
Abstract
Current surgical literature on wound healing often excludes immunosuppressed individuals, such as those with HIV, due to their clinical complexity. Underlying disease processes can negatively influence perioperative outcomes through prolonged wound healing and increased infection risk. This review summarises factors that influence wound healing in patients with HIV undergoing orthopaedic surgery and highlights literature gaps in HIV-specific outcomes that inform intervention timing, duration, and surveillance.
Introduction
In 2021, the global prevalence of human immunodeficiency virus (HIV) was 40 million (Carter et al 2024). Antiretroviral therapy (ART) enables patients to achieve undetectable viral loads and longer life expectancies, making them susceptible to common ageing issues, such as decreased bone mineral density (BMD) (Biver 2022). Unfortunately, people living with HIV (PLWH) experience fragility fractures 10 years earlier than the general population, with an increased risk of 35%–68% (Biver 2022). HIV-related BMD changes can vary based on treatment status and length, but the extent of the interplay of these factors remains unclear. BMD significantly declines during the first 2 years of initiating any ART regimen due to HIV-infected lymphocytes and macrophages releasing receptor activator of nuclear factor kappa-B ligand (RANK-L), which signals increased osteoclast activity and promotes bone breakdown (Biver 2022). Long-term ART use demonstrates BMD improvement, which may be from viral suppression that reduces RANK-L led osteoclastic recruitment, slowing down the rate of bone loss (Biver 2022). However, the mechanisms are not fully understood.
With increased fracture risk, PLWH may require orthopaedic interventions. However, surgical literature is limited on wound healing outcomes for PLWH. Hence, exploring this intersection is pivotal for ensuring equitable care in a vulnerable patient population. This review summarises literature regarding physiological and social factors that may impact patients with HIV undergoing orthopaedic surgery and identifies gaps in evidence related to optimising postoperative healing.
Wound healing overview
Wound healing is a multi-phase physiological process that occurs following tissue injury, comprising four overlapping phases: (1) haemostasis, (2) inflammation, (3) proliferation, and (4) remodelling (Ozgok Kangal & Kopitnik 2025). Within minutes, haemostasis begins with locally damaged blood vessels vasoconstricting to prevent further blood loss. The inflammatory response is initiated, releasing cytokines, such as interleukin-1 (IL-1), interleukin-6 (IL-6), and interleukin-8 (IL-8) that promote platelet activation and aggregation (Bester & Pretorius 2016). A fibrin mesh is formed and later replaced by a permanent clot, while platelets continue to release cytokines recruiting neutrophils and macrophages through chemotaxis (Mahmoud et al 2024, Ridiandries et al 2018).
Subsequently, neutrophils and macrophages clear debris and bacteria, triggering inflammation (Cialdai et al 2022). Fibroblasts supported by platelet-derived growth factor (PDGF), fibroblast growth factor (FGF), and transforming growth factor-beta (TGF-β) promote angiogenesis and extracellular matrix synthesis (Cialdai et al 2022, Talbott et al 2022). As the fibroblasts synthesise new tissue, endothelial cells contribute to vessel repair. New blood vessels provide oxygen and nutrients to support local remodelling efforts to restore skin integrity (Velnar & Gradisnik 2018). The coordinated activation of these cellular components and inflammatory mediators drives wound healing processes.
Pathophysiology of impaired wound healing in HIV
Immune dysregulation
HIV delays wound healing by infecting and depleting CD4+ T cells and exhausting host cell machinery. Enhanced metabolic demand from facilitating viral replication increases the workload of host cell endoplasmic reticulum and mitochondria, leading to decreased production of proteins and lipids essential for tissue repair (Gerg & Dobrovolny 2025, Sevilya et al 2018). Chronic inflammation caused by persistent viral presence may reduce the transition of macrophages from the M1 (pro-inflammatory) state to the M2 (anti-inflammatory) state (Neff et al 2020). As a result, pro-inflammatory cytokines such as IL-6 and TNF-alpha are secreted in abundance and impair the timely recruitment and function of T-regulatory cells and pro-angiogenic monocytes critical to the later phases of wound healing (Figure 1). Cumulatively, these effects create a highly inflammatory microenvironment that may delay wound closure, fracture consolidation, and graft integration (Lombardi et al 2024, Mahmoud et al 2024, Masyuko et al 2020, Schilrreff & Alexiev 2022).
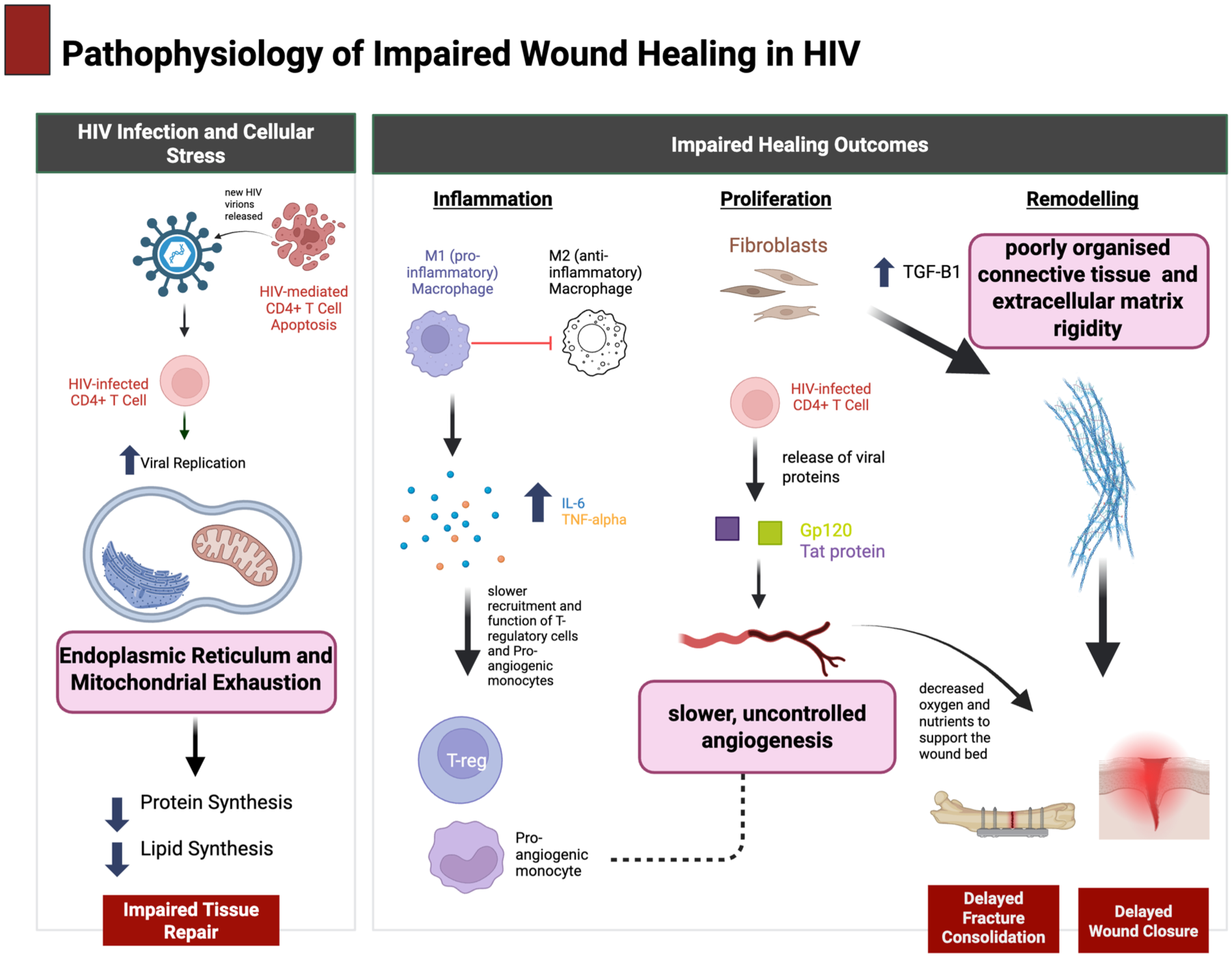
Pathophysiology of impaired wound healing in HIV created in BioRender (Hunt 2026; https://BioRender.com/s0xn1ec)
Angiogenesis
Angiogenesis is integral to supplying the wound with nutrients during the proliferative phase. Even with ART use, endothelial dysfunction persists as the virus may reduce the bioavailability of vascular endothelial growth factor (VEGF) signalling through downregulation of VEGFR-2 and sequestration of soluble vascular endothelial growth factor receptor-1 (sVEGFR-1) (Lee et al 2025, van der Mescht et al 2025). Viral components, such as Trans-Activator of Transcription (Tat) proteins and glycoprotein 120 (Gp120), are secreted from HIV-infected cells and may contribute to aberrant endothelial growth at the wound site. Specifically, Tat proteins mimic VEGF and bind to endothelial cells promoting uncontrolled angiogenesis, while Gp120 directly induces endothelial cell apoptosis and alters the expression of adhesion molecules (Anand et al 2018, Cafaro et al 2020). Cumulatively, these effects limit oxygen and nutrient delivery at the wound site.
Fibroblast and collagen impairment
At normal levels, transforming growth factor-beta-1(TGF-β1) supports wound healing through regulation of fibroblasts and matrix deposition; however, when chronically elevated, as observed in PLWH, TGF-β1 promotes excessive matrix deposition and rigidity (Maina et al 2016, Marts et al 2019). Concurrently, the activity of enzymes involved in tissue remodelling, such as matrix metalloproteinases and their inhibitors, are dysregulated in PLWH, leading to connective tissue fibrosis (Diaz et al 2011). Altogether, these alterations may compromise the integrity of surgical wounds, contributing to the formation of weak and poorly organised tissue susceptible to complications such as wound dehiscence, infection, and disordered scarring.
Antiretroviral therapy
Antiretroviral therapy (ART) improves overall health by disrupting the HIV life cycle and increasing the CD4+ T cell count (Love et al 2024, Zhang & Ruan 2023). Nevertheless, ARTs are not created equally. Protease inhibitors are associated with vascular dysfunction, dyslipidaemia, impaired fibroblast collagen synthesis, and osteoblast inhibition (Bruder-Nascimento et al 2020, Kalra et al 2023, Szoka et al 2019). These effects increase the risk of nutrient deprivation, hypoxia, and poor tissue quality at the site of wounds. In addition, Tenofovir, a nucleoside reverse transcriptase inhibitor (NRTI), increases kidney excretion of phosphate, which may result in osteomalacia and decreased bone mineralisation (Joseph et al 2023). These findings indicate that ART decreases, but does not eliminate complications, including delayed fracture healing and recovery.
Clinical trends in orthopaedic surgery for PLWH
Osteonecrosis of the femoral head is increasingly prevalent among PLWH within the past 20 years driven by immune dysregulation and protease inhibitor use (Du et al 2024, Lima et al 2009, Yang et al 2025). Compared with the general population, where the annual risk of symptomatic osteonecrosis ranges from 0.010% to 0.135%, people living with HIV have an estimated 100-fold increase in reported symptomatic osteonecrosis development (Diallo et al 2021, Parsonage et al 2005, Yang et al 2025). Studies have shown that early magnetic resonance imaging (MRI) is pivotal in detection and intervention and may optimise joint survival and femoral head integrity (Lima et al 2009). Early fractures may benefit from minimally invasive techniques such as percutaneous core decompression to reduce infection risk (Lin et al 2020). Fracture healing outcomes are heterogeneous but often demonstrate prolonged healing with low CD4+ counts, poor nutrition, or protease inhibitor use (Ma et al 2020). However, consistent ART demonstrates healing outcomes comparable to patients that are HIV-negative (Ma et al 2020). ART regimens with adverse effects on bone, like protease inhibitors, should be reviewed in collaboration with HIV specialists, considering if benefits outweigh risks.
Total joint arthroplasty outcomes have improved in the highly active antiretroviral therapy (HAART) era to mirror infection rates of individuals that are HIV-negative, although some population-based studies indicate longer hospital stays in PLWH (Boylan et al 2015, Jacob et al 2022). Additional risk factors, such as intravenous drug use, increase the risk of a periprosthetic joint infection (PJI) (Jacob et al 2022, Ma et al 2020, Parvizi et al 2006). Individualised risk stratification and early identification are paramount to reduce PJI risk, such as microbiologist-guided antibiotic coverage and duration, using incisional negative pressure wound therapy (NWPT), and increasing wound surveillance.
Orthopaedic considerations to support wound healing in PLWH
Current orthopaedic strategies that prioritise augmenting bone healing have similar principles for PLWH and seronegative patients. Exposed bone necessitates prompt debridement and soft-tissue coverage between 3 and 7 days after injury to reduce infection and flap failure; delayed coverage increases complications even when NPWT is used (Coles 2020). Fasciocutaneous and muscle flaps can achieve similar bone healing or infection rates compared to seronegative cohorts, though fasciocutaneous flaps may minimise donor morbidity (Coles 2020).
NPWT is a wound healing adjunct used to reduce bacterial load and dead space oedema, while increasing blood flow, and granulation tissue formation (Wang et al 2019). Several trauma meta-analyses show decreased deep surgical site infection rates with NPWT and reduced wound dehiscence in open fractures compared with conventional dressings (Grant-Freemantle et al 2020, Wang et al 2019). However, these results do not explicitly delineate outcomes for PLWH, creating uncertainty in appropriate treatment duration.
Mechanical stabilisation from bone grafting can be essential for restoring structural support. For larger fractures in patients with giant cell tumours, bone grafts provide osteoconduction and osteoinduction properties to improve function and reduce the risk of amputation (Xu et al 2021). Although derived from a separate immunocompromised group, these findings may suggest that properly executed grafting and fixation procedures can restore function with reduced complications in PLWH. Future research should focus on reporting PLWH-specific outcomes to guide the development of perioperative care protocols.
Social determinants of health
Social stigma
Social stigma remains widespread and continues to impact quality of life for PLWH. Disclosure concerns and anticipation of negative perceptions are prevalent among Black and Hispanic women, men who have sex with men, and individuals with a diagnosis of 10 years or less (Beer et al 2022). Clinically, social stigma has been associated with reduced ART use and adherence, as well as an increased prevalence of missed HIV care visits (Beer et al 2022). These care lapses can lead to delayed diagnosis and treatment of wound healing complications, which can complicate recovery efforts.
Healthcare stigma
Current literature reports that lower self-rated competence in HIV care contributes to negative perceptions by healthcare professionals (Ahmed et al 2025) and can result in dehumanising treatment – such as reduced empathy and dismissive communication – in addition to confidentiality breaches (Jaimes et al 2024). These provider behaviours exacerbate shame and feelings of stigma. This internalisation has been shown to decrease with cognitive behavioural therapy and community support (Abbas et al 2023, Bhatta & Liabsuetrakul 2017, Denison et al 2020, Kalichman et al 2018). Anti-stigma training for healthcare professionals may be a beneficial adjunctive solution to improve medical care for PLWH.
Mental health and substance use
For elderly patients with HIV, studies have found an increased risk of comorbid anxiety and depression in over 40% of participants, compared with depression rates of 6%–15% and anxiety rates of up to 15% among elderly patients without HIV (Soliman et al 2020). In addition, substance use disorders (SUDs) are prevalent among PLWH, often co-existing alongside other mental health diagnoses (Lier et al 2024). Developing a mood disorder may be due to a combination of stigmas around age, sexual orientation, and race, highlighting the vulnerability of elderly and minority patients and the importance of appropriate support to aid their recovery. Patients with SUD will benefit from harm reduction services, pharmacologic treatments, and behavioural programmes (Lier et al 2024).
Gaps in literature
Evidence gathered on healing outcomes in PLWH remains sparse. Much of the literature consists of retrospective studies or single-centre series limited by low generalisability. Shortcomings with these studies include reporting complications, hospital stay duration, and functional recovery of patients without stratification by HIV disease burden (i.e. immune status, viral load, ART adherence status) and comorbidities. Such stratification is essential as these factors play a cumulative role in delaying wound healing (Talari & Goyal 2020). High-quality RCTs are needed to provide tailored guidance on NPWT efficacy and immune status-based timing of surgical interventions in PLWH.
The literature regarding perioperative antibiotic prophylactic use for PLWH is currently generalised across immunocompromised patient groups (Pletz et al 2020, Schwetz & Fauci 2019). Immunosuppression varies within a condition as heterogeneous as HIV with levels of chronic inflammatory and genetic markers differing among PLWH (Bhatta & Liabsuetrakul 2017, Freeman et al 2016). PLWH differ from treatment-induced immunocompromised patients because ongoing viral presence contributes to aberrant immune functioning in addition to immune deficiency (Schwetz & Fauci 2019). Therefore, generalisation of the immunosuppressed status obscures the unique risks and social stigma that PLWH face, potentially leading to antibiotic underuse or overuse.
Future directions
Recent studies in predictive modelling show increased SSI risk in HIV patients with independent risk factors including longer operation time, CD4 count > 430.75 µL, erythrocyte sedimentation rate > 17.46, and procalcitonin > 0.22 (Ma et al 2020). Integrating these models into electronic health record systems could provide real-time SSI risk probabilities and guide targeted antibiotic prophylaxis.
Perioperative nutrition management may address modifiable risk factors before surgery for PLWH. Immunonutrition containing arginine, nucleotides, and omega-3 fatty acids has demonstrated decreased length of hospital stay and complications in orthopaedic patients (Alito & de Aguilar-Nascimento 2015, Kaye et al 2019, Taylor et al 2025). In addition, the Enhanced Recovery After Surgery (ERAS) programme, which involves perioperative assessment of patients’ stress response to surgery, recommends a clear carbohydrate drink 2–3 h prior to surgery to decrease the risk of postoperative protein loss (Kaye et al 2019). Nutrition optimisation protocols in orthopaedic surgery are still developing. Further studies are needed to determine optimal nutritional formulation timing and duration in seropositive patients. Integrating immunonutrition with nomogram models and optimised ART could become a comprehensive strategy to reduce complications in especially high-risk patients.
Conclusion
This review highlights various factors such as immune suppression, chronic inflammation, and psychological and social influences that may impair wound healing in PLWH undergoing orthopaedic surgery. Overall, healing outcomes for PLWH on consistent ART are comparable to HIV-negative counterparts; however, the rise in osteonecrosis development with protease inhibitor use warrants informed consent and shared-decision making. Application of the ERAS protocol for preoperative assessment of immune status, CD4 cell count, and viral load can be useful in risk stratification for surveillance; however, further research is needed to guide intervention strategies and timelines. Care of PLWH in orthopaedic surgery is strengthened with a multidisciplinary team of infectious disease specialists and primary care providers who aid in monitoring healing and escalate care referrals when necessary. These efforts integrate social and psychological inputs as well as predictive modelling to achieve optimal outcomes.
Footnotes
Acknowledgements
The authors have no acknowledgements to declare. Figure 1 was created using BioRender (Hunt 2026; ![]() ).
).
Author contributions
Jocelyn Hunt: Conceptualisation, Methodology, Investigation, Writing – Original Draft, Writing – Review and Editing, Validation, Visualisation.
Kaela Williams: Data Curation, Writing – Original Draft, Writing – Review and Editing. Citation Management.
Vinay Patel: Data Curation, Writing – Original Draft, Writing – Review and Editing.
Setareh Khani: Data Curation, Writing – Original Draft, Writing – Review and Editing.
Samantha Monteriro: Data Curation, Writing – Original Draft, Writing – Review and Editing.
Emmanuela Beliard: Data Curation, Writing – Original Draft, Writing – Review and Editing.
Janae Rasmussen: Conceptualisation, Supervision, Validation, Visualisation, Writing – Review and Editing, Final Approval of Manuscript.
All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not required.
Consent to participate
Not applicable. No individual person’s data are included in this manuscript.
Consent for publication
Not applicable. No identifiable details, images, or videos were included from studies.
Statements and declarations
Not applicable. This review article did not involve studies conducted by the authors on human participants or animals.
Data availability statement
Data sharing is not applicable to this article as no new data were created or analysed in this study.