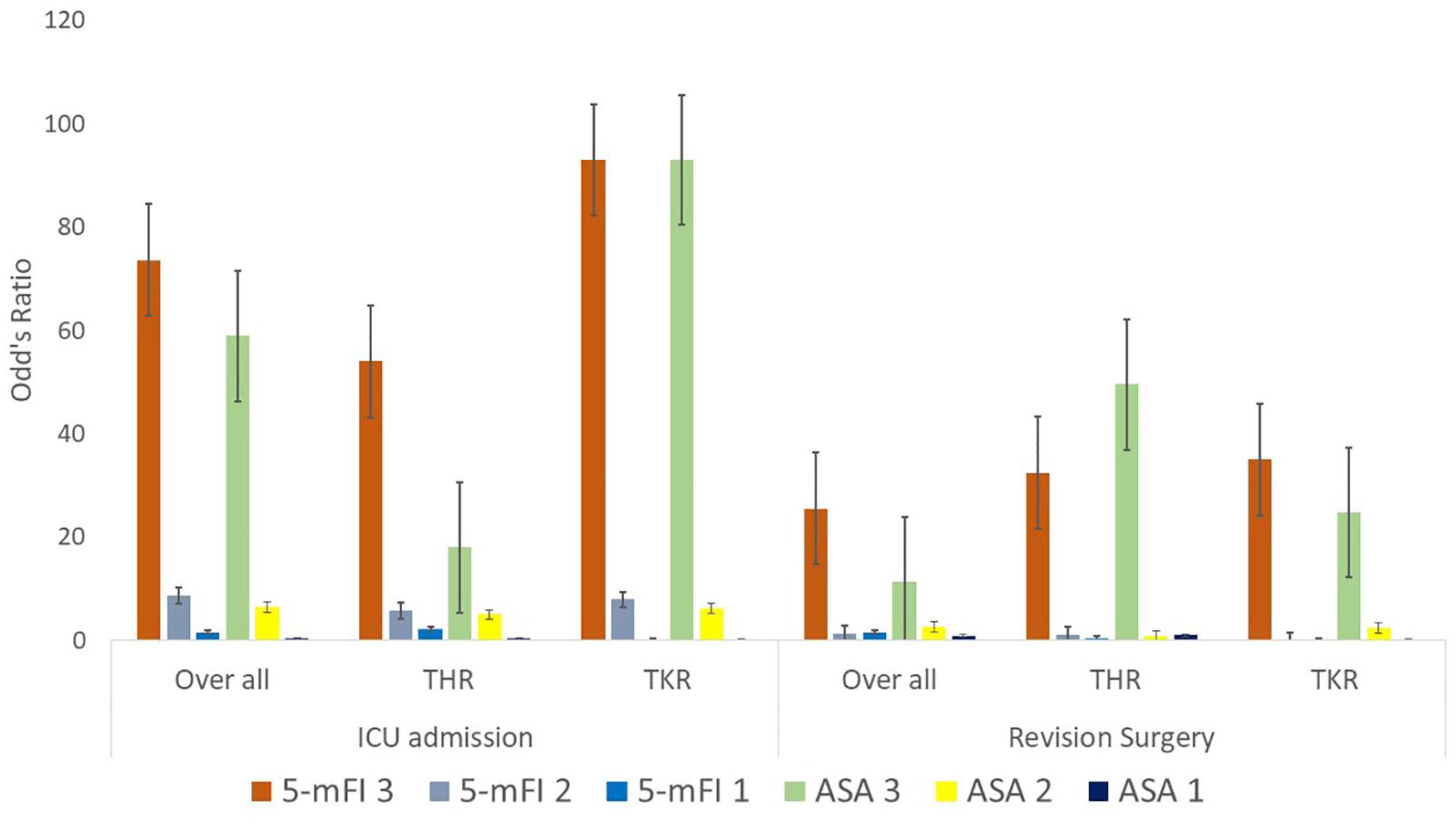
Comparative evaluation of 5-factor modified frailty index with ASA classification for ICU admission and revision surgery
The risk of revision surgery was also considerably higher in patients with a 5-mFI value of 3 (Table 6) (Figure 1).
Comparative evaluation of 5-factor modified frailty index with ASA classification for revision surgery
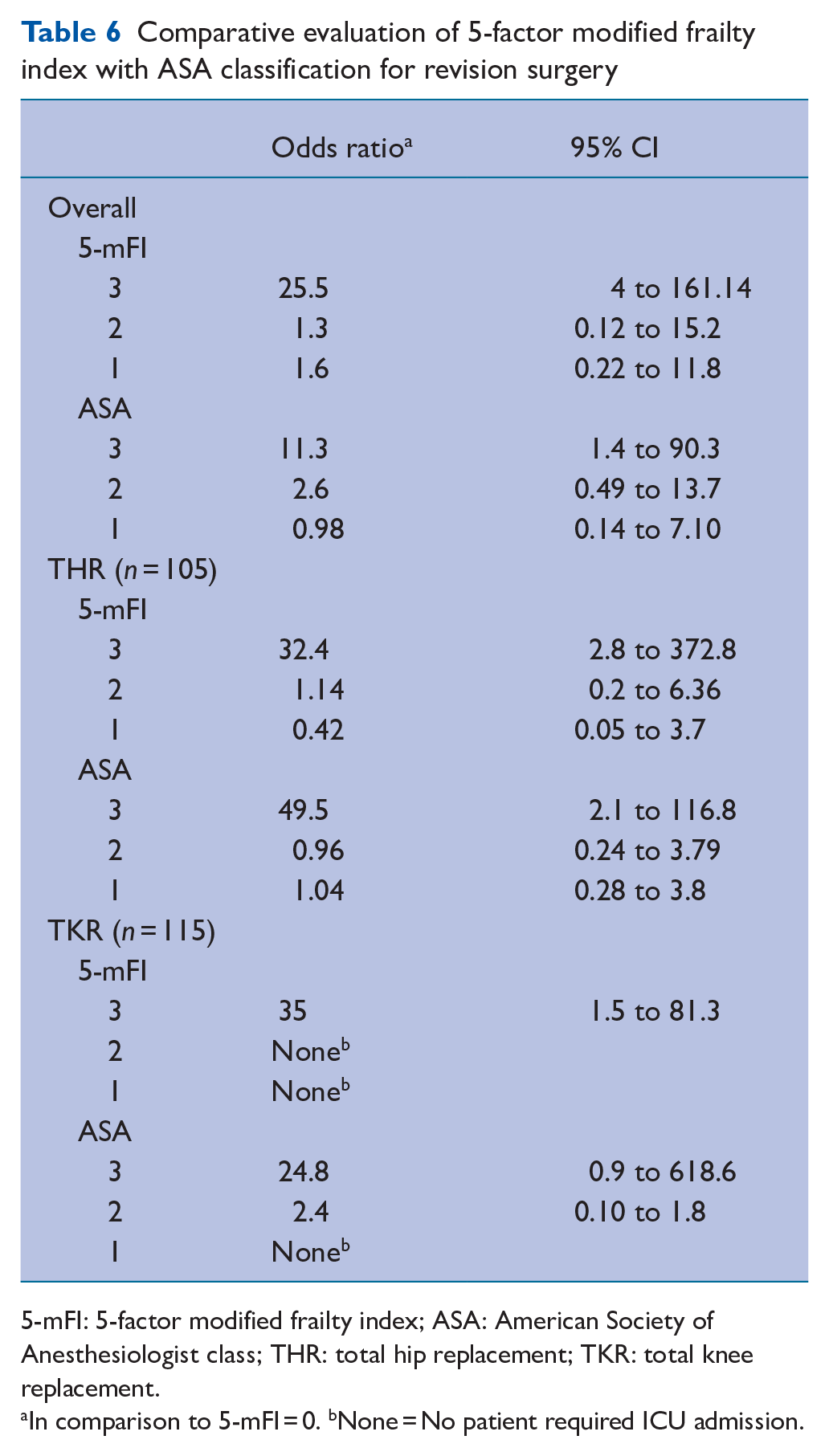
5-mFI: 5-factor modified frailty index; ASA: American Society of Anesthesiologist class; THR: total hip replacement; TKR: total knee replacement.
In comparison to 5-mFI = 0. bNone = No patient required ICU admission.
Discussion
The current prospective study found both ASA and 5-mFI had a significant association with postoperative ICU requirements following arthroplasty. However, the predictive odds of 5-mFI status for postoperative complications and revision of surgery were higher; specifically, patients with 5-mFI value 3 had the maximum risk of ICU admission explicitly following THR.
Similarly, few retrospective data also acknowledged the predictive utility of mFI-5 for postoperative complexities and incorporating the 5-mFI into the clinical decision-making process for optimisation strategies in primary hip and knee arthroplasty to improve patient outcomes (Bellamy et al 2017, Traven et al 2019). Previous studies assessing the mFI-11 also echoed similar findings (Runner et al 2017, Shin et al 2016).
However, while Shin et al (2016) reported a value of mFI ⩾ 0.45 is an independent predictor of ‘Clavien-Dindo grade IV complications’ following arthroplasty along with age > 75, body mass index ⩾ 40, ASA class ⩾ 4, Bellamy et al (2017) acknowledged mFI as a better predictor of readmission than ASA and age for readmission (‘OR 14.72, 95% CI 6.95 to 31.18, p < 0.001’), postoperative complications (‘OR 3.63, 95% CI 1.64 to 8.05, p = 0.002’), revision surgeries (‘OR 8.78, 95% CI 3.67 to 20.98, p < 0.001’), and with increasing mFI the risk of complications, readmission, revision surgeries, and mortality increased remarkably.
Our cohort had no mortality in 30 days of follow-up, and no association was found between age and blood loss. A comparatively younger population with a shorter duration of surgery by the same group of surgeons could probably be the explanation.
The definitions of postoperative frailty mortality have evolved. McIsaac et al (2016) reported 9.4% mortality in frail patients compared to 2.1% among non-frail patients a year after THR. The 30-day mortality following THR is reported to be between 0% and 0.35% (Belmont et al 2014, Doro et al 2006, Parvizi et al 2001, Shah 2004).
Frailty is often termed as ‘unsuccessful ageing’. It can be an age-related, multi-dimensional state of the receded physiologic reserve with reduced resilience and increased vulnerability to stressors. With the recent advancement in medical sciences, providing cost-effective, high-quality care without any significant complications is stressed, and any predictive model for risk stratification and optimisation is of interest. The frailty index is one such novel model, initially comprising 70 variables. While the mFI originally was a subset of 11 of these variables, since 2012, the mFI-5 has become synonymous with the frailty index with five specific conditions (Gani et al 2017). The mFI can be rapidly obtained through objective history-taking, and it has less subjective variability than the ASA classification. It can be calculated preoperatively without intraoperative variables and used to optimise frail patients’ preoperatively and perioperative plans accordingly. Apart from arthroplasty, the utility of mFI in patients undergoing colectomy (Obeid et al 2012), head and neck surgeries (Adams et al 2013), or vascular surgery (Karam et al 2013) for predicting ‘Clavien-Dindo grade IV complications’ and mortality is well documented.
Strengths and limitations
While this study is prospective, the assessment of complications was restricted to only 30 days following surgery, and each variable was given similar weightage instead of their severity. The generalisability is also limited for being a single-centre study. Also, the majority of the patients were around 65 years old; thus, further studies on specific subdivisions within the geriatric age group (young-old (65–74), Middle-old (75–84), Old-old (>85)) are required as the prevalence of chronic diseases, cognitive impairments, and functional limitations varies.
Conclusions
The ASA classification and the 5-factor modified frailty index significantly correlated with postoperative ICU requirements. However, the 5-mFI exhibited a more robust predictive capacity for both postoperative ICU requirements and the likelihood of revision surgery, particularly a 5-mFI score of 3 in total hip replacement procedures. The 5-mFI is a valuable instrument for assessing frailty and surgical risk, particularly in patients undergoing THR and integration of 5-mFI into preoperative assessments could aid clinicians in identifying high-risk patients, ultimately informing better perioperative planning and management strategies.
Footnotes
Author contributions
Dr Soumya Sarkar: data extraction, Data analysis, drafting the manuscript.
Dr Deepak Gautam: Data collection.
Dr Rahul Kumar Anand: Conceptualisation, data collection, editing.
Dr Devansh Goyal: Data collection.
Dr Sahil Batra: Data collection.
Prof. Rajesh Malhotra: Conceptualisation, data collection.
Dr Puneet Khanna: Conceptualisation, data collection, editing.
Dr Dalim Kumar Baidya: Data collection.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical clearance
IEC-326/03.05.2019, AIIMS New Delhi, dated 07.05.2019
Prior presentations
Not applicable.