
Abstract
Objective:
The objective is to compare the effectiveness of verbal instructions alone versus verbal instructions combined with visual guidance in achieving optimal patient positioning for spinal anaesthesia.
Methods:
A comparative observational study was conducted among 70 adult patients undergoing elective surgery under spinal anaesthesia in the lateral decubitus position. Patients were divided into two groups: Group A received verbal instructions alone, while Group B received verbal instructions with visual guidance. Outcomes assessed included time taken for positioning, time for needle placement, number of attempts, first-pass success, and anaesthetist satisfaction.
Results:
Visual guidance improved patient positioning, reduced procedure time, decreased number of attempts, and increased first-pass success. Anaesthetist satisfaction was higher in the visual guidance group.
Conclusion:
Visual guidance is a simple and effective adjunct to verbal instructions, improving positioning and procedural efficiency in spinal anaesthesia.
Introduction
Spinal anaesthesia (subarachnoid block, SAB) remains a widely used technique due to its effectiveness and safety profile; however, procedural success depends on multiple technical and patient-related factors (Ledesma et al 2024, Paliwal et al 2024). The success or failure of SAB depends on accurate identification of anatomical landmarks and proper needle placement in the subarachnoid space (Miller & Pardo 2011). The procedure is commonly performed using landmark-based techniques, and the quality of these landmarks is a key determinant of procedural difficulty (de Oliveira Filho et al 2002). Factors such as age, gender, body mass index, and spinal abnormalities are known to be associated with difficulty in performing SAB (Atallah et al 2004).
Multiple attempts at needle insertion may lead to patient discomfort and dissatisfaction, and in some cases, refusal to undergo the procedure. In addition, patient positioning plays a crucial role in the success of SAB (Atallah et al 2004, de Oliveira Filho et al 2002, Rhee et al 2010). The procedure can be performed in sitting, lateral, and, rarely, prone positions. The lateral position is often preferred in fragile, unwell, or sedated patients, as it is more comfortable and may facilitate better spread of local anaesthetic, resulting in improved sensory blockade (Inglis et al 1995, Sharma et al 2022).
In addition to optimising patient positioning, several techniques have been explored to improve the success of SAB, including preprocedural ultrasound imaging, paraspinous approaches, and real-time ultrasound-guided techniques, particularly in patients with difficult anatomy (Poots & Chin 2024).
Despite these advances, achieving optimal positioning still requires active patient cooperation. Patients are typically guided using verbal instructions; however, misinterpretation of these instructions can make it difficult to achieve the desired posture, leading to delays and increased procedural difficulty (de Oliveira Filho et al 2002, Gurunathan et al 2018).
The use of visual guidance may improve patient understanding and facilitate correct positioning. Visual aids simplify complex instructions, enhance communication, and reduce misinterpretation, thereby improving patient cooperation and procedural efficiency (Ansari et al 2024, Hegde et al 2024, Hoonakker et al 2023, Van Beusekom et al 2015).
Therefore, this study aimed to compare the effectiveness of verbal instructions alone with verbal instructions combined with visual guidance in achieving optimal patient positioning for SAB. The primary outcome was the time taken for successful needle placement. Secondary outcomes included first-pass success, number of attempts, need for assistance, needle redirections, and anaesthetist satisfaction.
Methods
This comparative observational study was conducted in the operating theatre complex of a tertiary care teaching hospital from May 2023 to May 2024 after obtaining approval from the Institutional Ethics Committee (Approval No: YEC-1/2023/132) and registration with the Clinical Trials Registry of India (CTRI/2023/08/056164). The study was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants prior to inclusion in the study.
A total of 70 patients were assessed for eligibility during the study period. All patients met the inclusion criteria and none fulfilled the exclusion criteria; therefore, all 70 patients were included in the final analysis and allocated into two groups (Figure 1).
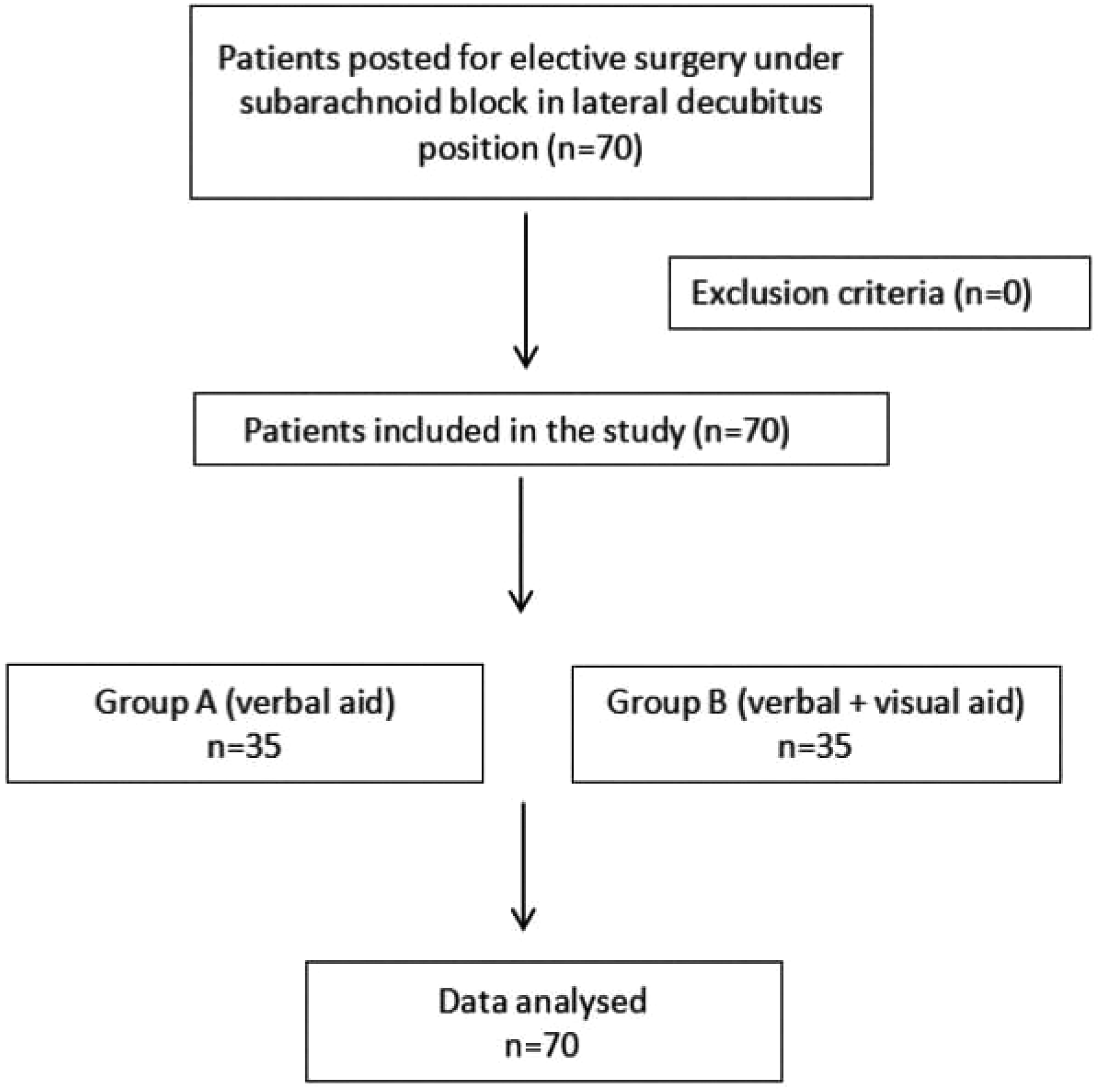
CONSORT flow diagram of patient enrolment and allocation
Preanaesthetic evaluation was carried out for all patients prior to surgery, including routine investigations and spinal examination. On arrival in the operating theatre, standard monitoring including pulse oximetry, non-invasive blood pressure, and electrocardiography was applied, and intravenous access was secured.
Patients were allocated into two groups using a consecutive sampling method based on the time of admission to the operating theatre. In Group A, patients were instructed verbally by the anaesthesia technician to assume the lateral decubitus position, including flexion of the neck, hips, and knees to achieve a foetal posture. In Group B, in addition to verbal instructions, patients were shown a visual image demonstrating the correct positioning in the lateral decubitus position (Figures 2 and 3). The visual aid depicted optimal flexion of the neck, back, and hips and was shown immediately prior to positioning. Patients were guided to replicate the posture demonstrated in the image. All spinal anaesthesia procedures were performed by multiple anaesthetists with comparable experience in spinal anaesthesia, following a standardised protocol to minimise inter-operator variability. The anaesthetist performing the procedure was not blinded to group allocation.

Illustration of lateral decubitus position used for visual guidance (Group B)
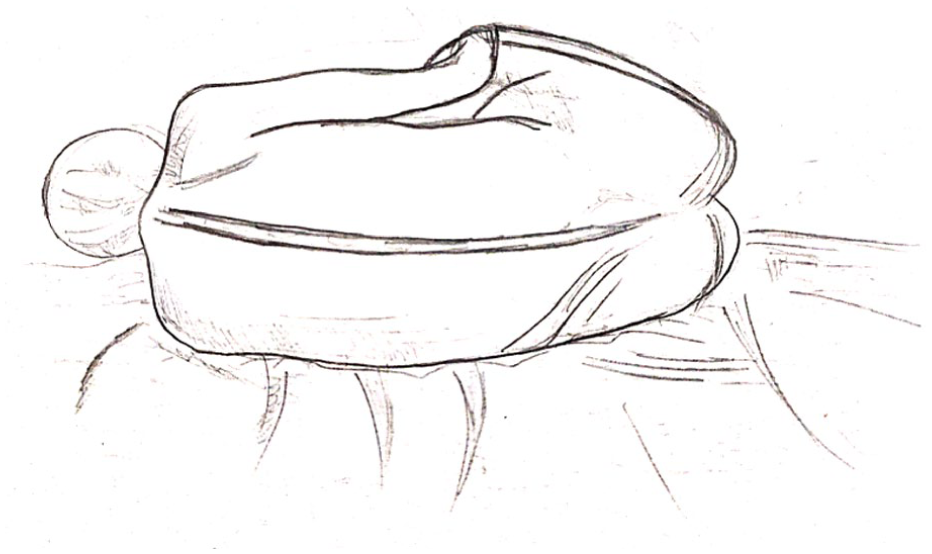
Posterior view of lateral decubitus position
Under strict aseptic precautions, the anaesthetist prepared the patient for the procedure. A timer was initiated at the start of positioning instructions. Patients were guided into position by an anaesthesia technician according to group allocation. Once the desired position was achieved, the anaesthetist performed the SAB.
The following parameters were recorded by the principal investigator:
Time taken for needle placement (defined as the interval from initiation of positioning instructions to successful injection of the spinal drug into the subarachnoid space).
Time taken to achieve optimal positioning (defined as the interval from initiation of positioning instructions to achievement of the desired lateral decubitus position, as assessed by the anaesthetist).
Number of attempts (defined as the number of skin punctures).
First-pass success rate (defined as successful needle placement on the first attempt).
Number of needle redirections.
Number of personnel required to assist the procedure.
Anaesthetist satisfaction score assessed on a numerical scale from 1 (very unsatisfied) to 5 (very satisfied).
Statistical analysis
The collected data were summarised using SPSS version 23 software. Continuous variables were expressed as mean ± standard deviation, and categorical variables as frequency and percentage. The independent t-test or Mann–Whitney U test was used to compare the two groups, as appropriate. A p-value of <0.05 was considered statistically significant. For normally distributed continuous variables, 95% confidence intervals were calculated and reported along with mean values to describe the precision of estimates. For non-normally distributed variables, data were presented as median with interquartile range and analysed using the Mann–Whitney U test.
Result
Seventy patients were included in the study, with 35 patients allocated to Group A (verbal instructions) and 35 to Group B (verbal instructions combined with visual guidance). The study population consisted of patients undergoing elective lower abdominal and lower limb surgeries. The mean age in Group A was 48.77 ± 7.86 years and in Group B was 45.14 ± 11.22 years. The gender distribution was comparable between the groups, with 8 females (22.9%) and 27 males (77.1%) in Group A, and 9 females (25.7%) and 26 males (74.3%) in Group B (Table 1).
Comparison of demographic variables between two groups
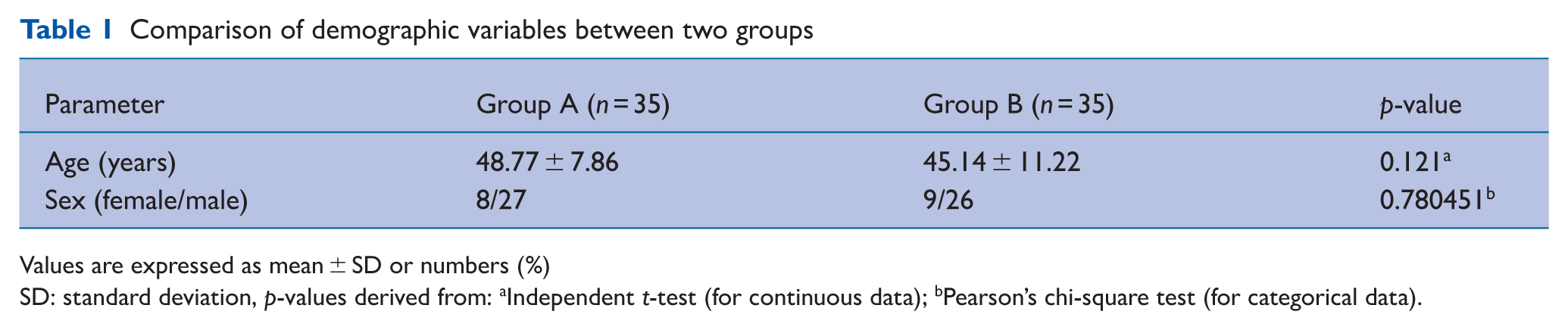
Values are expressed as mean ± SD or numbers (%)
SD: standard deviation, p-values derived from: aIndependent t-test (for continuous data); bPearson’s chi-square test (for categorical data).
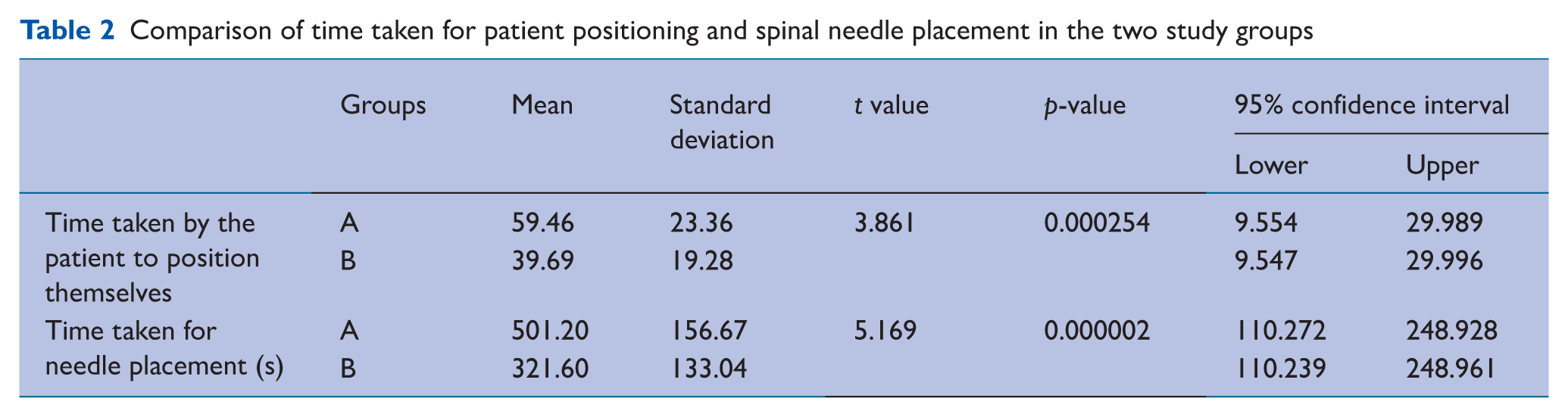
The time required for patients to assume the required position was significantly greater in Group A (59 s) than in Group B (40 s) (p = 0.000254). Similarly, the mean time taken for successful needle placement was significantly longer in Group A (501 ± 156.67 s) compared to Group B (321 ± 133.04 s) (p = 0.000002) (Table 2, Figure 4).
Comparison of time taken for patient positioning and spinal needle placement in the two study groups
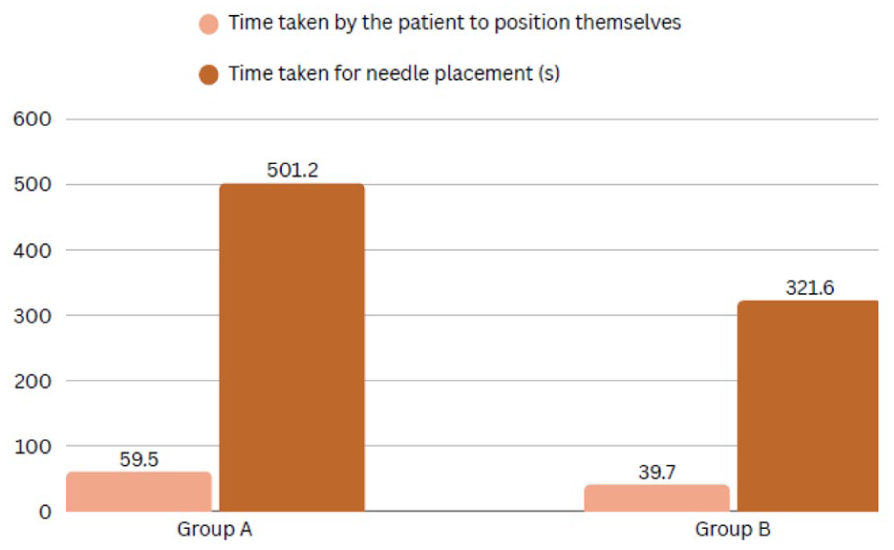
Comparison of time taken for patient positioning and needle placement between the two groups
First-pass success was achieved in 60% of patients in Group B compared to 17.1% in Group A, demonstrating a statistically significant difference (p = 0.0005). The median number of attempts required for successful needle placement was higher in Group A (2 [IQR 2–3]) compared to Group B (1 [IQR 1–2]) (p = 0.000262) (Table 3, Figure 5).
Comparison of secondary outcomes between the two groups
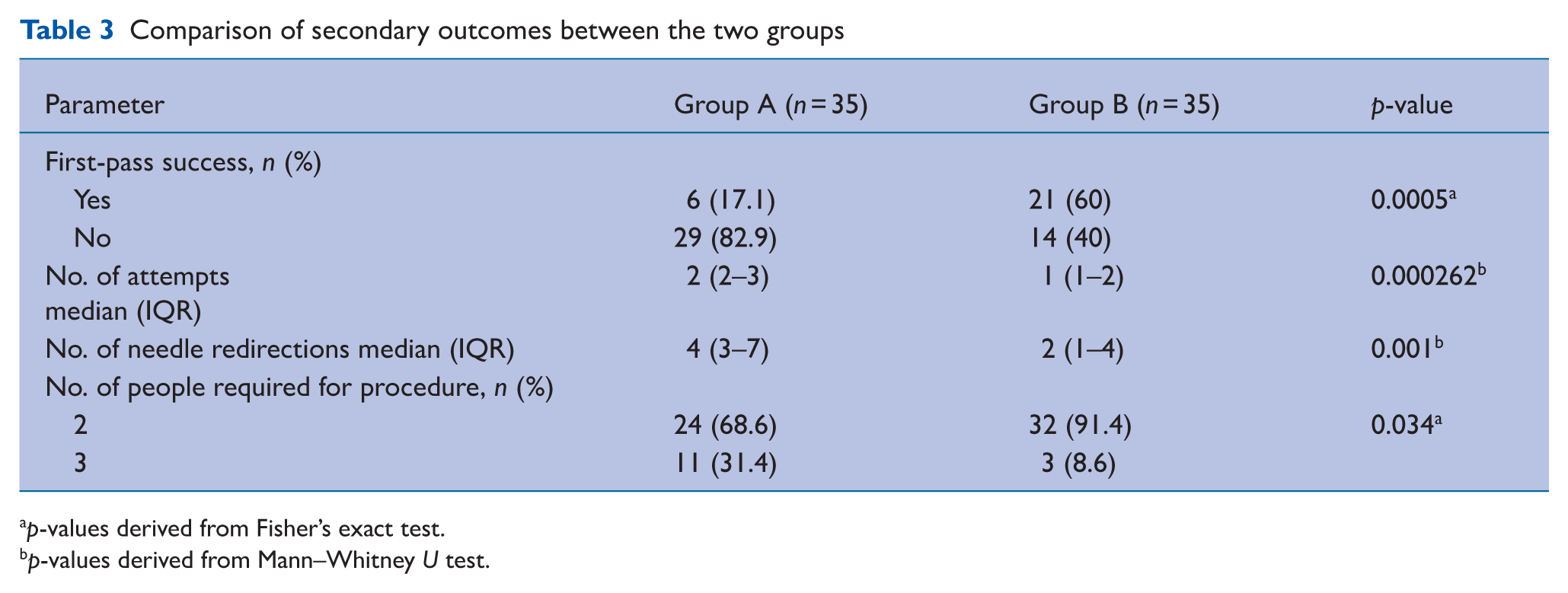
p-values derived from Fisher’s exact test.
p-values derived from Mann–Whitney U test.
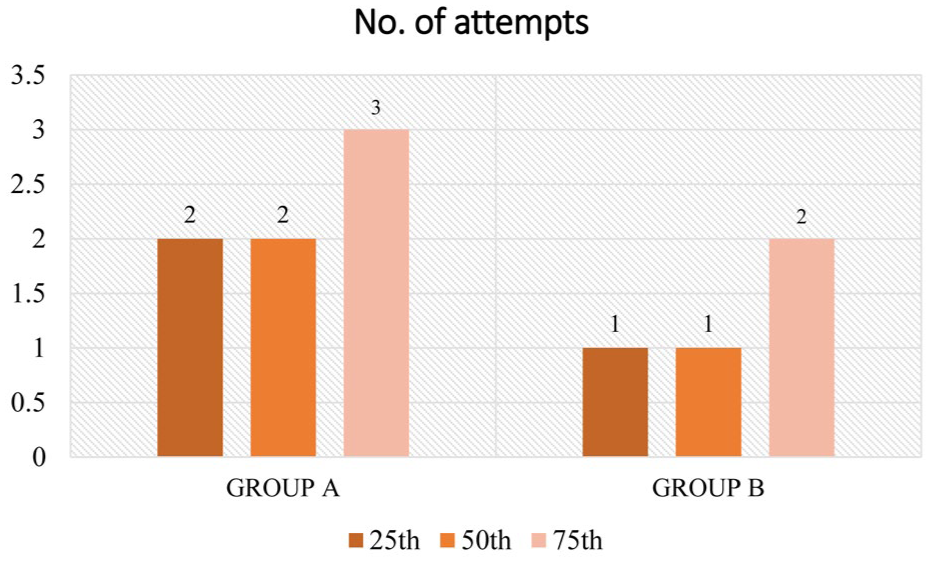
Comparison of number of attempts for spinal needle placement between the two study groups
The median number of needle redirections was also significantly greater in Group A (4 [IQR 3–7]) than in Group B (2 [IQR 1–4]) (p = 0.001) (Table 3, Figure 6).
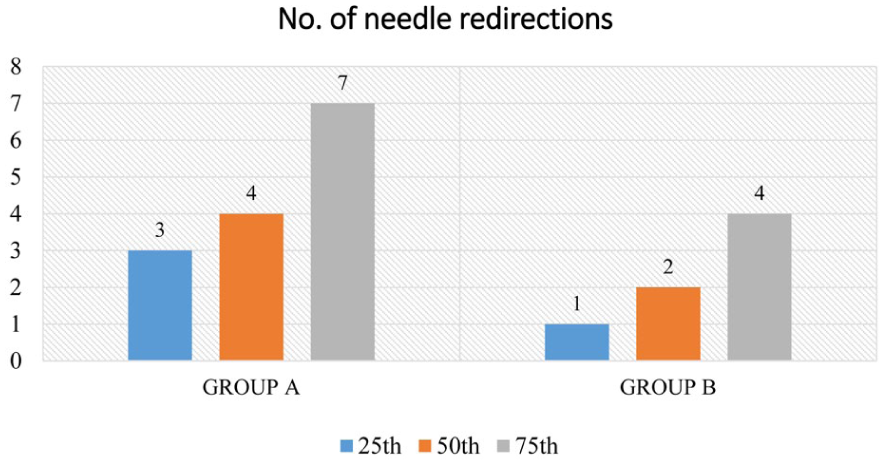
Comparison of number of needle redirections between the two study groups
Regarding personnel requirement, 68.6% of patients in Group A required two personnel and 31.4% required three personnel to complete the procedure. In contrast, 91.4% of patients in Group B required two personnel and only 8.6% required three personnel (p = 0.034) (Table 3).
Anaesthetist satisfaction scores (0–5 scale) were significantly higher in Group B, with a median score of 4 compared to 3 in Group A (p = 0.00031) (Figure 7).
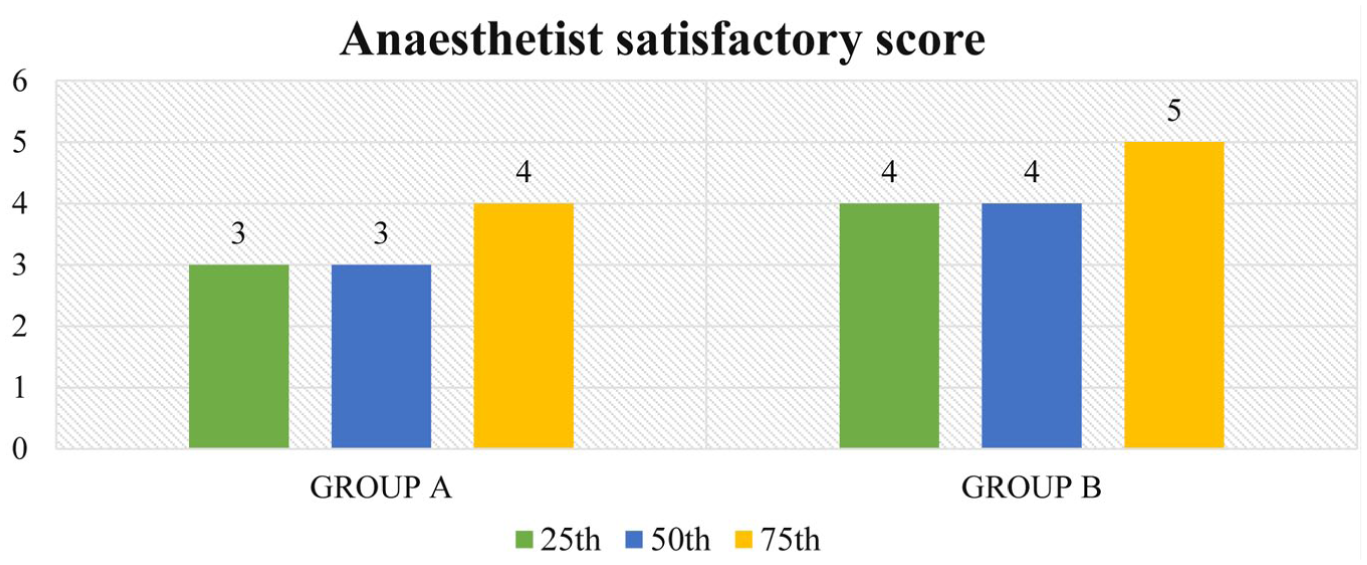
Comparison of anaesthetist satisfaction scores between the two study groups
Discussion
Images can enhance understanding by visually illustrating the relationships between concepts; as a result, they can significantly influence the effectiveness of instructions, ensuring that the intended message or guidance is more readily comprehended and followed (Van Beusekom et al 2015). Visual aids have also been shown to improve patient comprehension, reduce misinterpretation, and enhance cooperation during clinical procedures. Recent studies have demonstrated that visual guidance can facilitate better communication and improve procedural outcomes in clinical settings (Hegde et al 2024, Mudigere et al 2025).
The data presented in this study compare the performance of two groups (Group A and Group B), and significant differences were observed between the groups across all variables studied. A major difference was noted in the time taken for needle placement, as well as the time taken by the patient to position themselves, with Group A taking significantly longer compared to Group B. Our findings are consistent with previous studies, including those by Ansari et al (2024), Gurunathan et al (2018), Hegde et al (2024) and Mudigere et al (2025), which demonstrated that the use of visual aids improves patient positioning and reduces procedural difficulty.
In addition to patient positioning strategies, several techniques have been explored to improve the success of neuraxial blocks, including preprocedural ultrasound imaging, paraspinous approaches, and real-time ultrasound-guided techniques, particularly in patients with difficult anatomy (Poots & Chin 2024). While these methods improve accuracy, they require additional equipment and technical expertise. In contrast, the use of simple visual aids, as demonstrated in this study, offers a simple, cost-effective, and easily implementable alternative to improve procedural success.
In previous studies determining factors associated with difficult spinal or epidural block, patient positioning has been identified as an important determinant of successful neuraxial block (Kim et al 2011, Ružman et al 2014). First-pass success has been found to be strongly associated with the adequacy of patient positioning, quality of anatomical landmarks, and good palpability of the interspinous space (Chien et al 2003, Kim et al 2011). In our study, the first-pass success rate was significantly higher in Group B (60%) compared to Group A (17.1%).
Multiple attempts at needle insertion may result in patient discomfort, increased risk of complications such as spinal haematoma and postdural puncture headache, and potential neural injury (Atallah et al 2004, Atashkhoei et al 2019). In our study, the median number of attempts required to complete the procedure was significantly lower in Group B compared to Group A, indicating improved procedural success with the use of visual aids.
Effective flexion of the spine is known to reduce the requirement for needle redirections and improve ease of access to the subarachnoid space (Biswas et al 2012). In the present study, patients in Group B required fewer needle redirections compared to Group A, further supporting the effectiveness of visual guidance in achieving optimal positioning.
The number of attempts and procedural difficulty have also been shown to influence both patient satisfaction and anaesthetist satisfaction (Rhee et al 2010). In our study, anaesthetist satisfaction was significantly higher in Group B, likely due to reduced procedure time, fewer attempts, and higher first-pass success rates.
Our study has several strengths. To the best of our knowledge, this is one of the few studies to evaluate the effectiveness of a simple and easily implementable intervention, namely visual guidance in addition to verbal instructions, for patient positioning during spinal anaesthesia in the lateral decubitus position. Unlike previous studies (Gurunathan et al 2018), additional parameters such as time taken for patient positioning and number of needle redirections were also evaluated.
Limitations
This study has certain limitations. Although body mass index and patient weight were not formally assessed, the inclusion of only ASA physical status I patients may have limited variability in patient characteristics, thereby excluding patients with obesity or significant comorbidities. This may affect the generalisability of the findings to more complex patient populations.
In addition, several potential confounding factors such as needle type and gauge, approach (midline or paramedian), and the influence of anaesthetist experience were not formally analysed as study variables. Operator experience has been reported to influence the success of neuraxial block placement, although findings in the literature remain variable (Baheti & Laheri 2021, Kim et al 2011, Ružman et al 2014). However, procedures in the present study were performed by anaesthetists with comparable experience following a standardised protocol, which may have reduced inter-operator variability.
The study was conducted at a single centre with a relatively small sample size, which may limit external validity. Furthermore, the anaesthetist performing the procedure was not blinded to group allocation, which may have introduced performance bias.
In addition, the quality of anatomical landmarks was not assessed, and study outcomes were primarily based on procedural time and technical parameters. Patient-related factors such as educational status and literacy level were also not formally evaluated, which may have influenced interpretation of verbal and visual instructions, although the visual aid was designed to be simple and easily comprehensible.
Finally, the study population consisted of relatively younger patients (⩽60 years), which may limit the applicability of the findings to elderly patients who may differ in anatomical characteristics, cooperation, and physical flexibility.
Conclusion
Visual guidance of the lateral position, when combined with verbal instructions, improves patient positioning for spinal anaesthesia, enhances procedural efficiency, reduces the number of attempts, and increases anaesthetist satisfaction. This simple and practical approach can be easily incorporated into routine clinical practice.
Further multicentre studies with larger and more diverse patient populations, including individuals with varying ASA physical status and body habitus, are required to improve the generalisability of these findings. Future research could also evaluate the effectiveness of different types of visual aids, such as video-based guidance, and assess patient preferences for instructional methods.
Footnotes
Acknowledgements
The authors express their gratitude to the participants and staff who contributed to this study. No external writing or editorial assistance was received. Artificial intelligence tools were used only for language refinement and formatting, with full responsibility of content retained by the authors.
Author contributions
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
Ethical approval was obtained from Yenepoya Ethics Committee (Yenepoya Medical College Hospital).
Consent to participate
Written informed consent was obtained from all participants.
Consent for publication
Not applicable.
Data availability
Data is available from the corresponding author on reasonable request.