
Abstract
Background
Multidisciplinary perioperative pathways are associated with improved outcomes in colorectal surgery, but evidence on real-world implementation is still scarce, especially in limited-resource settings.
Methods:
An audit was conducted targeting first-year outcomes after implementation of the Optimised Recovery Programme in Colorectal Surgery at a tertiary public hospital since February 2024. Results were compared with a historical pre-implementation cohort treated in 2022. Outcomes and quality indicators were analysed using descriptive statistics.
Results:
Despite a higher proportion of patients with severe systemic disease in the optimised recovery cohort, mean hospital length of stay decreased substantially, as well as readmission rates, with no increase in 30-day mortality.
Conclusions:
Real-world implementation of a multidisciplinary perioperative pathway was feasible and safe, even in a high comorbidity population and limited-resource setting. These findings support the value of structured perioperative systems of care and multidisciplinary coordination in routine clinical practice.
Keywords
Introduction
Background
Over the past two decades, perioperative care has undergone a substantial transformation, driven by the growing recognition that surgical outcomes depend not only on technical performance but also on coordinated, multidisciplinary perioperative systems of care (Kehlet 2011, Ljungqvist et al 2017). Enhanced Recovery After Surgery (ERAS®) pathways represent one of the most influential models in this evolution, integrating evidence-based interventions across the preoperative, intraoperative and postoperative phases to attenuate surgical stress, preserve physiological function and accelerate recovery (Ljungqvist et al 2017).
In colorectal surgery, ERAS-based pathways have consistently demonstrated reductions in postoperative complications, length of hospital stay and health care costs while improving patient experience and functional recovery (Fearon et al 2005, Feldheiser et al 2016, Greco et al 2014, Lee et al 2014, Varadhan et al 2010). As a result, ERAS principles are now widely considered a standard of care in elective colorectal procedures (Gustafsson et al 2019, 2025). Nevertheless, translating these recommendations into routine clinical practice remains challenging. Real-world implementation often requires substantial organisational change, multidisciplinary coordination and sustained professional engagement, factors that are frequently underestimated in controlled research environments (Gillissen et al 2013, Thanh et al 2020).
Despite the strong evidence supporting ERAS pathways, implementation across health care systems has been heterogeneous (Gillissen et al 2013, Thanh et al 2020). Barriers commonly reported include limited institutional resources, absence of dedicated digital platforms, variability in professional adherence and difficulties in integrating perioperative teams across departmental boundaries (Gillissen et al 2013, Gramlich et al 2017, Thanh et al 2020). Consequently, a significant gap persists between guideline recommendations and everyday perioperative practice, particularly within public health care systems operating under financial and organisational constraints (Gramlich et al 2017).
In this context, real-world evaluations of ERAS-based implementation strategies are increasingly recognised as essential to complement evidence derived from randomised controlled trials (Peden et al 2019, Sauro et al 2024). Understanding how perioperative pathways are operationalised in routine practice, how teams adapt protocols to local realities and what outcomes can be achieved outside highly resourced centres is fundamental for the broader dissemination of high-value perioperative care models (Gramlich et al 2017, Peden et al 2019, Sauro et al 2024).
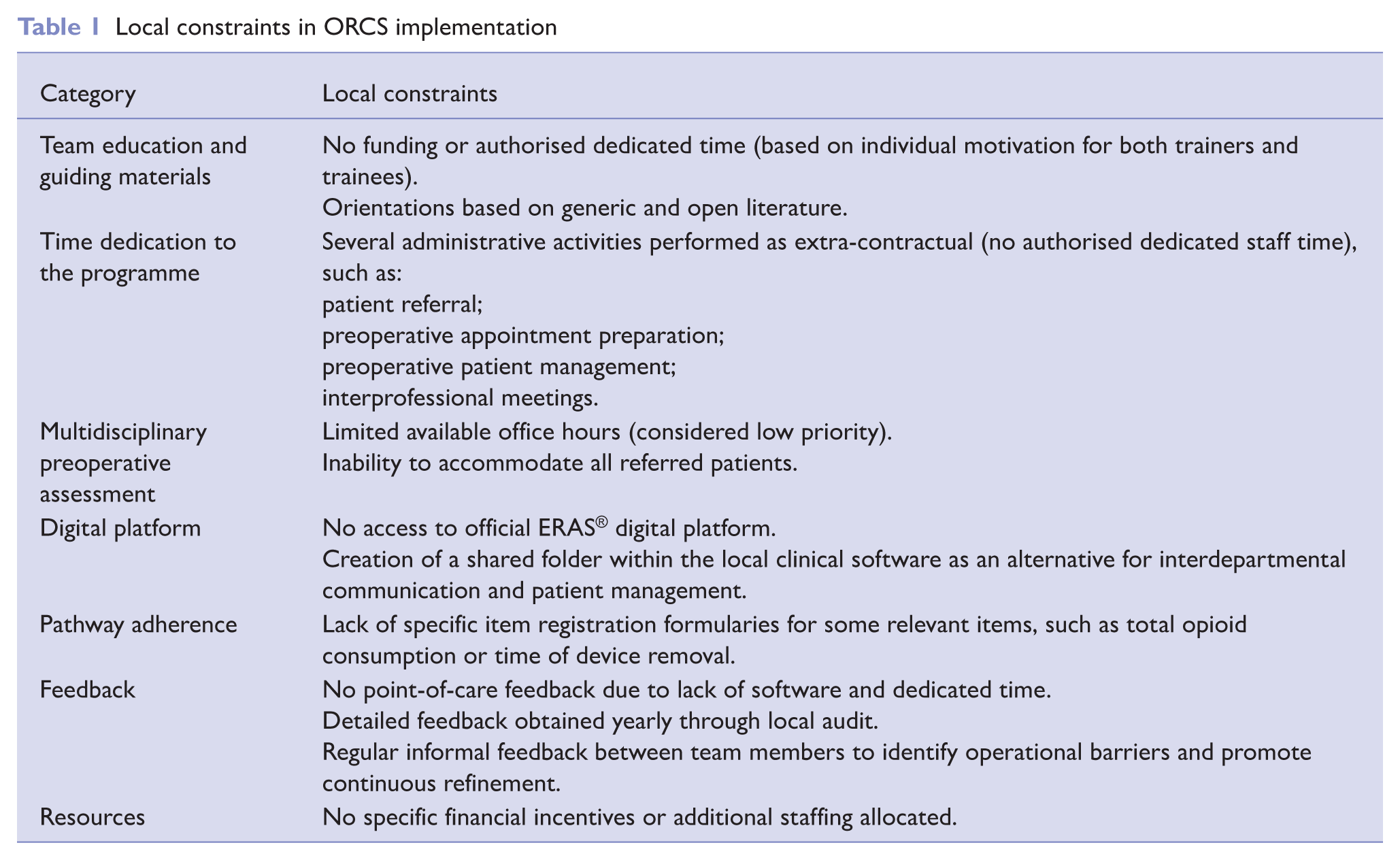
At our institution, previous local audits highlighted opportunities for improvement in perioperative coordination and postoperative recovery following elective colorectal surgery (Rodrigues et al 2024). In response, a multidisciplinary team initiated the implementation of an ERAS-based perioperative pathway – the Optimised Recovery Programme in Colorectal Surgery (ORCS) – adapted to the local organisational context, which included limited staff and dedicated time and no access to the official ERAS® digital platform (Gramlich et al 2017, Thanh et al 2020). To compensate for these limitations, the programme emphasised structured preoperative multidisciplinary assessment, standardisation of key perioperative care processes and enhanced communication across clinical teams (Gramlich et al 2017, Kehlet 2011, Ljungqvist et al 2017, Thanh et al 2020).
Methods
Study design
We conducted a retrospective cohort analysis, evaluating the first year of implementation of an ERAS-based multidisciplinary perioperative care pathway for elective colorectal surgery at a public tertiary hospital. Clinical and system-level outcomes observed after pathway implementation were compared with those from a historical pre-implementation cohort (Rodrigues et al 2024).
This study is reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for observational research.
Setting
The study was performed at a tertiary public hospital within the Portuguese National Health Service, providing specialised surgical care. Prior to implementation, perioperative management of colorectal surgery followed conservative, non-standardised pathways, with limited formal coordination between perioperative disciplines.
In response to previously identified variability in perioperative practices, a multidisciplinary working group initiated the development of a structured perioperative pathway based on ERAS® principles, adapted to local organisational constraints (Rodrigues et al 2024).
Programme design and implementation
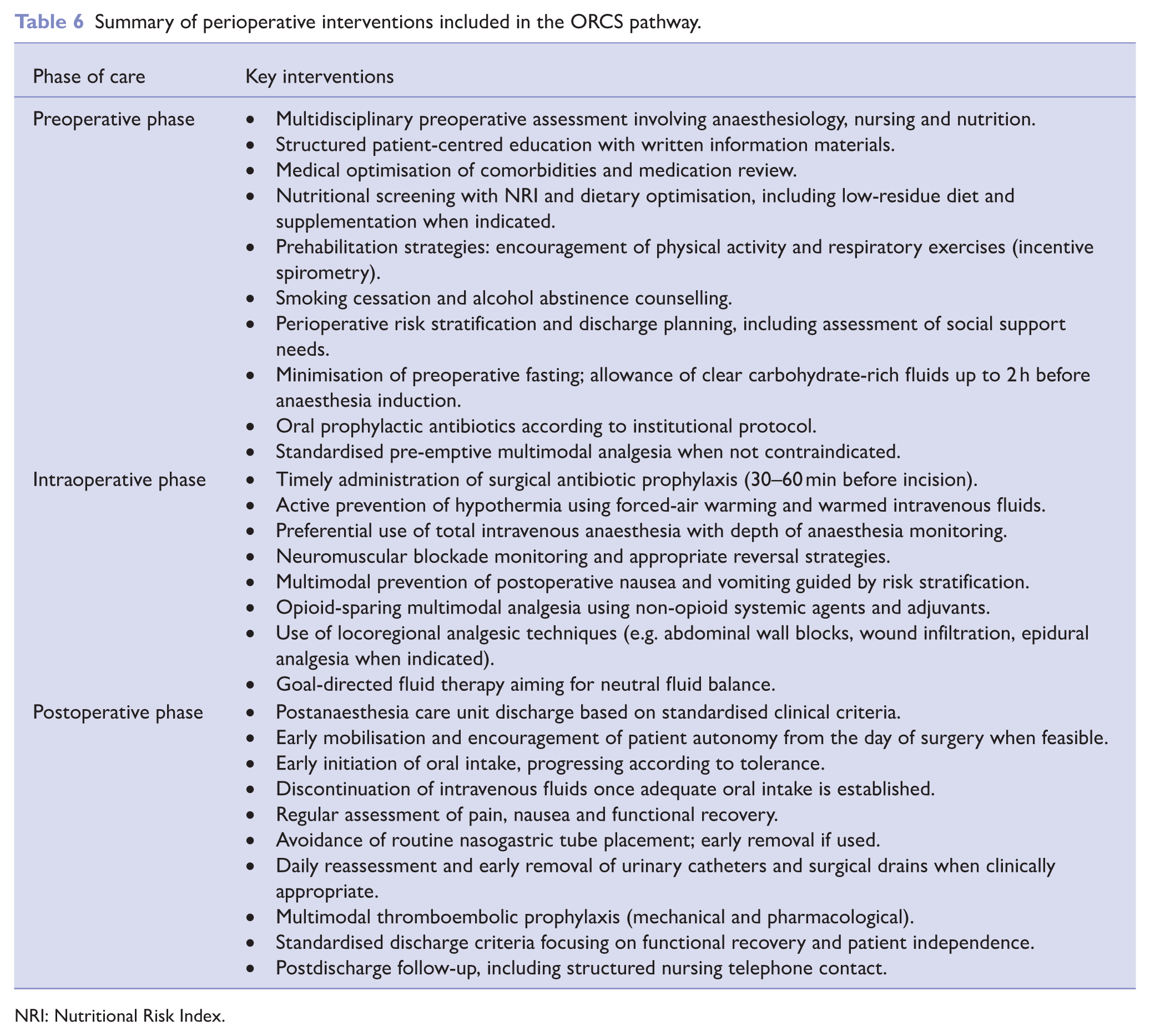
The Optimised Recovery Programme in Colorectal Surgery (ORCS) was designed as a multidisciplinary perioperative care pathway encompassing the preoperative, intraoperative and postoperative phases of care. The programme was implemented in February 2024, guided by the 2018 ERAS® Society recommendations for elective colorectal surgery and adapted to local clinical workflows (Gustafsson et al 2019). Detailed information can be found in the Appendix section (Table 6).
Key elements of the programme included:
Structured multidisciplinary preoperative assessment involving anaesthesiology, nursing and nutrition.
Standardisation of selected perioperative care processes, such as surgical drain and urinary catheter removal.
Early postoperative mobilisation and oral intake.
Predefined discharge criteria.
Enhanced interprofessional communication throughout the perioperative period.
Implementation occurred through an interactive multidisciplinary initiative rather than through a single institutional mandate. Educational sessions were delivered to clinical teams prior to programme launch and written perioperative guidance materials, as well as checklists, were developed for both health care professionals and patients.
Table 1 provides a summarised overview of local operational constraints and some alternatives adopted as tools for workflow simplification.
Local constraints in ORCS implementation
Participants
Adult patients undergoing elective major colorectal surgery between February 2024 and January 2025 were managed within the ORCS pathway and constituted the post-implementation cohort. Patients undergoing emergency surgery, combined non-colorectal procedures or those referred less than 1 week prior to surgery were excluded, as adequate preoperative pathway implementation was not feasible.
A historical pre-implementation cohort comprised patients who underwent elective major colorectal surgery between January and December 2022, prior to the introduction of ORCS, using previously collected institutional audit data.
Variables and data collection
Data were retrospectively extracted from electronic medical records and institutional databases following hospital discharge.
Collected variables included patient demographics, comorbidities, American Society of Anesthesiologists (ASA) physical status classification, type of surgical procedure, surgical approach and perioperative process indicators.
Primary outcomes included hospital length of stay (LOS), 30-day readmissions and 30-day mortality. Secondary outcomes comprised selected postoperative complications and perioperative process indicators, including timing of mobilisation, initiation of oral intake, use and duration of nasogastric tubes, urinary catheters and surgical drains.
Estimated inpatient cost savings were calculated based on the observed reduction in LOS and national reference values for daily hospitalisation costs (Fronteira et al 2025).
Data analysis
Descriptive statistics were used to summarise demographic characteristics, perioperative processes and clinical outcomes. Continuous variables are presented as means with ranges, and categorical variables as frequencies and percentages.
Given the observational nature of the study and the absence of randomisation, analyses were primarily exploratory and focused on describing trends associated with pathway implementation rather than establishing causal relationships.
Results
Participants and descriptive data
A total of 166 patients were initially assigned to the ORCS protocol. Of these, 57 patients were excluded from the analysis for the following reasons: cancellation of the planned procedure (n = 4), concomitant non-colorectal surgeries performed (n = 3) and insufficient referral timing (< 1 week; n = 50). After applying these exclusions, the final ORCS cohort consisted of 109 patients. This group was compared with a pre-implementation cohort of 93 patients (pre-ORCS) (Rodrigues et al 2024).
Patient characteristics in each group (pre-ORCS vs. ORCS group) are summarised in Table 2. Obesity, respiratory disease and active smoking were twice as prevalent in the pre-ORCS group. However, despite higher global prevalence of comorbidities in the pre-ORCS group, ASA physical status classification pointed towards worse systemic disease in the ORCS group, with 50% of the patients classified as ASA III (vs. 29% of patients in pre-ORCS). Previously published data of the pre-ORCS cohort found no correlation between these variables and complications (Rodrigues et al 2024).
Patient characteristics in each group (pre-ORCS vs ORCS)
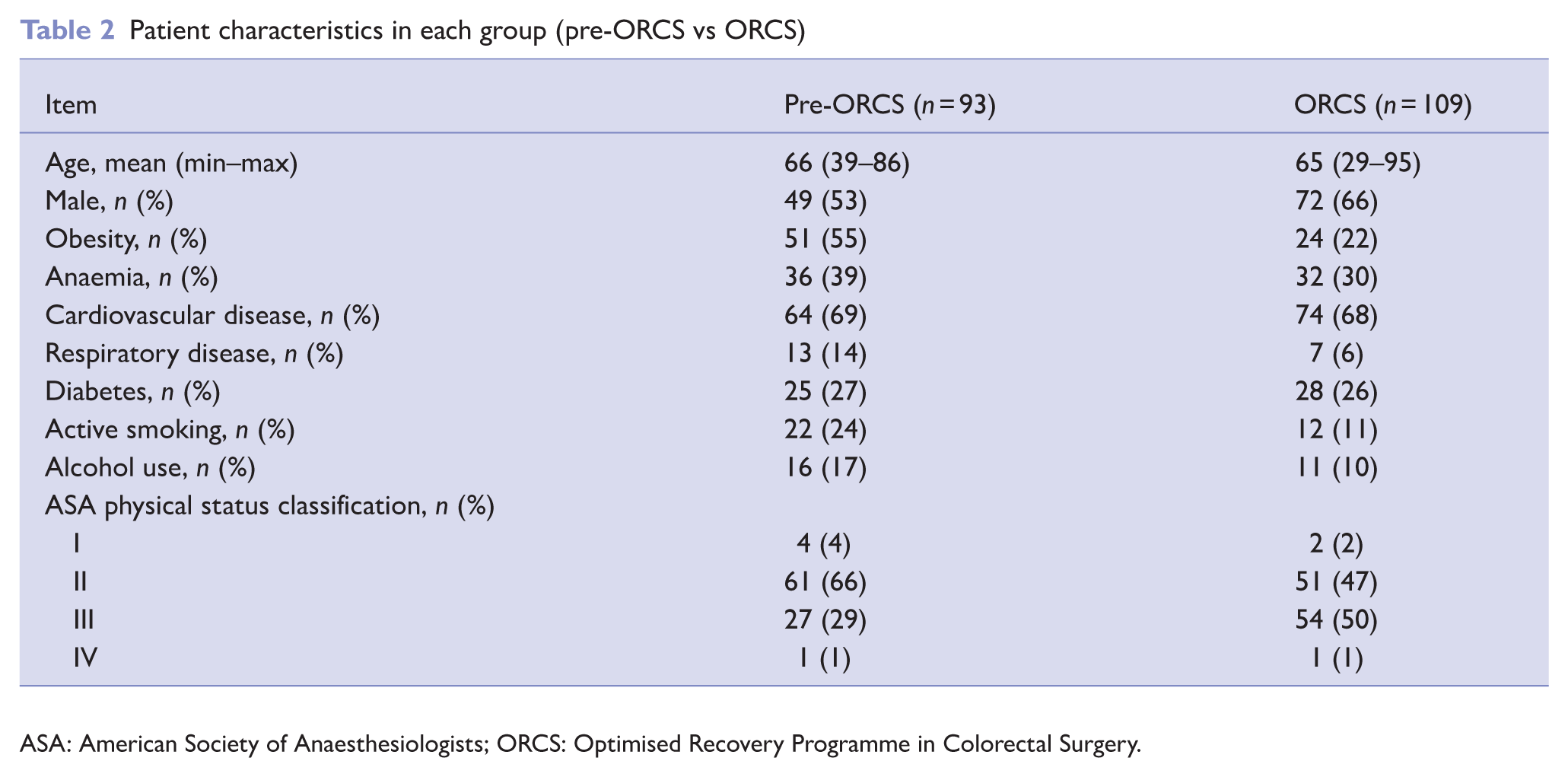
ASA: American Society of Anaesthesiologists; ORCS: Optimised Recovery Programme in Colorectal Surgery.
Unlike pre-ORCS, all ORCS patients (n = 109) underwent a preoperative consultation. In the ORCS group, 61 (44%) patients required additional evaluations or interventions from other specialities, including transfusion medicine, endocrinology, cardiology, pulmonology, internal medicine, vascular surgery, general and family medicine and otorhinolaryngology, for appropriate preoperative optimisation. Two (2%) patients required reassessment during the preoperative consultation process, which delayed clearance for surgery by approximately 6 days. Ultimately, all patients were deemed fit for surgery.
Table 3 provides an overview of the procedure types performed and the corresponding surgical approaches.
Procedure types in each group (pre-ORCS vs ORCS)
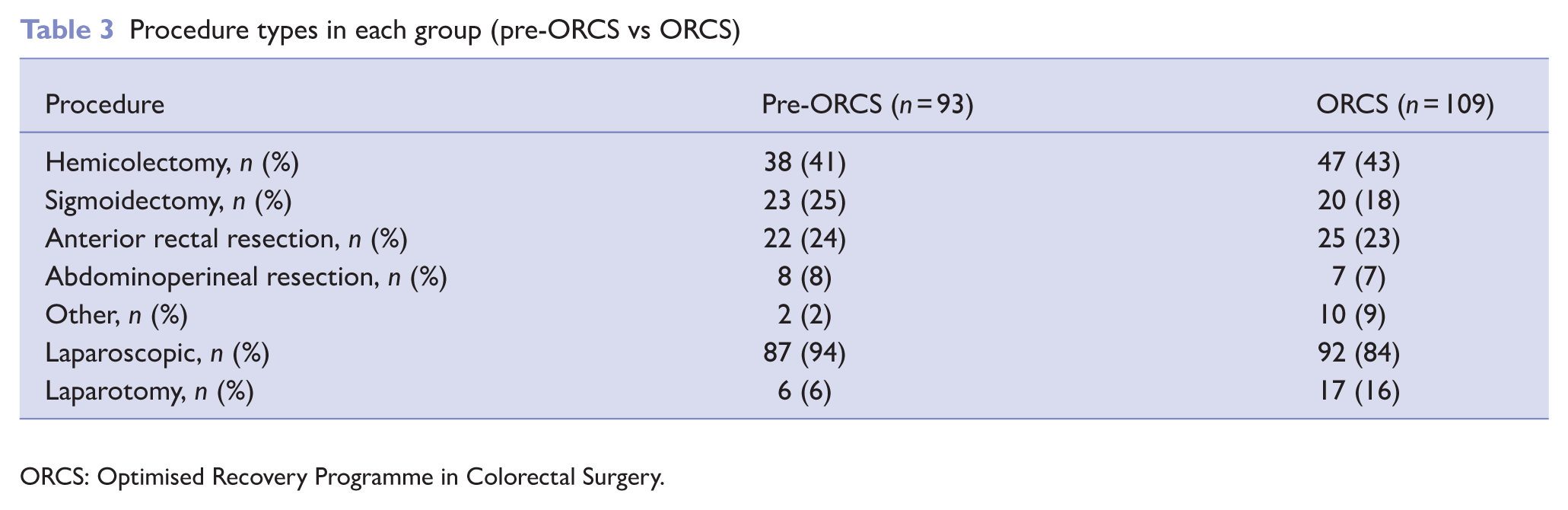
ORCS: Optimised Recovery Programme in Colorectal Surgery.
Outcome data
Tables 4 and 5 outline postoperative quality indicators and metrics, complications and major outcomes. Regarding postoperative complications, the most frequent were anastomotic dehiscence (n = 7, 6%) along with postoperative ileus (n = 7, 6%) and urinary tract infection observed in seven (6%) patients. A reduction was noted in the incidence of common surgical complications, including surgical site infection (n = 6, 5%) and postoperative ileus (n = 7, 6%), as well as medical complications such as urinary tract infection (n = 7, 6%), cardiovascular events (n = 3, 3%) and respiratory complications (n = 3, 3%), despite this group having a higher incidence of ASA III patients. However, wound (n = 3, 3%) and anastomotic dehiscence (n = 7, 6%) were paradoxically increased.
Quality indicators performance in each group (pre-ORCS vs ORCS)
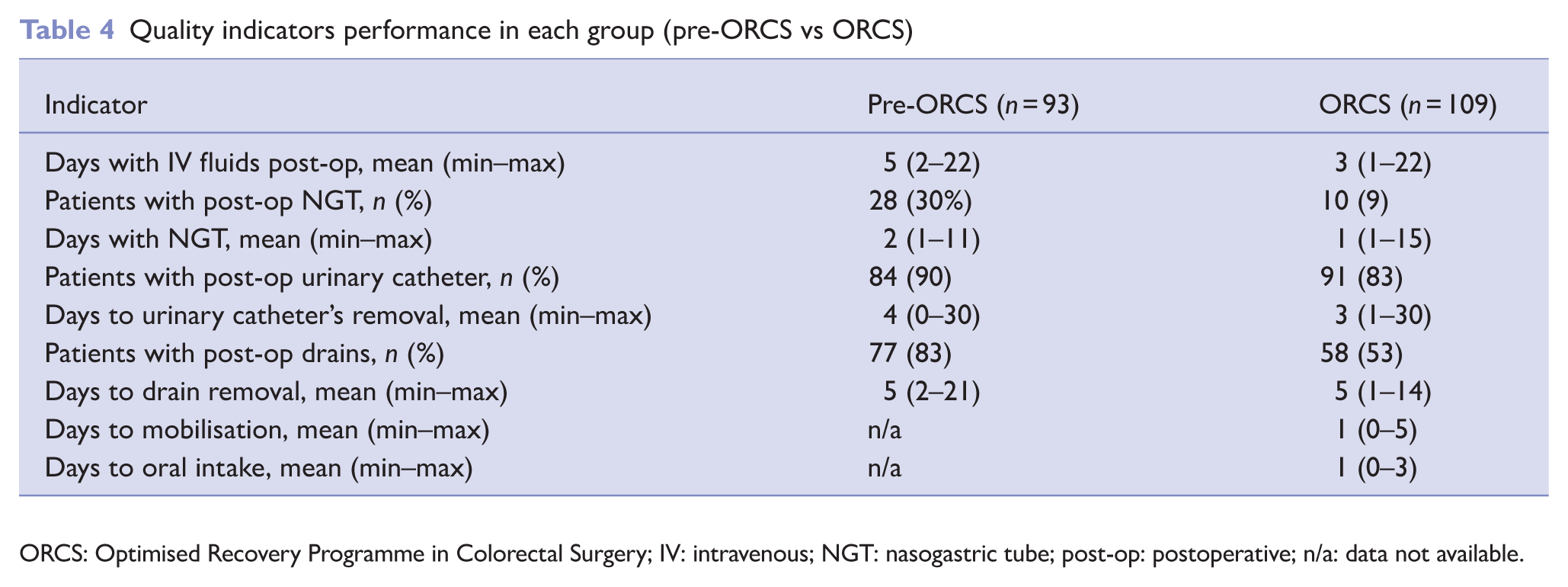
ORCS: Optimised Recovery Programme in Colorectal Surgery; IV: intravenous; NGT: nasogastric tube; post-op: postoperative; n/a: data not available.
Complications and major outcomes in each group (pre-ORCS vs ORCS)
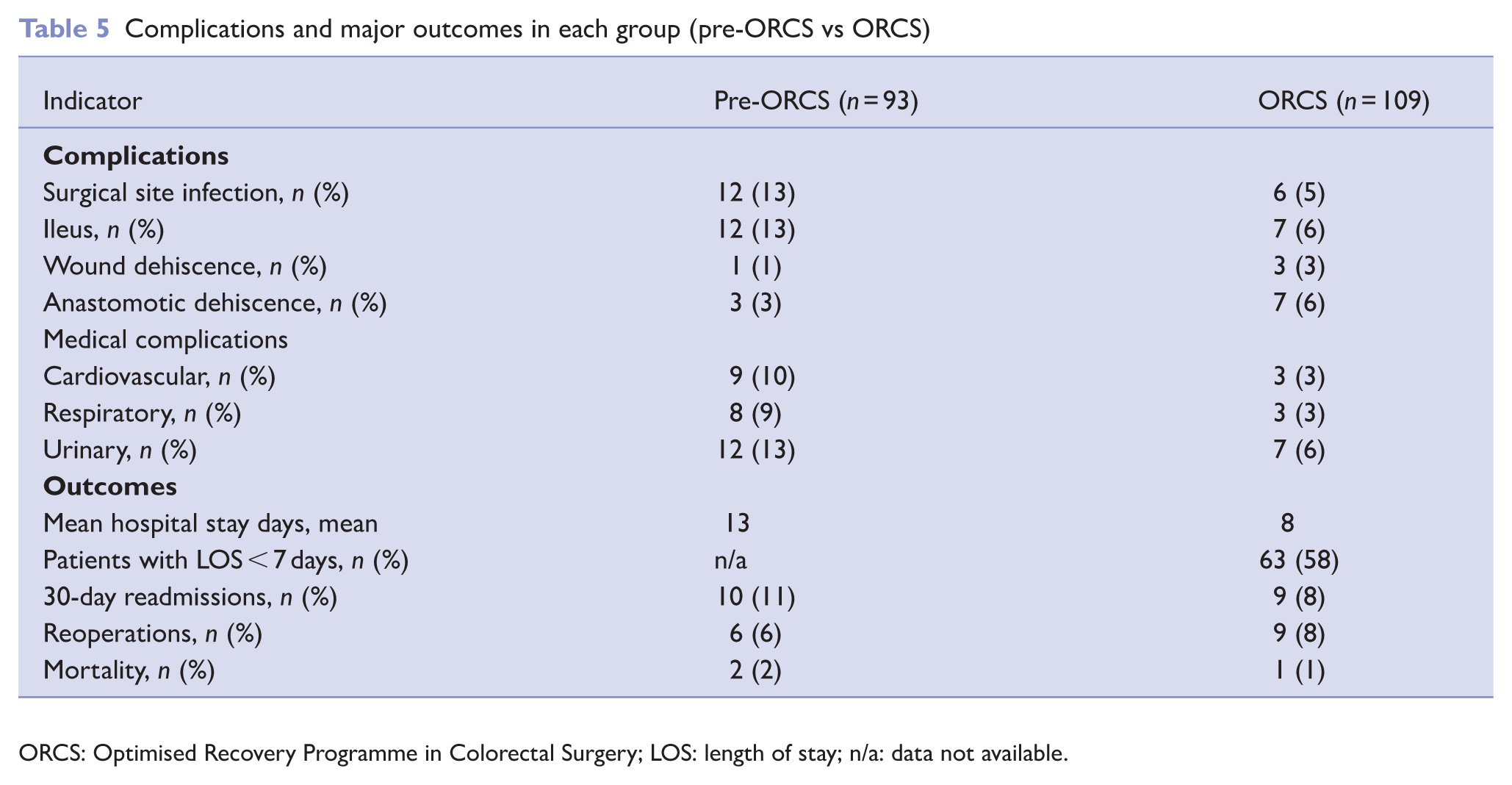
ORCS: Optimised Recovery Programme in Colorectal Surgery; LOS: length of stay; n/a: data not available.
Patients undergoing colorectal surgery within the ORCS protocol framework had a mean hospital LOS of 8 days, representing a reduction of 5 days compared to the pre-ORCS period. Post-discharge readmission rates at 30 days postoperatively decreased from 10 (11%) to 9 (8%), and a non-increase in overall mortality (2% vs. 1%) was observed.
Discussion
Key results
Following implementation of the ORCS pathway, a substantial reduction in hospital LOS was observed, with a mean decrease of 5 days compared with the pre-implementation period. Importantly, these gains were achieved without an increase in 30-day readmissions or mortality, supporting the safety of early discharge within a structured perioperative framework.
In parallel, improvements were observed across multiple perioperative process indicators, including earlier mobilisation, earlier initiation of oral intake and reduced utilisation of invasive devices such as nasogastric tubes, urinary catheters and surgical drains. Collectively, these findings suggest that the observed reductions in LOS were not driven by premature discharge but rather by more efficient and coordinated recovery pathways.
The reduction in postoperative medical complications observed in the ORCS cohort, despite a higher proportion of ASA III patients, further supports the importance of perioperative optimisation and multidisciplinary coordination in mitigating risk among medically complex surgical populations. The observed increase in laparotomic surgery translates into a greater number of complex cases with local tumour invasion, sometimes precluding video-assisted procedures, further dictating the importance of these structured and goal-directed approaches.
Interpretation
Our analysis demonstrates that structured perioperative coordination can be successfully introduced into routine clinical practice and is associated with meaningful improvements in system-level outcomes, even in a population with a high burden of comorbidity and without access to dedicated ERAS infrastructure.
Rather than reflecting the effect of isolated clinical interventions, the observed outcomes likely represent the cumulative impact of improved perioperative system organisation.
Lessons from real-world practice
Several implementation-related insights emerged from this experience. First, meaningful improvements in perioperative outcomes were achievable without formal certification or access to the official ERAS® digital platform. While such tools undoubtedly facilitate compliance monitoring and feedback, our findings suggest that substantial gains can still be realised through local leadership, professional engagement and structured communication.
Second, the multidisciplinary preoperative appointment played a central role. Beyond clinical optimisation, this encounter functioned as a unifying moment for aligning patient expectations, reinforcing shared recovery goals and fostering accountability across professional groups. This highlights the importance of early patient engagement as a catalyst for downstream perioperative behaviour.
Third, implementation was primarily driven by bottom-up initiative rather than top-down institutional mandate. Although this approach required sustained individual commitment, it also promoted local ownership and adaptability – factors that may be critical for successful implementation in resource-constrained health care systems.
Comparison with existing literature
Our findings are consistent with previous studies demonstrating reduced LOS and improved recovery following ERAS pathway implementation in colorectal surgery (Greco et al 2014, Varadhan et al 2010). However, much of the existing evidence originates from highly resourced centres or from studies supported by dedicated ERAS infrastructure.
In contrast, the present study contributes to the growing body of literature exploring pragmatic, real-world ERAS implementation, reinforcing the external validity of ERAS principles across diverse health care settings.
Strengths and limitations
This study has several limitations. Its retrospective, non-randomised design limits causal inference, and residual confounding cannot be excluded. The use of a historical control group may also introduce bias related to temporal changes in clinical practice.
In addition, formal measurement of adherence to individual ERAS elements was not systematically captured, precluding analysis of compliance–outcome relationships. Follow-up was limited to 30 days, preventing assessment of longer-term functional recovery and late complications. Finally, the economic analysis was based on estimated inpatient costs and should be interpreted as indicative rather than definitive.
Despite these limitations, the study has important strengths. It reflects routine clinical practice, includes a medically complex patient population and provides a comprehensive evaluation of perioperative processes alongside clinical outcomes. The pragmatic nature of the implementation enhances the relevance of the findings for institutions facing similar organisational and resource constraints.
Implications for future research
Future work should focus on prospective evaluation of pathway adherence, incorporation of digital monitoring tools and exploration of patient-reported outcomes to further characterise the full impact of perioperative care redesign.
Footnotes
Appendix 1
Summary of perioperative interventions included in the ORCS pathway.
| Phase of care | Key interventions |
|---|---|
| Preoperative phase | • Multidisciplinary preoperative assessment involving anaesthesiology, nursing and nutrition. • Structured patient-centred education with written information materials. • Medical optimisation of comorbidities and medication review. • Nutritional screening with NRI and dietary optimisation, including low-residue diet and supplementation when indicated. • Prehabilitation strategies: encouragement of physical activity and respiratory exercises (incentive spirometry). • Smoking cessation and alcohol abstinence counselling. • Perioperative risk stratification and discharge planning, including assessment of social support needs. • Minimisation of preoperative fasting; allowance of clear carbohydrate-rich fluids up to 2 h before anaesthesia induction. • Oral prophylactic antibiotics according to institutional protocol. • Standardised pre-emptive multimodal analgesia when not contraindicated. |
| Intraoperative phase | • Timely administration of surgical antibiotic prophylaxis (30–60 min before incision). • Active prevention of hypothermia using forced-air warming and warmed intravenous fluids. • Preferential use of total intravenous anaesthesia with depth of anaesthesia monitoring. • Neuromuscular blockade monitoring and appropriate reversal strategies. • Multimodal prevention of postoperative nausea and vomiting guided by risk stratification. • Opioid-sparing multimodal analgesia using non-opioid systemic agents and adjuvants. • Use of locoregional analgesic techniques (e.g. abdominal wall blocks, wound infiltration, epidural analgesia when indicated). • Goal-directed fluid therapy aiming for neutral fluid balance. |
| Postoperative phase | • Postanaesthesia care unit discharge based on standardised clinical criteria. • Early mobilisation and encouragement of patient autonomy from the day of surgery when feasible. • Early initiation of oral intake, progressing according to tolerance. • Discontinuation of intravenous fluids once adequate oral intake is established. • Regular assessment of pain, nausea and functional recovery. • Avoidance of routine nasogastric tube placement; early removal if used. • Daily reassessment and early removal of urinary catheters and surgical drains when clinically appropriate. • Multimodal thromboembolic prophylaxis (mechanical and pharmacological). • Standardised discharge criteria focusing on functional recovery and patient independence. • Postdischarge follow-up, including structured nursing telephone contact. |
NRI: Nutritional Risk Index.
Acknowledgements
The authors are very grateful to several contributors, namely Sérgio Zenha, Dalila Freitas, Ana Sofia Oliveira, Sofia Neves and Mihran Portugalyan (development of the programme), as well as Sofia Muller (data collection). The editing of this manuscript was assisted by artificial intelligence (ChatGPT).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical considerations
All patients provided informed consent for inclusion in the programme. Data were collected retrospectively, anonymised prior to analysis and handled in accordance with institutional data protection policies. Formal ethical committee approval was waived under local governance regulations for quality improvement activities.