
Abstract
Background:
The growing adoption of local anaesthesia in surgical practice expands procedures that can be undertaken with patients fully awake. This shift introduces both opportunities and challenges for perioperative care, as patients remain conscious, and influenced by environmental, interpersonal and sensory factors.
Aim:
To synthesise and interpret adult patients’ experiences of undergoing surgery while awake under local anaesthesia.
Methods:
A systematic qualitative literature review was conducted, drawing on peer-reviewed studies published between 2010 and 2025. An inductive analytic approach was applied. Nine studies were included.
Results:
Four overarching themes were identified: (1) the need for respectful, tailored communication; (2) the centrality of the perioperative team’s presence and cohesion; (3) experiences of exposure, vulnerability and fluctuating control; and (4) strategies employed by patients to cope with intraoperative stressors. Across studies, continuous, person-centred communication and empathetic engagement reduced anxiety and enhanced perceived safety.
Conclusions:
In awake surgery, interpersonal communication, team behaviours and the environmental context profoundly shape patients’ intraoperative experiences. Person-centred communication, ethical attentiveness and a supportive perioperative presence are essential to fostering trust, reducing distress and enabling meaningful patient involvement. Theatre nurses and Operating Department Practitioners play a pivotal role in sustaining a safe, humane environment for awake patients.
Keywords
Introduction
Demand for surgical care continues to rise, with year-on-year increases reported in both inpatient and outpatient specialist services. Advances in techniques mean procedures that once required general anaesthesia can now be undertaken under local anaesthesia, often with shorter recovery, less postoperative pain and reduced costs of care (Tu et al 2022). When local anaesthesia is used, patients remain awake and receptive to sensory and interpersonal cues. The operating theatre environment therefore has a direct influence on patients’ intraoperative experiences and subsequent recovery (Tinnfält & Nilsson 2011). To provide holistic, person-centred care, perioperative teams – particularly theatre nurses or Operating Department Practitioners (ODPs), who are essential allied health professionals working in operating theatres in the United Kingdom, specialising in anaesthetics, surgery and recovery – must be sensitive to patients’ experiences and actively create a sense of safety through technical proficiency and an empathetic, professional manner.
Background
Local anaesthesia is cost-effective and avoids adverse effects associated with general anaesthesia. It is especially advantageous for minor procedures, where patient participation may be required or where comorbidities make general anaesthesia less suitable (DeLamar 2011). Techniques that began in, for example, hand surgery are now, according to MacNeill & Mayich (2019), applied in foot and ankle surgery. Complex procedures are increasingly undertaken with patients conscious (Caddick et al 2012). While awake, patients’ attentional focus and sensitivity to environmental and verbal cues can heighten; negative impressions – including incidental comments – may exacerbate anxiety, stress and pain (Caddick et al 2012).
Anxiety in these contexts may relate to fear of pain, bodily vulnerability, loss of control and worries about diagnosis and prognosis (Tinnfält & Nilsson 2011). These factors underscore the value of a person-centred model of care, whereby decisions are made in partnership and the patient’s preferences, and life situation are considered throughout the care process (SFS 1998: 531). Theatre nurses and ODPs have a dual responsibility, to ensure technical safety – including asepsis – and to communicate effectively in support of person-centred care, a philosophy prioritising the patient’s unique needs, wishes and values (Ekman & Norberg 2020).
Several practical considerations arise in awake surgery. For example, the naming of instruments can provoke anxiety, whereas a calm atmosphere and supportive dialogue can be reassuring (Caddick et al 2012).
The surgical environment
For many, the operating theatre is unfamiliar. Patients may be asked to walk partially undressed into a bright, equipment-laden room, lie on a narrow table and overhear technical discussions among staff (Caddick et al 2012). Bright lights, limited visual fields following positioning and unfamiliar sounds contribute to discomfort (Ellingsen 2012, Tinnfält & Nilsson 2011). Masks and other barriers make communication harder, and the operating table may be adjusted without warning, compounding the sense of immobility and exposure (Tinnfält & Nilsson 2011).
Responsiveness from the theatre nurse and ODPs can foster involvement and safety (Martinsen 2012). Team dynamics and non-verbal communication also shape the patient’s emotional state, underscoring the importance of professional discourse and body language (Ellingsen 2012). Sensory impressions inform the team’s understanding of patient cues and guide supportive actions (Martinsen 2012).
Because patients can hear and infer much of what is happening, attending to their needs through ongoing explanation promotes safety (Khu et al 2022). As awake procedures become more common, theatre nurses and ODPs must adapt practices to ensure safe, effective and person-centred care informed by a deeper understanding of lived patient experience.
Aim
To investigate adult patients’ experiences of undergoing surgery while awake under local anaesthesia.
Methods
Design
A systematic literature review based on qualitative methodology and an inductive approach was conducted to address the aim. Systematic reviews seek, select, appraise and synthesise relevant literature in a structured way (Bettany-Saltikov & McSherry 2016). The qualitative focus was chosen to capture the depth and context of lived experience rather than to generalise to populations (Polit & Beck 2010). Patterns were derived inductively from the data, which mean that the researcher reads through the data and allows codes to emerge/names concepts as they emerge (Danielsson 2017, Fridlund & Mårtensson 2017). It can be described as a ‘bottom-up’ analytic strategy.
Eligibility criteria and population, exposure, outcome and type of study framework
The PEOT framework (Population, Exposure, Outcome, Type of study) guided inclusion and exclusion criteria (Bettany-Saltikov & McSherry 2016): Population, adults undergoing surgery; Exposure, awake under local anaesthesia; Outcome, patients’ perspectives; Type, qualitative studies. Original, peer-reviewed studies in English with ethical approval, published 2010–2025, were eligible. Sample size was not an exclusion criterion.
Data sources and search strategy
CINAHL and PubMed were searched as core health-science databases. Test searches identified keywords and subject headings; CINAHL Headings and PubMed MeSH were combined with free-text terms using Boolean operators OR (within blocks) and AND (between blocks). Filters were applied for year of publication and peer review. Due to low yield, the date range was extended to 2010–2025. Searches were quality-assured with librarian support and documented using a Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flow diagram (Figure 1).
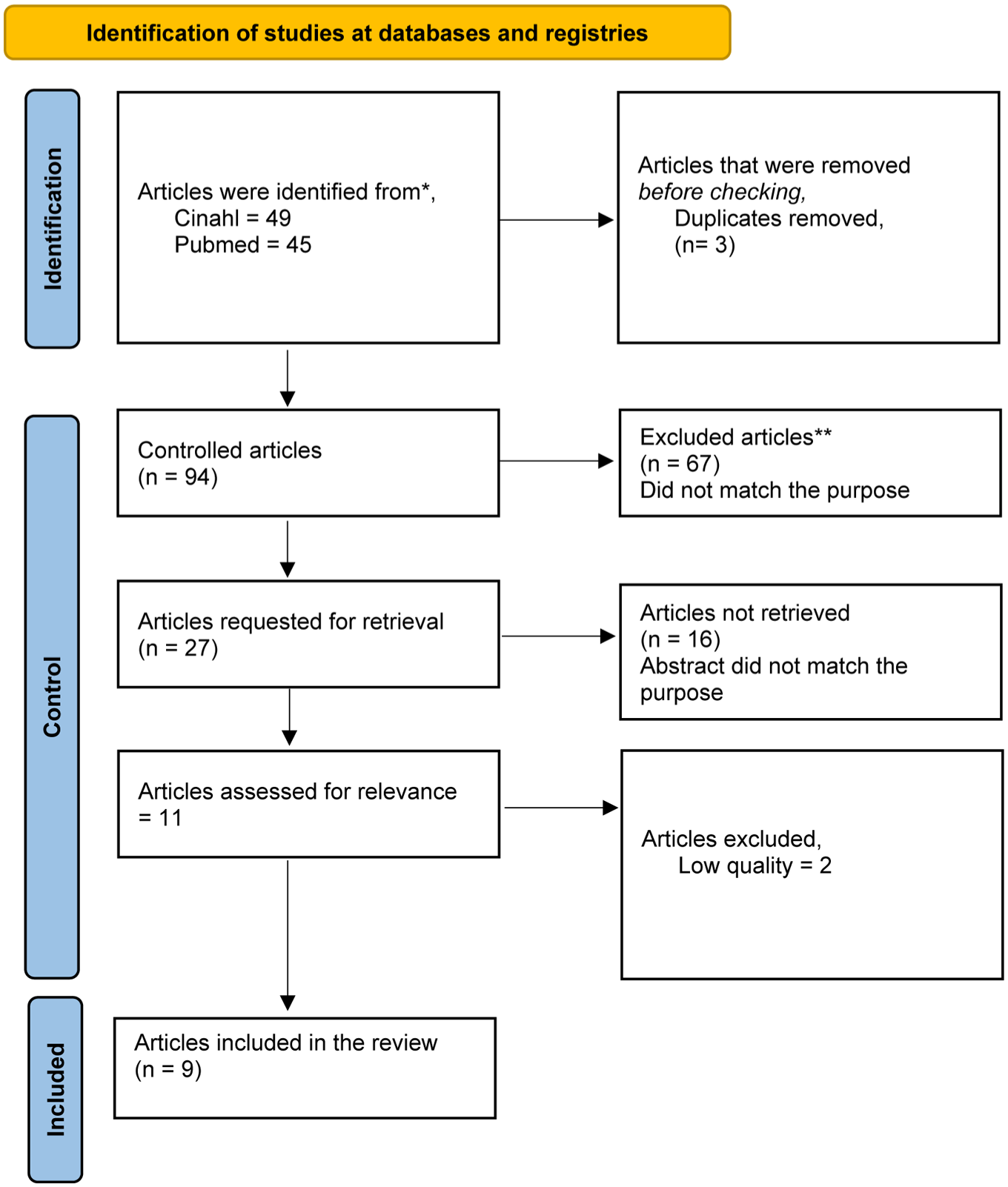
Flow chart according to PRISMA
Study selection and quality appraisal
Eligible full texts were appraised using the JBI Critical Appraisal Checklist for Qualitative Research (Lockwood et al 2015) and Bettany-Saltikov and McSherry’s (2016) review template with a 0–2 scoring system. Two studies were excluded for insufficient quality; nine were included. Mixed-methods studies were eligible if the qualitative component was methodologically sound and relevant (Polit & Beck 2021).
Data extraction and analysis
Data were extracted from result sections and organised in matrices with source and location markers. Open coding was undertaken, followed by grouping into categories and overarching themes. Categories were iteratively reviewed and consolidated. Validation was enhanced through repeated analyses over time and supervisory input. Final themes were checked against source texts, to ensure coverage and coherence, following Bettany-Saltikov and McSherry’s (2016) nine-step guidance.
Ethical considerations
This review synthesised published studies that had received ethics approval. No new data were collected. Ethical considerations focused on faithful representation, transparency and integrity (Booth et al 2019, Kjellström 2017). As a single-author review, reflexivity regarding potential bias and language limitations was maintained; systematic procedures for selection, appraisal and analysis aimed to reduce bias.
Results
Nine studies (four from Sweden, three from England, two from Canada) using semi-structured interviews (two with additional quantitative components) informed the synthesis (2010–2025). Analysis generated four themes with subthemes, summarised below.
Patients’ need for respectful communication
Patient-centred information during the procedure
Inadequate information before and during surgery increased uncertainty, anxiety and a sense of alienation (Nordblom et al 2023). Continuous, tailored updates reassured patients that the procedure was progressing as planned, although preferences for detail varied (Ericsson et al 2018, Howie et al 2016, Percy et al 2024, Wernström et al 2017).
Interprofessional communication and patient experience
Technical exchanges between staff were audible to patients and could either reassure or heighten anxiety depending on clarity and tone (Ericsson et al 2018). Positive, friendly and professional team communication fostered trust; unclear or tense exchanges exacerbated fear (Hudson et al 2015, Nordblom et al 2023, Percy et al 2024).
The importance of the care team
Trust and presence
Close, attentive presence by a team member – through eye contact, touch or non-verbal signals – reduced feelings of isolation and vulnerability (Ericsson et al 2018, Karlsson et al 2012, Percy et al 2024). Many patients placed strong trust in clinicians, particularly surgeons, which lessened anxiety (Howie et al 2016, Hudson et al 2015).
Participation and involvement
Patients valued being listened to and included in decisions; acknowledgement of emotions and symptoms strengthened their sense of participation (Karlsson et al 2012, Percy et al 2024, Wernström et al 2017).
Exposure and vulnerability in an unfamiliar environment
Balancing control and surrender
Immobility, restricted vision and surgical sounds heightened vulnerability (Ericsson et al 2018, Karlsson et al 2012). Trust in team expertise helped some patients relinquish control and feel safe; detailed, comprehensible information restored a sense of control for others (Howie et al 2016, Percy et al 2024, Wernström et al 2017).
Physical and psychological stressors
Reports of inadequate anaesthesia led to pain, sometimes unreported by patients who normalised it (Ericsson et al 2018, Hudson et al 2015). Lack of preparation amplified psychological distress, whereas clear preoperative information mitigated anxiety (Hudson et al 2015, Nordblom et al 2023). The public, high-tech environment reinforced feelings of exposure and objectification (Nordblom et al 2023).
Coping strategies during awake surgery
Creating a personal ‘bubble’
Patients commonly used attentional strategies, for example, focusing on a fixed point or listening selectively to manage unpleasant sensations and emotions, thereby sustaining a zone of control (Howie et al 2016, Nordblom et al 2023).
External stimuli
Music and headphones had mixed effects; for many, they were calming and distracting, occasionally creating positive associations; for others, they were intrusive or risked linking preferred music with negative memories (Jadavji-Mithani et al 2015, Karlsson et al 2012). Humour, prayer and other cognitive strategies were also used (Howie et al 2016, Wernström et al 2017).
Discussion
Methodological considerations
A qualitative systematic review enabled in-depth synthesis of subjective experiences, from a broader perspective (Allwood 2022, Polit & Beck 2021). The chosen method was deemed appropriate as we aimed to investigate adult patients’ experiences of undergoing surgery while awake under local anaesthesia. There is limited knowledge about adult patients’ experiences of undergoing surgery while awake under local anaesthesia. Interviews were considered to reveal the perspectives of few patients in a single hospital. Risks of single-author bias and language limitations were addressed through transparent methods, established appraisal tools and supervisory triangulation (Bettany-Saltikov & McSherry 2016, Lockwood et al 2015). The inclusion of studies involving regional anaesthesia or intermittent sedation is a limitation given the focus on local anaesthesia; however, awake experiences remained central and analytically relevant. The geographic spread (Sweden, England, Canada) may limit transferability beyond Western settings, although comprehensive searching and librarian input reduce the risk of missed studies.
Interpretation and implications
Lack of information and disconnected team talk can intensify uncertainty and anxiety. An explicitly person-centred communicative environment – combining continuous updates, acknowledgement of feelings and respectful non-verbal presence – supports autonomy and safety (Dahlberg & Segersten 2010, Sandman & Kjellström 2016). In the high-tech theatre, patients’ risk being reduced to objects; empathic engagement and small gestures (eye contact, hand-holding) counteract objectification and build trust (Bäckström 2012, DeLamar 2011, Karlsson et al 2013).
Coping strategies should be supported and individualised. Music or distraction aids many but not all; offering choice avoids one-size-fits-all interventions and aligns with equitable, person-centred care (Dahlborg et al 2022, Trängeberg & Stomberg 2013).
Societal and service implications
As indications for local anaesthesia expand, more patients will be awake during surgery (Caddick et al 2012, Tu et al 2022). Potential system benefits include shorter recovery and lower costs; however, anaesthetic choice must remain responsive to patient anxiety, pain tolerance and procedural complexity (Bowen et al 2023, DeLamar 2011).
Conclusion
Patients’ experiences of awake surgery are shaped by communication, team behaviours and the unfamiliar, technologically dense environment. Continuous, tailored information and empathic presence reduce stress, strengthen control and promote autonomy. Seeing and engaging the patient as a person – not merely a surgical site – is fundamental to ethically sustainable, person-centred perioperative care.
Future research
Prospective qualitative studies could explore how structured, nurse-led preoperative encounters and intraoperative communication protocols affect anxiety, perceived control and recovery among awake patients. Implementation work is also warranted to embed person-centred practices in theatre workflows, including meeting the theatre nurse or ODPs preoperatively to establish rapport and tailor supportive strategies.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.