
Abstract
This case report describes the perioperative management of a massive solitary fibrous tumour of the pleura in a 77-year-old woman undergoing thoracotomy. The tumour, occupying a substantial portion of the right hemithorax, posed significant challenges regarding airway management, haemodynamic stability, and postoperative recovery. A comprehensive anaesthetic strategy was employed, including advanced monitoring, lung isolation, multimodal analgesia, and preemptive planning for potential complications. Careful intraoperative coordination minimised blood loss and maintained haemodynamic stability, avoiding the need for transfusion. Postoperative analgesia was effectively managed with a thoracic epidural catheter, facilitating early mobilisation and respiratory recovery. The patient experienced a favourable postoperative course and was discharged home on the seventh day. This case underscores the importance of individualised anaesthetic planning and multidisciplinary collaboration when managing large intrathoracic tumours.
Keywords
Background
Solitary fibrous tumour of the pleura (SFTP) is a rare neoplasm, typically originating from the submesothelial mesenchymal layer of the visceral pleura. These tumours account for an incidence of approximately 2.8 cases per 100,000 people annually, reflecting their infrequent occurrence in clinical practice. When classified by size, a massive SFTP is defined as one that exceeds 15 cm in diameter or occupies more than 40% of the hemithorax (Cardillo et al 2012, Shen et al 2023).
The management of massive SFTP poses significant challenges in the perioperative setting, particularly during thoracotomy. The potential complications associated with these tumours – such as airway collapse, vascular compression, and haemorrhage – necessitate careful anaesthetic planning and surgical technique.
In this report, we describe the perioperative approach to a massive intrathoracic SFTP of the right hemithorax. Our case highlights the unique challenges faced during such procedures and aims to contribute to the understanding of effective anaesthetic approaches in similar clinical scenarios.
Case report
Written informed consent was obtained from the patient for the publication of this case report, including the use of non-identifiable clinical details and photographs. The patient was fully informed about the purpose of the report and assured that all information would be handled confidentially and anonymously. All identifying information has been omitted to protect the patient’s privacy.
A 77-year-old woman (height 154 cm, weight 53 kg), ASA II, was scheduled for resection of a solitary fibrous tumour in the right middle pulmonary lobe via thoracotomy. Her medical history was significant for adequately controlled type II diabetes, arterial hypertension, hypothyroidism, and dyslipidaemia.
An initial chest X-ray, performed as part of a primary health care evaluation for dyspnoea, revealed a marked elevation of the right hemidiaphragm (Image 1). This finding was confirmed by thoracic computed tomography, which demonstrated a mass in the right hemithorax measuring approximately 15 × 16 cm in the axial plane and 17 cm craniocaudally. A needle biopsy confirmed the diagnosis of solitary fibrous tumour. Cardiac testing (transthoracic echocardiography) and laboratory investigations were unremarkable. Pulmonary function testing revealed a restrictive ventilatory pattern, with postbronchodilator parameters of forced vital capacity (FVC) 58.5%, forced expiratory volume in 1 s (FEV1) 59.2%, and FEV1/FVC 78.3%. The patient was scheduled for surgical resection of the tumour via thoracotomy.
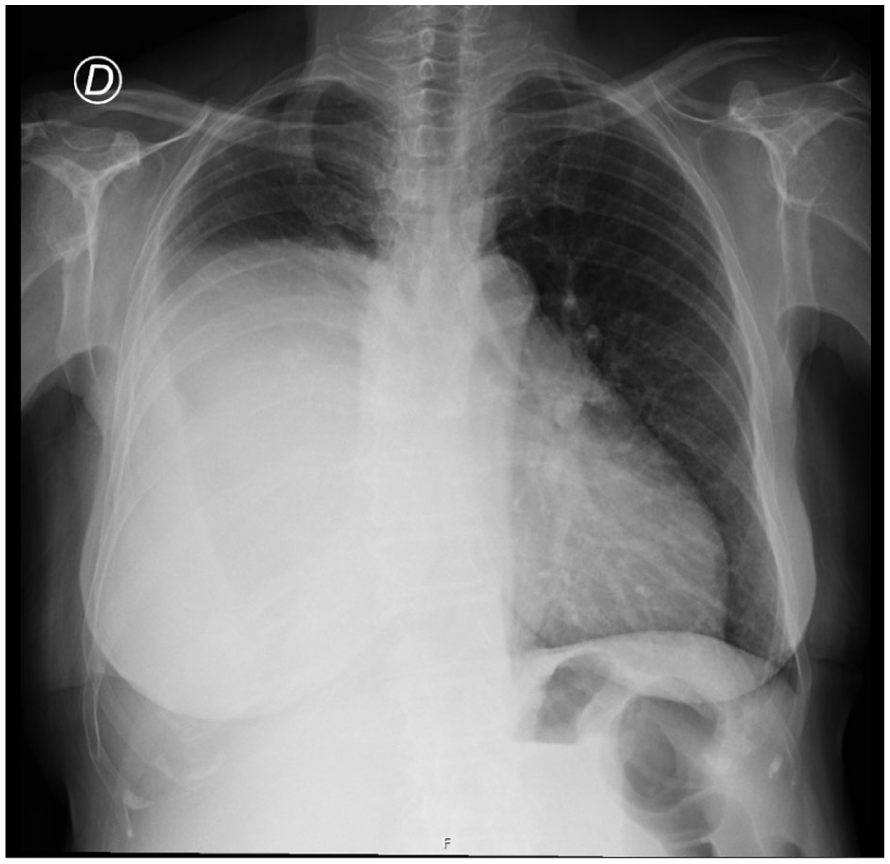
Preoperative X-ray showing marked elevation of the right hemidiaphragm
The patient was admitted the day before surgery, and two units of blood were cross-matched in advance. Following standard ASA monitoring (including bispectral index, cerebral oximetry, and invasive arterial pressure in the left radial artery), general anaesthesia was induced with fentanyl 100 µg, propofol 80 mg, and rocuronium 60 mg, and maintained with sevoflurane (minimum alveolar concentration 0.8). After induction, a central venous catheter was inserted into the right internal jugular vein, and tranexamic acid 1 g was administered. Tracheal intubation was performed using a 35-Fr left double-lumen endobronchial tube, with correct placement verified by fibreoptic bronchoscopy.
A right posterolateroanterior thoracotomy was performed through the seventh intercostal space (Image 2). Surgical exploration revealed a large tumoural mass occupying the lower two-thirds of the right hemithorax. Blunt dissection identified a pedicle at the pleural base, likely associated with the middle lobe. The tumour, measuring approximately 23 cm at its longest axis, was excised (Image 3). No additional pleural implants were observed. Haemostasis was verified, and haemostatic agents were applied to minor bleeding sites. Two chest drains (apical and basal) were placed, and the thoracotomy was closed in layers. Ropivacaine was infiltrated at the surgical site for postoperative analgesia. Estimated blood loss was 200 mL. The patient remained haemodynamically stable throughout, and intraoperative haemoglobin (after tumour resection) was 9.9 g/dL.
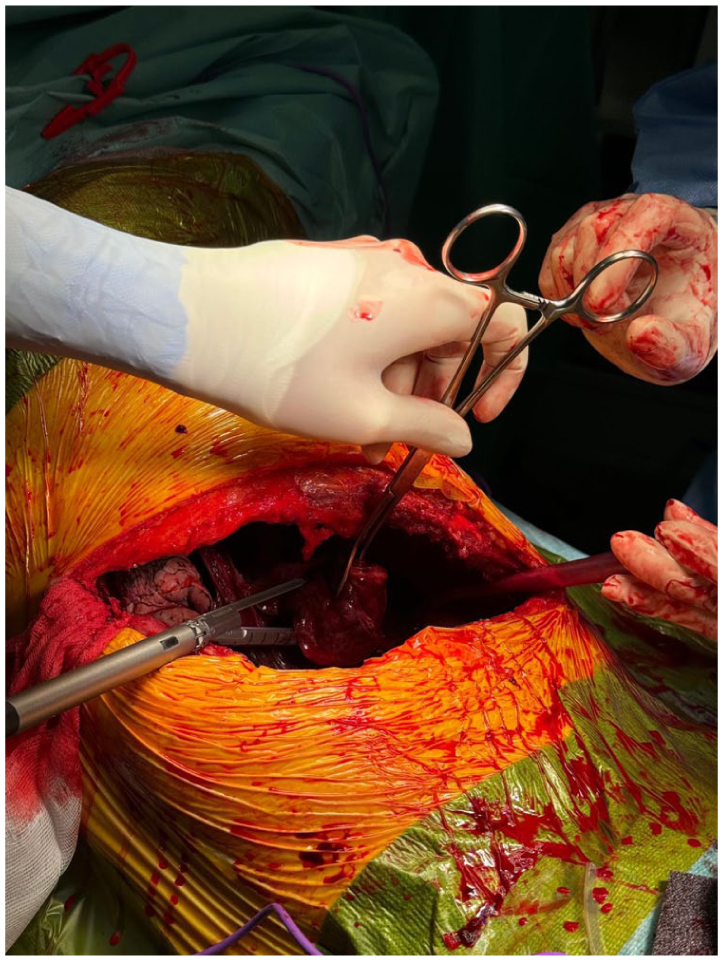
Surgical approach: right posterolateroanterior thoracotomy with an incision in the seventh intercostal space

Excised massive pulmonary fibrous tumour (approximately 23 cm in its longest axis)
Intraoperative systemic analgesia included a remifentanil infusion (0.07 µg/kg/min), ketamine 20 mg, magnesium sulphate 2 g, paracetamol 1 g, and tramadol 100 mg.
Following the procedure, a thoracic epidural catheter was inserted between the T6–T7 interspace. The patient was extubated and transferred to the intensive care unit for postoperative monitoring, where she remained for one day before transfer to the cardiothoracic surgery unit.
During the postoperative period, due to anaemia (haemoglobin 6.9 g/dL), ferric carboxymaltose was administered, resulting in an improvement to 9.9 g/dL. No major perioperative complications were observed. Postoperative chest X-rays demonstrated satisfactory recovery and pulmonary re-expansion (Image 4). Pain was well controlled using programmed intermittent epidural boluses of ropivacaine, supplemented by systemic analgesia. The epidural catheter was removed on the sixth postoperative day once pain was controlled. The maximum reported pain score was 3/10, with no motor block observed.
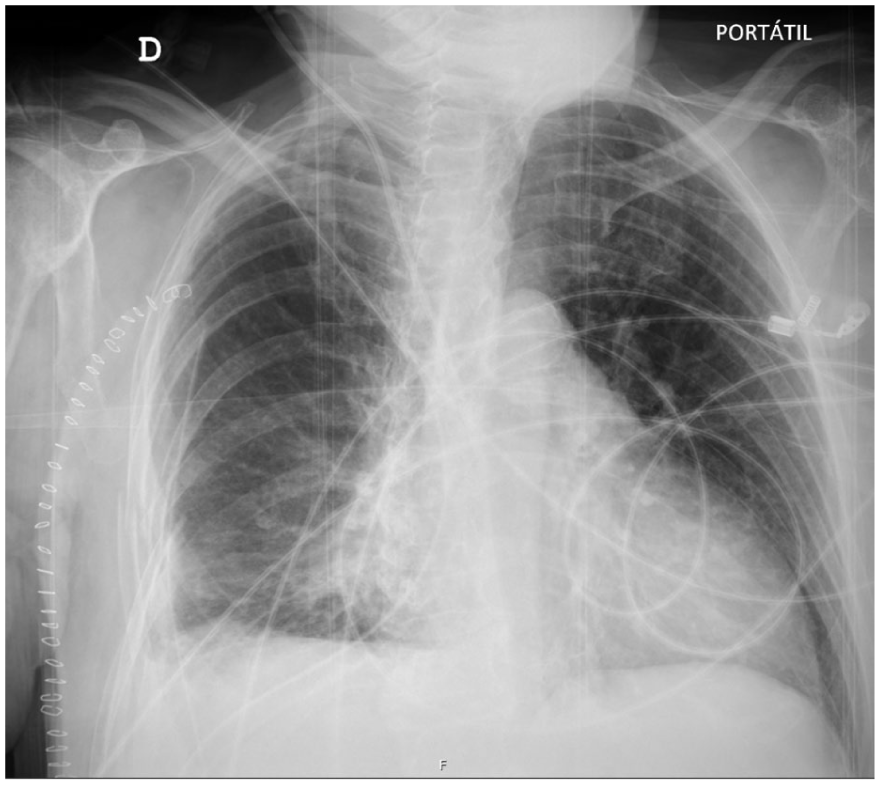
Postoperative follow-up X-ray showing satisfactory progress (re-expansion of the right lung previously collapsed by the massive fibrous tumour)
The patient was discharged home on the seventh postoperative day and referred to the pulmonology service for continued postoperative kinesitherapy and follow-up evaluation.
Discussion
In this case, we present a 77-year-old woman diagnosed with a massive solitary fibrous tumour of the right hemithorax, which posed significant challenges for anaesthetic management due to airway and great vessel compression. SFTPs account for less than 5% of all pleural tumours, making them an uncommon neoplasm (Shen et al 2023). Their slow clinical progression often allows them to remain asymptomatic for years, leading to delayed diagnosis. Many patients with SFTP are diagnosed incidentally through chest radiography rather than presenting with evident clinical symptoms (Jadczak et al 2014). The complete surgical resection of a massive lung tumour is particularly challenging due to the complexity of the surgical technique and the respiratory and circulatory instability associated with the tumour’s size and extensive blood supply.
Given the potential for circulatory instability, invasive blood pressure monitoring and central venous catheterisation were indispensable components of our anaesthetic plan. In addition, preparation for emergency resuscitative measures, including extracorporeal circulation, is vital when managing tumours that may severely compromise respiratory and circulatory function.
During surgery, careful attention must be paid to the risk of perineural invasion, particularly involving the phrenic nerve. Invasion of the phrenic nerve can significantly impair respiratory movement on the affected side, thereby adversely affecting the prognosis for patients with massive SFTP (Shen et al 2023).
An essential aspect of managing this case was close monitoring of haemoglobin levels, given the size of the tumour and its extensive vascular supply, which substantially increased the risk of intraoperative blood loss. In this instance, we were able to avoid the need for blood transfusion through meticulous perioperative planning – ensuring an adequate preoperative haemoglobin level, administering tranexamic acid intraoperatively to minimise bleeding, and enhancing the patient’s iron reserves postoperatively with ferric carboxymaltose. These measures, combined with precise surgical technique, contributed to maintaining stable haemoglobin levels throughout the procedure and optimised the patient’s perioperative outcome.
Another important consideration in this case was the management of postoperative pain. Given the large thoracotomy incision required for tumour resection, effective postoperative analgesia was crucial to ensure a smooth recovery. Inadequate pain control could result in poor ventilation, atelectasis, and increased postoperative morbidity. To address this, a thoracic epidural catheter was placed, providing effective analgesia and improving the patient’s respiratory mechanics postoperatively, as well as her ability to cooperate with kinesitherapy. The success of this analgesic strategy facilitated early mobilisation and reduced the risk of pulmonary complications.
Conclusion
The anaesthetic management of massive SFTP is not well documented in the literature, and our case provides valuable insights into effective strategies. The unique challenges presented by large tumours necessitate individualised approaches tailored to each patient’s condition.
In conclusion, this case highlights the importance for anaesthetists to recognise the specific challenges posed by massive lung tumours and to adapt their management strategies accordingly. Our experience may serve as a useful reference for clinicians managing similar cases in the future.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Consent for publication
Written informed consent was obtained from the patient for the publication of this case report, including the use of non-identifiable clinical details and photographs. The patient was fully informed about the purpose of the report and assured that all information would be handled confidentially and anonymously. All identifying information has been omitted to protect the patient’s privacy.