
Abstract
Introduction:
The choice of analgesic technique for total knee arthroplasty affects its rehabilitation and surgical outcomes. This study evaluates this choice on short-term postoperative quality of life.
Methods:
In this prospective observational study, patients were categorised into two groups: epidural analgesia or peripheral nerve blocks. The medical and intraoperative data of 36 adult patients undergoing scheduled total knee arthroplasty was collected. The researchers applied the Knee Injury and Osteoarthritis Outcome Score (KOOS), EuroQoL 5 Dimension Score (EQ-5D) and Clinical Frailty Scale questionnaires, preoperatively and at 48 hours postoperatively.
Results:
Both groups showed postoperative improvement in pain, mobility and perceived health status. However, no significant differences were observed between the groups across any of the outcome measures, suggesting comparable postoperative results.
Discussion:
Although epidural analgesia has traditionally been favoured, no clear advantage was identified. These results support the consideration of both techniques in clinical practice and highlight the need for further research on long-term, patient-centred recovery indicators.
Keywords
Introduction
Osteoarthritis is one of the most prevalent diseases in developed countries, affecting approximately 7% of the global population (Diseases & Injuries 2020, Hunter et al 2020). The most typical manifestation is pain and stiffness in the weight-bearing joints (Long et al 2022). The knee osteoarthritis’ treatment aims to reduce the patient’s pain and to improve their function, mobility and quality of life (QoL). Total knee arthroplasty (TKA) is recommended if symptoms significantly decrease the QoL, despite optimal nonsurgical treatment (Carr et al 2012). The burden of this disease is expected to escalate as life expectancy increases, with the corresponding increase in health care expenditure related to TKA. This high health-related cost demonstrates that this is a priority area for health care policy development (Singh et al 2019).
The traditional metrics (number of surgeries performed, procedure costs) are still used to assess the performance of health services, but they offer limited insight into the actual impact on patients. The assessment of the QoL is one of the key dimensions of patient-centred health systems and has proved to provide relevant information to assess the impact and benefit of surgical interventions (Edgman-Levitan & Schoenbaum 2021, Urbach 2005).
Despite the benefits of TKA, it is a surgery associated with high levels of postoperative pain (Chan et al 2013). Its recovery is influenced by multiple factors, including postoperative pain control and rehabilitation progress (Doo et al 2020, Lee et al 2015). The choice of the analgesic technique has a high influence in short-term recovery outcomes. Effective pain management improves early mobility, rehabilitation adherence and reduces opioid consumption with its potential complications and side effects (Gaffney et al 2017).
The epidural catheter analgesia is a technique that allows continuous and effective pain control, potentially reducing the need for systemic analgesia and opioid consumption (Kianian et al 2024, Memtsoudis et al 2019). However, epidural analgesia is associated with several side effects that can impact QoL, such as higher incidence of urinary retention, pruritus and hypotension (Rodriguez-Patarroyo et al 2021). Peripheral nerve blocks (PNB) are an alternative to postoperative pain control. PNB provides prolonged analgesia, less risks than neuraxial approach, lower incidence of adverse effects and a potentially optimised functional recovery and may require less frequent nursing interventions, further streamlining postoperative care (Ilfeld 2017). However, few studies have directly compared the impact of these two techniques on early postoperative QoL and functional outcomes in TKA patients.
The main objective of this study is to evaluate the impact of the chosen analgesia technique on the patient-reported outcomes in the immediate postoperative period of TKA. As a secondary aim, we studied the impact of Clinical Frailty Scale, age, gender, education level and length of hospital stay on immediate patient-reported outcomes.
Methods
This prospective observational study was approved by the research ethics committee of our institution (reference 445/2024). Informed consent was obtained from all the patients.
This study included all adult patients admitted at a university hospital for a scheduled unilateral TKA with the diagnosis of primary osteoarthritis during 6 weeks. A total of 40 patients were enrolled, but only 36 patients completed the evaluation. The four remaining patients did not consent to complete the questionnaire after the first interview. Patients under 18 years of age, undergoing urgent/emergent procedures or surgical revision procedures, unable to provide informed consent or to complete the questionnaires due to illiteracy or language barrier were excluded.
The data collection occurred preoperatively, until 24 hours before surgery and in the postoperative period, 48–72 hours after surgery. In the preoperative period, researchers applied the CFS (Canadian Study of Health and Aging Clinical Frailty Scale) (Rockwood & Theou 2020). The KOOS (Knee Injury and Osteoarthritis Outcome Score) and EQ-5D (EuroQoL 5 Dimension Score) (both the five domains descriptive system and the overall health assessment by the Visual Analogue Scale) were applied in the preoperative and postoperative periods (Collins et al 2016, Ferreira et al 2013, Goncalves et al 2009, Janssen et al 2019). All three questionnaires are validated to the Portuguese population.
From the patients’ clinical records, the following data was collected: age, sex, weight, height, level of education and previous medical history. Data regarding the anaesthetic technique, duration of anaesthesia and surgery, length of hospital stay, postoperative analgesia prescribed and any intraoperative or postoperative complications were also collected.
This being a prospective observational study, patients were allocated into two groups based on the analgesic technique chosen by the anaesthetist, not by any form of random assignment: (1) Epidural Analgesia Group (EAG) – patients in whom postoperative pain control was delivered via an epidural catheter; (2) Peripheral Nerve Block Analgesia Group (PNBAG) – patients in whom a PNB was performed as a pain-management technique. The analgesia regimen to the EAG consisted in a continuous epidural infusion with ropivacaine and sufentanil in the first 48 hours, associated with intravenous (IV) analgesia with paracetamol, cetorolac and tramadol during hospital stay. Whereas in the PNBAG, the PNBs were performed using ropivacaine, the analgesia regimen with IV paracetamol and cetorolac and a continuous IV infusion of tramadol during the hospital stay. We access the two groups in the 48–72 hours postoperatively, after the effect of single-shot technique in the PNBAG wear off, to realise if a continuous infusion was truly necessary.
KOOS is a questionnaire designed to assess short- and long-term patient-relevant outcomes following knee injury. It is composed of 42 items, distributed into five domains evaluating knee-related symptoms, function and QoL in individuals with knee injuries or osteoarthritis: Pain – assessment of the intensity and frequency of pain in different situations; symptoms – includes aspects such as joint stiffness and the presence of oedema; activities of daily living (ADL) – impact of symptoms on the performance of daily tasks; sport and recreation function – limitations in more physically demanding activities; and knee-related QoL – patient perception of their condition and its impact on wellbeing. It is scored separately for each domain, ranging from 0 to 100, where 0 represents greater impairment and 100 indicates absence of symptoms (Collins et al 2016, Goncalves et al 2009).
The EQ-5D score evaluates health states in five dimensions: Mobility, Self-Care, Usual Activities, Pain/Discomfort and Anxiety/Depression. Each dimension has three response categories: no problems (score of 1), some problems (score of 2) and extreme problems (score of 3). The EQ-5D Visual Analogue Scale was also assessed, evaluating the patients’ overall health, where 0 is the worst value, that is, the worst imaginable health state, and 100 is the best, representing the best imaginable health state (Ferreira et al 2013, Janssen et al 2019).
The CFS is a tool used to assess the general level of fitness or frailty in older adults. The scale classifies individuals in a range from 1 (very fit) to 9 (terminally ill), considering factors such as comorbidities, function and cognition (Rockwood & Theou 2020).
Statistical analysis
The dataset was analysed using descriptive and inferential statistical methods. Continuous variables were assessed by Mann–Whitney U Test. Categorical variables were analysed using the chi-square test or Fisher’s exact test. To assess the difference between the preoperative and postoperative periods, every preoperative score of each domain of the KOOS and the EQ-5D score was subtracted to the corresponding postoperative KOOS or EQ-5D score. A significance level of p < 0.05 was used for all statistical tests to determine significant differences between the two groups.
Variables with a p-value < 0.20 were included in a multivariate logistic regression model to identify potential independent predictors of postoperative outcomes. The logistic regression results were reported as odds ratios (OR) with 95% confidence intervals (CI), adjusting for relevant confounders. In this model, EAG was coded as 0, and PNBAG was coded as 1.
To identify the eventual variables, other than the chosen analgesia, which could interfere with the KOOS score, the Mauchly sphericity test was applied, and accordingly, the Greenhouse-Geisser and Huynh-Feldt tests.
Results
The 36 patients that completed the evaluation were grouped based on the analgesic technique selected by their clinical care teams: EAG (n = 30) and PNBAG (n = 6).
The demographic characteristics of the two groups are presented in Table 1, showing no significant differences between them. Age distribution was similar (p = 0.885), and sex distribution did not differ significantly between groups (p = 0.609). Regarding patients’ medical history, no statistically significant differences were observed between groups in the prevalence of comorbidities.
Demographic characteristics and comorbidities of the patients that completed evaluation
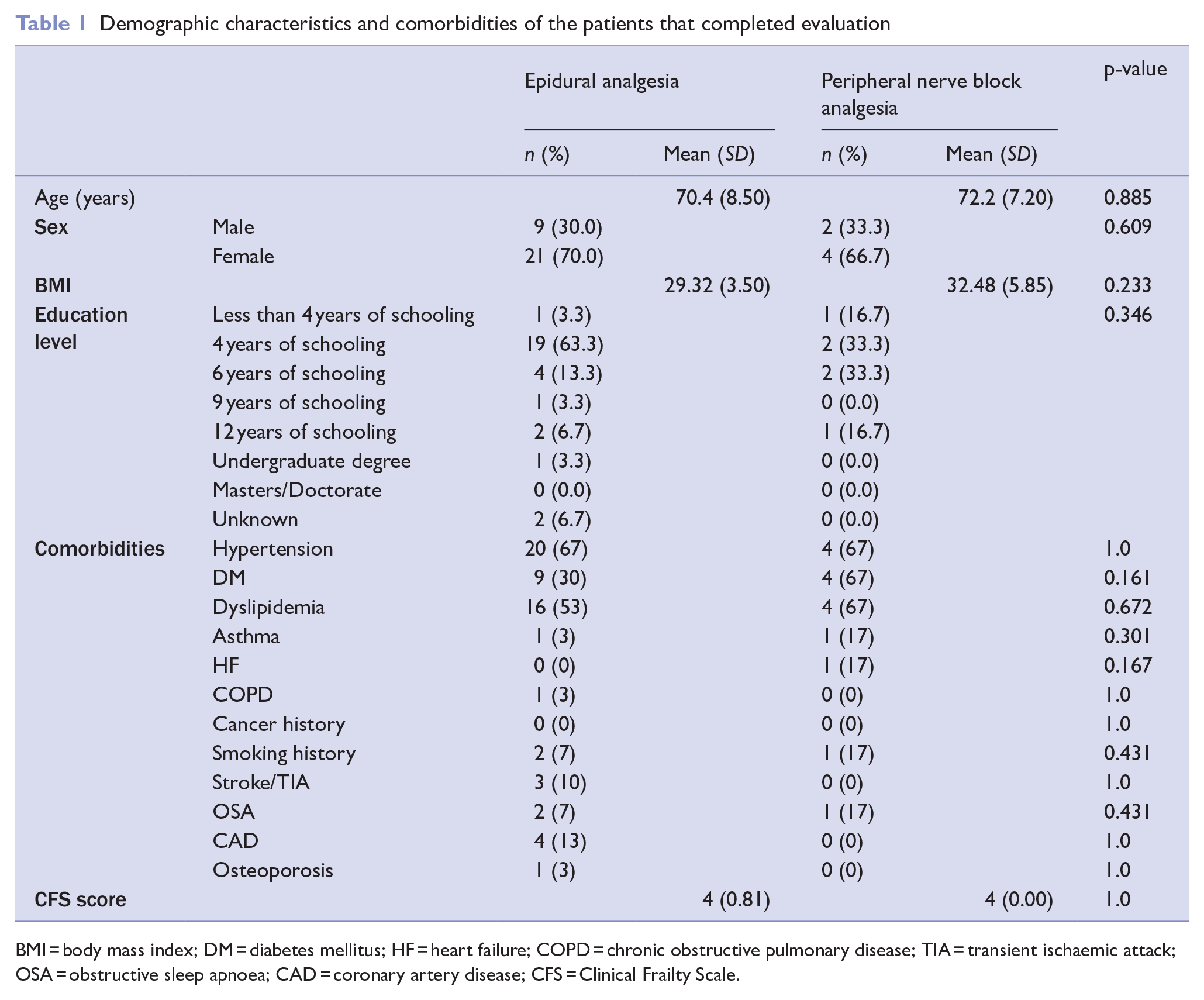
BMI = body mass index; DM = diabetes mellitus; HF = heart failure; COPD = chronic obstructive pulmonary disease; TIA = transient ischaemic attack; OSA = obstructive sleep apnoea; CAD = coronary artery disease; CFS = Clinical Frailty Scale.
Considering the KOOS domains, the comparison between the two groups is presented in the Results section Table 2. In the Symptoms subdomain, there was a statistically significant difference between groups (p = 0.046). However, when this variable was included as an independent variable in the multivariate logistic regression model, the OR was 1.027 (0.982–1.075) with no statistical significance (p = 0.247) (Table 3). There were also no statistically significant differences between groups considering the mean difference in the subdomains of Pain (p = 0.442), the ADL (p = 0.852) and Sports (p = 0.852). Considering the Knee-Related QoL subdomain, although the EAG showed a lesser deterioration (M = −1.68; SD = 2.30) than the PNBAG (M = −3.47; SD = 2.99), the p-value was 0.135. Following the bivariate analysis, a logistic regression model was conducted, being the KOOS QoL Difference included as an independent variable. It did not show a significant difference (p = 0.204) with the OR of 1.244 (0.888–1.742) (Table 3).
Score differences for the KOOS and EQ-5D questionnaires and bivariate analysis results
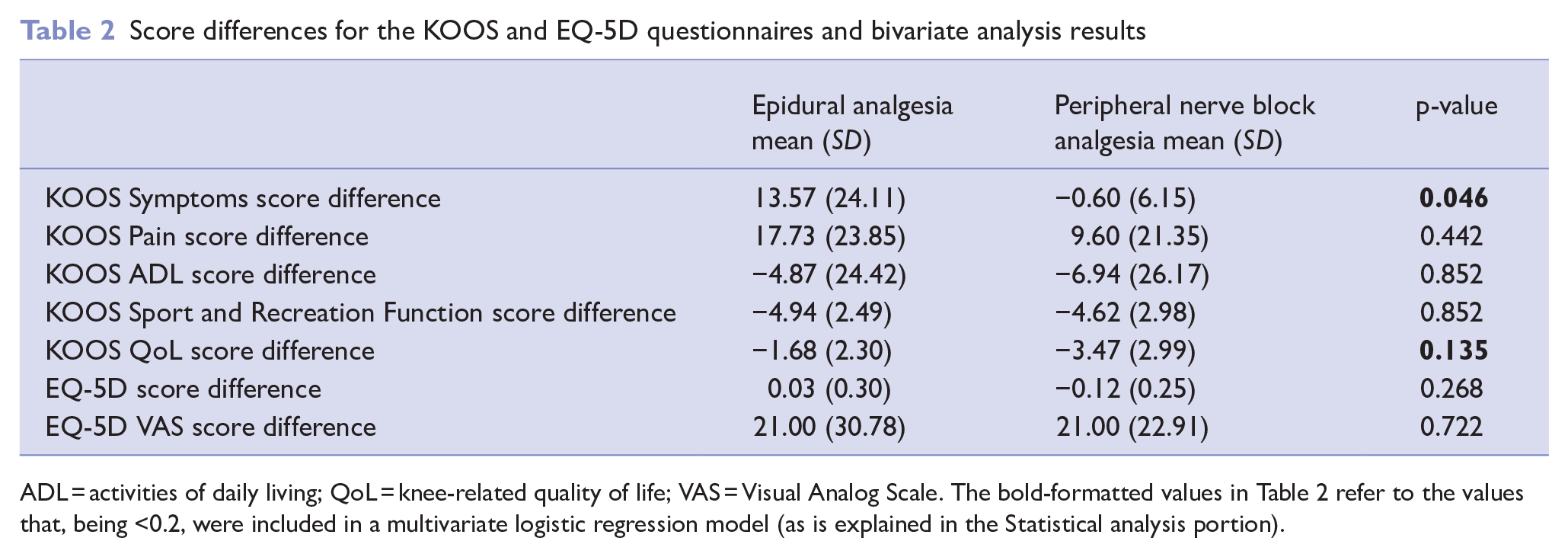
ADL = activities of daily living; QoL = knee-related quality of life; VAS = Visual Analog Scale. The bold-formatted values in Table 2 refer to the values that, being <0.2, were included in a multivariate logistic regression model (as is explained in the Statistical analysis portion).
Logistic regression analysis of predictors of analgesic technique selection
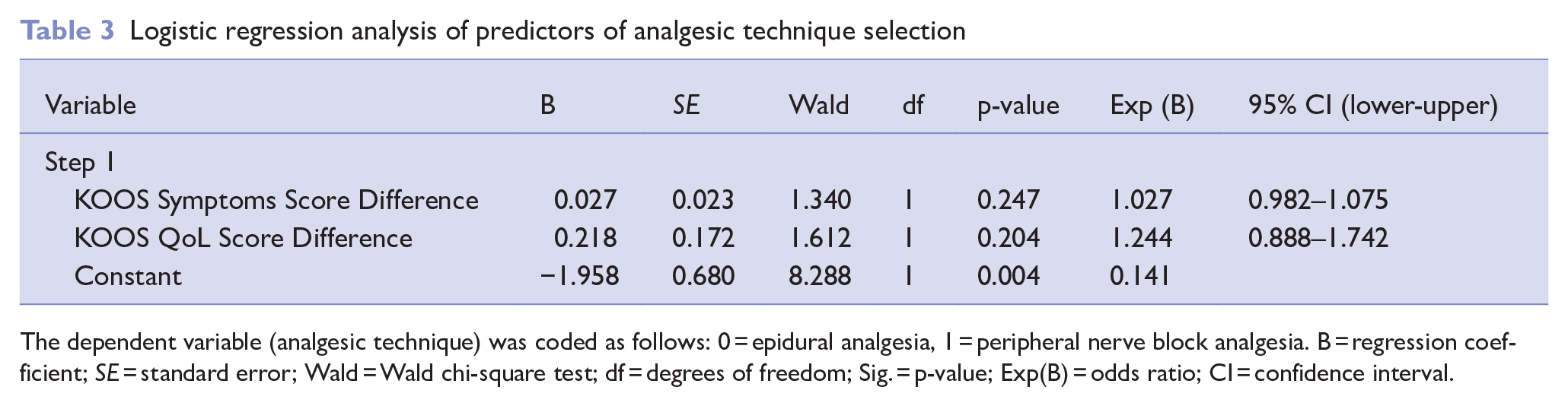
The dependent variable (analgesic technique) was coded as follows: 0 = epidural analgesia, 1 = peripheral nerve block analgesia. B = regression coefficient; SE = standard error; Wald = Wald chi-square test; df = degrees of freedom; Sig. = p-value; Exp(B) = odds ratio; CI = confidence interval.
To assess the trends found in the different KOOS domains, the Greenhouse-Geisser and Huynh-Feldt tests were conducted according to the Mauchly sphericity test evaluation results (Tables 4 and 5). Of the results between the subject factors, it can be concluded that the gender, educational background and BMI did not show significant results, meaning that these do not interfere with the KOOS score. An interaction was, however, identified between KOOS score and age, concluding that the patient’s age influences the perception of the different KOOS domains (p = 0.012).
Repeated measures ANOVA results evaluating the effect of time and KOOS scores on patient outcomes

Interaction effects between KOOS scores and clinical variables in the repeated measures ANOVA analysis
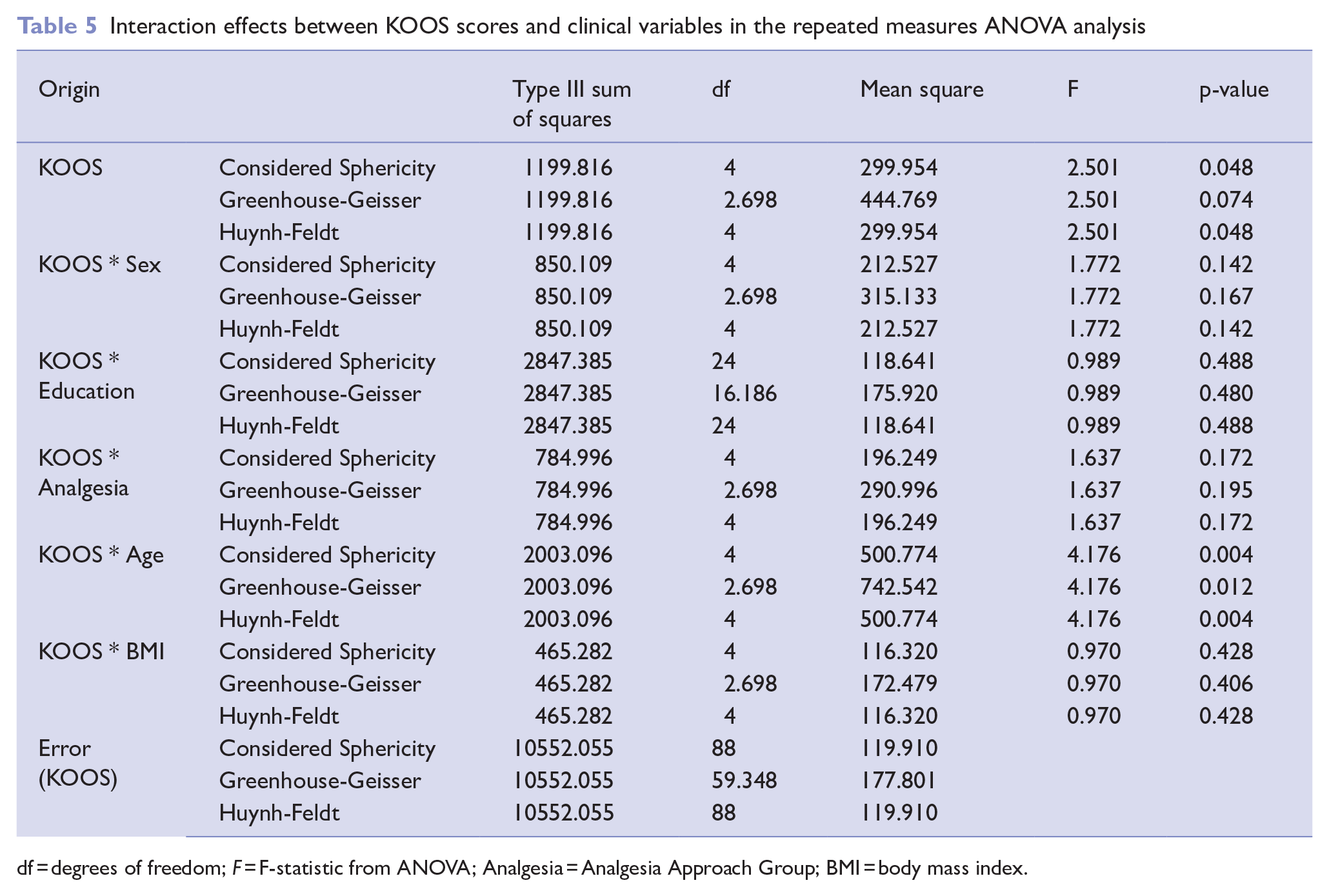
df = degrees of freedom; F = F-statistic from ANOVA; Analgesia = Analgesia Approach Group; BMI = body mass index.
The difference in EQ-5D scores from preoperative to postoperative assessment (Table 2) showed contrasting trends between groups. In the epidural group, the mean EQ-5D difference was 0.03 (SD = 0.30), while in the PNB group, the mean difference was −0.12 (SD = 0.25). Despite this trend, the difference between the two groups was not statistically significant (p = 0.268). Regarding the EQ-5D VAS score difference, both groups showed a mean increase of 21 in postoperative score.
The mean length of hospital stay was 4.9 days (SD = 1.2) in the EAG and 5.0 days (SD = 3.5) in the PNBAG. The median hospital stay was 4 days in both groups, indicating that most patients had a similar duration of hospitalisation regardless of the analgesic technique used (p = 0.881).
Discussion
This study evaluated the impact of epidural analgesia and PNBs on immediate patient-reported outcomes after TKA. The findings indicate that, although both techniques resulted in comparable outcomes in the 48–72 hours postoperatively, there are subtle differences in patient-reported outcomes that warrant further exploration.
KOOS bivariate analysis revealed that both groups experienced similar improvements across the Pain, ADL and Sport and Recreation Function domains, reinforcing the notion that both techniques offer similar functional benefits in the early postoperative period, as is reported by Gerrard et al (2017).
The EQ-5D descriptive system and Visual Analogue Scale scores showed no significant differences between groups. Interestingly, regarding the EQ-5D score difference, patients in the EAG experienced a modest improvement in perceived health status postoperatively. Despite this trend, the difference was not statistically significant, suggesting that both analgesic techniques had comparable short-term effects on health-related QoL.
Both these results contrast with typical trends reported in the literature, where PNB often results in better early functional outcomes (Memtsoudis et al 2016). These findings highlight the variability in early postoperative recovery, likely influenced by factors such as individual pain perception, surgical stress and mobility limitations immediately following TKA.
While epidural analgesia has traditionally been favoured, primarily due to its well-established efficacy in pain control and functional recovery (Rawal 2012), our findings indicate that PNBs offer a viable alternative with comparable early recovery outcomes. This is particularly relevant given the lower risk profile associated with PNBs. Compared to neuraxial analgesia, regional anaesthesia techniques have been shown to reduce the incidence of haemodynamic instability, urinary retention, motor block and postoperative nausea and vomiting, all of which can delay recovery (Hutton et al 2018). These advantages make PNBs an attractive option, especially in patients with pre-existing cardiovascular conditions or other contraindications to neuraxial techniques. These results emphasise the need for a more individualised approach when selecting analgesic techniques, considering not only pain scores but also broader recovery parameters such as mobility, side effects and overall patient experience.
Limitations of the study
While this study offers valuable insights into the impact of analgesic techniques on postoperative outcomes, certain limitations should be acknowledged. This was an observational prospective study, and every analgesia technique was the anaesthetist’s responsibility, with no standardisation considering each postoperative analgesia prescription. The small sample size may also limit the generalisability of the findings, and the short follow-up period (48 hours) prevents an assessment of long-term functional recovery, pain control and QoL improvements. The specific timing of the PNB (preoperatively or postoperatively) and the catheter placement were also not evaluated.
Conclusions and suggestions for further research
This study found that, between epidural analgesia and PNBs, no technique was considered to be superior regarding patient-reported outcomes in the immediate postoperative period for TKA. Both techniques provided effective pain relief and functional recovery, with a similar impact on QoL. These findings suggest that PNBs may serve as a viable alternative to the epidural catheter, particularly given their lower risk profile.
Longer-term studies are needed to determine whether functional recovery, mobility and pain control remain comparable beyond the immediate postoperative period and to assess patients’ satisfaction between these two analgesic techniques. It should also be addressed in additional research the difference between different PNBs and their effectiveness compared with epidural analgesia.
Footnotes
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical declarations
This study was approved by the Research Ethics Committee of the Unidade Local de Saúde São João (approval no. 445/2024) on January 16th, 2025.
Consent to participate
All participants signed a written consent before any interview or data collection.
Consent for publication
Not applicable.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.