
Abstract
Background:
Under general anaesthesia, the impact of body positioning on different organs is mostly determined by the subsequent changes in the cardiovascular system, which are monitored with standard monitors. However, there is no objective method of neuromonitoring, therefore impacts on brain homeostasis are mainly conjectural. Near-infrared spectroscopy is a non-invasive method for monitoring tissue cerebral oxygenation. In this study, we aimed to observe the effects of the prone position on cerebral oxygenation in patients under general anaesthesia.
Methods:
The study involved 44 patients undergoing spine surgeries in a prone position under general anaesthesia. Regional oxygen saturation readings were initially taken in the supine position and monitored continuously after transitioning to the prone position. A decrease in regional oxygen saturation of more than 20% was considered clinically significant.
Results:
A significant drop in blood pressure (p = 0.02) and heart rate (p = 0.04) was observed after positioning patients prone under general anaesthesia. In addition, end-tidal carbon dioxide levels rose notably after 30 min in the prone position (p = 0.017). Importantly, while no significant differences were found in cerebral oxygenation between the supine and prone positions, one patient did experience right-sided vision loss postoperatively.
Conclusion:
Using near-infrared spectroscopy monitors is recommended for patients with comorbidities and those undergoing surgeries with extended durations in the prone position.
Keywords
Introduction
The primary goal of safe anaesthesia is to ensure adequate oxygen delivery according to metabolic needs, thereby achieving supply-demand matching. Studies have established a connection between episodes of cerebral oxygen desaturation during surgery and neurocognitive dysfunction, prolonged hospital stays, morbidity, and mortality in patients (Deschamps et al 2016, Kong et al 2022, Tian et al 2022, Wang et al 2019). Although cerebral desaturation can adversely affect patient outcomes, the brain often receives the least attention during surgery, as no standard monitor is typically used for assessing cerebral blood flow. While cerebral homeostasis, particularly oxygenation status, can be monitored using devices like jugular bulb oximetry or cerebral microdialysis catheters, their routine use is discouraged due to their invasive nature. Near-infrared spectroscopy (NIRS) oximetry devices have been utilised in clinical practice for cardiac and vascular surgery since the 1980s. Recently, the application of cerebral oximetry using NIRS has expanded to include perioperative brain oxygenation monitoring in vulnerable populations under general anaesthesia (GA) (Yu et al 2018).
The prone position is commonly used in various neurosurgical procedures. However, this non-physiological position significantly affects cardiopulmonary mechanics and cerebral haemodynamic. Intra-abdominal pressure compresses the inferior vena cava, while intrathoracic pressure reduces left ventricular compliance and filling. As a result, ventricular capacity decreases, leading to reduced stroke volume and hypotension. Several studies have associated the prone position with increased intracranial pressure (ICP), elevated intraocular pressure, changes in cerebral blood flow, and decreased cerebral oxygen supply (Roth et al 2014, Van Wicklin 2020). Considering that the cumulative effects of prone positioning may alter cerebral haemodynamic, we planned to conduct an observational study to evaluate the impact of the prone position on cerebral oxygenation in anaesthetised patients.
Material and method
After providing informed consent, 44 patients from an Indian tertiary hospital participated in the current study. The institutional ethical committee granted the required consent. The study is not registered in Clinical Trials Registry- India (CTRI) and the duration of the study was 12 months. The data recorded in the study were collected during the years 2021–2022. Consent was obtained from the patients during their preoperative checkup, with the option to withdraw at any time before the surgery. This observational study included all adult patients (aged 15 to 85), characterised as I or II ASA (American Society of Anaesthesiologists) grade, who underwent spine procedures lasting more than 60 min, under GA and in the prone position. The study excluded patients with anaemia, hemoglobinopathy, any intraoperative intravenous dye use, carotid artery disease (stenosis/malformation), preexisting structural cerebral disease, and the likelihood of intraoperative blood transfusion (if expected blood loss > 20% of total blood volume). The patients with anaemia, hemoglobinopathy, dye use, and massive blood loss were excluded as these things will affect the cerebral oximetry reading and thus act as confounders.
When the patient arrived in the operating room, they were positioned in the supine position – lying on their back with their face and torso facing upwards. All standard ASA monitors were attached, and intravenous access was secured. After the forehead was cleaned with an alcohol swab, NIRS electrodes were placed on each side of the forehead, 3–5 cm above the brow line, and linked to the INVOS 5100 NIRS monitor (Covidien 11c-15; Hampshire Street Mansfield, MA 02048, USA). Baseline readings of regional oxygen saturation (rSO2) were recorded at baseline – first reading as the patient laid on the table (S0), 5 min before induction in the supine position for 5 min (S1), and 5 min after intubation (S2). After that, the recordings were taken 5 min after (P1) prone position and then at intervals of 15 to 60 min (P2, P3, P4, and P5) of the surgery. GA was induced using Fentanyl 2 µg/kg as pre-induction and propofol 1.5 mg/kg for induction and maintenance with oxygen/N2O with desflurane. Vecuronium 0.1 mg/kg was used as a muscle relaxant throughout surgery. The patient was kept on volume control mode with tidal volume maintained at 6–8 mL/kg, end-tidal carbon dioxide (EtCO2) in the range of 35–40 mm of Hg, respiratory rate (RR) between 12 and 15 breaths per minute, inspiratory to the expiratory ratio (I:E) of 1:2, fraction of oxygen (FiO2) of 0.4, and positive end-expiratory pressure (PEEP) of 6 cm of H2O. Any adverse event in the intraoperative period like significant blood loss, desaturation (defined as pulse oximetry (SpO2) < 90% for more than 30 s), bronchospasm, hypotension (defined as mean arterial pressure) < 60 mm of Hg for more than 1 min), and hypothermia (temperature <35 °C) were noted.
After positioning the patient in the prone position – lying face down on their stomach with their back facing upwards – the head was maintained in a neutral position using a headrest. The target mean arterial pressure was maintained within 20% of the patient’s baseline. Once the surgery concluded the patient was turned back to a supine position and was reversed with glycopyrrolate and neostigmine and extubated on the table. The readings for rSO2 were recorded for 1 h because most of the surgeries conducted were Laminectomies and were finished within 90 min of proning. Second, there are certain studies conducted in the past that after 60 min the rSO2 values were back to the supine levels and were unchanged afterward.
In case of cerebral desaturation, steps are to be taken check the position of the head and neck to ensure that there is no mechanical obstruction to the cerebral blood flow, maintain the mean arterial pressure to avoid any fall in cerebral perfusion pressure, maintain normal SaO2, keep the PaCO2 within the range of 35 mm of Hg to 45 mm of Hg, optimise the Hb and keep the value above 8 g/dL, and, finally consider any further condition which may increase cerebral oxygen consumption (such as convulsions or hyperthermia).
Data were coded and recorded in MS Excel spreadsheet programme. SPSS version 23. (IBM Corp) was used for data analysis. Descriptive statistics was elaborated in the form of means/standard deviation and medians/standard deviations and medians/interquartile range (IQR) for continuous variables and frequencies and percentages for categorical variables. Data was presented graphically wherever appropriate for data visualisation using histograms/box-and-whisker plots/column charts for continuous data and bar charts/pie charts for categorical data.
Group comparisons for continuously distributed data were made using the independent sample ‘t’ test when comparing two groups. For the power of 80% and an alpha error of 0.05, the minimum sample size required is 44. To compensate for attrition bias, 50 consecutive eligible patients were enrolled in the study (Murniece et al 2020).
Results
The STROBE guidelines were followed in the conduct of this observational study. Six participants out of 50 consecutive patients evaluated for the study were excluded from the trial for various reasons (Figure 1).
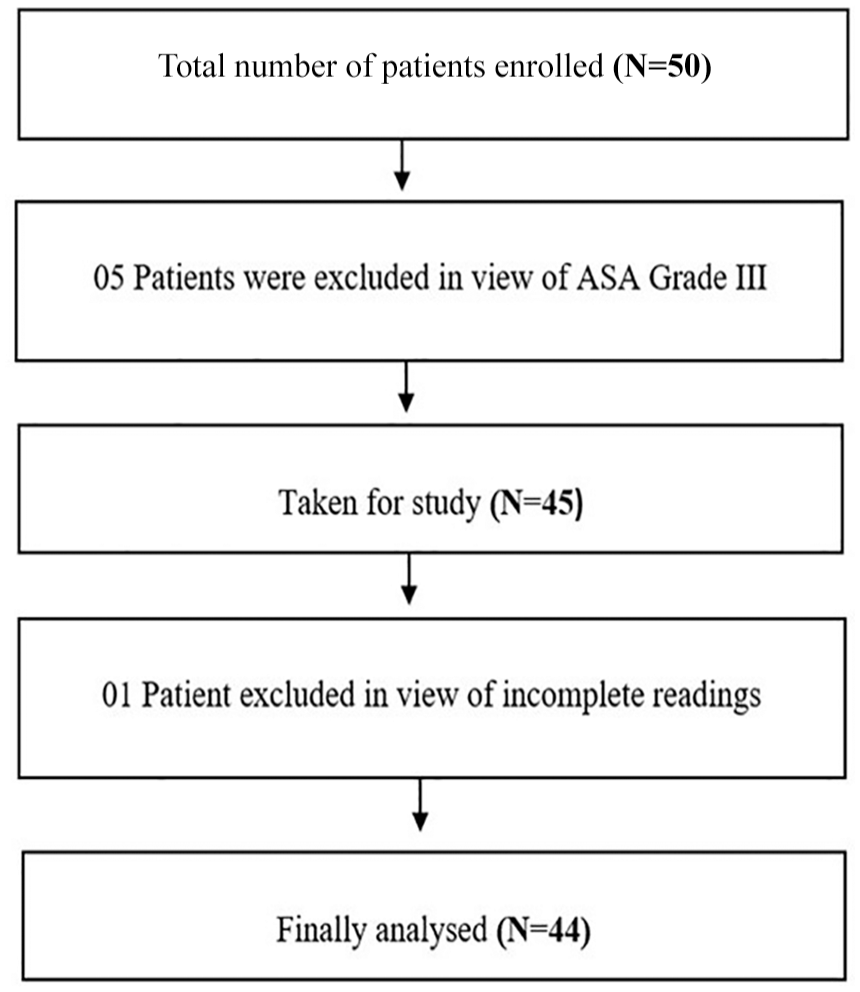
Flow chart showing enrolment and analysis.
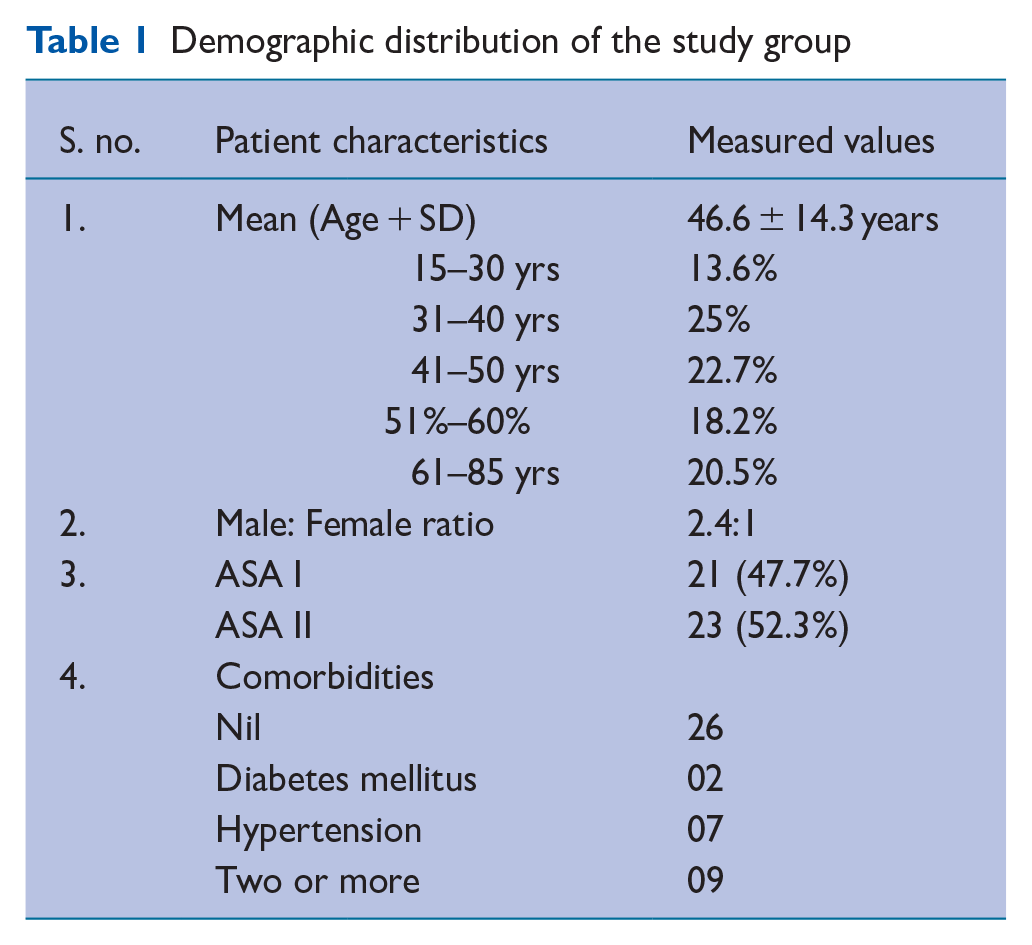
Similar distribution across age groups was seen, with 25% of participants between the ages of 31 and 40 (Table 1). The mean ± SD of age in the study group was 46.6 ± 14.3 years, and the minimum–maximum age range was 15–85 years. The study group was predominantly male, ASA I/II, and had no comorbidities (Table 1).
Demographic distribution of the study group
Mean arterial pressure and RR dropped significantly after proning most patients (p = 0.02, 0.004). Heart rate (HR) decreased significantly after 15 min of prone position (p = 0.044) (Tables 2 and 3). Mean arterial pressure, SpO2, and temperature found no changes in the first 60 min of the prone position (Table 3). However, HR, mean arterial pressure, and RR distributions after induction (supine position) are significantly higher than HR distributions after 15 min of prone position (p = 0.044, 0.275, 0.072, respectively) (Table 3). The distribution of rSO2 on both sides after induction (supine position) did not differ significantly from rSO2 immediately after prone, 15, 30, 45, and 60 min of prone positions (Table 2). There was no significant difference between the rSO2 values recorded at the P1 interval and the rest of the values recorded in the prone position. There was no effect on the duration of the surgery on rSO2 values.
Distribution of the mean values with SD values in respect of the measured variable
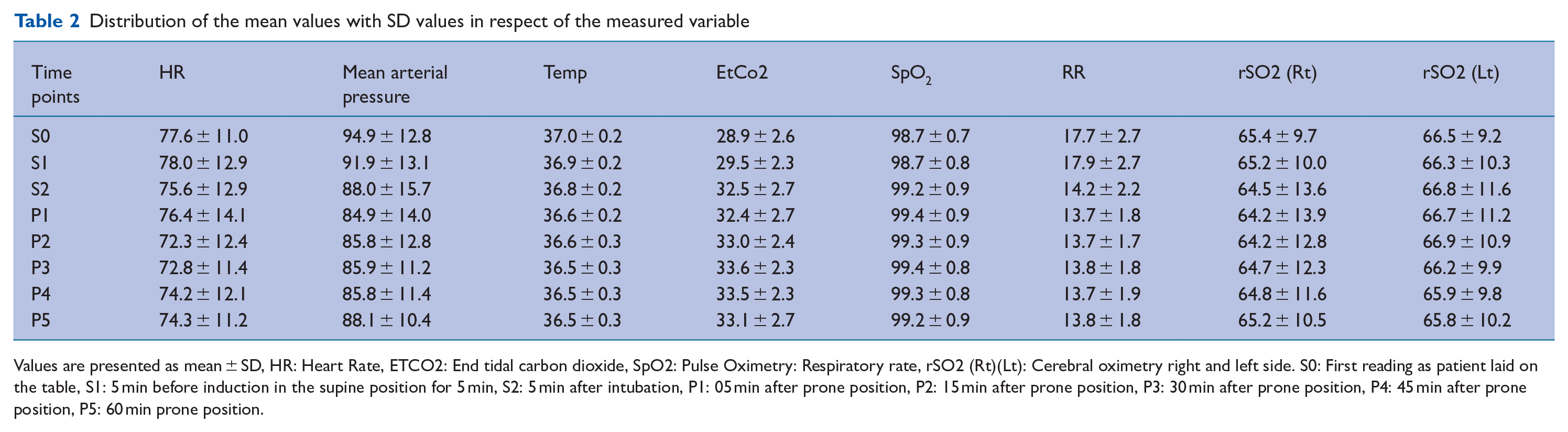
Values are presented as mean ± SD, HR: Heart Rate, ETCO2: End tidal carbon dioxide, SpO2: Pulse Oximetry: Respiratory rate, rSO2 (Rt)(Lt): Cerebral oximetry right and left side. S0: First reading as patient laid on the table, S1: 5 min before induction in the supine position for 5 min, S2: 5 min after intubation, P1: 05 min after prone position, P2: 15 min after prone position, P3: 30 min after prone position, P4: 45 min after prone position, P5: 60 min prone position.
Paired comparison of the mean values
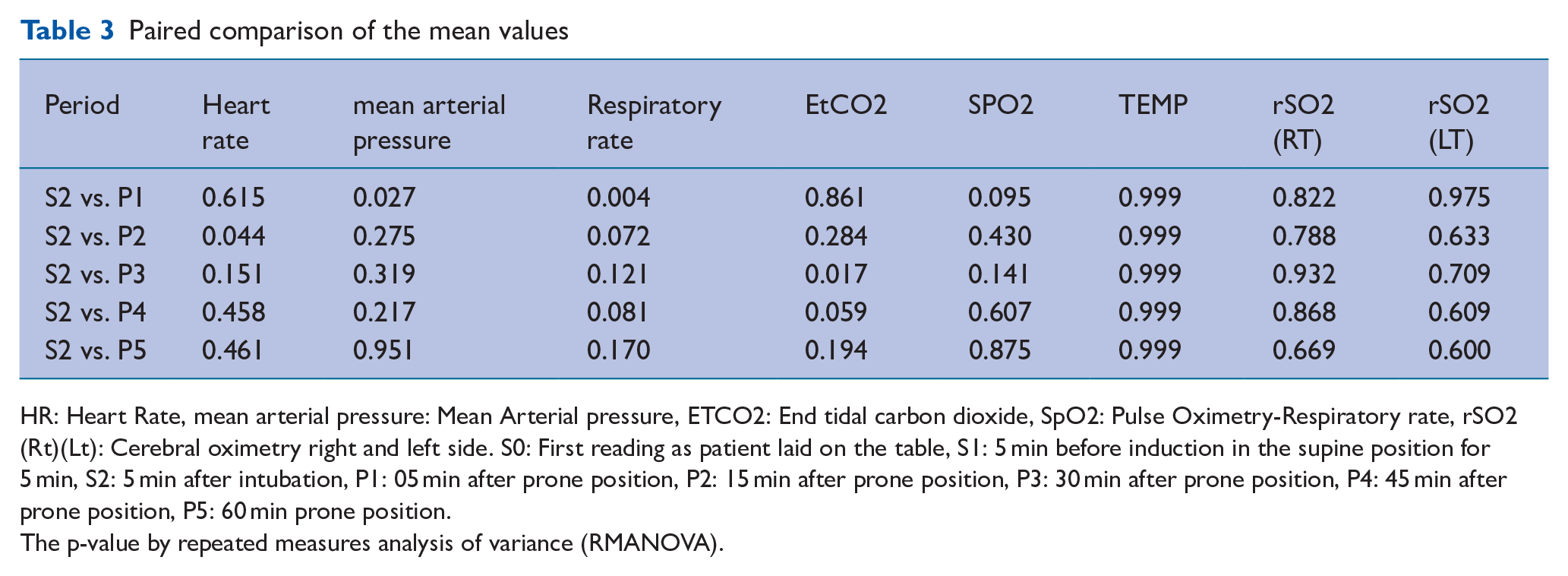
HR: Heart Rate, mean arterial pressure: Mean Arterial pressure, ETCO2: End tidal carbon dioxide, SpO2: Pulse Oximetry-Respiratory rate, rSO2 (Rt)(Lt): Cerebral oximetry right and left side. S0: First reading as patient laid on the table, S1: 5 min before induction in the supine position for 5 min, S2: 5 min after intubation, P1: 05 min after prone position, P2: 15 min after prone position, P3: 30 min after prone position, P4: 45 min after prone position, P5: 60 min prone position.
The p-value by repeated measures analysis of variance (RMANOVA).
In our study, there were three patients in which transient hypotension was noted after proning. However, it was transient and could be easily managed with intravenous fluid and Vasopressors. Notably, despite these haemodynamic alterations, the cerebral tissue oxygenation was maintained, and no significant fall in rSO2 was noticed. In our study, we noted two cases with a fall in rSO2. The first patient’s lower regional rSO2 was attributed to an abnormal head position. This diagnosis was confirmed because once the patient’s head position was corrected, the rSO2 values returned to the normal range and were displayed continuously on the monitor without interruption. In the second patient, sudden hypotension resulted in a dip in right-sided rSO2 after proning, and despite all corrective measures, the rSO2 values on the right side remained below 50. The surgery lasted 6 h with the patient in the prone position, and the rSO2 of the right side was always significantly lower than the baseline values. The patient was haemodynamically stable throughout the surgery with minimal blood loss. Postoperatively, the patient complained of right-sided vision loss, which on fundoscopy was suggestive of central retinal artery occlusion. None of the patients required a blood transfusion, and none experienced blood loss exceeding 20% of their total blood volume.
Discussion
Anaesthesia for lumbar spine surgery requires patients to be turned from a supine to a prone position under GA. Prone positioning can elicit significant haemodynamic changes resulting in a fall in arterial pressure and tissue perfusion and respiratory changes causing increased intrathoracic and intra-abdominal pressure, resulting in reduced venous return, preload, and possibly raised ICP (Dharmavaram et al 2006).
In this study, we noted the mean HR and mean arterial pressure to be significantly higher after induction (supine) than the haemodynamics after 15 min of prone positioning. These haemodynamic changes may have been the result of intubation stress, although neuromonitoring was not utilised during the study to confirm this. Furthermore, our study’s noted fall in mean arterial pressure immediately after proning is well documented. Backofen (1985) suggested that the prone position is associated with a fall in stroke volume and has no effect on HR, further decreasing cardiac output. Yokoyama et al (1991) described that the heart’s position at a hydrostatic level above the head and limb may cause a decrease in venous return to the heart and consequently decrease the cardiac output. Our institution uses the Wilson frame commonly for spine surgery, making the head position slightly lower than the heart. Sudheer et al (2006) described the increased intra-thoracic pressure leading to a decrease in left ventricular compliance, thus causing a fall in cardiac output. In our study, we found that there was a fall in mean arterial pressure immediately after proning, but the mean arterial pressure was always maintained above 65 mm of Hg.
Although the prone position has been proven beneficial regarding respiratory mechanics and ventilation. It is regularly employed in patients with acute respiratory distress syndrome and, recently, in COVID-19 pneumonia (Flynn Makic et al 2020). Studies describe the changes in prone ventilation, like an increase in functional residual capacity due to a reduction in cephalad pressure on the diaphragm, thus causing the atelectatic segments to open up and improve ventilation (Edgcombe et al 2008, Flynn Makic et al 2020).
Despite the transient haemodynamic alterations following proning, there was no significant variation in the regional cerebral oximetry readings. We likely had a healthier population (almost 60% of patients had no comorbidities), but the lag in the monitoring window during proning and the monitoring epoch of the NIRS monitor may be possible confounders. However, the subsequent readings were well within the normal limits, and it may be speculated that changes in cerebral oxygenation during and immediately following proning were unlikely to be clinically relevant. A similar study was conducted by Murniece et al (2020), which monitored the regional cerebral oxygen saturation during spinal surgery under GA. In their study, they monitored only the values at four intervals. Like our study, the authors noted no significant difference in rSO2 in the prone position compared to the supine position.
In our study, there were three patients in which transient hypotension was noted after proning. However, it was transient and could be easily managed with intravenous fluid and vasopressors. Notably, despite these haemodynamic alterations, the cerebral tissue oxygenation was maintained, and no significant fall in rSO2 was noticed. This finding agrees with the study by Tran et al (2020) who demonstrated the association between rSO2 and mean arterial pressure by cerebral oximetry index and postulated that there is no correlation between rSO2 and mean arterial pressure if the mean arterial pressure is within the auto-regulatory limits.
In our study, we noted two cases with transient fall in rSO2 – the first case probably due to head position not in neutral. Andersen et al (2014) have strongly recommended a neutral position for proper rSO2. The second patient, a known hypertensive, had sudden hypotension after induction, although the blood pressure (BP) normalised with vasopressors intraoperatively.
Limitation
The most significant limitation of the study was the frequency of the probe detachments after pronation of the patient, generating erroneous readings. The cases included in the study, nevertheless, had uninterrupted readings of rSO2. Cerebral oxygenation is affected by several factors like HR, BP, temperature, and oxygen saturation; thus, all these factors are also studied to reduce the confounders, but several cerebral physiological factors can affect cerebral oxygenation and are not studied in the study, like ICP and metabolic contents. For future research, it is recommended that NIRS is more commonly used in routine surgeries, and for understanding the changes in cerebral oxygenation, more confounders like ICP are also studied.
Conclusion
Under anaesthesia, we are still far from attaining a non-invasive universal ideal neuromonitoring device. Nevertheless, NIRS may be a close correlate of brain health. No significant changes were noted during prone positioning in our study, but it may be relevant in patients with comorbidities and impaired cerebrovascular reserve. It is advisable to use NIRS in patients with comorbidities and surgeries requiring longer prone position duration.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
IRB number
IEC/Oct/2019 dt 18 Oct 2019, Armed Forces Medical College, Pune, India