
Abstract
Background:
Every year 15% of all operative procedures take place in people with diabetes. Suboptimal glycaemic control is associated with increased postoperative complications. This study aimed to identify why people with diabetes have their operations cancelled and introduce interventions to reduce the rate of cancellation.
Methods:
A retrospective review of all adult people with diabetes with cancelled surgery in 2024 was completed in an inner-city teaching hospital. A new perioperative guideline for elective surgery in people with diabetes was implemented and cancellations were re-audited in June 2025.
Results:
Postintervention 7% of cancellations were due to suboptimal diabetes control, with none occurring within 2 weeks of surgery (previously 10% and 63%). Prior to intervention, only 32% of patients proceeded to surgery within 1 year of initial cancellation.
Conclusion:
People with diabetes experience significant delays to surgery; however, targeted perioperative guidelines enable early identification of suboptimal glycaemic control and reduced cancellations. This work highlights the importance of locally tailored perioperative pathways.
Introduction
In the United Kingdom, more than 323,000 operations are performed each year on people with diabetes (PwD), representing approximately 15% of all operative procedures (CPOC 2023). Suboptimal glycaemic management in the preoperative period is linked to numerous adverse outcomes including hypoglycaemia, hyperglycaemia, infection, delayed wound healing, increased length of stay and increased mortality (Frisch et al 2010, Page et al 2020).
By 2065, 26% of people in the United Kingdom will be over 65 years, and 46% will be 50 years or older (Centre for Ageing Better 2025). With our ageing population, the rising prevalence of comorbidities such as diabetes and the increasing ability to operate safely in this cohort, perioperative medicine is an increasingly topical and relevant field. Early recognition and optimisation of comorbidities are essential for safe and effective management of surgical patients. An estimated 5.8 million people in the United Kingdom live with diabetes, with prevalence increasing with age (Diabetes UK 2025). As this burden grows, timely identification and management of PwD are critical to substantially reduce perioperative complications and minimise the risk of surgical cancellations (Galway et al 2021).
Current evidence-based practice around perioperative care of PwD has been strongly influenced by the 2018 National Confidential Enquiry into Patient Outcome and Death (NCEPOD) report Highs and Lows, which reviewed PwD aged ⩾ 16 years undergoing surgery requiring at least one overnight stay. The report highlighted a lack of coordinated diabetes management across specialties and identified major shortcomings in preoperative assessment (NCEPOD 2018). For example, 43.4% of preoperative assessment clinics (POACs) in the study did not have specific guidance for PwD undergoing surgery. Furthermore, any guidelines that do exist are often complicated and difficult to implement, involving multi-step perioperative pathways (Page et al 2020). These inconsistencies compromise quality of care and lead to avoidable cancellations, especially when patients are deemed unfit due to suboptimal glycaemic control.
In response, evidence-based strategies have been developed and implemented to improve perioperative care and reduce cancellations. These include monitoring glycaemic control using HbA1c testing, prioritising diabetic patients early on theatre lists to minimise prolonged fasting, optimising perioperative management of anti-hyperglycaemic medications and actively engaging patients to be able to manage their condition throughout the surgical pathway (CPOC 2023). The Improve the Perioperative Pathway for Patients with Diabetes (IP3D) project implemented a specialist perioperative diabetes nurse, a preoperative optimisation clinic and a perioperative passport designed to empower patients to take control of their surgical journey, maintain healthy blood glucose levels and improve their general health (Page et al 2020).
The importance of these measures is underscored by large-scale data. A study examining reasons for surgical cancellations across 60,000 operations found that PwD had a 25.97% higher likelihood of cancellation compared to people without diabetes (cancellation rates 9.7% vs. 7.7%, 99% confidence interval (CI) = 1.54%) (Cho et al 2018). This highlights the direct impact of diabetes on surgical outcomes and reinforces the need for systematic, proactive perioperative management to reduce preventable cancellations.
Against this national backdrop, a local audit at an inner-city teaching hospital in December 2022 sought to evaluate how these issues manifest in practice. The audit reviewed referrals for perioperative diabetes management over 4 weeks and identified multiple shortcomings in the local pathway. Multiple referral sources, inappropriate use of speciality services, non-standardised documentation of perioperative plans and delays to diabetes team referral were all highlighted as reasons for suboptimal care for PwD. It was also noted that a significant proportion of these patients were having their operations cancelled.
The aim of this project was therefore to identify how many PwD have their operations cancelled, the reasons their operations were cancelled and, finally, to implement strategies to reduce the rate of cancellation.
Methods
Primary audit cycle
A retrospective observational study was performed on all adult PwD who had their surgery cancelled in our centre for a duration of 1 month (April 2024). Variables collected included type of diabetes, diabetes medication, surgical speciality and operation, preoperative HbA1c, reason and time of surgery cancellation, subsequent actions taken to improve glycaemic control and total delay to eventual surgery.
Review of current practice and guidelines
Key areas for improvement were highlighted:
Referrals should be made at time of referral for surgery to avoid unnecessary delays in glycaemic optimisation.
Education and training for staff involved in referring or receiving perioperative referrals was needed.
The date of surgery, priority, time and duration of surgery (number of missed meals) needed to be recorded on referral to the diabetes team.
A perioperative diabetes plan should be recorded on Epic for all patients with type 1 diabetes (T1DM).
To tackle some of the problems identified in the first cycle, a new guideline was created which aimed to provide a single point of access to the diabetes service and a clear referral pathway for patient optimisation (Figure 1).
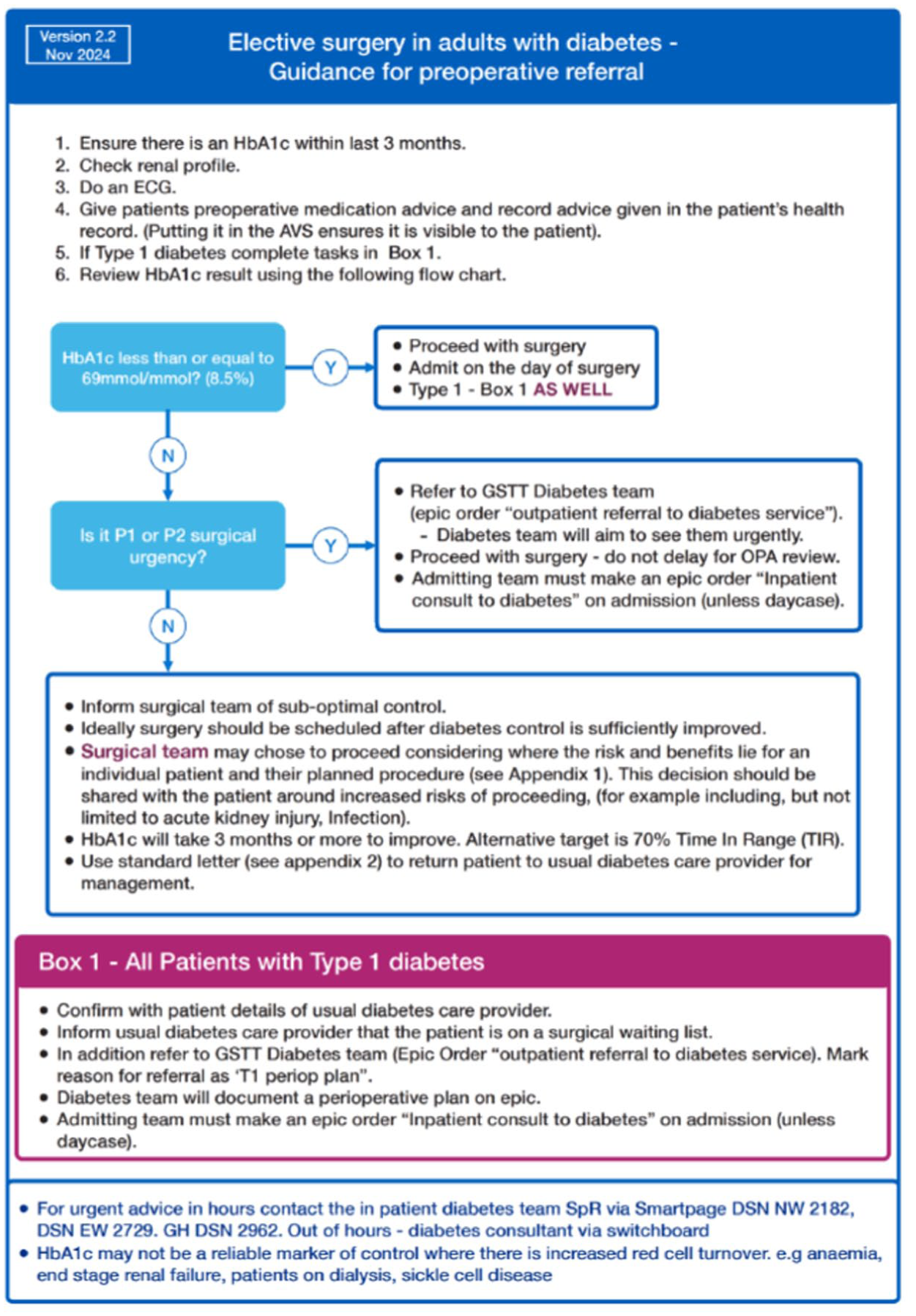
The new ‘Elective Surgery in Adults with Diabetes – Guidance for Preoperative Referral’ guidelines
The main changes to the guideline involved the use of the trust’s new electronic health record (EHR) system Epic to create a single portal for referring to the diabetes team for preoperative optimisation. The national framework for clinical prioritisation of surgical procedures (P1 – emergency, P2 < 1 month, P3 < 3 months, P4 > 3-month delay possible) was also used to aid triage of referrals within our service. Figure 2 summarises the perioperative pathway for PwD undergoing surgery at our centre. All people with T1DM on any surgical priority pathway should be referred as high risk and need a perioperative plan formalised on Epic. All PwD on P1/2 surgical pathways and with suboptimal control (HbA1c ⩾ 69 mmol/mol) should be referred to the diabetes team via Epic, and the diabetes team would aim to review urgently as an inpatient or outpatient. All people with Type 2 Diabetes (T2DM) on P3/4 pathways with suboptimal control should be referred to their local/current provider or their general practitioner (GP).
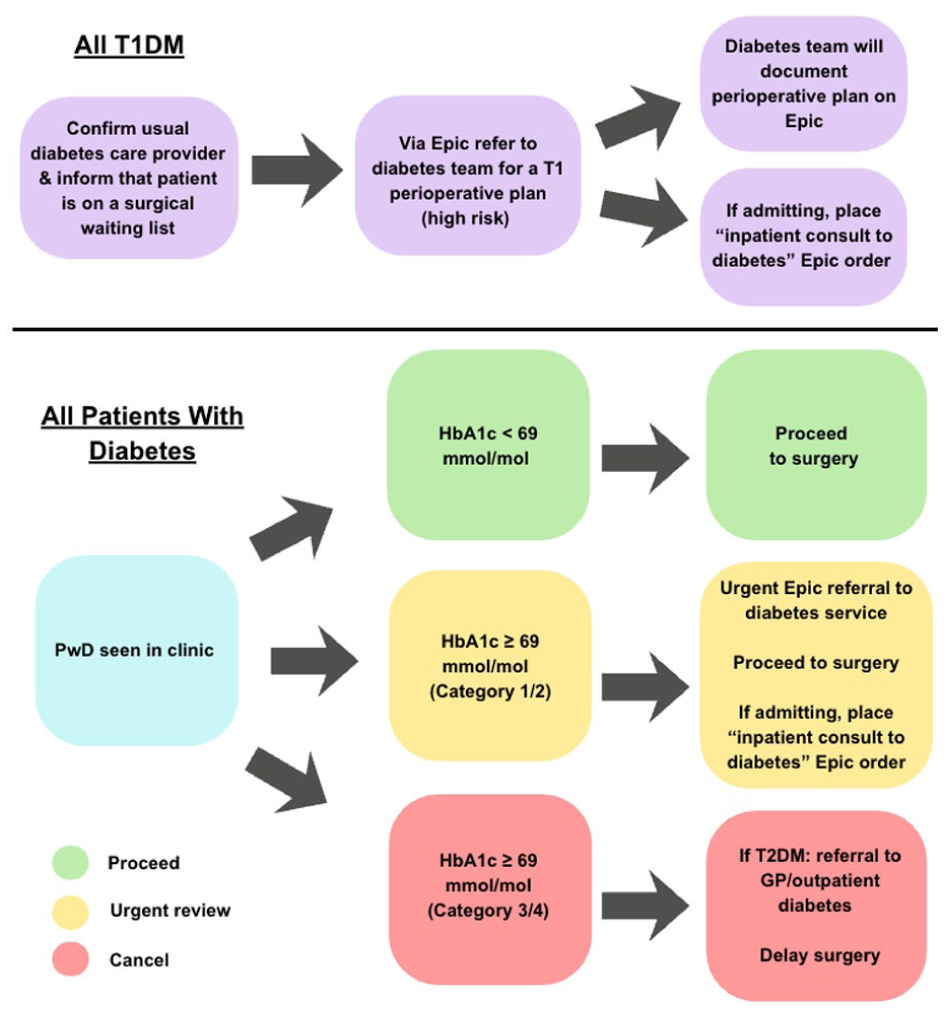
Flowchart summarising the perioperative pathway for PwD undergoing surgery at our centre, highlighting involvement of the multidisciplinary team (MDT)
All advice given to any PwD regarding preoperative management of their diabetes should be recorded in their after-visit summary so that it remains visible and accessible to patients on their health record after consultation.
The surgical team of any PwD on P3/4 pathways with suboptimal control should be notified, and ideally, the operation should be rescheduled until after diabetes control has sufficiently improved (HbA1c < 69 mmol/mol). An individualised risk assessment evaluating the type and urgency of surgery, patient’s overall health and comorbidities, duration and management of diabetes and potential benefits of surgery versus risks associated with elevated HbA1c can be performed with a multidisciplinary team (MDT) discussion involving the surgeon, anaesthetist, endocrinologist and primary care team. If a decision was made to postpone surgery in patients with T2DM, a standardised letter should be returned to the patient’s usual diabetes care provider for ongoing management.
This guideline went through peer review among the Perioperative Quality Improvement Diabetes Working Group, which consisted of a consultant anaesthetist with a specialist interest in perioperative care, diabetes consultants and an advanced nurse practitioner. The guideline was also approved by the trust’s diabetes governance teams.
Dissemination of new perioperative referral guidelines
The new guideline was launched on the trust intranet clinical guidelines page. To increase awareness of the project, the audit results and new guidelines were sent to the audit department leads of all surgical specialties at the trust which included general surgery, trauma & orthopaedics (T&O), ear, nose & throat (ENT) surgery, gynae-oncology, plastic surgery, vascular surgery, urology, breast surgery, cardiothoracic surgery and ophthalmology.
The results of the first audit and new guidelines were also presented at the general surgery, vascular surgery and T&O monthly audit meetings to try and encourage engagement with the new referral pathway. The key message to surgical specialties was identification of PwD with suboptimal glycaemic control by ‘the right team at the right time’. Clinicians were encouraged to check HbA1c and refer for optimisation when waitlisting for surgery rather than waiting for the POAC to detect suboptimal control, by which time optimisation would be too late and surgery would likely be cancelled.
To ensure the new guidelines would also be enacted in POAC, the guidelines were also disseminated to the perioperative nurses.
Results
Audit in April 2024
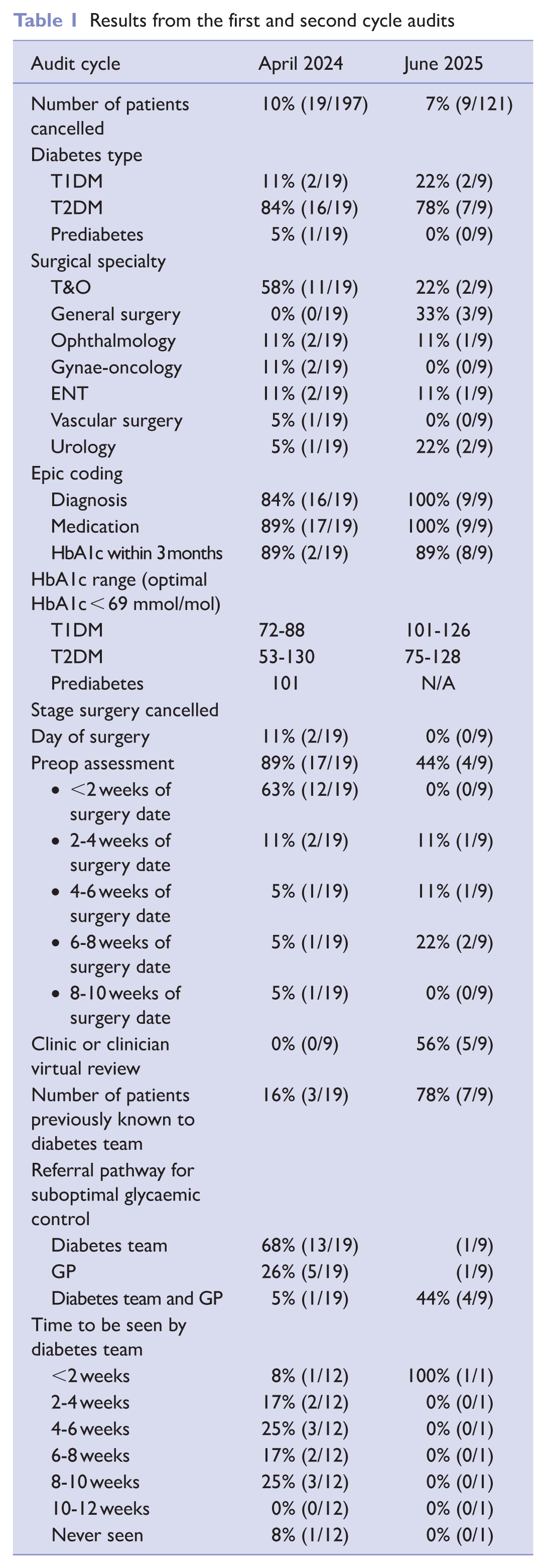
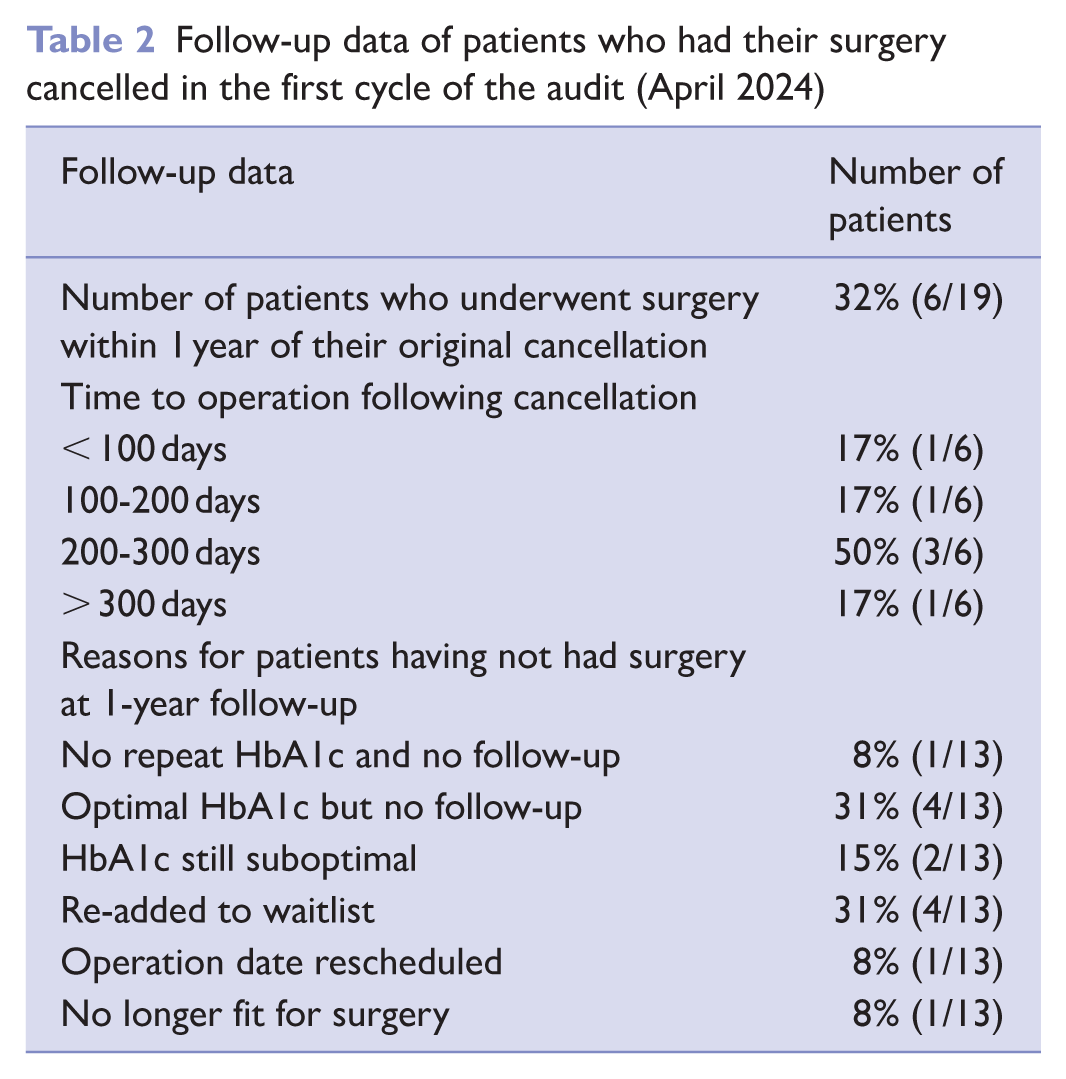
In April 2024, 19 out of 197 patients had their operations cancelled due to their glycaemic control (Table 1). Two patients were T1DM, 16 patients were T2DM and one patient was prediabetic patient. In total, 84% of patients had their diabetes diagnosis and 89% had their diabetes medications coded on Epic. In total, 95% had suboptimal HbA1c, and subsequently their operation was cancelled, and one patient had an optimal HbA1c, but their operation was still cancelled (HbA1c 53 mmol/mol but orthopaedic team wanted HbA1c < 50 mmol/mol). In total, 89% of patients had HbA1c within 3 months of their operation date. In total, 89% of patients had their operations cancelled at preoperative assessment, and 11% had their operation cancelled on the day of surgery. In total, 68% of patients were referred to the diabetes team for optimisation, 26% of patients were referred to their GP and 5% were referred to their GP and the diabetes team. Only 16% of patients were previously known to the diabetes team. On review 1 year later in April 2025, only 32% of the 19 patients who had their surgeries cancelled in April 2024 had undergone their operation (Table 2).
Results from the first and second cycle audits
Follow-up data of patients who had their surgery cancelled in the first cycle of the audit (April 2024)
Audit in June 2025
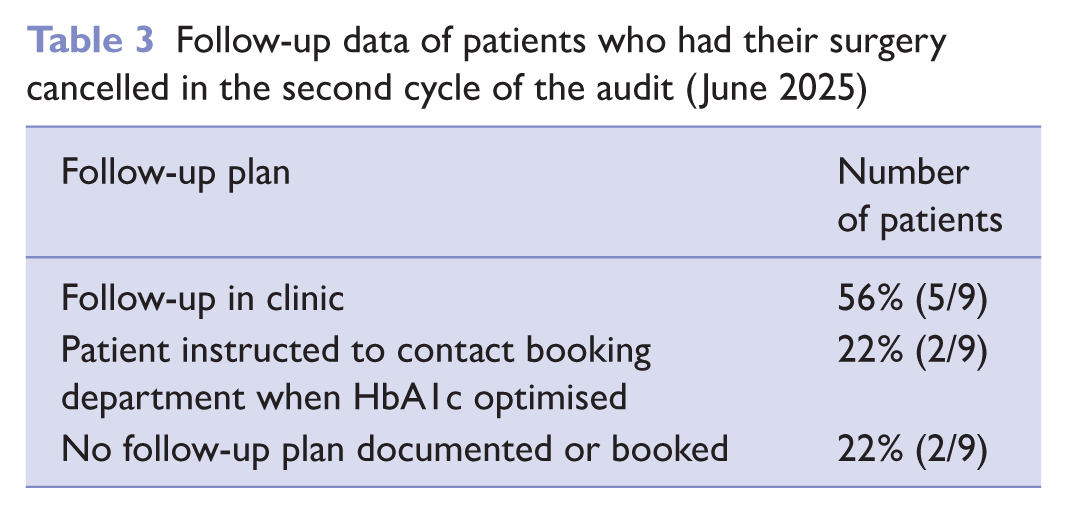
In June 2025, nine out of 121 patients had their operations cancelled due to their glycaemic control (Table 1). Two patients were T1DM, and seven patients were T2DM. In total, 100% of patients had their diabetes diagnosis and medication coded on Epic. All PwD with cancelled surgeries had suboptimal HbA1c, and 89% had an HbA1c within 3 months of their operation date. In total, 44% of patients had operations cancelled at preoperative assessment, and 56% were cancelled in the clinic or following virtual clinician review. No patients had their surgery cancelled within 2 weeks of their surgery date. In total, 78% of patients were already known to the diabetes team. In total, 44% of these patients were referred to their GP and the diabetes team for optimisation; one patient was referred solely to their GP, and one patient was referred as a new patient to the diabetes team and seen within 2 weeks of referral. Three months after cancellation, 78% of patients had follow-up arrangements planned (Table 3).
Follow-up data of patients who had their surgery cancelled in the second cycle of the audit (June 2025)
Discussion
Following the initial audit, several areas were identified for improvement. A new guideline was introduced with the aim to optimise perioperative diabetes control and, by doing so, identify suboptimally controlled patients early, enable specialist review, reduce complications associated with suboptimal glycaemic control and reduce the rate of surgical cancellations.
Following the implementation of the new guideline, the total number of PwD who had their surgeries cancelled reduced. The number of patients with a recorded diabetes diagnosis on Epic improved to 100%, which is vital in ensuring PwD are identified on our EHR. This ensures MDTs are aware of the diagnosis when surgery is booked and during the perioperative period. Furthermore, 100% of patients had their diabetes medications coded on Epic, allowing for accurate management of medications perioperatively, reducing perioperative glycaemic variability.
The use of Epic as an integrated EHR provides several advantages compared with paper-based or older systems. Epic permits quick and easy access to patient data including recent HbA1c levels, past medical history and current medications. This allows for early identification of patients who need optimisation prior to surgery and promotes timely communication between MDTs. The benefits of Epic compared with other systems in reducing surgical cancellations in PwD represent an interesting avenue of further research; however, this is outside the scope of this project.
The use of a single point of access for referral to the diabetes team via Epic also enabled streamlining of referrals and prioritisation of patient review. This is highlighted by the increased number of PwD already known and seen by the diabetes team before POAC and the timely review of the one newly referred patient within 2 weeks. We also observed increased instances of POAC directly communicating with the operating surgeon prior to cancellation, along with increased follow-up of those whose surgeries were cancelled, highlighting the benefits of an MDT approach.
During the second cycle, no patients had their surgeries cancelled within 2 weeks of their operation date. While this is important from a scheduling perspective, it also highlights that patients with suboptimally controlled diabetes are being highlighted earlier in the preoperative pathway. In addition, there was an increase in the number of patients who had their surgeries cancelled during outpatient clinics and on virtual review, suggesting that clinicians were reviewing the HbA1c of patients on their waitlist and referring for optimisation earlier. This shift indicated a more proactive approach from surgical colleagues, reflecting an improved awareness and integration of perioperative diabetes management into routine surgical planning. When viewed in the context of the 2018 NCEPOD report and IP3D project, this represents a shift towards following national recommendations of timely optimisation of PwD ahead of surgery and an MDT approach to management (NCEPOD 2018, Page et al 2020).
A key concern from the first audit was the number of patients still awaiting surgery a year after cancellation. Presenting our findings at multiple surgical audit meetings allowed surgical teams to directly engage with the new guideline and clarify department-specific questions. A suggestion for further improvement involving integrating HbA1c with an automated referral to the diabetes team within the operative booking form on Epic was also made. Given the number of patients still awaiting surgery 1 year following our first audit, specialties were also encouraged to review their follow-up pathways for PwD with cancelled surgery. This effort has been reflected in the increased number of patients who were followed up by the specialties postcancellation in the second cycle of our audit.
Generally, documentation around the reason surgery was cancelled in all patients waitlisted for surgery was lacking. It is likely that as a result many PwD who had their surgeries cancelled during our audit period have not been evaluated, and so the numbers we have recorded are likely an under-representation. Possibly due to the small sample size, we were therefore unable to draw any statistically significant results from our data.
While there was a decrease in the overall number of PwD having their surgeries cancelled, there was an increase in PwD having surgery cancelled in certain specialties after the new guideline. This is likely not reflective of the new guidelines but possibly a combination of Epic coding extraction, consultant list availability during the audited period and patient-specific complexity.
Going forward, we are in discussion with the Epic programming team to try and introduce a prompt to review HbA1c in PwD on our operation booking form. An automatic referral to the patient’s general practice would then be suggested if HbA1c is suboptimal. We will also strive to encourage better documentation of optimisation plans and the reasons surgeries are cancelled.
Conclusion
The introduction of the perioperative diabetes management guidance has led to improvements in early recognition, optimisation and management of PwD undergoing surgery. By promoting early identification of suboptimal glycaemic control, through MDT communication and collaboration, we have seen a reduction in the number of PwD having their operation cancelled. These changes reflect progress towards the recommendations set out in the 2018 NCEPOD report, IP3D project and 2023 CPOC guideline, which highlight early optimisation and coordinated perioperative care as key principles of perioperative management of PwD (CPOC 2023, NCEPOD 2018, Page et al 2020). Supported by improved access to data using an advanced EHR in Epic and designing a perioperative diabetes dashboard, this study represents a shift towards a safer and patient-centred approach to care.
Footnotes
Acknowledgements
We acknowledge Dr Craig Johnstone for his assistance with data extraction from Epic and Professor Janaka Karraliedde, Dr Anna Brackenridge and Dr Dulmini Kariyawasam for their contributions in developing the guidelines.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical considerations
This study has not required research ethics approval but has been granted local audit approval.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Data availability
Data will be made available on request.