
Abstract
Acquired haemophilia A is a severe and rare coagulation disorder caused by autoantibodies (inhibitors) against factor VIII. We present a case of acquired haemophilia A diagnosed during preoperative evaluation for lung tumour resection. Laboratory evaluation showed prolonged activated partial thromboplastin time (aPTT), reduced factor VIII activity, and detectable factor VIII inhibitors. Immunosuppressive therapy with oral prednisone led to normalisation of coagulation parameters and elimination of factor VIII inhibitors within 4 weeks. Surgical resection was performed without haemorrhagic complications. This case highlights the importance of early diagnosis and timely intervention in acquired haemophilia A to enhance clinical outcomes and mitigate the risk of haemorrhagic complications. Late identification of the disorder can have potentially catastrophic consequences in patients undergoing thoracic surgery.
Keywords
Introduction
Acquired haemophilia A (AHA) is a severe and rare coagulation disorder (annual incidence ≈1.48 per million) resulting from autoantibodies (inhibitors) against factor VIII (FVIII) that leads to bleeding, which is often spontaneous and severe (Collins et al 2007). Although most cases are idiopathic, some cases are associated with malignancy (Collins et al 2007, Knoebl et al 2012). This condition is potentially life-threatening, especially in patients requiring surgery. Early identification of AHA is crucial for the multidisciplinary surgical team; late recognition of the disease or insufficient preoperative preparation can have catastrophic consequences, particularly in patients undergoing thoracic surgery.
We report a case of AHA diagnosed during the pre-anaesthetic evaluation of a patient scheduled for lung nodule resection. Preoperative assessment was essential for optimising the medical condition of the patient and reducing the risk of surgery. We obtained written patient consent and ethics committee approval to publish this case study.
Case report
A 76-year-old male was scheduled to undergo a left lower lobe segmentectomy due to a pulmonary nodule suggestive of malignancy. He had a history of dyslipidaemia, chronic obstructive pulmonary disease, smoking, and hyperuricaemia. Previous surgical interventions included transurethral resection of the prostate, transurethral bladder resection, hip replacement, and intestinal resection, all without bleeding episodes. He had allergies to nonsteroidal anti-inflammatory drugs (NSAIDs), acetaminophen, aspirin, and clavulanic acid. During the preoperative evaluation, both the pre-assessment nursing staff and the anaesthetist noticed and documented multiple ecchymoses on both forearms. The patient mentioned that these lesions had developed in the past few months due to minor trauma. There was no family history of bleeding.
The laboratory workup showed an activated partial thromboplastin time (aPTT) of 46.4 s (reference range = 21.6–30.0 s). The platelet count, prothrombin time/international normalised ratio, and fibrinogen levels were within normal limits. Further tests showed FVIII activity at 8.5% (normal = 60%–120%) and an FVIII inhibitor at 3.6 BU/mL (normal = <0.7 BU/mL) (Figure 1). A thromboelastogram (TEG) was conducted, revealing a prolonged reaction time (R) in the citrated kaolin (CK) test of 21.5 min (normal range = 4.6–9.1) (Figure 2). A panel of immunological studies was all normal or negative. AHA was identified as a suspected paraneoplastic syndrome linked to a lung tumour.
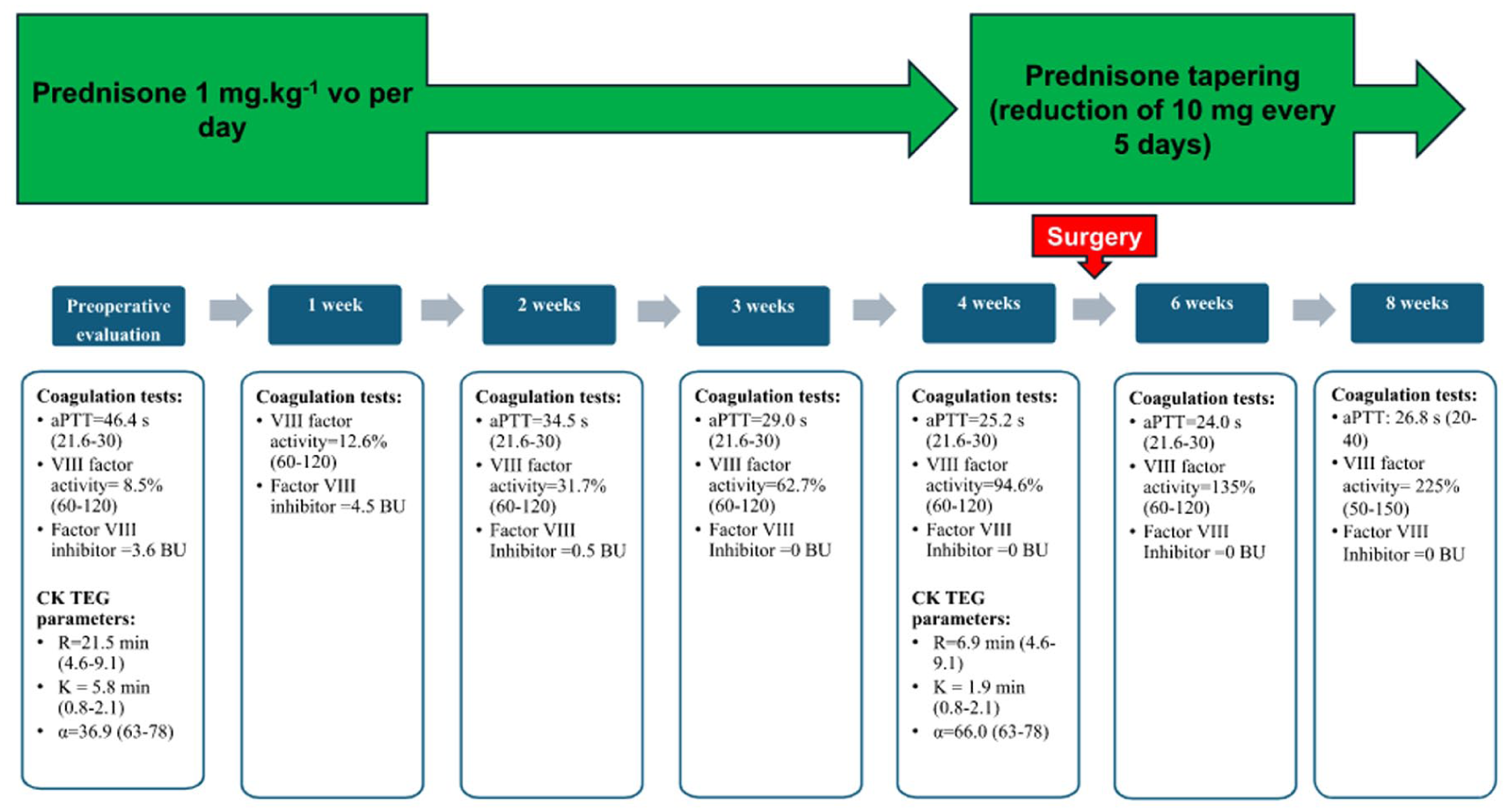
Timeline of interventions and laboratory measurements
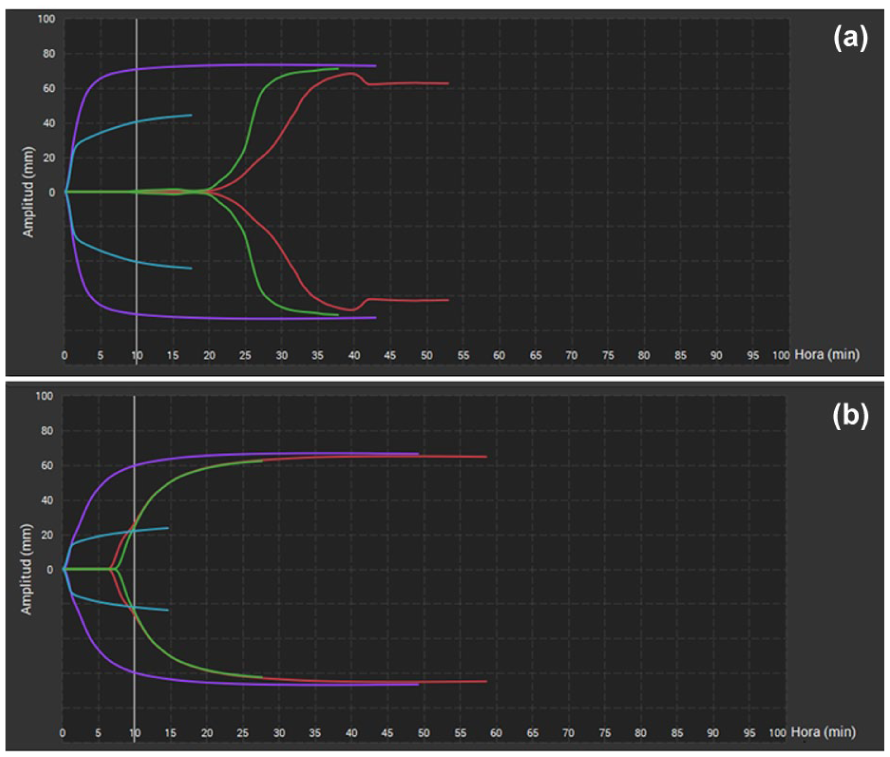
TEG6S traces: (a) preoperative evaluation showed prolonged R time and (b) after 4 weeks of immunosuppressive therapy, R time normalised
Given these findings, the anaesthetic, thoracic surgery, and haematology teams convened a multidisciplinary meeting. Because major thoracic surgery carried a high bleeding risk, the elective procedure was deferred until the coagulopathy had been corrected.
Immunosuppression was initiated with oral prednisone 1 mg⸱kg−1 per day for 4 weeks with the aim of reducing the inhibitor titre. After 4 weeks of treatment, aPTT and R in CK TEG normalised. FVIII activity exceeded 50%, and FVIII inhibitors were undetectable (Figure 1). Surgical tumour resection and lymphadenectomy were performed without significant haemorrhagic complications. Postoperatively, pharmacological thromboprophylaxis with low molecular weight heparin was introduced without adverse events, and the patient was discharged after 5 days. A tapering regimen of corticosteroids was initiated, with prednisone reduced by 10 mg per day every 5 days until the treatment was completed. Prior to discharge, comprehensive education was provided to the patient and family, focusing on the corticosteroid tapering schedule, vigilance for early bleeding signs, and the importance of immediate clinical assessment if any clinical warning symptoms occur.
At the 8-week postoperative follow-up, FVIII levels were within the normal range, and the FVIII inhibitor remained undetectable (Figure 1). In addition, TEG results had returned to normal (Figure 2). The pathological diagnosis was squamous cell carcinoma T1cN0M0. In the latest evaluation, conducted 4 months after surgery, the patient displayed no symptoms and maintained normal FVIII activity levels.
Discussion
Although AHA is a rare clinical entity, our case report highlights the importance of having a high index of suspicion in patients with lung cancer and an altered preoperative aPTT. Late recognition of the disease or insufficient preoperative preparation can have catastrophic consequences in patients undergoing thoracic surgery.
AHA usually presents two incidence peaks: the first is associated with pregnancy and autoimmune disorders, and the second occurs in older age (>60 years) (Kruse-Jarres et al 2017). Most cases are idiopathic (≈50%), but malignancy is linked to 11.8%–14.6% of cases, mainly involving solid tumour cases (Collins et al 2007, Knoebl et al 2012).
AHA is a rare condition that should be suspected in any patient presenting with recent or acute bleeding symptoms accompanied by an unexplained prolonged aPTT (Tiede et al 2020). Nevertheless, there is often a discrepancy between laboratory phenotype (aPTT and inhibitor FVIII titre) and clinical severity (Collins et al 2007). Nogami (2016) described the use of TEG to establish a bleeding risk phenotype in patients with haemophilia. TEG can offer a personalised analysis of a patient’s haemostasis to detect a haemorrhagic profile and enhance treatment. However, the usefulness of TEG in the diagnosis and treatment of AHA is not well established and requires further research.
The preoperative management of AHA should be focused on achieving three objectives: preventing and controlling bleeding, eradicating autoantibodies, and treating the underlying disease (Kruse-Jarres et al 2017). Approximately 30% of patients do not require initial haemostatic treatment due to the absence of severe haemorrhages, a clinical presentation consistent with our patient (Collins et al 2007, Knoebl et al 2012). Consequently, elective invasive procedures or major surgeries should be postponed until FVIII levels return to normal. First-line haemostatic management can be performed using bypassing agents, such as recombinant activated FVII or activated prothrombin complex concentrate, or replacement therapy with human or porcine FVIII concentrates. Porcine FVIII can achieve haemostasis, even with human inhibitors (Kruse-Jarres et al 2017, Tiede et al 2020).
The second treatment goal is to remove inhibitory autoantibodies using immunosuppressive therapy. Collins et al (2007) and Knoebl et al (2012) reported that this therapeutic approach achieves remission in about 60%–80% of patients after a median of 5–6 weeks. First-line treatment typically consists of oral prednisone 1 mg⸱kg−1 daily for a maximum of 4−6 weeks followed by tapered withdrawal (Kruse-Jarres et al 2017, Tiede et al 2020); our patient successfully achieved complete remission with this regimen, demonstrating normalised FVIII activity (>50%) and undetectable inhibitors. Patients with high-risk baseline markers (FVIII <1 IU/dL or inhibitor >20 BU) or those who do not show improvement within 3–5 weeks of first-line therapy should escalate to second-line therapy incorporating cyclophosphamide or rituximab (Kruse-Jarres et al 2017, Tiede et al 2020). Inhibitor titre and FVIII activity should be monitored at least weekly during immunosuppressive treatment. After remission, corticosteroids are tapered, and FVIII levels are monitored monthly for the first 6 months to check for recurrence.
Beyond haematological management and follow-up, this case also underscores key considerations for perioperative clinical practice. During the preoperative assessment, it is important to maintain a high index of suspicion due to the heterogeneous presentation of AHA and the limited clinical awareness of this rare entity, which frequently delays diagnosis (Kruse-Jarres et al 2017). Considering that 30% of patients remain asymptomatic at the time of diagnosis, the international recommendations published by Tiede et al (2020) emphasise that any unexplained aPTT prolongation prior to surgery should be investigated (Recommendation 1C).
These patients should undergo surgery only in specialist centres and under the direct supervision of a haematologist with expertise in this condition (Kruse-Jarres et al 2017, Tiede et al 2020). In addition, these centres should ensure access to advanced coagulation testing and prompt rescue haemostatic treatments during the perioperative period (Poston & Kruse-Jarres 2022). Before any surgical procedure, it is mandatory to assess baseline FVIII activity through detailed laboratory testing. Even when laboratory values have normalised and complete remission is achieved, close postoperative monitoring remains critical due to the persistent risk of recurrence (Kruse-Jarres et al 2017, Poston & Kruse-Jarres 2022).
Finally, regarding venous thromboembolism prophylaxis, for nonbleeding hospitalised patients with normal FVIII levels, pharmacological thromboprophylaxis should be administered in accordance with clinical guidelines (Kruse-Jarres et al 2017, Tiede et al 2020). After documented inhibitor eradication and once endogenous FVIII activity exceeds 50 IU/dL, patients who were previously on antiplatelet or anticoagulation medications may also resume these treatments as appropriate (Tiede et al 2020).
In summary, this case highlights the importance of having a high level of suspicion in patients with unexplained bruising and an isolated prolonged aPTT to achieve an early diagnosis and timely intervention in AHA to enhance clinical outcomes and mitigate the risk of severe haemorrhagic complications. Additional research is warranted to assess the potential role of thromboelastography in the diagnosis and management of AHA.
Footnotes
Author contributions
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and informed consent statements
The authors obtained written patient consent and ethics committee approval for the publication of this case study.