
Abstract
Introduction:
Preoperative anxiety is a common distressing phenomenon that negatively affects surgical outcomes and postoperative recovery. This narrative review synthesised evidence on effectiveness of non-pharmacological interventions in managing preoperative anxiety.
Methodology:
A structured literature search was conducted across PubMed, Hinari Research4Life, Cochrane Library, and Directory of Open Access Journals, focusing on studies evaluating non-pharmacological interventions in surgical patients, published within the last 5 years. Out of 359 total records identified, only 24 studies met inclusion criteria following structured screening process using Scale for the Assessment of Narrative Review Articles guidelines.
Results:
The findings suggest that various psychological interventions, including virtual reality, music therapy, mindfulness-based approaches, and cognitive-behavioural techniques, are associated with reductions in preoperative anxiety in several patient populations. These interventions offer non-invasive and potentially accessible means of improving perioperative care in well-resourced settings. However, variability in study design, intervention protocols, and outcome measures limits direct comparison across studies. As a narrative synthesis, the findings should be interpreted with consideration of these methodological differences.
Conclusion:
Non-pharmacological interventions, particularly virtual reality and mindfulness, are effective alternatives/adjuncts to pharmacological methods for reducing preoperative anxiety. However, heterogeneity of interventions and outcome measures limits generalisability. Future research should include large-scale randomised controlled trials, standardisation of outcome measures, and culturally adapted studies in different populations.
Introduction
Undergoing surgery is inherently stressful, and regardless of procedure type, patients frequently report worry, apprehension, and nervousness prior to surgery. Although preoperative anxiety represents a natural human reaction to perceived threat, it can become problematic in treatment contexts, affecting patient cooperation and recovery. Preoperative anxiety is a well-documented phenomenon experienced from the time surgery is scheduled, and it has the potential to negatively influence both psychological wellbeing and postoperative outcomes (Baagil et al 2023).
Preoperative anxiety manifests with behavioural (avoidance, agitation, sleep disturbances), emotional (fear, distress), cognitive (persistent worry and uncertainty), and physical symptoms (nausea, sweating, haemodynamic instability) (Stamenkovic et al 2018). Patients may present with palpitations, dyspnoea, abdominal pain, diarrhoea, or urinary frequency (Friedrich et al 2022). Common fears include surgical complications, disability, postoperative pain, and impaired daily functioning (Mathew et al 2022). In children, separation from parents and induction of anaesthesia exacerbate anxiety and may lead to maladaptive behaviours such as enuresis, temper tantrums, or nighttime crying (Caumo et al 2001).
The type of surgery and anaesthesia also contributes to anxiety levels (Bedaso et al 2022). Research suggests anxiety is more prevalent among women and young adults (Kiyohara et al 2004). Preanesthetic information significantly reduces anxiety, while fear of death, dependency, and family concerns predict higher anxiety levels (Woldegerima et al 2018, Zeb et al 2019).
Unmanaged preoperative anxiety has clinical consequences, including prolonged extubation time, greater postoperative pain, slower recovery, and increased risk of complications, leading to extended hospital stay and higher health care costs (Shebl et al 2025, Turksal et al 2020). Pharmacological interventions are effective but often associated with adverse effects such as hypotension, arrhythmias, respiratory depression, nausea, vomiting, and sedation (Kisielewska et al 2025). Consequently, non-pharmacological approaches provide non-invasive and potentially accessible means of improving perioperative care in well-resourced settings.
Non-pharmacological interventions target not only patients but also healthcare providers and caregivers involved in perioperative care. Evidence suggests effectiveness across different age groups. This review synthesises recent evidence on psychological, non-pharmacological strategies to alleviate preoperative anxiety.
Methodology
This narrative review was performed and reported in accordance with the Scale for the Assessment of Narrative Review Articles (SANRA) guidelines (Baethge et al 2019).
A structured literature search was performed to identify studies evaluating the effectiveness of psychological, non-pharmacological interventions in reducing preoperative anxiety among patients undergoing surgery under general or local anaesthesia. Four electronic databases were searched: PubMed, Hinari Research4Life, Cochrane Library, and the Directory of Open Access Journals. The search was completed on 24 August 2025.
A reproducible search strategy was developed for each database. For PubMed, the following search string was used: (‘Preoperative Anxiety’[Title/Abstract] OR ‘Anxiety/prevention and control’[Mesh]) AND (‘Psychological Intervention’[Title/Abstract] OR ‘Psychosocial Intervention’[Mesh]) AND (‘Surgery’[Title/Abstract] OR ‘General Surgery’[Mesh]))
Filters were applied to restrict results to articles published within the last 5 years (2020–2025), in the English language, and involving human subjects. The PubMed search yielded 239 records, which when combined with results from other databases gave a total 359 records. Equivalent search strategies, adapted to database-specific indexing systems, were used for the remaining databases.
The inclusion criteria were defined as (1) studies published within the last 5 years, (2) experimental study design, (3) use of non-pharmacological psychological interventions (PIs), (4) participants undergoing surgical procedures under general or local anaesthesia, and (5) assessment of preoperative anxiety as an outcome measure. Studies were excluded if they were review articles, meta-analyses, study protocols, non-interventional studies, not published in English, or did not assess preoperative anxiety.
Study selection followed a structured multi-stage screening process. All retrieved records were compiled and screened based on titles and abstracts using the predefined inclusion and exclusion criteria. Studies not meeting eligibility criteria were excluded at this stage. Full-text articles of potentially relevant studies were then assessed for eligibility. Reasons for exclusion at the full-text stage included lack of clearly defined PI, absence of relevant outcome measures, or ineligible study design. The study selection and screening process were performed by the authors, with uncertainties resolved through discussion.
A total of 359 records were identified across all databases. After title and abstract screening, 320 records were excluded. Thirty-nine full-text articles were assessed for eligibility, of which 15 were excluded. Finally, 24 studies met the inclusion criteria and were included in the narrative synthesis. The study selection process is illustrated in Figure 1.
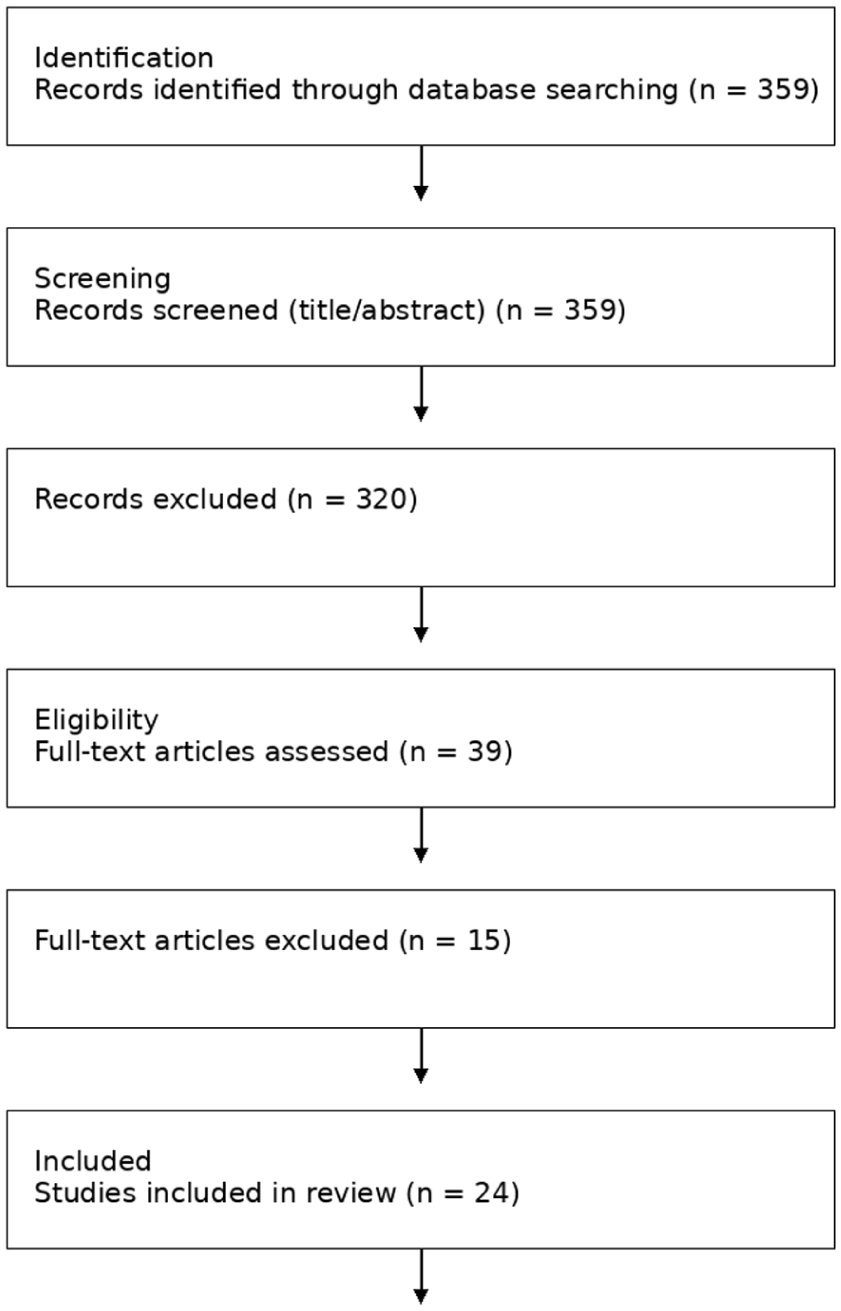
Flow diagram illustrating the study selection process for the narrative review
Data from the included studies were extracted and organised in tabular format, including study characteristics, type of intervention, sample population, and key findings. Given the narrative nature of the review, methodological quality and reporting considerations of the included studies were assessed using the SANRA framework.
Efforts were made to ensure a comprehensive and balanced synthesis of the available literature through consistent application of predefined eligibility criteria and a structured screening process. However, as a narrative review, the findings are based on qualitative synthesis rather than quantitative aggregation.
Risk of bias and quality assessment
To minimise selection bias, predefined inclusion and exclusion criteria were applied consistently across all databases. Studies were screened systematically based on relevance, study design, and outcome measures. Although this review is narrative in nature, efforts were made to ensure a comprehensive and balanced representation of available evidence.
Results
A total of 359 records were identified through database searches. After screening titles and abstracts, 320 records were excluded as they were systematic reviews or meta-analyses, lacked intervention, were study protocols, were not in English, did not involve intervention for patients’ preoperative anxiety, did not assess preoperative anxiety as an outcome, involved non-psychosocial interventions, or were duplicates, retracted articles, or had no abstract available. Thirty-nine full-text articles were then assessed for eligibility, resulting in an additional 15 exclusions due to duplication, full text not being in English, not assessing preoperative anxiety as outcome, involving non-psychosocial interventions, interventions not being clearly defined, or not involving interventions for the patient’s preoperative anxiety. Ultimately, 24 studies met the inclusion criteria and were included in the narrative review. Quality appraisal using the SANRA instrument demonstrated generally high methodological quality among the included studies, with a mean score of 10.8/12 (range 10–12). The interventions discussed in the selected studies were given to patients at time points ranging from a few weeks to a few hours before the surgery. The interventions were primarily aimed at alleviating preoperative anxiety, with some studies also assessing outcomes such as postoperative pain, fatigue, and relaxation.
The nature of the interventions varied greatly across studies, with some studies employing multiple intervention types. Some studies employed multimodal interventions and are therefore discussed across more than one category. Seven studies utilised virtual reality (VR)-based intervention, while nine studies employed educational interventions. Other intervention methods used to alleviate preoperative anxiety in the included studies were hypnosis (2), music therapy (1), cognitive behavioural therapy (CBT)-based interventions (5), mindfulness and relaxation interventions (5), Emotional Freedom Technique (EFT) intervention (1), and combined digital health intervention (1).
Wu et al (2022) found that a 5-min VR preoperative simulation in 99 children (4–12 years) undergoing elective surgery significantly reduced preoperative anxiety, improved induction compliance, and boosted parental satisfaction versus conventional verbal preparation method. Furthermore, Chiu et al (2023) reported that an 8-min immersive 360° VR video tour with education, delivered 2–4 weeks preoperatively to 74 adults undergoing their first elective surgery under general anaesthesia, significantly lowered anxiety and stress, and enhanced preparedness compared to standard care.
By contrast, studies by Liu et al (2023) and Amiri et al (2023) compared the effectiveness of VR as an immersive method of delivering content compared to standard two-dimensional (2D) video delivery. Amiri and colleagues utilised the TSCO VR glasses (model TVR 568) and displayed a 4-min and 35-s long educational video aimed at improving preoperative anxiety among patients undergoing open heart surgery. Liu and colleagues employed the YVR2 device (an HMD) to improve comfort and immersion, and the content displayed in both 2D and VR modes involved an 18-min comprehensive PI, with surgery introduction and simulation (4 min), patient interviews involving sharing experiences of anxiety and coping (8 min), and scenic virtual tours (5 min). The intervention was given to patients undergoing carotid artery stenting (CAS) procedure for the first time. Both the studies employed the State Anxiety measure from the State Trait Anxiety Inventory (18) to assess preoperative anxiety. Furthermore, Samnakay et al (2025) demonstrated that, among 200 children aged 4–13 years, distraction via 3D VR goggles during anaesthetic induction yielded similar reductions in preoperative anxiety and high induction compliance relative to 2D video on tablets, with no significant intergroup differences. Mathari et al (2024) also found that a single immersive 360° VR tour (∼24 days preoperatively) did not significantly reduce preoperative anxiety versus traditional education in 121 adults undergoing cardiac surgery, though it markedly enhanced postoperative satisfaction and preparedness.
Educational intervention: Nine of the included studies employed an educational intervention, with largely positive outcomes. Sadeghi et al (2025) used a multimedia 2D video-based intervention with overall nine separate videos focused on anatomy and function; advantage of surgery and potential complications; pre-surgical, surgical, and post-surgical procedure; and instructions for breathing exercises post-surgery. Baseline preoperative anxiety scores were also measured by the State Anxiety measure from the STAI only for two of the four groups in the Solomon four-group design (E1 – experimental and C1 – control). Outcomes assessed in the preoperative phase after intervention included preoperative anxiety as measured by the State Anxiety measure from the STAI and haemodynamic parameters for all groups (E1, E2, C1, and C2). Pain was also measured postoperatively for all groups.
The study found that multimedia education significantly reduced preoperative state anxiety in intervention groups compared to controls (p = 0.006). However, no differences in postoperative anxiety or pain were observed at 24 h post-surgery (p > 0.05). Haemodynamic parameters showed expected physiological changes perioperatively, not differing significantly between groups.
Celik and Balci (2025) found that a 10-min child-friendly animated video explaining the anaesthesia process led to significantly lower preoperative anxiety scores compared to a control group. Similarly, Bourneix et al (2025) implemented a comprehensive support procedure involving an explanatory booklet and a film of the patient pathway; while the results were not statistically significant due to a small sample size, the median anxiety score was below the cutoff in the intervention group, whereas the control group had a median anxiety score above the cutoff. For adult surgical patients, Shekhar et al (2022) conducted three 45-min psychoeducation sessions that successfully produced a significant reduction in pre-surgery anxiety levels. Kharod et al (2022) utilised a structured anaesthesia information sheet available in multiple languages, which was proven to reduce preoperative anxiety more efficiently than conventional verbal counselling. Alles et al (2023) employed a 3-week multimodal prehabilitation including cancer education and relaxation techniques that significantly lowered anxiety among newly diagnosed patients. Karamad et al (2023) targeted breast cancer patients using a training booklet approved by specialists, which resulted in significantly lower anxiety compared to routine training. Kocaturk et al (2024) demonstrated that preoperative informative interviews were effective in significantly reducing both preoperative anxiety scores in patients undergoing maxillofacial surgery. Finally, Díaz Luengo et al (2023) demonstrated in a randomised controlled trial (RCT) that preoperative information via storybooks, videos, or both – delivered to 125 parents and their children aged 8–12 undergoing surgery – significantly reduced preoperative anxiety in children and parents compared to standard care, with the combined intervention proving most effective.
Hypnosis: Hypnosis was used as an intervention in the Rousseaux et al’s (2022) study. The hypnosis intervention was provided in the form of a pre-recorded 20-min audio session including relaxing imagery (e.g. sunrise, beautiful landscape) and suggestions for positive body sensations. The hypnosis intervention was found to be similarly effective in reducing preoperative anxiety as compared to VR-based, combined VR and hypnosis interventions, and a control group (receiving standard medical care) among patients scheduled for cardiac surgery in the ICU.
Music intervention: Music therapy was employed by Li et al (2025) as an intervention to reduce perioperative anxiety and postoperative pain in young nulliparous women undergoing laparoscopic cystectomy for endometriosis. Music therapy was administered using preselected music from a hospital-developed ‘Emotional Regulation through Music’ mini-programme. Patients listened to self-selected music daily for 30 min via headphones or speakers starting 1 day before surgery and continuing for 7 postoperative days. The control group received only standard medical care without any music intervention. Post-intervention, no significant differences were observed in postoperative pain (assessed using VAS) and perioperative anxiety (assessed using GAD-7 administered at baseline as well as 1 day, 3 days, and 7 days post-surgery) between the two groups.
Digital health intervention: Kondylakis et al (2025) assessed the effectiveness of a digital health intervention, the CARINAE DH platform, in reducing perioperative stress among patients scheduled for various surgeries. The platform combines a mobile app that incorporates health recommender systems (HRSs) along with educational content and mental wellbeing exercises based on CBT principles, a VR component for educational content and mental wellbeing exercises, and a clinical web application for patient support and tools for healthcare providers. The intervention started from the first hospital visit (2–4 weeks pre-surgery) through hospital admission (1–3 days pre-surgery), discharge (1 week post-surgery), and remote follow-up (14 days post-surgery). Patients could use the intervention at home as desired, and its effectiveness was compared against standard medical care protocols. The study found that the intervention group experienced significant improvements in stress (VAS Stress at admission improved by 5%, at discharge by 11.1% compared to baseline 2–4 weeks prior to surgery), pain (VAS Pain at admission improved by 31.2% compared to baseline 2–4 weeks prior to surgery), and anxiety (HADS Anxiety after surgery improved by 15.6% compared to baseline 2–4 weeks prior to surgery). Negative affect (PANAS-Negative) at admission also improved by 17.5% compared to the baseline measure 2–4 weeks before surgery.
CBT-based intervention: Two of the included studies used manualised CBT-based interventions. Horn et al (2022) investigated whether baseline depressive symptoms, anxiety, and illness beliefs moderated effects of preoperative PIs before coronary artery bypass graft (CABG) surgery on depressive symptoms, anxiety, and illness beliefs pre-surgery, 1 week, and 6 months post-surgery. Participants were randomised to one of three groups – standard medical care (SMC), optimisation of expectations (EXPECT), or emotional support (SUPPORT). The EXPECT intervention group received a PI aimed at optimising patients’ expectations (realistic disease/surgery understanding, positive outcome expectations, self-efficacy) through two 50-min individual sessions separated by two 20-min phone calls. The SUPPORT group received a PI providing equal time/attention and emotional support, but without expectation work over the sessions. While both interventions had no significant impact on preoperative anxiety (measured by the Hospital Anxiety and Depression Scale) compared to standard medical care, patients with high baseline depressive symptoms (measured by HADS) were found to have significantly lower depressive symptoms in the intervention conditions compared to the control group.
Horn et al (2025) also utilised the EXPECT intervention delivered through a 30- to 40-min session on the day before surgery, followed by two booster phone calls (approx. 15–20 min) at 4 and 8 weeks post-surgery aimed at improving postoperative recovery by reducing illness-related disability (measured by the Pain Disability Index). The secondary outcome measures included preoperative anxiety as measured by the Amsterdam Preoperative Anxiety and Information Scale (APAIS), heart-related quality of life (Minnesota Living with Heart Failure Questionnaire – MLHFQ; SF-12 physical and mental), generalised anxiety (GAD-7), depression (PHQ-9), and expected illness perception (IPQ-E). Overall, no significant overall difference was found on the primary outcome (PDI) or preoperative anxiety for the two groups over four points of assessment – baseline, post intervention, and two post-surgery measures. However, significant moderation was observed due to the patients’ baseline need for information, where patients with a high need for information who received EXPECT had significantly less pre-surgery anxiety and fewer quality of life restrictions 4–6 days after surgery compared to the control group. Overall, the manualised CBT-based intervention was not found to be effective for preoperative anxiety reduction, but showed promise in other important outcomes post-surgery.
Shekhar et al (2022) utilised three structured sessions to help abdominal surgery patients identify and modify anxiety-inducing thoughts, while Zheng et al (2022) implemented intensive daily CBT sessions for elderly cancer patients designed to correct adverse habits and enhance treatment confidence. Similarly, Alles et al (2023) employed a multimodal approach featuring a six-step problem-solving technique to prioritise manageable stressors and address negative cognitions related to a new cancer diagnosis. These interventions yielded statistically significant reductions in preoperative anxiety scores.
Finally, Jin et al (2025) provided a 30-min PI combining CBT strategies with progressive relaxation techniques, specifically deep breathing and guided visualisation, to address preoperative distress. The study reported that while both the PI and intravenous midazolam (MID) significantly reduced preoperative anxiety scores, the former uniquely alleviated distress through mindfulness-related electrophysiological modulations (alpha and gamma bands) rather than the sedation-based mechanism observed in the pharmacological group. These findings are further discussed in the next section.
Mindfulness and relaxation intervention: Five of the included studies used mindfulness and relaxation techniques as an intervention. Jin et al (2025), as described above, compared the effects of PI and intravenous MID on alleviating preoperative anxiety in breast cancer patients, using EEG power spectrum analysis as an objective measure alongside clinical scales for anxiety (VAS-A), and other clinical monitoring indices including sedation level, heart rate, mean arterial pressure (MAP), oxygen saturation, and so on. The PI, administered around 30 min prior to surgery, involved 30+ min of cognitive therapy and progressive relaxation including deep breathing and guided visualisation (mindfulness-based approach). The comparison group received intravenous MID once at the dosage 0.02 mg/kg prior to surgery. The findings showed that both PI and MID significantly reduced VAS-A anxiety scores and MAP after intervention. The MID group showed a significant decrease in oxygen saturation and sedation level compared to the PI group. With regard to EEG power spectra analysis, both groups showed decreased theta power in the frontal-parietal region; however, the PI group showed increased alpha, beta, and gamma power in the frontal, central, and parietal regions, suggesting the effect of mindfulness intervention. The MID group, by contrast, showed increased low-frequency power and decreased gamma power reflecting the sedation effect. Thus, the two interventions reduced preoperative anxiety through different biopsychological mechanisms.
Shekhar et al (2022) gave three structured sessions of breathing and relaxation training, which led to a statistically significant reduction in anxiety levels immediately before abdominal surgery compared to a control group. Similarly, Zheng et al (2022) instructed elderly patients in imaginative relaxation techniques and deep breathing at a rate of six breaths per minute, resulting in noticeably lower preoperative anxiety scores on the day prior to surgery. In a multimodal approach for cancer patients, Alles et al (2023) combined diagnosis education with progressive deep muscle relaxation training, which significantly decreased the prevalence of anxiety compared to the control group at a 3-week follow-up prior to surgery. Hanley and Garland (2022) demonstrated that a single 15- to 20-min session of mindfulness of breath – focusing on meta-awareness of thoughts and sensations – was sufficient to induce self-transcendent states that predicted immediate and significant decreases in preoperative anxiety for orthopaedic patients.
EFT intervention: Only one of the selected studies utilised the EFT intervention for preoperative anxiety reduction. Karatas Okyay et al (2025) studied the EFT intervention, comprising two 30- to 40-min guided sessions administered 1 week apart at 32–38 weeks of gestation. The practice involved rhythmic tapping on specific acupuncture points, supplemented by twice-daily self-administered homework. They found that the practice of EFT led to a statistically significant reduction in state anxiety scores compared to the control group (p < 0.001), successfully mitigating maternal psychological distress before planned caesarean sections.
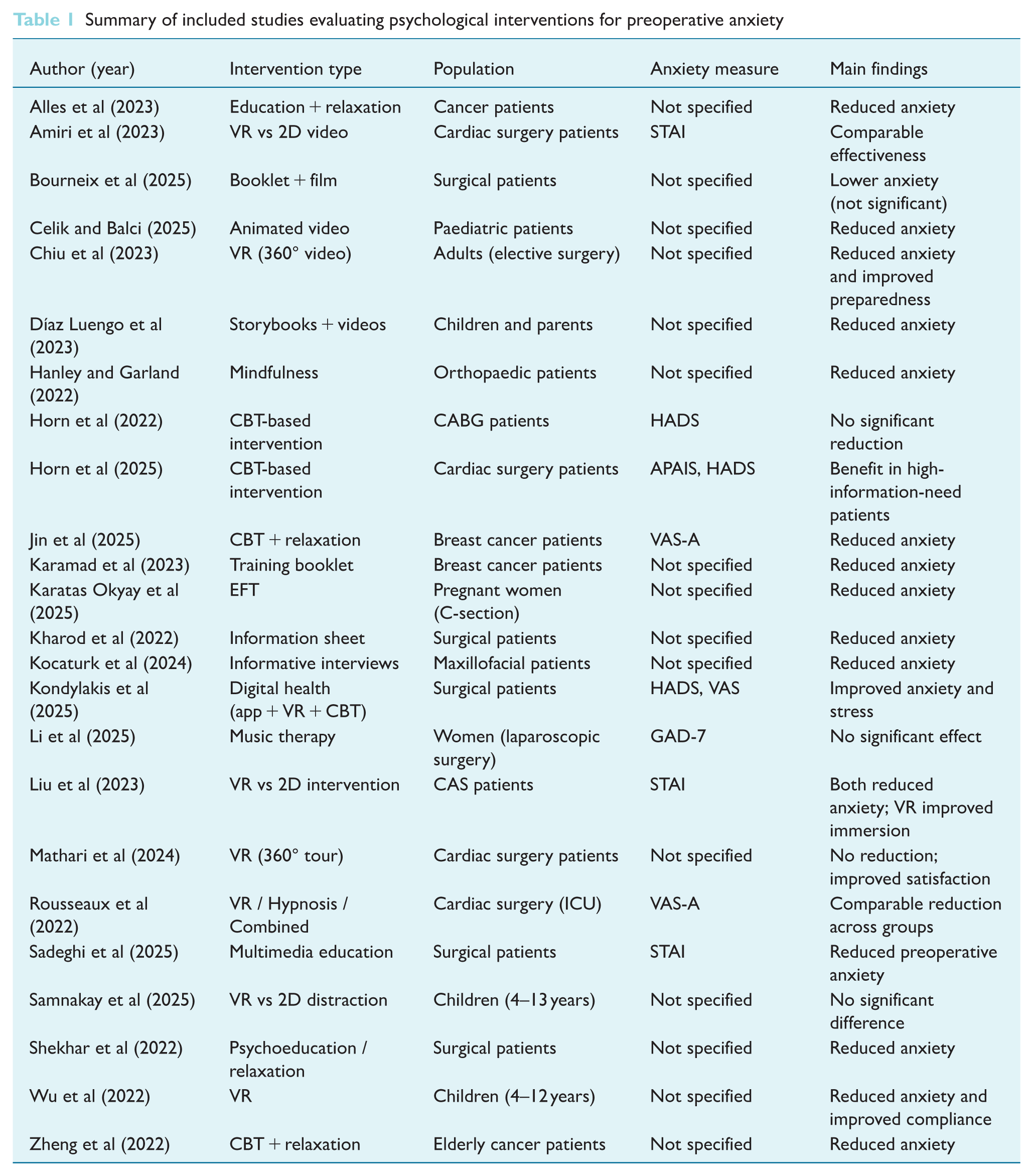
A summary of the included studies is presented in Table 1.
Summary of included studies evaluating psychological interventions for preoperative anxiety
Discussion
This narrative review aimed to synthesise the evidence on the effectiveness of non-pharmacological interventions in reducing preoperative anxiety among surgical patients. The findings from the studies reviewed suggest that a variety of PIs – including VR, CBT, educational programmes, hypnosis, EFT and mindfulness – can effectively alleviate preoperative anxiety, often with comparable results to pharmacological methods. The diverse nature of the included studies, spanning different surgical procedures and patient demographics, underscores the broad applicability of these approaches.
Synthesis of findings and clinical implications: The most frequently studied interventions identified were VR-based interventions, which were found to be more effective than standard 2D video delivery in reducing anxiety. This suggests that the immersive, multi-sensory experience of VR can possibly create a more powerful distraction and relaxation response. This has significant clinical implications, as VR offers a potentially scalable and engaging tool for pre-anaesthetic preparation, particularly for younger patients or those with high baseline anxiety.
Similarly, CBT-based and mindfulness/relaxation interventions demonstrated positive results. The study by Jin et al (2025) is particularly insightful as it objectively compared a PI to MID using EEG analysis. The finding that both approaches reduced anxiety through different biopsychological mechanisms (sedation vs active mind-body engagement) highlights the unique benefits of psychological care. For clinical practice, this means non-pharmacological methods can be used as a primary or supplementary approach, particularly for patients who may be sensitive to the side effects of sedatives like MID.
The review also showed that educational interventions, whether video-based or integrated into digital platforms, can significantly reduce anxiety. This reinforces the importance of clear, accessible patient information. However, the varying effectiveness of interventions like music therapy and CBT-based manualised approaches (Horn et al 2022, 2025) suggests that the success of these methods may depend on specific patient characteristics, the timing of the intervention, and the individual’s baseline needs, such as the need for information. Furthermore, since high-technology interventions may not be widely available in low-resource settings, simpler approaches such as written information and breathing techniques remain valuable.
Implications for perioperative practice
The findings of this review suggest several practical strategies that perioperative care staff can implement to help reduce preoperative anxiety. Simple, low-resource interventions such as guided breathing exercises or brief mindfulness techniques can be introduced in the preoperative holding area. Providing structured preoperative information through verbal counselling or written materials may also help patients with a high need for information.
For paediatric populations, tablet-based educational videos or distraction techniques may be beneficial. Where resources permit, more advanced interventions such as VR may be considered as adjuncts. Importantly, nurses should assess individual patient preferences and anxiety levels to tailor interventions accordingly.
Overall, both high-technology and low-technology approaches have value, and selection should be guided by resource availability and patient needs.
Limitations of the review
Despite the valuable insights, this review has several limitations. The included studies demonstrated heterogeneity in intervention types, outcome measures, and study populations, limiting direct comparison. As a narrative review, no formal meta-analysis was conducted. The search was restricted to English-language studies and a limited number of databases, which may have resulted in omission of relevant literature.
Future research directions
Future research should focus on conducting large-scale RCTs to further compare the efficacy of different non-pharmacological interventions against each other and against standard pharmacological care. Studies should aim to standardise outcome measures for preoperative anxiety to allow for meaningful meta-analysis. There is a critical need for research in the culturally diverse populations, exploring culturally adapted PIs and their effectiveness on local populations. In addition, future studies should investigate patient-specific factors (e.g. baseline anxiety levels, personality traits, and type of surgery) to determine which interventions are most effective for specific patient profiles. Finally, research should evaluate the long-term impact of these interventions on postoperative recovery, patient satisfaction, and overall healthcare costs.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.